
Effectiveness of a Parent Training Programme for Parents of Adolescents with Autism Spectrum Disorders: Aiming to Improve Daily Living Skills

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Difficulty in Acquiring Daily Living Skills (DLSs) for Those with Autism Spectrum Disorder (ASD)
1.2. Parent Training (PT)
2. Materials and Methods
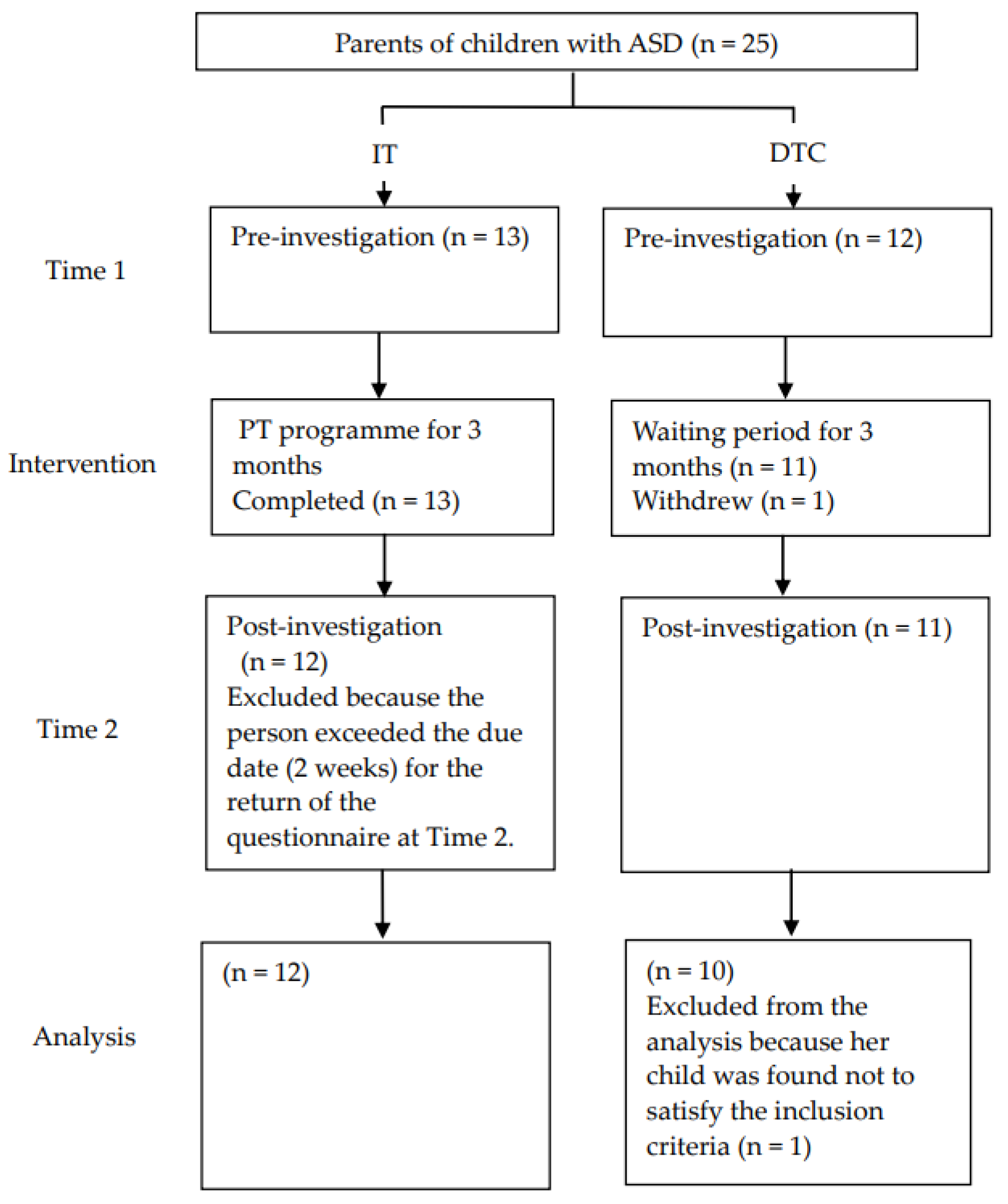
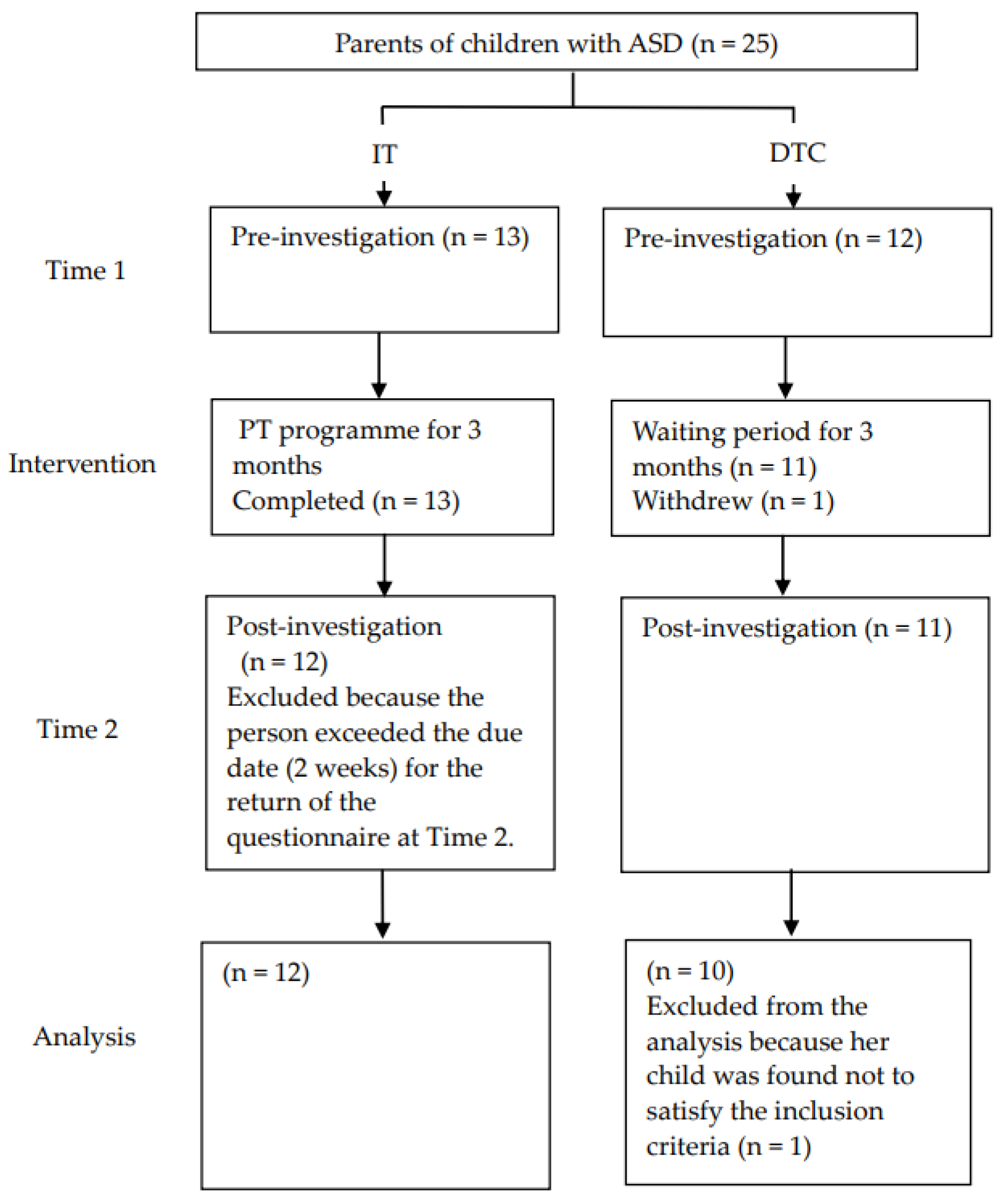
2.1. Participants
2.2. Measurement
2.2.1. Children’s Measurements
2.2.2. Parents’ Measures
2.2.3. Parent–Child Relationship Measures
2.2.4. Parents’ Statements Regarding Parent Training
2.3. The Intervention
2.4. Date Analyses
3. Results
3.1. Children’s Changes
3.2. Parents’ Changes
3.3. Parent–Child Relationship Changes
3.4. Analysis of Parents’ Statements Using the KJ Method
4. Discussion
4.1. Children’s Changes
4.2. Parents’ Changes
4.3. Parent–Child Relationship Changes
4.4. Limitations
4.5. Implications for Research and Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| (1) PT Techniques |
| Praising |
|
| How to teach DLSs |
|
| Ignoring |
|
| (2) Future tasks |
| Adolescent specific |
|
| Continuing PT techniques |
|
| Emotional control |
|
| (3) Changes due to receiving PT |
| Emotional aspects of parents |
|
| Reflection on parents’ responses to their child |
|
| Parents’ awareness |
|
| Improving parent and child behaviours |
|
| Promotion of understanding the child’s behaviour |
|
| (4) PT for adolescents |
|
| (5) Others |
|
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Sparrow, S.S.; Cicchetti, D.V.; Balla, D.A. Vineland Adaptive Behaviour Scales, 2nd ed.; Survey Forms Manual; Pearson: Minneapolis, MA, USA, 2005. [Google Scholar]
- Farley, M.A.; McMahon, W.M.; Fombonne, E.; Jenson, W.R.; Miller, J.; Gardner, M.; Block, H.; Pingree, C.B.; Ritvo, E.R.; Ritvo, R.A.; et al. Twenty-year outcome for individuals with autism and average or near-average cognitive abilities. Autism Res. 2009, 2, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Alvares, G.A.; Bebbington, K.; Cleary, D.; Evans, K.; Glasson, E.J.; Maybery, M.T.; Pillar, S.; Uljarević, M.; Varcin, K.; Wray, J.; et al. The misnomer of ‘high functioning autism’: Intelligence is an imprecise predictor of functional abilities at diagnosis. Autism 2020, 24, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Duncan, A.W.; Bishop, S.L. Understanding the gap between cognitive abilities and daily living skills in adolescents with autism spectrum disorders with average intelligence. Autism 2015, 19, 64–72. [Google Scholar] [CrossRef]
- Kanne, S.M.; Gerber, A.J.; Quirmbach, L.M.; Sparrow, S.S.; Cicchetti, D.V.; Saulnier, C.A. The role of adaptive behavior in autism spectrum disorders: Implications for functional outcome. J. Autism Dev. Disord. 2011, 41, 1007–1018. [Google Scholar] [CrossRef] [PubMed]
- Howlin, P.; Goode, S.; Hutton, J.; Rutter, M. Adult outcome for children with autism. J. Child Psychol. Psychiatry 2004, 45, 212–229. [Google Scholar] [CrossRef] [PubMed]
- Orsmond, G.I.; Shattuck, P.T.; Cooper, B.P.; Sterzing, P.R.; Anderson, K.A. Social participation among young adults with an autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 2710–2719. [Google Scholar] [CrossRef]
- Pugliese, C.E.; Anthony, L.; Strang, J.F.; Dudley, K.; Wallace, G.L.; Kenworthy, L. Increasing Adaptive Behavior Skill Deficits from Childhood to Adolescence in Autism Spectrum Disorder: Role of Executive Function. J. Autism Dev. Disord. 2015, 45, 1579–1587. [Google Scholar] [CrossRef]
- Pugliese, C.E.; Anthony, L.G.; Strang, J.F.; Dudley, K.; Wallace, G.L.; Naiman, D.Q.; Kenworthy, L. Longitudinal examination of adaptive behavior in autism spectrum disorders: Influence of executive function. J. Autism Dev. Disord. 2016, 46, 467–477. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.A.; Watson, S.L. The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 629–642. [Google Scholar] [CrossRef]
- Smith, L.E.; Hong, J.; Seltzer, M.M.; Greenberg, J.S.; Almeida, D.M.; Bishop, S.L. Daily experiences among mothers of adolescents and adults with autism spectrum disorder. J. Autism Dev. Disord. 2010, 40, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Kars, J.S.; Hecke, A.V.V. Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clin. Child Fam. Psychol. Rev. 2012, 15, 247–277. [Google Scholar] [CrossRef]
- Chiang, H.M.; Ni, X.; Lee, Y.S. Life Skills Training for middle and high school students with autism. J. Autism Dev. Disord. 2017, 47, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Okuno, H.; Nagai, T.; Sakai, S.; Mohri, I.; Yamamoto, T.; Yoshizaki, A.; Kato, K.; Tachibana, M.; Iwasaka, H.; Taniike, M. Effectiveness of modified parent training for mothers of children with pervasive developmental disorder on parents confidence and children’s behavior. Brain Dev. 2011, 33, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Iwasaka, H.; Shimizu, T.; Iida, J.; Kawabata, Y.; Chikaike, M.; Onishi, T.; Kishimoto, T. Efficacy of a parenting program as attention/hyperactivity disorder (AD/HD) therapy. Jpn. J. Child Adolesc. Psychiatry 2002, 43, 483–497. (In Japanese) [Google Scholar]
- Barkley, R.A. Defiant Children: A Clinician’s Manual for Parent Training, 2nd ed.; Guilford Press: New York, NY, USA, 1987. [Google Scholar]
- Whitham, C. Win the Whining War and Other Skirmishes: A Family Peace Plan; Perspective Publishing: Los Angeles, CA, USA, 1991. [Google Scholar]
- Kubo, N.; Iwasaka, H. Critical factors in the effectiveness of a modified parent training program as therapeutic intervention for children with pervasive developmental disorders. Jpn. J. Child Adolesc. Psychiatry 2013, 54, 552–570. (In Japanese) [Google Scholar]
- Black, M.E.; Therrien, W.J. Parent training programs for school-age children with autism: A systematic review. Remedial Spec. Educ. 2018, 39, 243–256. [Google Scholar] [CrossRef]
- Deb, S.; Retzer, A.; Roy, M.; Acharya, R.; Limbu, B.; Roy, A. The effectiveness of parent training for children with autism spectrum disorder: A systematic review and meta-analyses. BMC Psychiatry 2020, 20, 583. [Google Scholar] [CrossRef]
- Matsuo, R.; Inoue, M.; Maegaki, Y. A comparative evaluation of parent training for parents of adolescents with developmental disorders. Yonago Acta Med. 2015, 58, 109–114. [Google Scholar]
- Japanese WISC-IV Publication Committee. Japanese Wechsler Intelligence Scale for Children, 4th ed.; Nihon Bunka Kagakusha: Tokyo, Japan, 2010. [Google Scholar]
- Tsujii, M.; Murakami, T.; Kuroda, M.; Itou, H.; Hagiwara, T.; Someki, F. Vineland-II Adaptive Behavior Scales Manual, Japanese Version; Nihon Bunka Kagakusha: Tokyo, Japan, 2014. [Google Scholar]
- Achenbach, T.M. Integrative Guide for the 1991 CBCLI/4–18, YSR, and TRF Profiles; University of Vermont: Burlington, VT, USA, 1991. [Google Scholar]
- Itani, T.; Kanbayashi, Y.; Nakata, Y.; Kita, M.; Fujii, H.; Kuramoto, H.; Negishi, Y.; Tezuka, M.; Okada, A.; Natori, H. Standardization of child behavior checklist for ages 6–18. Psychiatr. Neurol. Paediatr. Jpn. 2001, 41, 243–252. [Google Scholar]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale, 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Kamio, Y. Japanese Social Responsiveness Scale, 2nd edition Manual; Nihon Bunka Kagakusha: Tokyo, Japan, 2017. [Google Scholar]
- Abidin, R.R. Parenting Stress Index Manual, 3rd ed.; Psychological Assessment Resources, Inc.: Odessa, FL, USA, 1990. [Google Scholar]
- Kanematsu, Y.; Araki, A.; Narama, M.; Shirahata, N.; Marumitsu, M.; Araya, R. Japanese Parenting Stress Index Manual; Koyoumondai Kenkyukai: Tokyo, Japan, 1999. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Kojima, M.; Furukawa, J. Japanese Manual for the Beck Depression Inventory-II; Nihon Bunka Kagakusha: Tokyo, Japan, 2003. [Google Scholar]
- Shinagawa, F.; Shinagawa, T.; Morikami, S.; Kawai, Y. TK-shiki Shindanteki Shin Oyakokankeikensa Manual (New TK Diagnostic Test for Parent-Child Relationship); Taken Publishing: Tokyo, Japan, 1972. [Google Scholar]
- Kawakita, J. Hassou-hou: Souzousei Kaihatsu no Tameni (The Way of Thinking for Creative Development); Chuokoron-shinsha: Tokyo, Japan, 1967. [Google Scholar]
- Duncan, A.; Meinzen-Derr, J.; Ruble, L.A.; Fassler, C.; Stark, L.J. A pilot randomized controlled trial of a daily living skills intervention for adolescents with autism. J. Autism Dev. Disord. 2022, 52, 938–949. [Google Scholar] [CrossRef]
- Duncan, A.; Ruble, L.A.; Meinzen, D.J.; Thomas, C.; Stark, L.J. Preliminary efficacy of a daily living skills intervention for adolescents with high-functioning autism spectrum disorder. Autism 2018, 22, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Kamiyama, T.; Ueno, A.; Noro, F. Parenting interventions for parents of children with developmental disabilities: A review and future directions. Jpn. J. Spec. Educ. 2011, 49, 361–375. [Google Scholar] [CrossRef] [Green Version]
- Okuno, H.; Nagai, T.; Mohri, I.; Yoshizaki, A.; Yamamoto, T.; Sakai, S.; Iwasaka, H.; Taniike, M. Effectiveness of a modified parent training of smaller group and shorter schedules for children with pervasive developmental disorders. No Hattatsu 2013, 45, 26–32. [Google Scholar]
- Duncan, A.; Liddle, M.; Stark, J.L. Iterative development of a daily living skills intervention for adolescents with autism without an intellectual disability. Clin. Child Fam. Psychol. Rev. 2021, 24, 744–764. [Google Scholar] [CrossRef]
| Session | Contents | Homework |
|---|---|---|
| 〈Session 1〉 Behavioural observation and understanding of ASD characteristics |
|
|
| 〈Session 2〉 Focus on good behaviours |
|
|
| 〈Session 3〉 Instructions that are easy for children to understand |
|
|
| 〈Session 4〉 Token economy |
|
|
| ||
| 〈Session 5〉 DLS support items Limit setting |
|
|
| 〈Session 6〉 Cooperation with school Summary |
| |
| 〈Follow-up〉 Conducted three months after the end of Session 6 |
|
| Variable | Group | T | χ2 | p | |||
|---|---|---|---|---|---|---|---|
| IT (n = 12) | DTC (n = 10) | ||||||
| Children | |||||||
| Age | Mean (SD) | 12.42 (1.61) | 11.50 (1.43) | 1.40 | 0.18 | ||
| Gender | Male | n | 11 | 9 | 0.02 | 0.89 | |
| Female | n | 1 | 1 | ||||
| WISC-IV | Full-scale IQ | Mean (SD) | 81.33 (9.02) | 85.20 (10.26) | −0.94 | 0.36 | |
| Type of schooling | Regular class | n | 1 | 3 | 0.19 | 0.23 | |
| Special education class | n | 11 | 7 | ||||
| Experience of professional support for parenting or childcare | Yes | n | 10 | 10 | 0.18 | 0.29 | |
| None | n | 2 | 0 | ||||
| Sibling | None | n | 6 | 2 | 2.84 | 0.24 | |
| One | n | 5 | 5 | ||||
| Two or more | n | 1 | 3 | ||||
| Parents | |||||||
| Age | Mean (SD) | 44.58 (4.76) | 43.70 (4.19) | 0.46 | 0.65 | ||
| University degree | Yes | n | 5 | 3 | 0.64 | 0.73 | |
| No | n | 5 | 4 | ||||
| Information not available | n | 2 | 3 | ||||
| Marital status | Single | n | 0 | 1 | 1.26 | 0.26 | |
| Married | n | 12 | 9 | ||||
| Measure | Group | n | Time 1 | Time 2 | F | p | Partial η2 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||||
| VABS-II | Composite | IT | 12 | 49.80 | 7.76 | 56.40 | 5.95 | — | ||
| DTC | 10 | 58.80 | 13.41 | 60.10 | 11.88 | |||||
| Communication | IT | 12 | 46.92 | 10.94 | 55.75 | 9.54 | 5.43 | 0.03 | 0.22 | |
| DTC | 10 | 59.40 | 15.44 | 58.00 | 13.93 | |||||
| DLSs | IT | 12 | 60.30 | 11.61 | 68.30 | 11.43 | 0.63 | 0.44 | 0.03 | |
| DTC | 10 | 69.70 | 10.61 | 72.60 | 9.89 | |||||
| Socialisation | IT | 12 | 55.75 | 10.42 | 62.25 | 4.51 | — | |||
| DTC | 10 | 61.90 | 14.76 | 63.60 | 13.60 | |||||
| CBCL | Internalisation T score | IT | 12 | 63.92 | 4.54 | 61.00 | 7.22 | 1.14 | 0.30 | 0.06 |
| DTC | 10 | 64.20 | 6.95 | 63.80 | 8.68 | |||||
| Externalisation T score | IT | 12 | 54.58 | 7.79 | 55.58 | 9.16 | 2.65 | 0.12 | 0.12 | |
| DTC | 10 | 62.30 | 8.74 | 59.10 | 10.47 | |||||
| SRS-2 | SCI T score | IT | 11 | 68.27 | 5.88 | 65.64 | 5.03 | — | ||
| DTC | 10 | 73.00 | 10.68 | 71.70 | 10.28 | |||||
| RRB T score | IT | 11 | 70.73 | 10.33 | 72.09 | 11.65 | 0.79 | 0.38 | 0.04 | |
| DTC | 10 | 69.70 | 14.50 | 68.00 | 15.25 | |||||
| Social awareness | IT | 11 | 56.27 | 6.89 | 59.45 | 7.71 | 1.14 | 0.30 | 0.06 | |
| DTC | 10 | 64.00 | 7.44 | 60.80 | 9.61 | |||||
| Social cognition | IT | 11 | 70.64 | 9.48 | 68.27 | 9.00 | 1.67 | 0.21 | 0.09 | |
| DTC | 10 | 73.90 | 10.31 | 73.90 | 8.91 | |||||
| Communication | IT | 11 | 68.55 | 5.74 | 65.36 | 7.94 | 1.09 | 0.31 | 0.06 | |
| DTC | 10 | 73.10 | 10.63 | 71.90 | 10.52 | |||||
| Social motivation | IT | 11 | 61.27 | 14.72 | 58.27 | 14.60 | 0.22 | 0.65 | 0.01 | |
| DTC | 10 | 65.00 | 13.69 | 62.00 | 6.34 | |||||
| Restricted interest and repetitive behaviour | IT | 11 | 71.18 | 9.86 | 72.09 | 11.65 | 0.73 | 0.40 | 0.04 | |
| DTC | 10 | 70.00 | 14.32 | 68.00 | 15.25 | |||||
| Child’s Number | DLSs Determined as a Goal at Session 4 | Achievement Classification of DLSs (Mother’s Report) | Other DLSs Conducted |
|---|---|---|---|
| 1 |
| 1 1 | |
| 2 |
| 3 |
|
| 3 |
| 2 | |
| 4 |
| 3 |
|
| 5 |
| 2 | |
| 6 |
| 1 | |
| 7 |
| 2 2 |
|
| 8 |
| 2 2 2 | |
| 9 |
| 1 |
|
| 10 |
| 3 |
|
| 11 |
| 2 |
|
| 12 |
| 2 |
| Measure | Group | n | Time 1 | Time 2 | F | p | Partial η2 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||||
| PSI Parenting Stress Index | Parent Total | IT | 12 | 111.00 | 12.63 | 110.41 | 16.69 | 0.01 | 0.91 | <0.01 |
| DTC | 10 | 115.30 | 24.03 | 113.00 | 19.91 | |||||
| Child Total | IT | 12 | 101.42 | 14.82 | 102.08 | 12.43 | 1.80 | 0.20 | 0.09 | |
| DTC | 10 | 116.60 | 15.60 | 108.90 | 20.54 | |||||
| BDI-II | Total score | IT | 12 | 11.17 | 6.59 | 12.25 | 8.31 | 3.86 | 0.06 | 0.17 |
| DTC | 10 | 13.00 | 8.76 | 10.20 | 7.36 | |||||
| Measure | Group | n | Time 1 | Time 2 | F | p | Partial η2 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||||
| Q 1 | Do you watch your child’s growth without becoming impatient? | IT | 12 | 2.83 | 0.90 | 3.17 | 0.69 | 0.90 | 0.35 | 0.05 |
| DTC | 10 | 2.80 | 0.98 | 2.90 | 0.94 | |||||
| Q 2 | Do you accept your child’s diagnosis of ASD? | IT | 12 | 4.67 | 0.47 | 4.33 | 0.85 | 0.35 | 0.56 | 0.02 |
| DTC | 10 | 3.40 | 1.50 | 4.10 | 0.70 | |||||
| Q 3 | Do you let your child do what he/she can do by him/herself? | IT | 12 | 3.58 | 0.76 | 3.42 | 0.95 | 0.16 | 0.70 | 0.01 |
| DTC | 10 | 3.70 | 0.90 | 3.60 | 0.66 | |||||
| Q 4 | Do you praise your child once or more a day? | IT | 12 | 3.08 | 1.26 | 3.75 | 1.23 | 4.70 | 0.04 | 0.20 |
| DTC | 10 | 3.10 | 1.04 | 2.90 | 1.22 | |||||
| Q 5 | Do you prepare a place where your child can relax? | IT | 12 | 3.67 | 1.11 | 3.50 | 1.04 | 1.45 | 0.24 | 0.07 |
| DTC | 10 | 3.00 | 0.89 | 3.70 | 1.00 | |||||
| Q 6 | Do you help your child to make friends? | IT | 12 | 3.08 | 0.95 | 3.08 | 1.11 | 0.37 | 0.55 | 0.02 |
| DTC | 10 | 3.00 | 1.10 | 2.80 | 0.87 | |||||
| Q 7 | Can you cope with your child’s inappropriate behaviour? | IT | 12 | 2.92 | 1.11 | 3.33 | 0.62 | 0.76 | 0.39 | 0.04 |
| DTC | 10 | 3.30 | 0.90 | 3.10 | 0.70 | |||||
| Q 8 | Do you communicate adequately with the school about your child’s problems in school? | IT | 12 | 3.75 | 0.83 | 3.58 | 0.76 | <0.01 | 0.96 | <0.01 |
| DTC | 10 | 3.60 | 0.80 | 3.50 | 0.67 | |||||
| Q 9 | Do you blame yourself less for having a child with ASD? | IT | 12 | 3.25 | 0.72 | 3.33 | 0.85 | 0.09 | 0.77 | <0.01 |
| DTC | 10 | 3.20 | 0.87 | 3.20 | 0.98 | |||||
| Q 10 | Are you less worried about your child? | IT | 12 | 2.75 | 0.72 | 2.75 | 0.83 | 0.06 | 0.80 | <0.01 |
| DTC | 10 | 2.60 | 1.02 | 2.70 | 1.10 | |||||
| Q 11 | Do you spend time on your own health or enjoyment? | IT | 12 | 3.00 | 0.91 | 3.25 | 0.83 | 0.02 | 0.88 | <0.01 |
| DTC | 10 | 3.70 | 1.00 | 3.60 | 1.20 | |||||
| Q 12 | Do you quarrel less with your family due to your child’s behaviour? | IT | 12 | 3.08 | 0.86 | 2.75 | 1.09 | 3.04 | 0.10 | 0.15 |
| DTC | 10 | 2.80 | 0.98 | 3.20 | 0.75 | |||||
| Q 13 | Do you ask your family members to assist your child? | IT | 12 | 3.25 | 1.01 | 2.92 | 1.04 | 0.02 | 0.90 | <0.01 |
| DTC | 10 | 2.50 | 1.02 | 2.60 | 1.11 | |||||
| Q 14 | Do you consult your family or friends about your troubles and not worry by yourself? | IT | 12 | 3.92 | 1.11 | 4.00 | 0.82 | ― | ||
| DTC | 10 | 3.40 | 1.20 | 3.50 | 1.28 | |||||
| Q 15 | Do you share your feelings with families who have children with a similar problem? | IT | 12 | 3.42 | 1.26 | 3.58 | 1.04 | <0.01 | 0.99 | <0.01 |
| DTC | 10 | 3.30 | 1.19 | 3.50 | 1.12 | |||||
| Q 16 | Do you utilise medical facilities and school and consultative organisations if required? | IT | 12 | 3.92 | 0.86 | 3.92 | 0.76 | 1.39 | 0.26 | 0.07 |
| DTC | 10 | 4.00 | 0.77 | 4.30 | 0.90 | |||||
| Q 17 | Do you understand your child’s behaviours and ideas/feelings/thoughts? | IT | 12 | 3.00 | 1.15 | 3.58 | 0.98 | 3.96 | 0.06 | 0.17 |
| DTC | 10 | 3.20 | 0.98 | 2.80 | 1.07 | |||||
| Q 18 | Do you feel happy being with your child? | IT | 12 | 3.83 | 1.34 | 3.92 | 1.04 | 0.25 | 0.62 | 0.01 |
| DTC | 10 | 3.60 | 1.02 | 3.60 | 1.11 | |||||
| Measure | Group | n | Time 1 | Time 2 | F | p | Partial η2 | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||||
| Dissatisfaction | IT | 12 | 25.83 | 3.05 | 24.58 | 5.13 | 0.75 | 0.39 | 0.04 |
| DTC | 9 | 24.56 | 2.67 | 24.67 | 2.78 | ||||
| Blame | IT | 12 | 24.67 | 3.59 | 23.75 | 4.81 | 0.05 | 0.83 | <0.01 |
| DTC | 9 | 27.00 | 1.76 | 24.89 | 3.06 | ||||
| Strictness | IT | 12 | 24.83 | 4.71 | 23.25 | 5.51 | 0.15 | 0.70 | 0.01 |
| DTC | 9 | 25.56 | 2.67 | 23.44 | 4.56 | ||||
| Expectations | IT | 12 | 25.58 | 4.96 | 24.50 | 4.82 | 0.01 | 0.94 | <0.01 |
| DTC | 9 | 24.33 | 5.75 | 23.67 | 5.79 | ||||
| Interference | IT | 12 | 22.17 | 4.74 | 21.89 | 5.22 | <0.01 | 0.99 | <0.01 |
| DTC | 9 | 23.00 | 4.24 | 22.44 | 4.93 | ||||
| Worry | IT | 12 | 21.75 | 5.60 | 22.00 | 4.73 | 0.71 | 0.41 | 0.04 |
| DTC | 9 | 21.22 | 4.66 | 23.11 | 4.89 | ||||
| Doting | IT | 12 | 18.83 | 6.00 | 20.83 | 5.96 | 0.52 | 0.48 | 0.03 |
| DTC | 9 | 21.56 | 4.22 | 23.67 | 4.24 | ||||
| Obedience | IT | 12 | 22.17 | 5.34 | 23.08 | 4.94 | 0.12 | 0.73 | 0.01 |
| DTC | 9 | 23.00 | 2.11 | 24.22 | 4.32 | ||||
| Contradiction | IT | 12 | 22.58 | 4.86 | 21.75 | 5.36 | 0.30 | 0.59 | 0.02 |
| DTC | 9 | 25.56 | 3.13 | 24.56 | 3.25 | ||||
| Measure | Group | n | Time 1 | Time 2 | F | p | Partial η2 | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||||
| Dissatisfaction | IT | 12 | 24.50 | 1.26 | 23.08 | 2.11 | 6.41 | 0.02 | 0.25 |
| DTC | 10 | 21.60 | 2.11 | 21.80 | 3.40 | ||||
| Blame | IT | 12 | 23.00 | 3.61 | 23.33 | 3.92 | 0.26 | 0.62 | 0.01 |
| DTC | 10 | 21.90 | 4.01 | 21.90 | 4.25 | ||||
| Strictness | IT | 12 | 23.25 | 2.35 | 23.42 | 3.20 | 0.40 | 0.53 | 0.02 |
| DTC | 10 | 22.30 | 2.72 | 22.10 | 2.91 | ||||
| Expectations | IT | 12 | 24.33 | 3.25 | 24.83 | 4.55 | — | ||
| DTC | 10 | 24.20 | 3.79 | 24.50 | 3.34 | ||||
| Interference | IT | 12 | 20.17 | 2.48 | 21.33 | 4.08 | 0.44 | 0.51 | 0.02 |
| DTC | 10 | 19.70 | 2.79 | 20.10 | 3.04 | ||||
| Worry | IT | 12 | 23.92 | 3.40 | 22.83 | 3.76 | 0.18 | 0.67 | 0.01 |
| DTC | 10 | 22.50 | 2.54 | 22.30 | 3.40 | ||||
| Doting | IT | 12 | 24.75 | 3.37 | 24.17 | 3.59 | 0.39 | 0.54 | 0.02 |
| DTC | 10 | 23.70 | 1.27 | 23.80 | 2.30 | ||||
| Obedience | IT | 12 | 24.08 | 3.12 | 23.08 | 3.99 | 1.34 | 0.26 | 0.07 |
| DTC | 10 | 23.80 | 2.27 | 24.00 | 2.83 | ||||
| Contradiction | IT | 12 | 24.42 | 2.10 | 25.00 | 4.07 | — | ||
| DTC | 10 | 23.30 | 2.15 | 23.70 | 1.64 | ||||
| Disagreement | IT | 12 | 23.67 | 3.22 | 25.00 | 3.08 | 0.37 | 0.55 | 0.02 |
| DTC | 10 | 22.30 | 5.33 | 24.70 | 4.37 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumura, N.; Fujino, H.; Yamamoto, T.; Tanida, Y.; Ishii, A.; Tatsumi, A.; Nakanishi, M.; Tachibana, M.; Mohri, I.; Okuno, H. Effectiveness of a Parent Training Programme for Parents of Adolescents with Autism Spectrum Disorders: Aiming to Improve Daily Living Skills. Int. J. Environ. Res. Public Health 2022, 19, 2363. https://doi.org/10.3390/ijerph19042363
Matsumura N, Fujino H, Yamamoto T, Tanida Y, Ishii A, Tatsumi A, Nakanishi M, Tachibana M, Mohri I, Okuno H. Effectiveness of a Parent Training Programme for Parents of Adolescents with Autism Spectrum Disorders: Aiming to Improve Daily Living Skills. International Journal of Environmental Research and Public Health. 2022; 19(4):2363. https://doi.org/10.3390/ijerph19042363
Chicago/Turabian StyleMatsumura, Nanako, Haruo Fujino, Tomoka Yamamoto, Yuki Tanida, Atsuko Ishii, Aika Tatsumi, Mariko Nakanishi, Masaya Tachibana, Ikuko Mohri, and Hiroko Okuno. 2022. "Effectiveness of a Parent Training Programme for Parents of Adolescents with Autism Spectrum Disorders: Aiming to Improve Daily Living Skills" International Journal of Environmental Research and Public Health 19, no. 4: 2363. https://doi.org/10.3390/ijerph19042363
APA StyleMatsumura, N., Fujino, H., Yamamoto, T., Tanida, Y., Ishii, A., Tatsumi, A., Nakanishi, M., Tachibana, M., Mohri, I., & Okuno, H. (2022). Effectiveness of a Parent Training Programme for Parents of Adolescents with Autism Spectrum Disorders: Aiming to Improve Daily Living Skills. International Journal of Environmental Research and Public Health, 19(4), 2363. https://doi.org/10.3390/ijerph19042363