
Feasibility of an Ultrasound-Based Method for Measuring Talar Displacement during the Anterior Drawer Stress Test Using a Telos Device: A Preliminary Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Anterior Drawer Stress Test
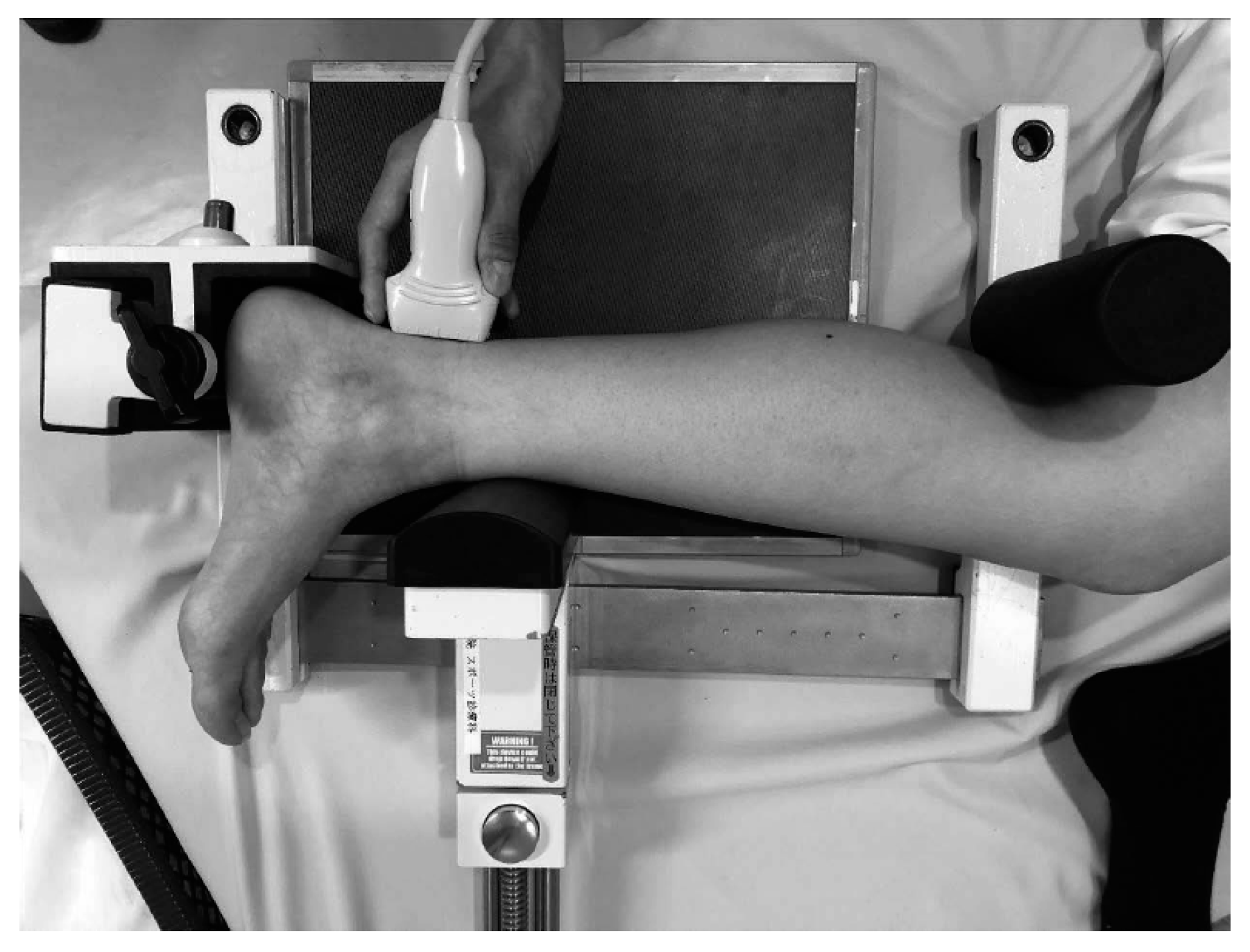
2.2.2. Positioning for the Anterior Drawer Stress Test
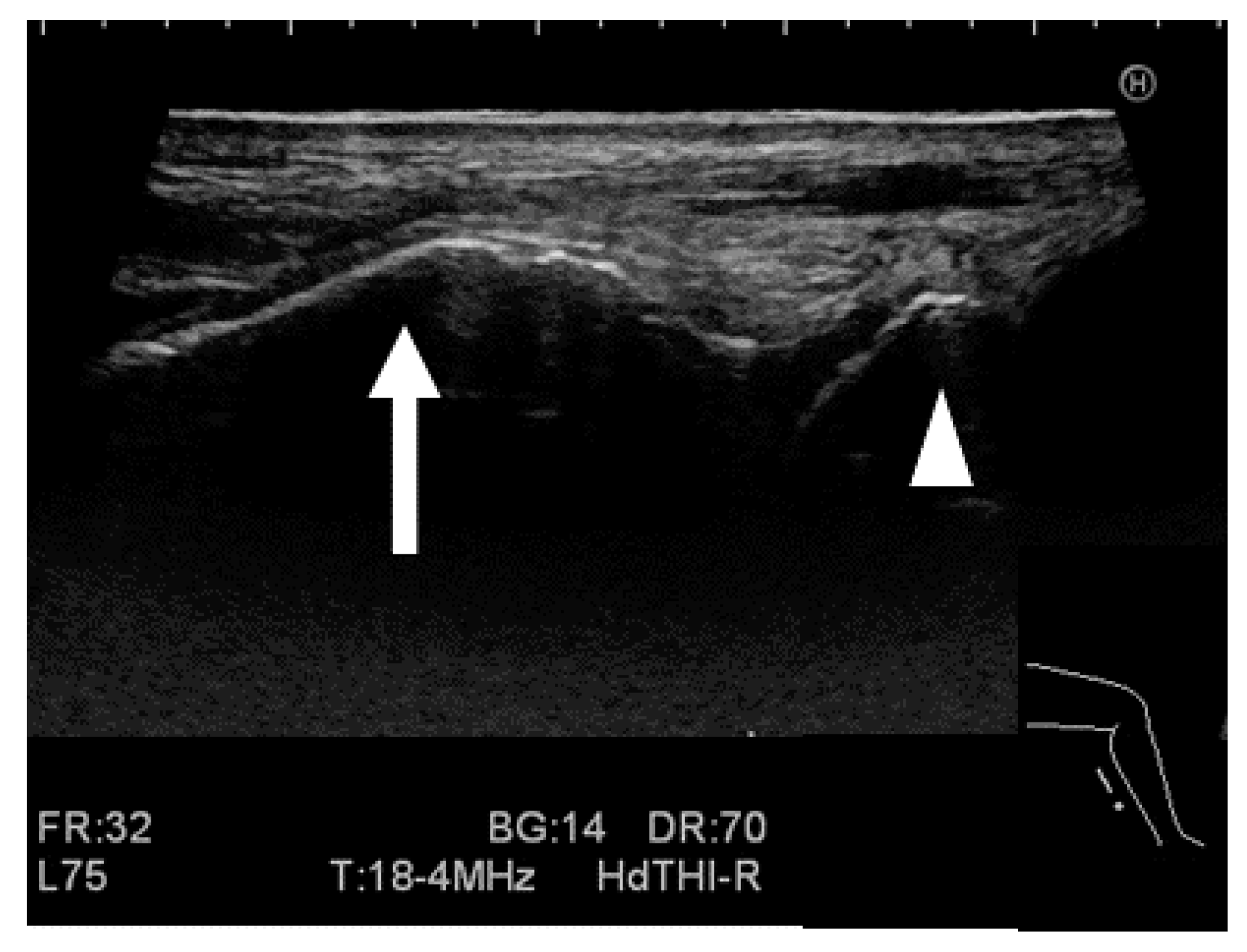
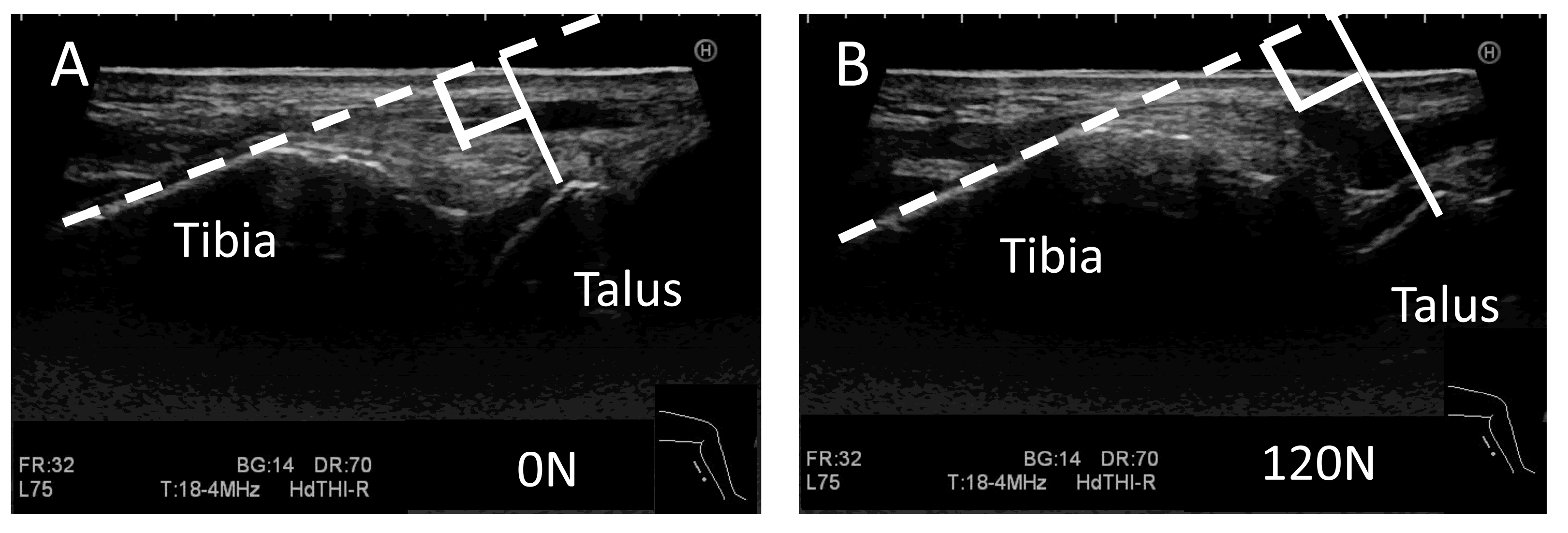
2.2.3. Ultrasound Stress Imaging Test
2.2.4. Stress X-ray Test
2.2.5. Measurement for the Stress Imaging Test
2.3. Statistical Analyses
3. Results
3.1. Self-Evaluation of Subjective Ankle Instability
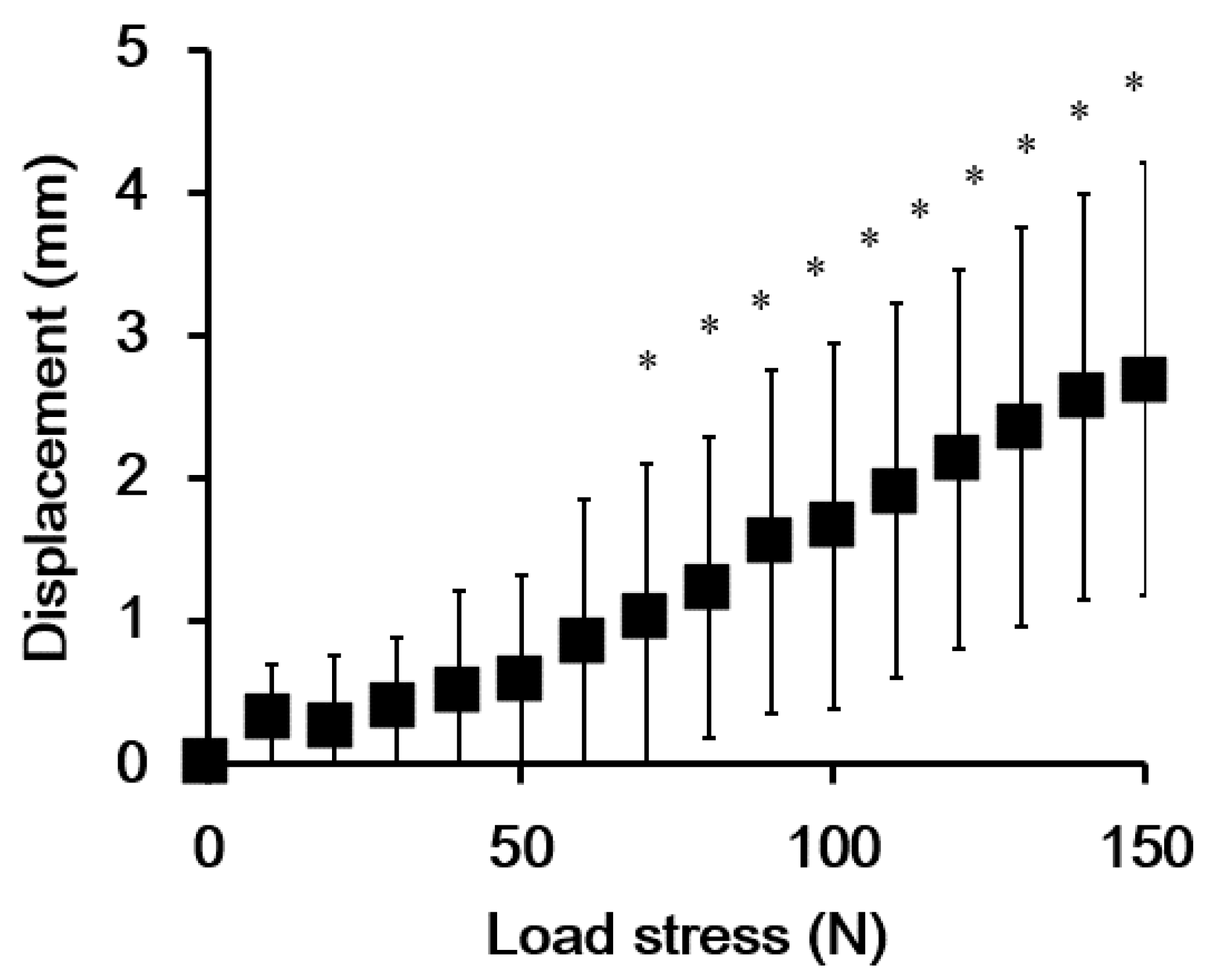
3.2. Validation of the Ultrasound-Based Method
3.3. Inter-Rater Reliability
3.4. Correlations between Talar Displacement Values Obtained from Ultrasound and X-ray Imaging Tests
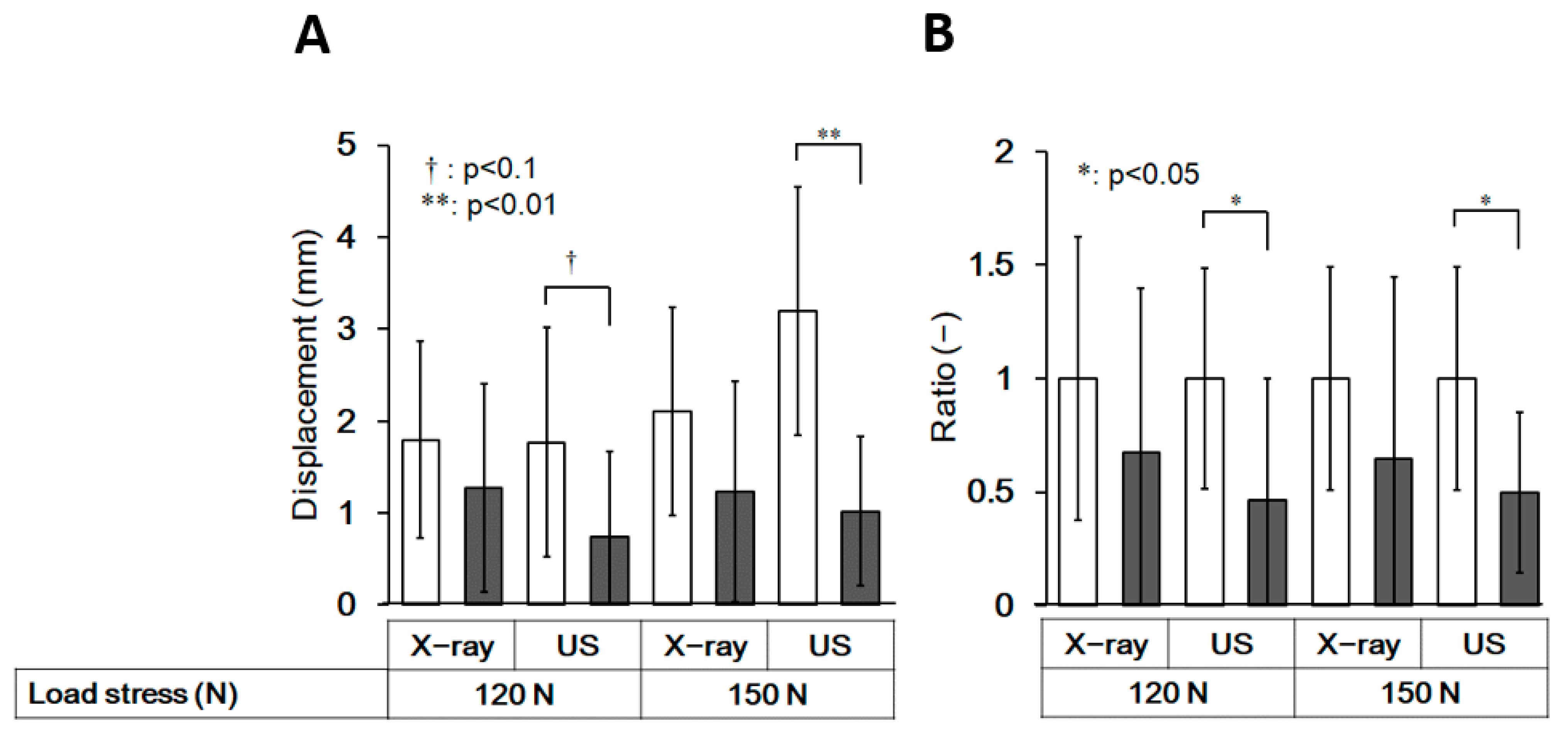
3.5. Comparison of the Extent of Anterior Displacement of the Talus between the Control and HAS Groups
3.6. Discrimination between Those with and without a History of Ankle Sprain by an Ultrasound Stress Imaging Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Swenson, D.M.; Collins, C.L.; Fields, S.K.; Dawn Comstock, R. Epidemiology of US high school sports-related ligamentous ankle injuries. Clin. J. Sport Med. 2013, 23, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.; Fourchet, F.; Fong, D.T.P.; Hertel, J.; Hiller, C.; Kaminski, T.; et al. Selection Criteria for Patients with Chronic Ankle Instability in Controlled Research: A Position Statement of the International Ankle Consortium. Br. J. Sports Med. 2014, 48, 1014–1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, P.A.; Bleakley, C.M.; Caulfield, B.M.; Docherty, C.L.; Fourchet, F.; Tik-Pui Fong, D.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; McKeon, P.O.; et al. Evidence Review for the 2016 International Ankle Consortium Consensus Statement on the Prevalence, Impact and Long-Term Consequences of Lateral Ankle Sprains. Br. J. Sports Med. 2016, 50, 1496–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gleim, G.W.; McHugh, M.P. Flexibility and Its Effects on Sports Injury and Performance. Sport Med. 1997, 24, 289–299. [Google Scholar] [CrossRef]
- Brito, L.B.; de Araújo, D.S.M.S.; de Araújo, C.G. Does Flexibility Influence the Ability to Sit and Rise from the Floor? Am. J. Phys. Med. Rehabil. 2013, 92, 241–247. [Google Scholar] [CrossRef]
- Pirri, C.; Fede, C.; Stecco, A.; Guidolin, D.; Fan, C.; Caro, R.D.; Stecco, C. Ultrasound Imaging of Crural Fascia and Epimysial Fascia Thicknesses in Basketball Players with Previous Ankle Sprains Versus Healthy Subjects. Diagnostics 2021, 11, 117. [Google Scholar] [CrossRef]
- Padua, E.; D’Amico, A.G.; Alashram, A.; Campoli, F.; Romagnoli, C.; Lombardo, M.; Quarantelli, M.; Di Pinti, E.; Tonanzi, C.; Annino, G. Effectiveness of Warm-up Routine on the Ankle Injuries Prevention in Young Female Basketball Players: A Randomized Controlled Trial. Medicina 2019, 55, 690. [Google Scholar] [CrossRef] [Green Version]
- Park, H.K.; Jung, M.K.; Park, E.; Lee, C.Y.; Jee, Y.S.; Eun, D.; Cha, J.Y.; Yoo, J. The Effect of Warm-Ups with Stretching on the Isokinetic Moments of Collegiate Men. J. Exerc. Rehabil. 2018, 14, 78–82. [Google Scholar] [CrossRef]
- Richmond, S.A.; Kang, J.; Doyle-Baker, P.K.; Nettel-Aguirre, A.; Emery, C.A. A School-Based Injury Prevention Program to Reduce Sport Injury Risk and Improve Healthy Outcomes in Youth: A Pilot Cluster-Randomized Controlled Trial. Clin. J. Sport Med. 2016, 26, 291–298. [Google Scholar] [CrossRef]
- Tarczyńska, M.; Sekuła, P.; Gawęda, K.; Szubstarski, M.; Przybylski, P.; Czekajska-Chehab, E. Stress radiography in the diagnosis and assessment of the outcomes of surgical treatment of chronic anterolateral ankle instability. Acta Radiol. 2020, 61, 783–788. [Google Scholar] [CrossRef]
- Glasgow, M.; Jackson, A.; Jamieson, A.M. Instability of the Ankle after Injury to the Lateral Ligament. J. Bone Jt. Surg. 1980, 62, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A. Evaluating and Differentiating Ankle Instability. J. Athl. Train. 2019, 54, 617–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.T.; Park, Y.U.; Jegal, H.; Park, J.W.; Choi, J.P.; Kim, J.S. New Method of Diagnosis for Chronic Ankle Instability: Comparison of Manual Anterior Drawer Test, Stress Radiography and Stress Ultrasound. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Luo, Z.P.; Kitaoka, H.B.; An, K.N. The Manual Stress Test May Not Be Sufficient to Differentiate Ankle Ligament Injuries. Clin. Biomech. 2000, 15, 619–623. [Google Scholar] [CrossRef]
- Wilkin, E.J.; Hunt, A.; Nightingale, E.J.; Munn, J.; Kilbreath, S.L.; Refshauge, K.M. Manual Testing for Ankle Instability. Man. Ther. 2012, 17, 593–596. [Google Scholar] [CrossRef]
- Oae, K.; Takao, M.; Uchio, Y.; Ochi, M. Evaluation of Anterior Talofibular Ligament Injury with Stress Radiography, Ultrasonography and MR Imaging. Skelet. Radiol. 2010, 39, 41–47. [Google Scholar] [CrossRef]
- Liu, W.; Siegler, S.; Techner, L. Quantitative Measurement of Ankle Passive Flexibility Using an Arthrometer on Sprained Ankles. Clin. Biomech. 2001, 16, 237–244. [Google Scholar] [CrossRef]
- World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed] [Green Version]
- Kunugi, S.; Masunari, A.; Noh, B.; Mori, T.; Yoshida, N.; Miyakawa, S. Cross-Cultural Adaptation, Reliability, and Validity of the Japanese Version of the Cumberland Ankle Instability Tool. Disabil. Rehabil. 2017, 39, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, J.; Peterson, L. Evaluation of Ankle Joint Function: The Use of a Scoring Scale. Foot 1991, 1, 15–19. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Rowntree, D. Statistics without Tears: A Primer for Non-Mathematicians, 1st ed.; Allyn and Bacon: Boston, MA, USA, 1981. [Google Scholar]
- Overholser, B.R.; Sowinski, K.M. Biostatistics Primer: Part 2. Nutr. Clin. Prac. 2008, 23, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Clinical Tests Have Limited Predictive Value for Chronic Ankle Instability When Conducted in the Acute Phase of a First-Time Lateral Ankle Sprain Injury. Arch. Phys. Med. Rehabil. 2018, 99, 720–725.e1. [Google Scholar] [CrossRef] [PubMed]
- Hirai, D.; Docherty, C.; Schrader, J. Severity of functional and mechanical ankle instability in an active population. Foot Ankle Int. 2009, 30, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Denegar, C.R.; Hertel, J.; Fonseca, J. The Effect of Lateral Ankle Sprain on Dorsiflexion Range of Motion, Posterior Talar Glide, and Joint Laxity. J. Orthop. Sports Phys. Ther. 2002, 32, 166–173. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | HAS | |||||||
|---|---|---|---|---|---|---|---|---|
| Load Stress (N) | ICC(2,2) | p-Value | 95% CI ‡ | SEM § | ICC(2,2) | p-Value | 95% CI ‡ | SEM § |
| 120 | 0.858 ** | 0.008 | 0.346–0.968 | 0.384 | 0.945 ** | 0.002 | 0.702–0.990 | 0.272 |
| 150 | 0.957 ** | 0.000 | 0.857–0.988 | 0.421 | 0.905 ** | 0.007 | 0.463–0.984 | 0.298 |
| Control | HAS | |||
|---|---|---|---|---|
| Load Stress (N) | R † | p-Value | R † | p-Value |
| 120 | 0.306 | 0.359 | 0.814 * | 0.026 |
| 150 | 0.044 | 0.898 | 0.827 * | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsutsumi, K.; Nakaya, U.; Koshino, Y.; Tateno, M.; Matsumoto, K.; Tanaka, M.; Yokoyama, M.; Horie, T.; Samukawa, M.; Kamishima, T.; et al. Feasibility of an Ultrasound-Based Method for Measuring Talar Displacement during the Anterior Drawer Stress Test Using a Telos Device: A Preliminary Study. Int. J. Environ. Res. Public Health 2022, 19, 2367. https://doi.org/10.3390/ijerph19042367
Tsutsumi K, Nakaya U, Koshino Y, Tateno M, Matsumoto K, Tanaka M, Yokoyama M, Horie T, Samukawa M, Kamishima T, et al. Feasibility of an Ultrasound-Based Method for Measuring Talar Displacement during the Anterior Drawer Stress Test Using a Telos Device: A Preliminary Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2367. https://doi.org/10.3390/ijerph19042367
Chicago/Turabian StyleTsutsumi, Kaori, Utayo Nakaya, Yuta Koshino, Mari Tateno, Kazuhisa Matsumoto, Mai Tanaka, Mika Yokoyama, Tatsunori Horie, Mina Samukawa, Tamotsu Kamishima, and et al. 2022. "Feasibility of an Ultrasound-Based Method for Measuring Talar Displacement during the Anterior Drawer Stress Test Using a Telos Device: A Preliminary Study" International Journal of Environmental Research and Public Health 19, no. 4: 2367. https://doi.org/10.3390/ijerph19042367
APA StyleTsutsumi, K., Nakaya, U., Koshino, Y., Tateno, M., Matsumoto, K., Tanaka, M., Yokoyama, M., Horie, T., Samukawa, M., Kamishima, T., & Tohyama, H. (2022). Feasibility of an Ultrasound-Based Method for Measuring Talar Displacement during the Anterior Drawer Stress Test Using a Telos Device: A Preliminary Study. International Journal of Environmental Research and Public Health, 19(4), 2367. https://doi.org/10.3390/ijerph19042367