
Relationship between Alcohol Intake and Chronic Pain with Depressive Symptoms: A Cross-Sectional Analysis of the Shika Study

 , , , , , , , , , , ,
, , , , , , , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
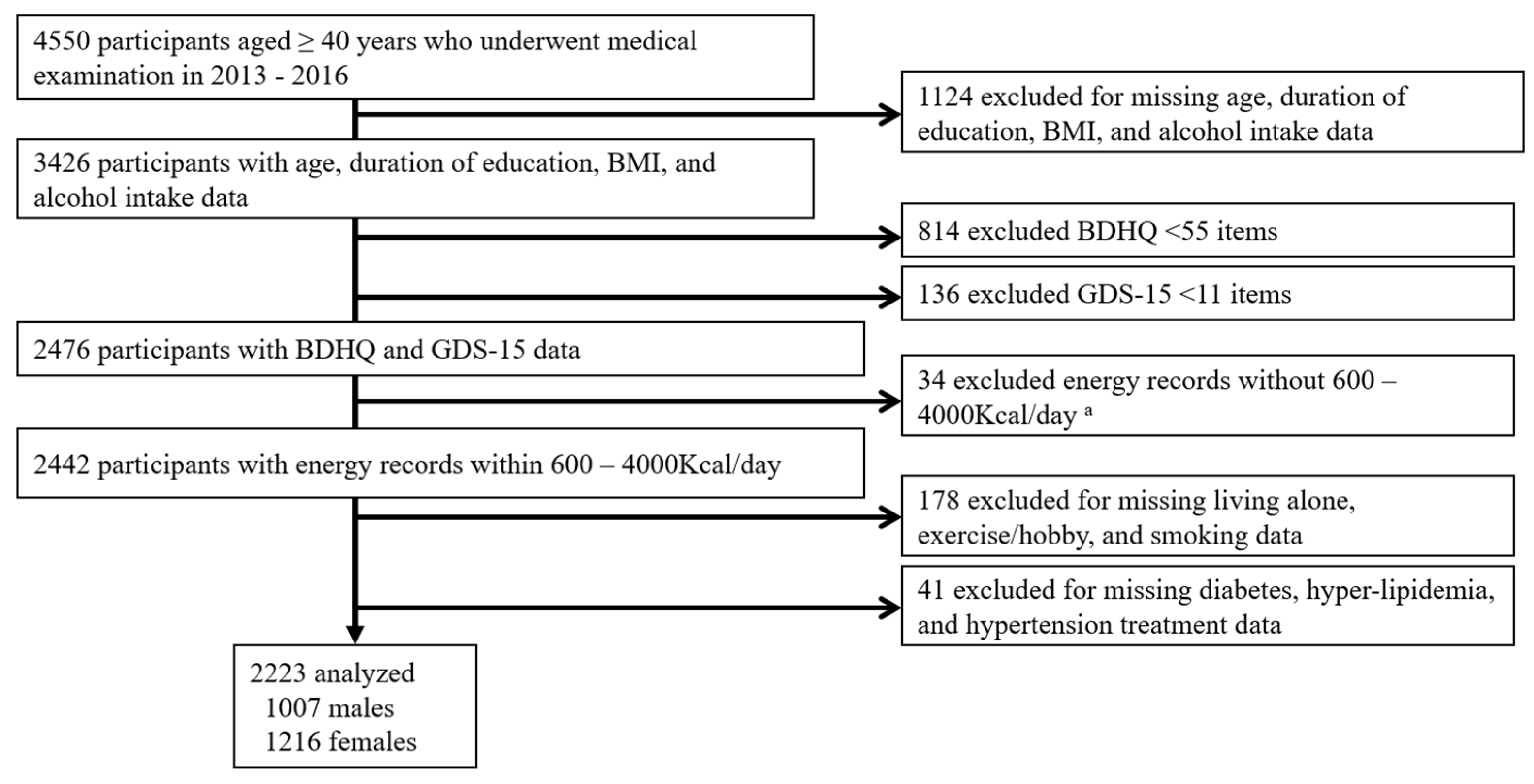
2.1. Participants
2.2. CP
2.3. Depressive State
2.4. Alcohol Intake Assessment
2.5. Questionnaire on Demographics
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Comparisons between Participants with/without Depressive Symptoms
3.3. Comparison between CP Groups
3.4. Effects of the Interaction between Depressive Symptoms and CP Groups
3.5. Multiple Logistic Regression Analysis of the Relationship between Alcohol Intake and CP Stratified by Depressive Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Treede, R.-D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. Chronic pain as a symptom or a disease: The IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakakibara, T.; Wang, Z.; Paholpak, P.; Kosuwon, W.; Oo, M.; Kasai, Y. A comparison of chronic pain prevalence in Japan, Thailand, and myanmar. Pain Physician 2013, 16, 603–608. [Google Scholar] [PubMed]
- Imai, R.; Imaoka, M.; Nakao, H.; Hida, M.; Tazaki, F.; Omizu, T.; Ishigaki, T.; Nakamura, M. Association between chronic pain and pre-frailty in Japanese community-dwelling older adults: A cross-sectional study. PLoS ONE 2020, 15, e0236111. [Google Scholar] [CrossRef] [PubMed]
- Yong, R.J.; Mullins, P.M.; Bhattacharyya, N. Prevalence of chronic pain among adults in the United States. Pain 2021, 163, e328–e332. [Google Scholar] [CrossRef] [PubMed]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 2020, CD011279. [Google Scholar] [CrossRef] [Green Version]
- Robins, M.T.; Heinricher, M.M.; Ryabinin, A.E. From Pleasure to Pain, and Back Again: The Intricate Relationship Between Alcohol and Nociception. Alcohol Alcohol. 2019, 54, 625–638. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, P.; Rui, J.; Zhao, X.; Lao, J. The Associated Factors and Clinical Features of Neuropathic Pain after Brachial Plexus Injuries: A cross-sectional study. Clin. J. Pain 2017, 33, 1030–1036. [Google Scholar] [CrossRef]
- Jarisch, R.; Wantke, F. Wine and Headache. Int. Arch. Allergy Immunol. 1996, 110, 7–12. [Google Scholar] [CrossRef]
- Boyer, J.; Bancel, E.; Perray, P.; Pouderoux, P.; Balmes, J.; Bali, J. Effect of Champagne Compared to Still White Wine on Peripheral Neurotransmitter Concentrations. Int. J. Vitam. Nutr. Res. 2004, 74, 321–328. [Google Scholar] [CrossRef]
- Capito, E.S.; Lautenbacher, S.; Wolstein, J.; Horn-Hofmann, C. Effects of oral alcohol administration on heat pain threshold and ratings of supra-threshold stimuli. Scand. J. Pain 2020, 20, 623–634. [Google Scholar] [CrossRef]
- Lovinger, D.M.; Roberto, M. Synaptic effects induced by alcohol. Curr. Top. Behav. Neurosci. 2010, 13, 31–86. [Google Scholar] [CrossRef] [Green Version]
- Lobo, I.A.; Harris, R.A. GABAA receptors and alcohol. Pharmacol. Biochem. Behav. 2008, 90, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasebikan, V.O.; Gureje, O. Lifetime and 7-day alcohol consumption in the elderly, prevalence and correlates: Reports from the Ibadan Study of Aging. Afr. J. Med. Med. Sci. 2015, 44, 33–41. [Google Scholar] [PubMed]
- Suzuki, K.; Tsujiguchi, H.; Miyagi, S.; Nguyen, T.T.T.; Hara, A.; Nakamura, H.; Shimizu, Y.; Hayashi, K.; Yamada, Y.; Nguyen, P.M.; et al. Association Between Serum 25-Hydroxyvitamin D Concentrations and Chronic Pain: Effects of Drinking Habits. J. Pain Res. 2020, 13, 2987–2996. [Google Scholar] [CrossRef]
- Narukawa, N.; Tsujiguchi, H.; Hara, A.; Miyagi, S.; Kannon, T.; Suzuki, K.; Shimizu, Y.; Nguyen, T.; Pham, K.; Suzuki, F.; et al. Relationship between Vitamin Intake and Health-Related Quality of Life in a Japanese Population: A Cross-Sectional Analysis of the Shika Study. Nutrients 2021, 13, 1023. [Google Scholar] [CrossRef]
- Sheng, J.; Liu, S.; Wang, Y.; Cui, R.; Zhang, X. The Link between Depression and Chronic Pain: Neural Mechanisms in the Brain. Neural Plast. 2017, 2017, 9724371. [Google Scholar] [CrossRef]
- Zis, P.; Daskalaki, A.; Bountouni, I.; Sykioti, P.; Varrassi, G.; Paladini, A. Depression and chronic pain in the elderly: Links and management challenges. Clin. Interv. Aging 2017, 12, 709–720. [Google Scholar] [CrossRef] [Green Version]
- Lipton, R.I. The effect of moderate alcohol use on the relationship between stress and depression. Am. J. Public Health 1994, 84, 1913–1917. [Google Scholar] [CrossRef] [Green Version]
- Karpyak, V.M.; Geske, J.R.; Hall-Flavin, D.K.; Loukianova, L.L.; Schneekloth, T.D.; Skime, M.K.; Seppala, M.; Dawson, G.; Frye, M.A.; Choi, D.-S.; et al. Sex-specific association of depressive disorder and transient emotional states with alcohol consumption in male and female alcoholics. Drug Alcohol Depend. 2019, 196, 31–39. [Google Scholar] [CrossRef]
- Karpyak, V.M.; Biernacka, J.M.; Geske, J.R.; Abulseoud, O.A.; Brunner, M.D.; Chauhan, M.; Hall-Flavin, D.K.; Lewis, K.A.; Loukianova, L.L.; Melnyk, G.J.; et al. Gender-specific effects of comorbid depression and anxiety on the propensity to drink in negative emotional states. Addiction 2016, 111, 1366–1375. [Google Scholar] [CrossRef]
- Tsujiguchi, H.; Hori, D.; Kambayashi, Y.; Hamagishi, T.; Asakura, H.; Mitoma, J.; Kitaoka, M.; Anyenda, E.O.; Nguyen, T.T.T.; Yamada, Y.; et al. Relationship between screen time and nutrient intake in Japanese children and adolescents: A cross-sectional observational study. Environ. Health Prev. Med. 2018, 23, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shika Town Population. September 2020. Available online: https://www.town.shika.lg.jp/jyuumin/shika_town_pop/reiwa2/shikatown_pop_202009.html (accessed on 8 August 2021).
- Sugishita, K.; Sugishita, M.; Hemmi, I.; Asada, T.; Tanigawa, T. A Validity and Reliability Study of the Japanese Version of the Geriatric Depression Scale 15 (GDS-15-J). Clin. Gerontol. 2017, 40, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.; Park, M.H.; Lee, S.-H.; Ko, Y.-H.; Kim, Y.-K.; Han, K.-M.; Jeong, H.-G.; Han, C. Usefulness of the 15-item geriatric depression scale (GDS-15) for classifying minor and major depressive disorders among community-dwelling elders. J. Affect. Disord. 2019, 259, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, M.; Haruna, M.; Matsuzaki, M.; Murayama, R.; Sasaki, S. Availability of two self-administered diet history questionnaires for pregnant Japanese women: A validation study using 24-hour urinary markers. J. Epidemiol. 2017, 27, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.; Binder, A.; Wasner, G. Neuropathic pain: Diagnosis, pathophysiological mechanisms, and treatment. Lancet Neurol. 2010, 9, 807–819. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Kuner, R.; Jensen, T.S. Neuropathic pain: From mechanisms to treatment. Physiol. Rev. 2021, 101, 259–301. [Google Scholar] [CrossRef]
- Barakat, A.; Hamdy, M.M.; Elbadr, M.M. Uses of fluoxetine in nociceptive pain management: A literature overview. Eur. J. Pharmacol. 2018, 829, 12–25. [Google Scholar] [CrossRef]
- de Araujo, D.S.M.; Nassini, R.; Geppetti, P.; De Logu, F. TRPA1 as a therapeutic target for nociceptive pain. Expert Opin. Ther. Targets 2020, 24, 997–1008. [Google Scholar] [CrossRef]
- Panconesi, A. Alcohol and migraine: Trigger factor, consumption, mechanisms. A review. J. Headache Pain 2008, 9, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.-C.; Strassman, A.M.; Burstein, R.; Levy, D. Sensitization and Activation of Intracranial Meningeal Nociceptors by Mast Cell Mediators. J. Pharmacol. Exp. Ther. 2007, 322, 806–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, R.; Gregor, D.; Peng, Z.; Li, J.; Bekker, A.; Ye, J. Chronic intermittent voluntary alcohol drinking induces hyperalgesia in Sprague-Dawley rats. Int. J. Physiol. Pathophysiol. Pharmacol. 2015, 7, 136–144. [Google Scholar] [PubMed]
- Fishbain, D.A.; Cutler, R.; Rosomoff, H.L.; Rosomoff, R.S. Chronic Pain-Associated Depression: Antecedent or Consequence of Chronic Pain? A Review. Clin. J. Pain 1997, 13, 116–137. [Google Scholar] [CrossRef] [PubMed]
- Valdés, M.; Garcia, L.; Treserra, J.; De Pablo, J.; De Flores, T. Psychogenic pain and depressive disorders: An empirical study. J. Affect. Disord. 1989, 16, 21–25. [Google Scholar] [CrossRef]
- Von Korff, M.; Simon, G. The relationship between pain and depression. Br. J. Psychiatry 1996, 168, 101–108. [Google Scholar] [CrossRef]
- Klauenberg, S.; Maier, C.; Assion, H.-J.; Hoffmann, A.; Krumova, E.K.; Magerl, W.; Scherens, A.; Treede, R.-D.; Juckel, G. Depression and changed pain perception: Hints for a central disinhibition mechanism. Pain 2008, 140, 332–343. [Google Scholar] [CrossRef]
- Ossipov, M.H.; Dussor, G.O.; Porreca, F. Central modulation of pain. J. Clin. Investig. 2010, 120, 3779–3787. [Google Scholar] [CrossRef] [Green Version]
- Picavet, H.S.J.; Vlaeyen, J.; Schouten, J.S. Pain Catastrophizing and Kinesiophobia: Predictors of Chronic Low Back Pain. Am. J. Epidemiol. 2002, 156, 1028–1034. [Google Scholar] [CrossRef]
- Somers, T.J.; Keefe, F.J.; Pells, J.J.; Dixon, K.E.; Waters, S.J.; Riordan, P.A.; Blumenthal, J.A.; McKee, D.C.; LaCaille, L.; Tucker, J.M.; et al. Pain Catastrophizing and Pain-Related Fear in Osteoarthritis Patients: Relationships to Pain and Disability. J. Pain Symptom Manag. 2009, 37, 863–872. [Google Scholar] [CrossRef]
- Maleki, N.; Oscar-Berman, M. Chronic Pain in Relation to Depressive Disorders and Alcohol Abuse. Brain Sci. 2020, 10, 826. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 2223) | p-Value a | ||||
|---|---|---|---|---|---|
| Male (n = 1007) | Female (n = 1216) | ||||
| Mean/n | SD/% | Mean/n | SD/% | ||
| Age, years | 68.78 | 8.41 | 69.65 | 9.36 | <0.001 |
| Living alone, n | 75 | 7.45 | 150 | 12.34 | <0.001 |
| Education, years | 11.39 | 3.01 | 10.88 | 2.50 | 0.006 |
| Without exercise/hobbies, n | 601 | 59.68 | 780 | 64.14 | 0.031 |
| Smoking history, n | 284 | 28.20 | 44 | 3.62 | <0.001 |
| BMI, kg/m2 | 23.41 | 2.97 | 22.64 | 3.23 | 0.079 |
| Diabetes treatment, n | 131 | 13.01 | 93 | 7.65 | <0.001 |
| Hyperlipidemia treatment, n | 111 | 11.02 | 218 | 17.93 | <0.001 |
| Hypertension treatment, n | 363 | 36.05 | 372 | 30.59 | 0.007 |
| Depressive symptoms, n | 350 | 34.76 | 396 | 32.57 | 0.276 |
| Alcohol (crude data), g | 19.85 | 25.09 | 2.02 | 6.30 | <0.001 |
| Alcohol (density method), % energy | 3.80 | 4.53 | 0.51 | 1.54 | <0.001 |
| No alcohol intake, n | 325 | 32.27 | 908 | 74.67 | <0.001 |
| CP | |||||
| Any, n | 74 | 7.35 | 131 | 10.77 | 0.006 |
| Head, n | 0 | – | 4 | 0.329 | 0.089 |
| Neck/shoulder/upper limb, n | 28 | 2.78 | 46 | 3.78 | 0.190 |
| Low back/knee, n | 56 | 5.56 | 95 | 7.81 | 0.036 |
| Foot, n | 15 | 1.49 | 23 | 1.89 | 0.467 |
| Without Depressive Symptoms (n = 657) | With Depressive Symptoms (n = 350) | p-Value a | |||
|---|---|---|---|---|---|
| Mean/n | SD/% | Mean/n | SD/% | ||
| Age, years | 68.55 | 7.84 | 69.21 | 9.38 | 0.260 |
| Living alone, n | 37 | 5.63 | 38 | 10.86 | 0.003 |
| Education, years | 11.49 | 3.23 | 11.21 | 2.56 | 0.130 |
| Without exercise/hobbies, n | 347 | 52.82 | 254 | 72.56 | <0.001 |
| Smoking history, n | 184 | 28.01 | 100 | 28.57 | 0.849 |
| BMI, kg/m2 | 23.53 | 2.84 | 23.19 | 3.18 | 0.089 |
| Diabetes treatment, n | 87 | 13.24 | 44 | 12.57 | 0.763 |
| Hyperlipidemia treatment, n | 81 | 12.33 | 30 | 8.57 | 0.070 |
| Hypertension treatment, n | 248 | 37.75 | 115 | 32.86 | 0.124 |
| Alcohol (crude data), g | 20.89 | 24.84 | 17.90 | 25.47 | 0.075 |
| Alcohol (density method), % energy | 3.95 | 4.38 | 3.53 | 4.79 | 0.175 |
| No alcohol intake, n | 190 | 28.92 | 135 | 38.57 | 0.002 |
| CP | |||||
| Any, n | 39 | 5.94 | 35 | 10.00 | 0.019 |
| Head, n | 0 | - | 0 | - | - |
| Neck/shoulder/upper limb, n | 15 | 2.28 | 13 | 3.71 | 0.188 |
| Low back/knee, n | 27 | 4.11 | 29 | 8.29 | 0.006 |
| Foot, n | 7 | 1.07 | 8 | 2.29 | 0.128 |
| Non-CP (Any) (n = 933) | CP (Any) (n = 74) | p-Value a | |||
|---|---|---|---|---|---|
| Mean/n | SD/% | Mean/n | SD/% | ||
| Male (n = 1007) | |||||
| Age, years | 68.60 | 8.28 | 71.03 | 9.73 | 0.040 |
| Living alone, n | 65 | 6.97 | 10 | 13.51 | 0.039 |
| Education, years | 11.48 | 3.03 | 10.27 | 2.56 | <0.001 |
| Without exercise/hobbies, n | 553 | 59.27 | 48 | 64.86 | 0.345 |
| Smoking history, n | 258 | 27.65 | 26 | 35.14 | 0.169 |
| BMI, kg/m2 | 23.36 | 2.96 | 24.02 | 3.03 | 0.076 |
| Diabetes treatment, n | 119 | 12.75 | 12 | 16.22 | 0.394 |
| Hyperlipidemia treatment, n | 103 | 11.04 | 8 | 10.81 | 0.952 |
| Hypertension treatment, n | 336 | 36.01 | 27 | 36.49 | 0.935 |
| Depressive symptoms, n | 315 | 33.76 | 35 | 47.30 | 0.019 |
| Alcohol (crude data), g | 19.73 | 25.04 | 21.39 | 25.76 | 0.594 |
| Alcohol (density method), % energy | 3.75 | 4.44 | 4.38 | 5.52 | 0.347 |
| No alcohol intake, n | 302 | 32.37 | 23 | 31.08 | 0.820 |
| CP | |||||
| Head, n | 0 | - | 0 | - | - |
| Neck/shoulder/upper limb, n | 0 | - | 28 | 37.84 | - |
| Low back/knee, n | 0 | - | 56 | 75.68 | - |
| Foot, n | 0 | - | 15 | 20.27 | - |
| Non-CP (Any) (n = 933) | CP (Any) (n = 74) | p-Value a | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean (95%CI) | n | Mean (95%CI) | n | DS | CP | DS × CP | ||
| Head pain | NDS | 3.87 (3.53, 4.21) | 657 | - (-, -) | 0 | 0.503 | - | - |
| DS | 3.67 (3.20, 4.14) | 350 | - (-, -) | 0 | ||||
| Neck/shoulder/ upper limb pain | NDS | 3.85 (3.51, 4.20) | 642 | 4.59 (2.37, 6.81) | 15 | 0.727 | 0.448 | 0.912 |
| DS | 3.65 (3.18, 4.13) | 337 | 4.20 (1.81, 6.59) | 13 | ||||
| Low back/knee pain | NDS | 3.81 (3.47, 4.16) | 630 | 5.18 (3.51, 6.86) | 27 | 0.043 | 0.75 | 0.053 |
| DS | 3.75 (3.27, 4.24) | 321 | 2.77 (1.17, 4.37) | 29 | ||||
| Foot pain | NDS | 3.85 (3.51, 4.19) | 650 | 5.43 (2.16, 8.69) | 7 | 0.102 | 0.886 | 0.129 |
| DS | 3.72 (3.24, 4.19) | 342 | 1.81 (−1.23, 4.86) | 8 | ||||
| Exp (B) | 95%Cl Lower | 96%Cl Upper | p-Value | ||
|---|---|---|---|---|---|
| With depressive symptoms (n = 350) | Alcohol (density method) | 0.986 | 0.905 | 1.074 | 0.746 |
| Without depressive symptoms (n = 657) | Alcohol (density method) | 1.090 | 1.018 | 1.167 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amatsu, T.; Tsujiguchi, H.; Hara, A.; Miyagi, S.; Kannon, T.; Suzuki, K.; Shimizu, Y.; Nguyen, T.T.T.; Pham, K.-O.; Suzuki, F.; et al. Relationship between Alcohol Intake and Chronic Pain with Depressive Symptoms: A Cross-Sectional Analysis of the Shika Study. Int. J. Environ. Res. Public Health 2022, 19, 2024. https://doi.org/10.3390/ijerph19042024
Amatsu T, Tsujiguchi H, Hara A, Miyagi S, Kannon T, Suzuki K, Shimizu Y, Nguyen TTT, Pham K-O, Suzuki F, et al. Relationship between Alcohol Intake and Chronic Pain with Depressive Symptoms: A Cross-Sectional Analysis of the Shika Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2024. https://doi.org/10.3390/ijerph19042024
Chicago/Turabian StyleAmatsu, Takashi, Hiromasa Tsujiguchi, Akinori Hara, Sakae Miyagi, Takayuki Kannon, Keita Suzuki, Yukari Shimizu, Thao Thi Thu Nguyen, Kim-Oanh Pham, Fumihiko Suzuki, and et al. 2022. "Relationship between Alcohol Intake and Chronic Pain with Depressive Symptoms: A Cross-Sectional Analysis of the Shika Study" International Journal of Environmental Research and Public Health 19, no. 4: 2024. https://doi.org/10.3390/ijerph19042024
APA StyleAmatsu, T., Tsujiguchi, H., Hara, A., Miyagi, S., Kannon, T., Suzuki, K., Shimizu, Y., Nguyen, T. T. T., Pham, K.-O., Suzuki, F., Kasahara, T., Nakamura, M., Hayashi, K., Shibata, A., Ogino, N., Konoshita, T., Kambayashi, Y., Tsuboi, H., Tajima, A., & Nakamura, H. (2022). Relationship between Alcohol Intake and Chronic Pain with Depressive Symptoms: A Cross-Sectional Analysis of the Shika Study. International Journal of Environmental Research and Public Health, 19(4), 2024. https://doi.org/10.3390/ijerph19042024