
Risk of Fall-Related Injuries Associated with Antidepressant Use in Elderly Patients: A Nationwide Matched Cohort Study

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
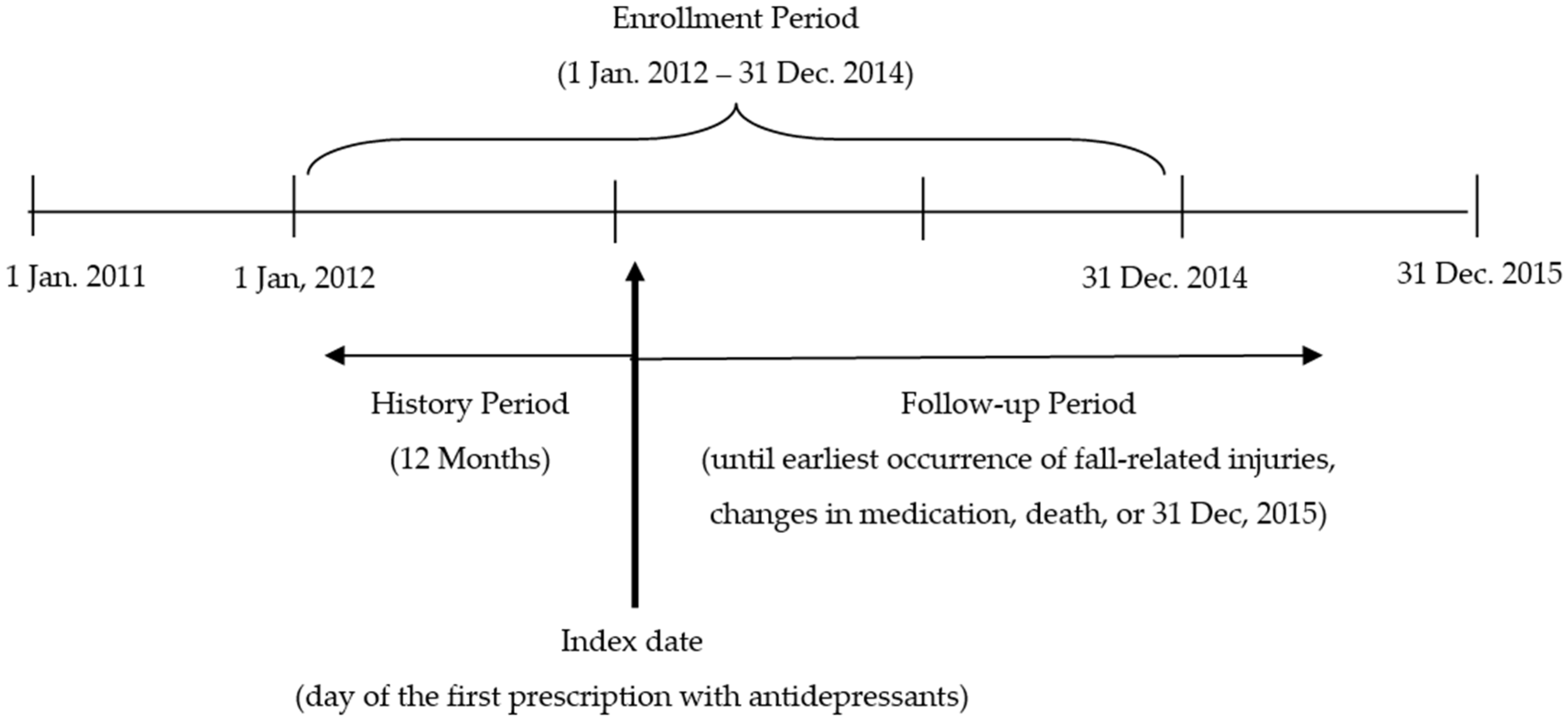
2.1. Study Design and Data Sources
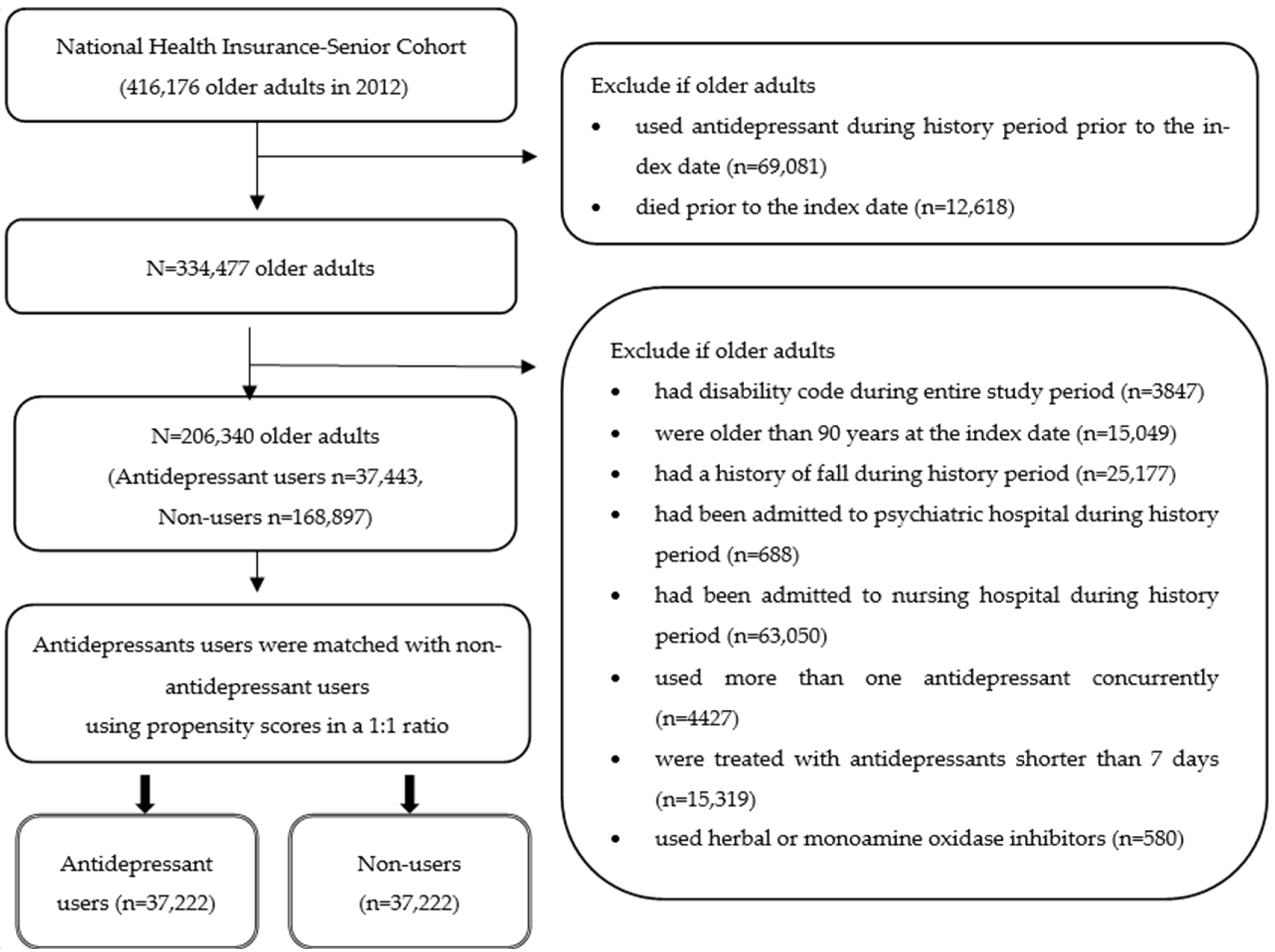
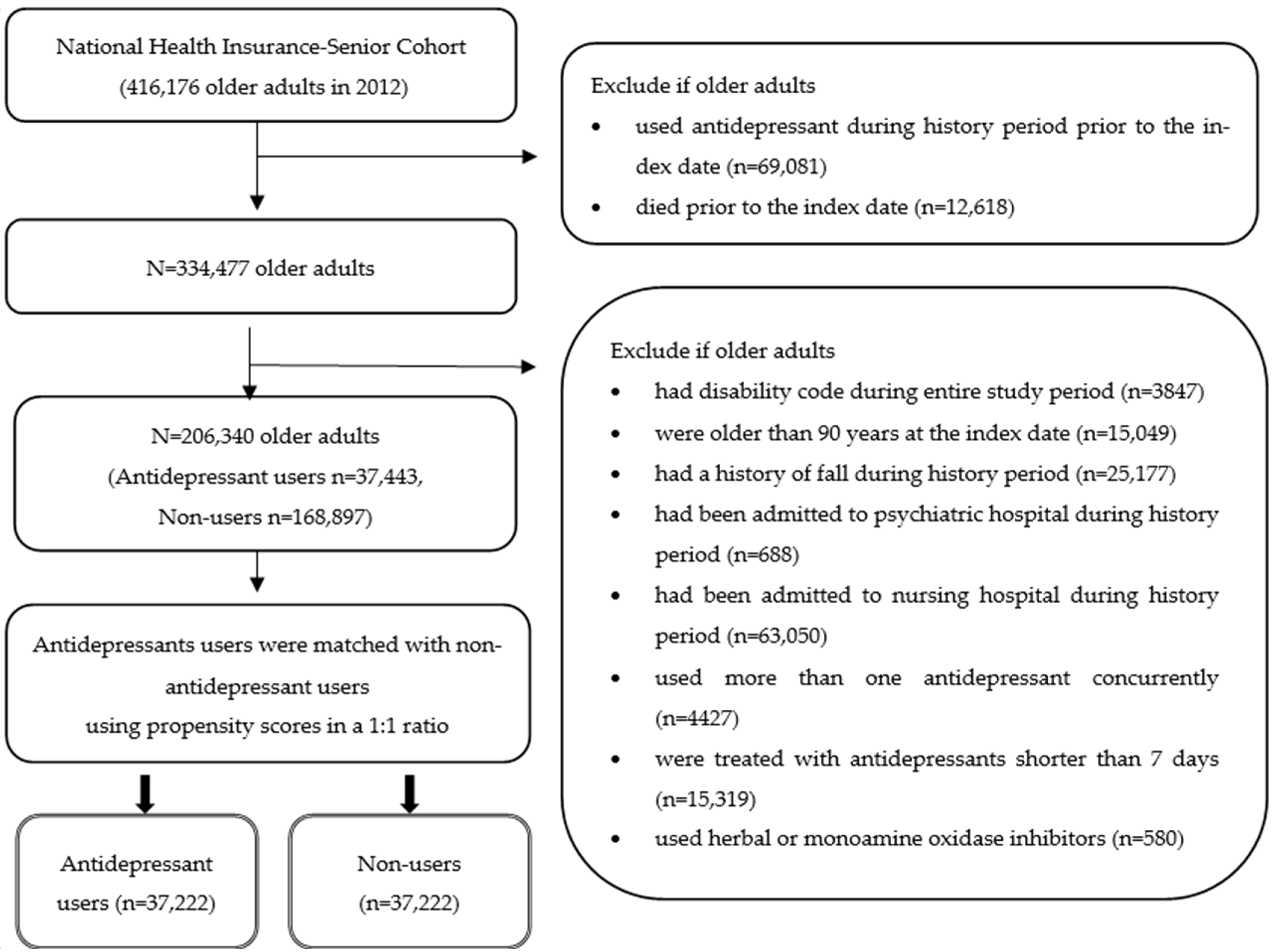
2.2. Study Population
2.3. Definition of Fall-Related Injuries
2.4. Exposure to Medications
2.5. Covariates: Demographics, Health Service Utilization, and Comorbidities
2.6. Data Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kovich, H.; Dejong, A. Common questions about the pharmacologic managmenet of depression in adults. Am. Fam. Physician 2015, 92, 94–100. [Google Scholar] [PubMed]
- Dipiro, J.; Gary, C.; Poset, L.; Haines, S.; Nolin, T.; Ellingrod, V. Pharmacotherapy: A Pathophysiologic Approach, 11th ed.; McGraw-Hill: Columbus, OH, USA, 2020. [Google Scholar]
- Wang, H.; Bahk, W.; Seo, J.; Woo, Y.; Park, Y.; Jeong, J.; Kim, W.; Shim, S.; Lee, J.; Jon, D.; et al. Korean Medication Algorithm for Depressive Disorder: Comparisons with Other Treatment Guidelines. Clin. Psychopharmacol. Neurosci. 2017, 15, 199–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilal-Dandan, R.; Brunton, L. Goodman and Gilman’s Manual of Pharmacology and Therapeutics, 2nd ed.; McGraw-Hill: Columbus, OH, USA, 2014. [Google Scholar]
- Marcum, Z.A.; Perera, S.; Thorpe, J.M.; Switzer, G.E.; Castle, N.G.; Strotmeyer, E.S.; Simonsick, E.M.; Ayonayon, H.N.; Philips, C.L. Antidepressant use and recurrent falls in community-dwelling older adults: Findings from the health ABC study. Ann. Pharm. 2016, 50, 523–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coupland, C.; Dhiman, P.; Morriss, R.; Arthur, A.; Barton, G.; Hippisley-Cox, J. Antidepressant use and risk of adverse outcomes in older people: Population based cohort study. BMJ 2011, 343, d4551. [Google Scholar] [CrossRef] [Green Version]
- Tamblyn, R.; Bates, D.; Buckeridge, D.; Dixon, W.; Girard, N.; Haas, J.; Habib, B.; Iqbal, U.; Li, J.; Sheppard, T. Multinational investigation of fracture risk with antidepressant use by class, drug, and indication. J. Am. Geriatr. Soc. 2020, 68, 1494–1503. [Google Scholar] [CrossRef]
- Marci, J.; Iaboni, A.; Kirham, J.; Maxwell, C.; Gill, S.; Vasudev, A.; Whitehead, M.; Seitz, D. Association between Antidepressants and Fall-Related Injuries among Long-Term Care Residents. Am. J. Geriatr. Psychatiry 2017, 25, 1326–1336. [Google Scholar]
- Gagne, J.; Patrick, A.; Mogun, H.; Solomon, D. Antidepressants and Fracture Risk in Older Adults: A Comparative Safety Analysis. Clin. Pharmacol. Ther. 2011, 89, 880–887. [Google Scholar] [CrossRef] [Green Version]
- Dahl, M.; Leander, K.; Vikstrom, M.; Frumerie, C.; Nordenmalm, S.; Moller, J.; Soderberg-Lofdal, K. CYP2D6 inhibiting drugs and risk of fall injuries after newly initiated antidepressant and antipsychotic therapy in a Swedish, register-based case-crossover study. Sci. Rep. 2021, 11, 5796. [Google Scholar] [CrossRef]
- Parker, M.; Moffet, H.; Adams, A.; Karter, A. An algorithm to identify medication nonpersistence using electronic pharmacy databases. J. Am. Med. Inform. Assoc. 2015, 22, 957–961. [Google Scholar] [CrossRef] [Green Version]
- Gardarsdottier, H.; Souverein, P.; Egbert, T.; Heerdink, E. Construction of drug treatment episodes from drug-dispensing histories is influenced by the gap length. J. Clin. Epidemiol. 2010, 23, 422–427. [Google Scholar] [CrossRef]
- Kim, Y.I.; Kim, Y.Y.; Yoon, J.L.; Won, C.W.; Ha, S.J.; Cho, K.D.; Park, B.R.; Bae, S.J.; Lee, E.J. Cohort profile: National health insurance service-senior (NHIS-senior) cohort in Korea. BMJ Open 2019, 9, e024344. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, A.; Formiga, F.; Plana-Ripoll, O.; Tobella, M.; Gil, A.; Pujol, R. Risk of falls in 85-year-olds is associated with functional and cognitive status: The Octabaix study. Arch. Gerontol. Geriatr. 2012, 54, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Moncada, L.V.V.; Mire, L.G. Preventing falls in older persons. Am. Fam. Physician 2017, 96, 240–247. [Google Scholar]
- Tinetti, M.E.; Speechley, M. Prevention of falls among the elderly. N. Engl. J. Med. 1989, 320, 1055–1059. [Google Scholar] [PubMed]
- Austin, P. Optimal caliper widths for propensity-score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Statist. 2011, 10, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.B.; Zingmond, D.S.; Keeler, E.B.; Jennings, L.A.; Wenger, N.S.; Reuben, D.B.; Ganz, D.A. Development of an algorithm to identify fall-related injuries and costs in Medicare data. Inj. Epidemiol. 2016, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.; Han, L.; Lee, D.S.; McAvay, G.J.; Peduzzi, P.; Gross, C.P.; Zhou, B.; Lin, H. Antihypertensive medications and serious fall injuries in a nationally representative sample of older adults. JAMA Intern. Med. 2014, 174, 588–595. [Google Scholar] [CrossRef]
- Lee, Y.G.; Kim, S.C.; Chang, M.S.; Nam, E.W.; Kim, S.G.; Cho, S.I. Complications and socioeconomic costs associated with falls in the elderly population. Ann. Rehabil. Med. 2018, 42, 120–129. [Google Scholar] [CrossRef] [Green Version]
- WHO Collaborating Centre for Drug Statistics Methodology. ATC Classification Index with DDDs. Available online: https://www.whocc.no/atc/structure_and_principles/ (accessed on 15 March 2021).
- Korea Pharmaceutical Information Center. KPIC Therapeutic Classification. Available online: https://www.health.kr/searchIngredient/KPICeffect.asp (accessed on 11 November 2021).
- American Geriatric Society Beers Criteria Update Expert Panel. American Geriatric Society 2019 updated AGS Beers criteria for potentially inappropriate medications use in older adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar]
- Aspinall, S.; Springer, S.; Zhao, X.; Cunningham, F.; Thrope, C.; Semla, T.; Shorr, R.; Hanlon, J. Central Nervous System Medication Burden and Risk of Recurrent Serious Falls and Hip Fractures in Veterans Affairs Nursing Home Residents. JAGS 2019, 67, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.A.; Shin, J.Y.; Park, B.J. Prevalence and predictors of polypharmacy among Korean elderly. PLoS ONE 2014, 9, e98043. [Google Scholar] [CrossRef] [PubMed]
- American Geriatrics Society; British Geriatrics Society; American Academy of Orthopaedic Surgeons Panel on Falls Prevention. Guideline for the prevention of falls in older persons. J. Am. Geriatr. Soc. 2001, 49, 664–672. [Google Scholar] [CrossRef]
- Mamdani, M.; Sykora, K.; Li, P.; Normand, S.L.T.; Streiner, D.L.; Austin, P.C.; Rochon, P.A.; Anderson, G.M. Reader’s guide to critical appraisal of cohort studies: 2. Assessing potential for confounding. BMJ 2005, 330, 960–962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, P. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Statist. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Zhuo, M.; Hawley, C.E.; Paik, J.M.; Bessette, L.G.; Wexler, D.J.; Kim, D.H.; Tong, A.Y.; Kim, S.C.; Patorno, E. Association of Sodium-Glucose Cotransporter–2 Inhibitors with Fracture Risk in Older Adults with Type 2 Diabetes. JAMA Netw. Open 2021, 4, e2130762. [Google Scholar] [CrossRef]
- Hwang, J.; Song, I.; Lee, E.; Ha, D.; Shin, J. Prevalence and predidctors of tricyclic antidepressant use among elderly Koreans in primary-care and specialty clincs. Int. J. Clin. Pharmacol. Ther. 2018, 56, 224–230. [Google Scholar] [CrossRef]
- Hanlon, J.; Zhao, X.; Naples, J.; Aspinall, S.; Perera, S.; Nace, D.; Castle, N.; Greenspan, S.; Thrope, C. Central Nervous System Medication Burden and Serious Falls in Older Nursing Home Residents. JAGS 2017, 65, 1183–1189. [Google Scholar] [CrossRef]
- Pratt, N.; Ramsay, E.; Ellet, L.; Nguyen, T.; Barrat, J.; Roughead, E. Association between Use of Multiple Psychoactive Medicines and Hospitalization for Falls: Retrospective Analysis of a Large Healthcare Claim Database. Drug Saf. 2014, 37, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.; Taylor-Rowan, M.; Soiza, R.L.; Quinn, T.J.; Loke, Y.K.; Myint, P.K. Anticholinergic burden measures and older people’s falls risk: A systematic prognostic review. Ther. Adv. Drug Saf. 2021, 12. [Google Scholar] [CrossRef]
- de Vries, M.; Seppala, L.J.; Daams, J.G.; van de Glind, E.M.M.; Masud, T.; van der Velde, N.; EUGM Task and Finish Group on Fall-Risk-Increasing Drugs. Fall-risk-increasing drugs: A systematic review and meta-analysis: I. cardiovascular drugs. J. Am. Med. Dir. Assoc. 2018, 19, 371.e1–371.e9. [Google Scholar] [CrossRef] [Green Version]
- Figueroa, J.J.; Basford, J.R.; Low, P.A. Preventing and treating orthostatic hypotension: As easy as A, B, C. Clevel. Clin. J. Med. 2010, 77, 298–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcum, Z.A.; Perera, S.; Newman, A.B.; Thorpe, J.M.; Switzer, G.E.; Gray, S.L.; Simonsick, E.M.; Shorr, R.I. Antihypertensive use and recurrent falls in community-dwelling older adults: Findings from the health ABC study. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1562–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seppala, L.J.; Wermelink, A.M.A.T.; de Vries, M.; Ploegmakers, K.J.; van de Glind, E.M.M.; Daams, J.G.; van der Velde, N.; EUGMS Task and Finish Group on Fall-Risk-Increasing Drugs. Fall-risk-increasing drugs: A systematic review and meta-analysis: II. psychotropics. J. Am. Med. Dir. Assoc. 2018, 19, e311–e371. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health & Welfare—Korea Suicide Prevention Center. Suicide Prevention Wite Book; Korea Suicide Prevention Center: Seoul, Korea, 2020.
- Health Insurance Review &Assessment Service. Detailed Criteria and Methods for Reimbursement of Medicaal Service (Drugs) and Its Evaluation Guidelines (Yoyang Geugyeo Jekyong Kijoon and Bangbub Sebu Sahang); G000J67-2017-67; Health Insurance Review & Assessment Service: Wonju, Korea, 2017; pp. 1–550.
- Wong, J.; Montulsky, A.; Eaguale, T.; Buckeridge, D.; Brahamowicz, M.; Tamblyn, R. Treatment Indications for Antidepressants Prescribed in Primary Care in Quebec, Canada, 2006–2015. JAMA 2016, 315, 2230–2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Kim, W.; Jang, T. Opioids and Antidepressants for Pain Control in Musculoskeletal Disease. J. Korean Orthop. Assoc. 2020, 55, 1–8. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Antidepressant Users (n = 37,222) | Matched Non-Users (n = 37,222) | Standardized Difference | |
|---|---|---|---|
| N (%) | N (%) | ||
| Demographics | |||
| Age, mean (±SD) | 76.7 (±4.5) | 76.7 (±4.5) | |
| 70–79 | 27,733 (74.5) | 27,770 (74.6) | 0.00 |
| 80–89 | 9489 (25.5) | 9452 (25.4) | |
| Income | |||
| 0–2nd quintile | 11,722 (31.5) | 11,517 (30.9) | 0.01 |
| 3–4th quintile | 10,499 (28.2) | 10,447 (28.1) | 0.00 |
| 5–10th quintile | 15,001 (40.3) | 15,258 (41.0) | 0.01 |
| Female | 22,691 (61.0) | 22,691 (61.0) | 0.00 |
| Metropolitan a | 13,925 (37.4) | 13,811 (37.1) | 0.01 |
| Health Service Utilization | |||
| Hospitalization b | 4554 (12.2) | 4297 (11.5) | 0.02 |
| No. of outpatient visits b | |||
| 0–7 | 16,508 (44.4) | 16,183 (43.5) | 0.02 |
| ≥8 | 20,714 (55.6) | 21,039 (56.5) | |
| Comorbidities | |||
| OA/RA | 19,920 (53.5) | 20,070 (53.9) | 0.01 |
| Malignant neoplasm | 3157 (8.5) | 3042 (8.2) | 0.01 |
| Cardiovascular diseases | 9760 (26.2) | 9739 (26.2) | 0.00 |
| Thyroid diseases | 5240 (14.1) | 4901 (13.2) | 0.03 |
| Hypertension | 25,514 (68.5) | 25,607 (68.8) | 0.01 |
| Osteoporosis | 10,588 (28.4) | 10,440 (28.0) | 0.01 |
| Neurologic diseases | 9459 (25.4) | 9213 (24.8) | 0.02 |
| Gastric ulcers | 13,150 (35.3) | 13,192 (35.4) | 0.00 |
| Antidepressant Users | TCAs (n = 16,127) N (%) | SSRIs (n = 5621) N (%) | SSREs (n = 9401) N (%) | SNRIs (n = 3146) N (%) | Trazodone (n = 2290) N (%) |
|---|---|---|---|---|---|
| No. of total medications, mean (±SD) | 12.5 (±7.7) | 11.9 (±8.7) | 12.6 (±7.4) | 13.0 (±8.0) | 13.0 (±10.1) |
| 0–10 | 7634 (47.3) | 3079 (54.8) | 4329 (46.1) | 1445 (45.9) | 1167 (51.0) |
| >10 | 8493 (52.7) | 2542 (45.2) | 5072 (54.0) | 1701 (54.1) | 1123 (49.0) |
| No. of CNS medications, mean (±SD) | 2.1 (±0.9) | 2.1 (±0.9) | 1.8 (±0.8) | 1.9 (±0.9) | 2.3 (±1.0) |
| 0 | 4885 (30.3) | 1661 (29.6) | 3825 (40.7) | 1195 (38.0) | 513 (22.4) |
| 1 | 6592 (40.9) | 2328 (41.4) | 3743 (39.8) | 1252 (39.8) | 920 (40.2) |
| ≥2 | 4650 (28.8) | 1632 (29.0) | 1833 (19.5) | 699 (22.2) | 857 (37.4) |
| Therapeutic classes of medications (except for CNS classes) | |||||
| Anti-inflammatories and antirheumatics | 9146 (56.7) | 1772 (31.5) | 4788 (50.9) | 2167 (68.9) | 847 (37.0) |
| Calcium channel blockers | 6415 (39.8) | 2172 (38.6) | 3567 (37.9) | 1274 (40.5) | 943 (41.2) |
| Antithrombotic agents | 6464 (40.1) | 2530 (45.0) | 3499 (37.2) | 1335 (42.4) | 1013 (44.2) |
| Angiotensin II antagonists | 2703 (16.8) | 999 (17.8) | 1553 (16.5) | 570 (18.1) | 438 (19.1) |
| H2-receptor antagonists | 7086 (43.9) | 1852 (33.0) | 4467 (47.5) | 1423 (45.2) | 769 (33.6) |
| Lipid modifying agents | 4653 (28.9) | 1818 (32.3) | 2592 (27.6) | 1049 (33.3) | 662 (28.9) |
| Drugs used for diabetes | 3515 (21.8) | 1199 (21.3) | 1753 (18.7) | 833 (26.5) | 498 (21.8) |
| Cough and cold preparations | 2871 (17.8) | 1128 (20.1) | 1780 (18.9) | 583 (18.5) | 553 (24.2) |
| Antihistamines for systemic use | 3186 (19.8) | 912 (16.2) | 1750 (18.6) | 522 (16.6) | 471 (20.6) |
| CNS medications | |||||
| Opioids | 6445 (40.0) | 1121 (19.9) | 3089 (32.9) | 1350 (42.9) | 512 (22.4) |
| Antiepileptics | 3152 (19.5) | 593 (10.6) | 684 (7.3) | 418 (13.3) | 272 (11.9) |
| Antipsychotics | 413 (2.6) | 614 (10.9) | 126 (1.3) | 74 (2.4) | 317 (13.8) |
| Anxiolytics | 5651 (35.0) | 2919 (51.9) | 3085 (32.8) | 732 (23.3) | 1137 (49.7) |
| Hypnotics and sedatives | 1474 (9.1) | 846 (15.1) | 803 (8.5) | 219 (7.0) | 721 (31.5) |
| DDD prescribed, mean (±SD) | 0.25 (±0.16) | 0.82 (±0.37) | 0.75 (±0.24) | 0.57 (±0.22) | 0.15 (±0.09) |
| >0–≤0.5 DDD | 14,974 (92.9) | 2049 (36.5) | 1513 (16.1) | 2430 (77.2) | 2278 (99.5) |
| >0.5–≤1.0 DDD | 1125 (7.0) | 3019 (53.7) | 7844 (83.4) | 681 (21.7) | 12 (0.5) |
| >1.0 DDD | 28 (0.2) | 553 (9.8) | 44 (0.5) | 35 (1.1) | 0 (0) |
| Fall-Related Injuries (FRIs) | ||||||
|---|---|---|---|---|---|---|
| No. of Patients | Person Years (PYs) | No. of FRIs | Incidence/ 1000 PYs * | Crude HR (95% CI) | Adjusted HR (95% CI) ** | |
| Age | ||||||
| 70–79 | 55,503 | 12,546.0 | 976 | 77.8 | Reference | Reference |
| 80–89 | 18,941 | 4722.9 | 490 | 103.8 | 1.41 (1.25–1.58) | 1.36 (1.21–1.53) |
| Female | 45,382 | 10,367.6 | 998 | 96.3 | 1.35 (1.20–1.52) | 1.37 (1.19–1.58) |
| Antidepressants | ||||||
| All | 37,222 | 8797.5 | 978 | 111.2 | 1.25 (1.09–1.44) | 1.30 (1.13–1.50) |
| By Class of Antidepressant | ||||||
| SNRIs | ||||||
| All | 3146 | 759.9 | 102 | 134.2 | 1.48 (1.18–1.87) | 1.54 (1.21–1.92) |
| Duloxetine | 2623 | 606.3 | 86 | 141.8 | 1.55 (1.21–1.98) | 1.59 (1.24–2.03) |
| Milnacipran | 351 | 106.8 | 11 | 103 | 1.19 (0.65–2.19) | 1.23 (0.67–2.25) |
| SSREs | ||||||
| All | 9401 | 1582.6 | 175 | 110.6 | 1.19 (0.98–1.45) | 1.20 (0.99–1.46) |
| Tianeptine | 9401 | 1582.6 | 175 | 110.6 | 1.19 (0.98–1.45) | 1.20 (0.99–1.46) |
| SSRIs | ||||||
| All | 5621 | 2050.1 | 234 | 114.1 | 1.34 (1.12–1.60) | 1.42 (1.19–1.71) |
| Escitalopram | 3573 | 1397.6 | 160 | 114.5 | 1.35 (1.11–1.65) | 1.43 (1.17–1.75) |
| Sertraline | 657 | 228.1 | 26 | 114 | 1.33 (0.89–1.99) | 1.44 (0.96–2.17) |
| Paroxetine | 643 | 225.1 | 31 | 137.7 | 1.62 (1.12–2.36) | 1.71 (1.18–2.49) |
| Fluoxetine | 583 | 129.5 | 11 | 84.9 | 0.95 (0.52–1.74) | 0.99 (0.54–1.81) |
| TCAs | ||||||
| All | 5621 | 2050.1 | 234 | 114.1 | 1.15 (0.98–1.36) | 1.21 (1.03–1.42) |
| Amitriptyline | 3573 | 1397.6 | 160 | 114.5 | 1.19 (1.00–1.42) | 1.23 (1.03–1.46) |
| Nortriptyline | 657 | 228.1 | 26 | 114 | 0.98 (0.75–1.29) | 1.03 (0.78–1.35) |
| Imipramine | 643 | 225.1 | 31 | 137.7 | 1.27 (0.91–1.77) | 1.50 (1.07–2.11) |
| Other | ||||||
| All | 2927 | 788.3 | 96 | 121.8 | 1.39 (1.10–1.77) | 1.47 (1.16–1.86) |
| Trazodone | 2290 | 589.6 | 75 | 127.2 | 1.45 (1.12–1.88) | 1.51 (1.17–1.96) |
| Mirtazapine | 443 | 123.2 | 16 | 129.8 | 1.49 (0.90–2.46) | 1.58 (0.95–2.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.-S.; Suh, D.; Choi, H.-S.; Park, H.-D.; Jung, S.-Y.; Suh, D.-C. Risk of Fall-Related Injuries Associated with Antidepressant Use in Elderly Patients: A Nationwide Matched Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 2298. https://doi.org/10.3390/ijerph19042298
Jung Y-S, Suh D, Choi H-S, Park H-D, Jung S-Y, Suh D-C. Risk of Fall-Related Injuries Associated with Antidepressant Use in Elderly Patients: A Nationwide Matched Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2298. https://doi.org/10.3390/ijerph19042298
Chicago/Turabian StyleJung, Yu-Seon, David Suh, Hang-Seok Choi, Hee-Deok Park, Sun-Young Jung, and Dong-Churl Suh. 2022. "Risk of Fall-Related Injuries Associated with Antidepressant Use in Elderly Patients: A Nationwide Matched Cohort Study" International Journal of Environmental Research and Public Health 19, no. 4: 2298. https://doi.org/10.3390/ijerph19042298
APA StyleJung, Y.-S., Suh, D., Choi, H.-S., Park, H.-D., Jung, S.-Y., & Suh, D.-C. (2022). Risk of Fall-Related Injuries Associated with Antidepressant Use in Elderly Patients: A Nationwide Matched Cohort Study. International Journal of Environmental Research and Public Health, 19(4), 2298. https://doi.org/10.3390/ijerph19042298