
Coexisting with the Life of Patients with Hemodialysis: Qualitative Meta-Synthesis Study of Life of Caregivers of Patients with Hemodialysis

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Collection Method
2.2.1. Literature Research and Selection
2.2.2. Quality Appraisal
2.3. Data Analysis and Synthesis
3. Results
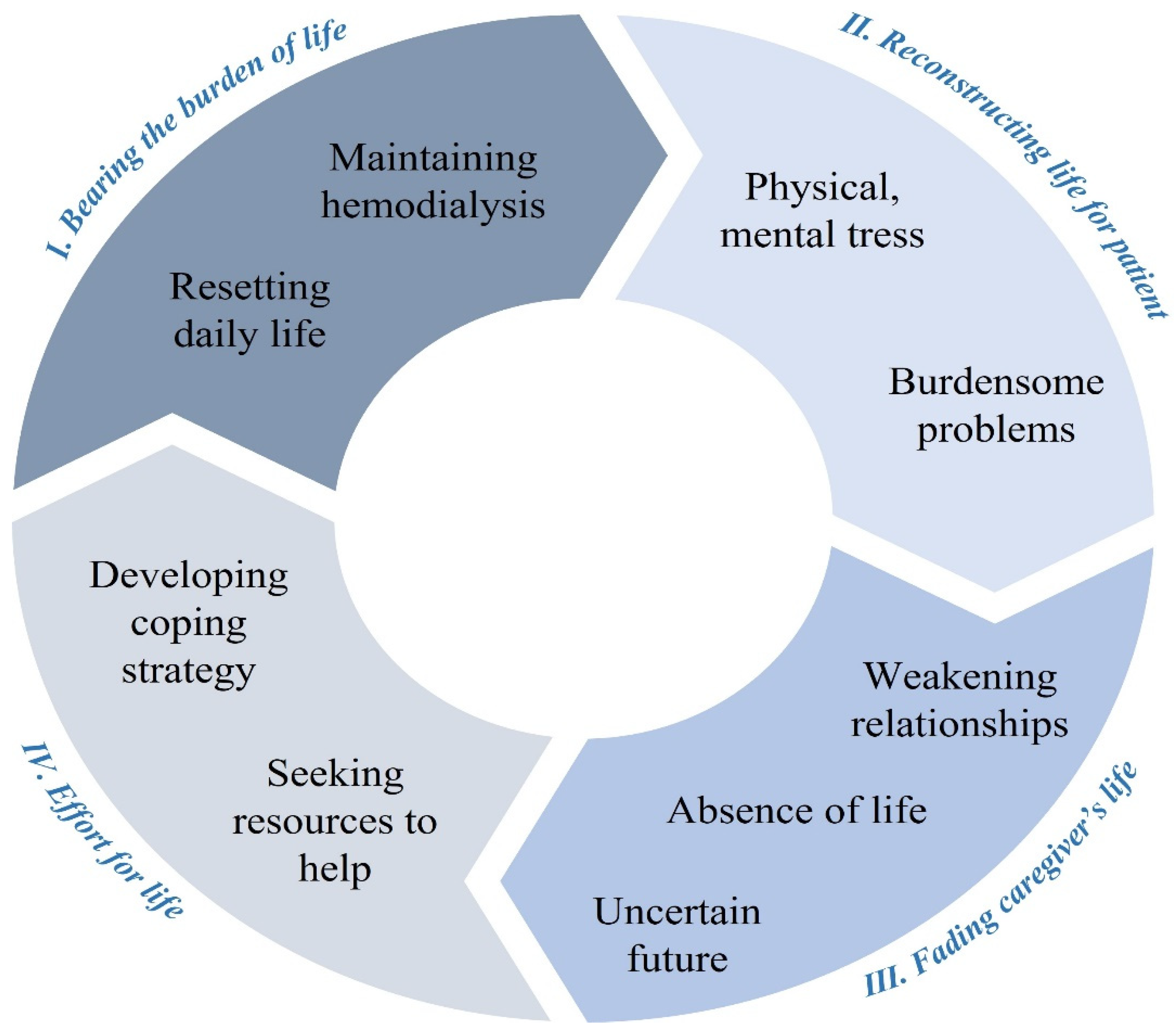
3.1. Theme Ⅰ. Bearing the Burden of Life as a Caregiver
3.1.1. Sub-Theme 1. Facing a Variety of Burdensome Problems
“The difficulty only when … like she cannot get up, have to carry her … Ya, to carry her, to bathe her.” (21, p.1227)
“Haha I know this is easier said than done … money is a very important thing. It will affect everything in our lives. Plus the fact that this is quite an expensive disease. I can only say as someone at the consumer end, more money is better” (21, p.1228)
“These patients have lots of difficulties and miseries such as transfer to the hemodialysis ward, doing household tasks, handling the patient’s bad temper, suffering from insomnia and so on. What should I say? They all affect the caregivers’ soul and mind so that I am willing to die.” (23, p.196)
3.1.2. Sub-Theme 2. Living an Unstable Life between Physical and Mental Stress
“Those are the days [when patient undergoes fistula de-clot at the hospital followed by dialysis at the clinic] that are really tiring. Those are the days that I just pray that she makes it through and she keeps her head up. I try to motivate her to keep her spirit up as well as mine.” (19, p.1365)
“It’s the many restrictions that make diet hard to follow. And sometimes, a news report may say that for example, avocado or bananas are good for people with diabetes. But she cannot eat it because of the calories and potassium? Yeah. I may be wrong, but my experience is that so many foods are difficult to follow. Actually, I’m not sure which (i.e., diabetes vs. ESRD) diet matters and has an impact.” (21, p.1227)
3.2. Theme Ⅱ. Reconstructing Life to Maintain Hemodialysis
3.2.1. Sub-Theme 3. Efforts at Home to Maintain Steady Hemodialysis
“I must take care of the fistula on her hand. She should take her medications on time. She needs to drink a little water and not consume certain foods. In sum, I am always mentally engaged, and I always think about the things that she should or should not have and whether there is pressure on the fistula of her hand?” (26, p.256)
“After some sessions, he gained weight, so his nurse asked why he has not observed the water restriction. Well, summer is hot, and my child becomes thirsty. What can I do? How can I tell him not to drink water? I am his mother.“ (27, e23)
3.2.2. Sub-Theme 4. Resetting Daily Life around the Patient
“... In hard conditions of caretaking, both planning and prioritization are important to me, that is, (to decide) which job is more important and valuable for my wife. In this way, the caring plan proceeds more comfortably and I’m more satisfied, as well...” (20, p.167)
“... His condition may get worse and time is gold for us. For this reason, I’ve written down all his requirements and planned and really coordinated all the jobs I do for him...” (20, p.167)
3.3. Theme Ⅲ. The Fading of Caregiver’s Own Life
3.3.1. Sub-Theme 5. Absence of the Caregiver’s Own Life
“I was the only one that really cared for her and I’ve been helping her. I really care for her; I don’t want nothing to happen to her. There’s nothing to do but to help her. “ (19, p.1366)
“She didn’t go for dialysis and she’s at home, my mind is not at peace at work also. I’m afraid ‘cause she’s alone. For me, looking after someone who’s sick comes with a lot of problems. Want to go out is a problem. ‘Cause as caregivers, when we’re out our minds are not at peace too. We’ll be thinking… scared if my wife falls, scared she’s that” (21, p.1231)
3.3.2. Sub-Theme 6. Weakening of Relationships around Caregivers
“My wife is on dialysis for about 5 years. In the first and second years, we had approximately no problems. But this disease destroys the dialysis person’s sexual feelings and severely affects the patient’s spouse, while underlying nervous tensions.” (23, p.196)
“I come here and sit for four hours. No one speaks with me. Nurses only connect the machine to my child without asking, ‘Are you okay?’ I like having someone to speak” (27, p.e22)
3.3.3. Sub-Theme 7. Anxiety from an Uncertain Future
“Cause like me, I got no maid, so I have to sacrifice my job. I have to stop my job for 7 years and take care of my mother.” (21, p.1230)
“The patient’s care process is lengthy. The caregiver should get up at 6 am in the morning and take the patient to a dialysis ward. He/she should spend 3–4 h over the patient’s bed in the hemodialysis ward. When the patient comes back home, the caregiver should massage his/her legs for half an hour and check whether he/she has any bleeding. This process is repeated three times a week. I certainly assert that caregivers are permanently getting involved in the process of care.” (23, p.197)
“That’s the hardest part, how to plan for the future… Caring for someone who has cared for you; that’s the biggest transition.” (28, p.29)
3.4. Theme Ⅳ. Effort to Relieve the Burden
3.4.1. Sub-Theme 8. Developing Coping Strategies
“... Everyday I’m [searching] on the internet and in books to learn something new and to be able to overcome the problems rather than allow them to defeat me...” (20, p.165)
“I kick box for one thing…hitting and kicking something as hard as you can helps a whole lot to deal with the frustration.”, “Now I get on the treadmill and run for 25 to 30 min. It feels great.” (28, p.29)
3.4.2. Sub-Theme 9. Seeking Help to Reduce the Burden on Themselves
“... In these times, if you don’t shout, no one will come to help you. You should always say what you’re doing so that others will come to help you. At home, in the family and in the community...” (20, p.165)
“Your love and your innate beliefs do not tell you that the patient is your mother, father, brother or spouse, but it is your innate belief and love that make you serve them with all your heart without ever tiring. I believe that such service is a belief and a value, and I greatly respect it.” (22, p.86)
3.5. Third-Order Synthesis: Understanding the Experiences of Caregivers Caring for Hemodialysis Patients
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, B.; Wulf, S.; Bikbov, B.; Perico, N.; Cortinovis, M.; De Vaccaro, K.C.; Flaxman, A.; Peterson, H.; Delossantos, A.; Haring, D. Maintenance dialysis throughout the world in years 1990 and 2010. J. Am. Soc. Nephrol. 2015, 26, 2621–2633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gayomali, C.; Sutherland, S.; Finkelstein, F.O. The challenge for the caregiver of the patient with chronic kidney disease. Nephrol. Dial. Transplant. 2008, 23, 3749–3751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, R.A. Chronic renal failure: Assessing the Fatigue Severity Scale for use among caregivers. J. Clin. Nurs. 2004, 13, 219–225. [Google Scholar] [CrossRef]
- Tong, A.; Lowe, A.; Sainsbury, P.; Craig, J.C. Parental perspectives on caring for a child with chronic kidney disease: An in-depth interview study. Child Care Health Dev. 2010, 36, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Alnazly, E. Coping strategies and socio-demographic characteristics among Jordanian caregivers of patients receiving hemodialysis. Saudi. J. Kidney Dis. Transpl. 2016, 27, 101. [Google Scholar] [CrossRef] [PubMed]
- Rak, E.C.; Hooper, S.R.; Belsante, M.J.; Burnett, O.; Layton, B.; Tauer, D.; Mantoo, B.; DeWalt, D.; Ferris, M.E. Caregiver word reading literacy and health outcomes among children treated in a pediatric nephrology practice. Clin. Kidney J. 2016, 9, 510–515. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J.C. Support interventions for caregivers of people with chronic kidney disease: A systematic review. Nephrol. Dial. Transplant. 2008, 23, 3960–3965. [Google Scholar] [CrossRef] [Green Version]
- Belasco, A.; Barbosa, D.; Bettencourt, A.R.; Diccini, S.; Sesso, R. Quality of life of family caregivers of elderly patients on hemodialysis and peritoneal dialysis. Am. J. Kidney Dis. 2006, 48, 955–963. [Google Scholar] [CrossRef]
- Noble, H.; Kelly, D.; Hudson, P. Experiences of carers supporting dying renal patients managed without dialysis. J. Adv. Nurs. 2013, 69, 1829–1839. [Google Scholar] [CrossRef]
- Affinito, J.; Louie, K. Positive Coping and Self-Assessed Levels of Health and Burden in Unpaid Caregivers of Patients with End Stage Renal Disease Receiving Hemodialysis Therapy. Nephrol. Nurs. J. 2018, 45, 373–379. [Google Scholar]
- Holloway, I.; Galvin, K. Qualitative Research in Nursing and Healthcare; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Walsh, D.; Downe, S. Meta-synthesis method for qualitative research: A literature review. J. Ad. Nurs. 2005, 50, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Cheung, K.L.; Nair, S.S.; Tamura, M.K.; Craig, J.C.; Winkelmayer, W.C. Thematic synthesis of qualitative studies on patient and caregiver perspectives on end-of-life care in CKD. Am. J. Kidney Dis. 2014, 63, 913–927. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.C.; Hanson, C.S.; Palmer, S.C.; Howard, K.; Morton, R.L.; Marshall, M.R.; Tong, A. Patient and caregiver perspectives on home hemodialysis: A systematic review. Am. J. Kidney Dis. 2015, 65, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Pourghaznein, T.; Manzari, Z.S.; Heydari, A.; Mousavi Bazaz, M. Basic needs of mothers with children undergoing hemodialysis: A meta-synthesis of qualitative studies. Evid. Based Care 2019, 8, 14–25. [Google Scholar] [CrossRef]
- Tong, A.; Lowe, A.; Sainsbury, P.; Craig, J.C. Experiences of parents who have children with chronic kidney disease: A systematic review of qualitative studies. Pediatrics 2008, 121, 349–360. [Google Scholar] [CrossRef]
- Noblit, G.W.; Hare, R.D.; Hare, R.D. Meta-Ethnography: Synthesizing Qualitative Studies; Sage: Newcastle Upon Tyne, UK, 1988. [Google Scholar]
- Singh, J. Critical appraisal skills programme. J. Pharmacol. Pharmacother. 2013, 4, 76. Available online: http://www.jpharmacol.com/text/asp?2013/4/1/76/107697 (accessed on 20 December 2021). [CrossRef] [Green Version]
- Calvin, A.O.; Engebreston, J.C.; Sardual, S.A. Understanding of Advance care planning by family members of persons undergoing hemodialysis. West. J. Nurs. Res. 2014, 36, 1357–1373. [Google Scholar] [CrossRef]
- Lee, V.Y.W.; Seah, W.Y.; Kang, A.W.C.; Khoo, E.Y.H.; Mooppil, N.; Griva, K. Managing multiple chronic conditions in Singapore—Exploring the perspectives and experiences of family caregivers of patients with diabetes and end stage renal disease on haemodialysis. Psychol. Health 2016, 31, 1220–1236. [Google Scholar] [CrossRef]
- Salehi-Tali, S.; Ahmadi, F.; Zarea, K.; Fereidooni-Moghadam, M. Commitment to care: The most important coping strategies among family caregivers of patients undergoing haemodialysis. Scand. J. Caring Sci. 2018, 32, 82–91. [Google Scholar] [CrossRef]
- Salehitali, S.; Ahmadi, F.; Dehkordi, A.H.; Noorian, K.; Fereidooni-Moghadam, M.; Zarea, K. Progressive exhaustion: A qualitative study on the experiences of Iranian family caregivers regarding patients undergoing hemodialysis. Int. J. Nurs. Sci. 2018, 5, 193–200. [Google Scholar] [CrossRef]
- Sari, D.; Afiyanti, Y. Family experience in treating children with chronic renal failure undergoing hemodialysis therapy. Enferm. Clin. 2018, 28, 321–324. [Google Scholar] [CrossRef]
- Pourghaznein, T.; Heydari, A.; Manzari, Z.; ValizadehZare, N. “Immersion in an Ocean of Psychological Tension:” The voices of mothers with children undergoing hemodialysis. Iran J. Nurs. Midwifery Res. 2018, 23, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, A.; Sajadi, S.A.; Moradian, S.T.; Akbari, R. Suspended life pattern: A qualitative study on personal life among family caregivers of hemodialysis patients in Iran. Int. Q. Community Health Educ. 2018, 38, 225–232. [Google Scholar] [CrossRef]
- Turner, C.; Finch-Guthrie, P. Experiences of caregivers caring for a family member who is using hemodialysis. Nephrol. Nurs. J. 2020, 47, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Pourghaznein, T.; Heydari, A.; Manzari, Z.S. Iranian mothers’ experiences with children undergoing hemodialysis: A hermeneutic phenomenological study. J. Pediatr. Nurs. 2018, 42, e19–e25. [Google Scholar] [CrossRef]
- Eslami, A.A.; Rabiei, L.; Abedi, H.A.; Shirani, M.; Masoudi, R. Coping skills of Iranian family caregivers’ in caretaking of patients undergoing hemodialysis: A qualitative study. J. Ren. Care 2016, 42, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Chhetri, S.K.; Baral, R. Caregiver burden among caregivers of patient undergoing hemodialysis in tertiary care center: A descriptive cross-sectional study. JNMA J. Nepal Med. Assoc. 2020, 58, 148–152. [Google Scholar] [CrossRef]
- Alnazly, E.K. Burden and coping strategies among Jordanian caregivers of patients undergoing hemodialysis. Hemodial. Int. 2016, 20, 84–93. [Google Scholar] [CrossRef]
- Hazzan, A.A.; Ploeg, J.; Shannon, H.; Raina, P.; Oremus, M. Association between caregiver quality of life and the care provided to persons with Alzheimer’s disease: Protocol for a systematic review. Syst. Rev. 2013, 2, 17. [Google Scholar] [CrossRef] [Green Version]
- Al-Rawashdeh, S.; Alshraifeen, A.; Rababa, M.; Ashour, A. Hope predicted quality of life in dyads of community-dwelling patients receiving hemodialysis and their family caregivers. Qual. Life Res. 2020, 29, 81–89. [Google Scholar] [CrossRef]
- Mollaoğlu, M.; Kayataş, M.; Yürügen, B. Effects on caregiver burden of education related to home care in patients undergoing hemodialysis. Hemodial. Int. 2013, 17, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Shukri, M.; Mustofai, M.A.; Md Yasin, M.A.S.; Tuan Hadi, T.S. Burden, quality of life, anxiety, and depressive symptoms among caregivers of hemodialysis patients: The role of social support. Int. J. Psychiatry Med. 2020, 55, 397–407. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Article No. | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 |
|---|---|---|---|---|---|---|---|---|---|---|
| Items | ||||||||||
| 1. Was there a clear statement of the aims of the research? | Y | Y | Y | Y | Y | Y | Y | N | Y | Y |
| 2. Is a qualitative methodology appropriate? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 3. Was the research design appropriate to address the aims of the research? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 4. Was the recruitment strategy appropriate to the aims of the research? | Y | Y | Y | Y | N | Y | Y | Y | Y | Y |
| 5. Was the data collected in a way that addressed the research issue? | Y | N | N | Y | Y | Y | N | Y | Y | Y |
| 6. Has the relationship between researcher and participants been adequately considered? | N | N | Y | Y | Y | Y | N | Y | Y | N |
| 7. Have ethical issues been taken into consideration? | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| 8. Was the data analysis sufficiently rigorous? | N | Y | N | N | Y | Y | N | N | N | N |
| 9. Is there a clear statement of findings? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 10. Was this research valuable? | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| Percentage (%) | 80 | 80 | 80 | 90 | 90 | 90 | 60 | 80 | 90 | 80 |
| Article No. | Author, (Year) | Sample Size (M:F) | Methodology | Age Range (Years) | Care Period | Relationship | Data Collection | Data Analysis | Key Findings |
|---|---|---|---|---|---|---|---|---|---|
| 19 | Amy O. Calvin et al. (2014) | 18 | Qualitative descriptive design | 21–67 (Average: 42) | 3–16 years | Spouse (7), Adult children (7), Parent (1), Sibling (1), Niece (1), Daughter-in-law (1) | Semi-structured interview | Glaserian approach | The overarching construct identified was one of Protection. Family members protect patients by
|
| 20 | Ahmad Ali Eslami et al. (2016) | 20 (6:14) | Descriptive exploratory design | Average: 45 | Not reported | Spouse (8), Daughter (6), Others (4) | Unstructured interview | Thematic analysis |
|
| 21 | Vanessa Y.W. Lee, et al. (2016) | 20 (5:15) | Qualitative method | Average: 54.2 ± 12.6 | Average: 7.1 ± 5.3 years | Son (1), Husband (4), Wife (10), Daughter (4), Mother (1) | In-depth interview | Inductive thematic analysis |
|
| 22 | Shahriar Salehi-tali et al. (2018) | 16 (8:8) | Qualitative study | 25–70 (Average: 41.5) | 3–11 years (Average: 7.34 years) | Father (1), Mother (2), Spouse (4), Boy (2), Daughter (1), Grandfather (1), Patient (1), Physician (1), Nurse (1), Social worker (1) | Semi-structured interview | Conventional content analysis | Commitment to care
|
| 23 | Shahriar Salehitali et al. (2018) | 16 (8:8) | Qualitative research | 25–70 | 3–11 years | Spouse (4), Son (2), Mother (3), Father (2), Daughter (2), Grandfather (1), Nurse (1), Doctor (1) | Semi-structured interview and observations | Content analysis | Progressive exhaustion
|
| 24 | Abbas Ebadi et al. (2018) | 19 (8:11) | Qualitative study | 27–78 (Average: 42.16 ± 48) | 46.33 ± 97.24 months (6–84) | Parent (2), Daughter (4), Son (3), Spouse (6) | In-depth interviews | Content analysis | Suspended life pattern
|
| 25 | Dian Sari et al. (2018) | 7 | Descriptive phenomenology | Not reported | Not reported | Not reported | In-depth interviews | Colaizzi technique |
|
| 26 | Tayebeh Pourghaznein et al. (2018) | 11 | hermeneutic phenomenology (step1–2) | 23–51 (Average: 38) | 2 months–8 years | Mother (11) | Semi-structured interview | hermeneutic phenomenology (step 3–6) | Immersion in an ocean of psychological tension
|
| 27 | Tayebe Pourghaznein et al. (2018) | 11 | hermeneutic phenomenology (step1–2) | 23–51 (Average: 38.00 ± 9.00) | 2 months–8 years | Mother (11) | Semi-structured interview | hermeneutic phenomenology (step 3–6) |
|
| 28 | Christine Turner, and Patricia Finch-Guthrie(2020) | 6 | descriptive phenomenology | 29–56 | 3.36 years (2 months–10 years) | Granddaughter (1), Daughter (3), Wife (1), Son-in-law (1) | Semi-structured | Giorgi method |
|
| Key Concepts from First and Second-Order Constructs | Sub-Themes | Themes |
|---|---|---|
| Dealing with the patient’s emotions The patient’s excessive dependence Responsibility for the patient’s life Need to transport patients regularly Financial burden |
| I. Bearing the burden of life as a caregiver |
| The agony of having to watch the patient’s pain Ignoring their inner feelings Extreme physical fatigue Emotionally exhausted Confusion caused by the complexity of the patient’s disease Guilt for the patient |
| |
| Management of the patient’s fistula Close observation of a patient to prevent sudden death Controlling patients for treatment guidelines Cooperation of the whole family |
| II. Reconstructing life to maintain hemodialysis |
| Personalizing care Decision-making about patient care Setting priorities based on patient’s need Adjusting daily life for hemodialysis |
| |
| Neglecting their physical health Thinking of everything as patient-centered Difficulty in leisure activities Decreased quality of life |
| III. The fading of caregiver’s own life |
| Deterioration of marital relationship Neglecting other family members Sacrifice of other families Difficulty in social life Feeling ignored by medical staff |
| |
| Unpredictable patient’s physical condition Uncertainty about caregiver’s future Disconnected employment Endless treatment process Expectations for a kidney transplant |
| |
| Learning from the experiences of acquaintances Information from diverse resources Having personal time Being separated from the caregivers’ life Development of hobbies |
| IV. Effort to relieve the burden |
| Dependence on religion Sharing the burdens with others Finding of resources to get help |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.-Y.; Lee, Y.-N. Coexisting with the Life of Patients with Hemodialysis: Qualitative Meta-Synthesis Study of Life of Caregivers of Patients with Hemodialysis. Int. J. Environ. Res. Public Health 2022, 19, 2163. https://doi.org/10.3390/ijerph19042163
Kim E-Y, Lee Y-N. Coexisting with the Life of Patients with Hemodialysis: Qualitative Meta-Synthesis Study of Life of Caregivers of Patients with Hemodialysis. International Journal of Environmental Research and Public Health. 2022; 19(4):2163. https://doi.org/10.3390/ijerph19042163
Chicago/Turabian StyleKim, Eun-Young, and Ye-Na Lee. 2022. "Coexisting with the Life of Patients with Hemodialysis: Qualitative Meta-Synthesis Study of Life of Caregivers of Patients with Hemodialysis" International Journal of Environmental Research and Public Health 19, no. 4: 2163. https://doi.org/10.3390/ijerph19042163
APA StyleKim, E.-Y., & Lee, Y.-N. (2022). Coexisting with the Life of Patients with Hemodialysis: Qualitative Meta-Synthesis Study of Life of Caregivers of Patients with Hemodialysis. International Journal of Environmental Research and Public Health, 19(4), 2163. https://doi.org/10.3390/ijerph19042163