
Prenatal Mercury Exposure and Neurodevelopment up to the Age of 5 Years: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Protocol
2.2. Search Strategy
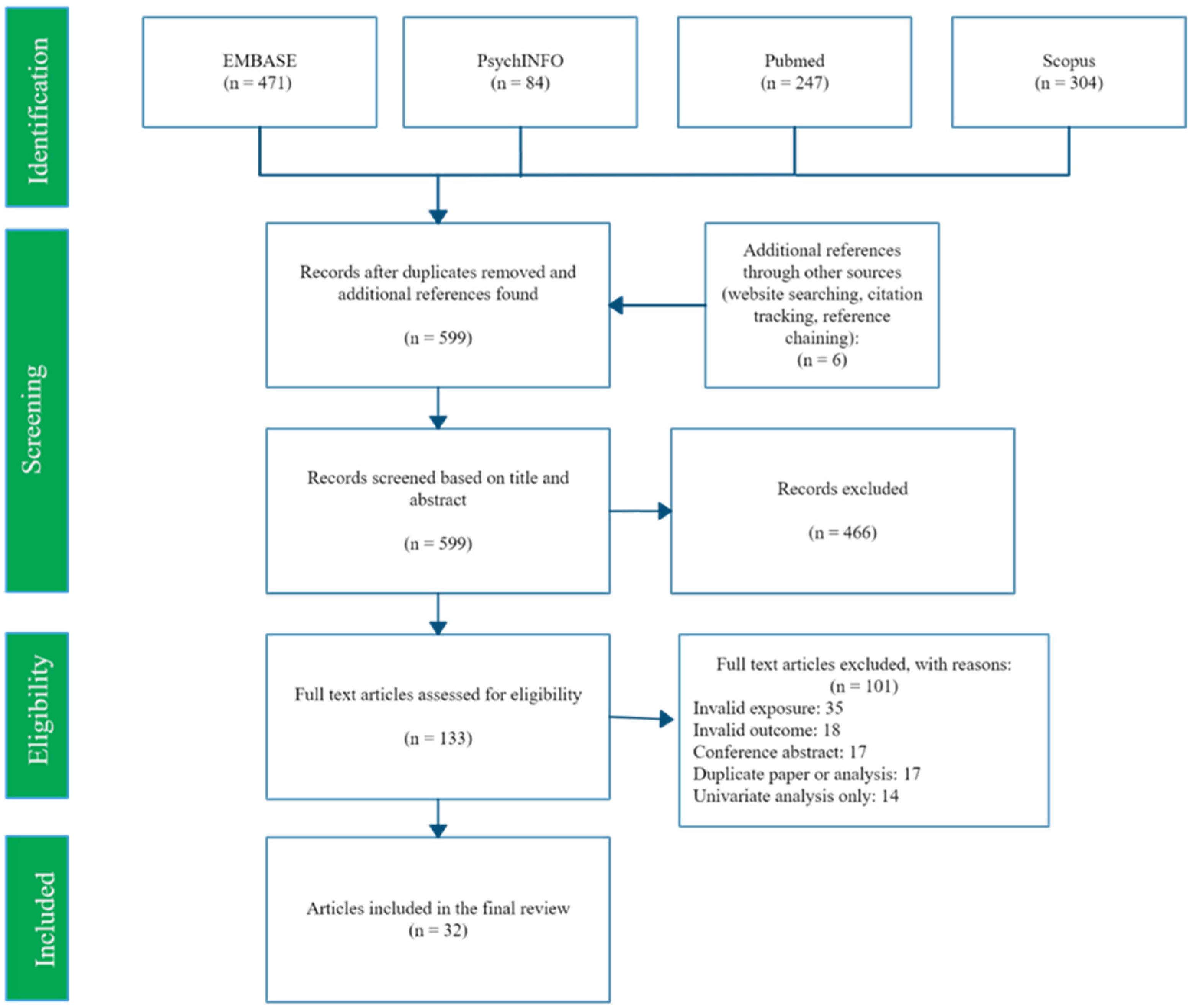
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Evidence Synthesis
- Cognition and language as measured by the Bayley Scales of Infant and Toddler Development II (BSID-II) Mental Developmental Index (MDI).
- Other measure of cognition, including attention, executive function, and memory.
- Motor function, fine, and gross.
- Communication and language development.
- Social development.
- General or composite measures of neurodevelopmental functioning.
3. Results
3.1. Study Characteristics
3.2. Evidence Summary
3.2.1. Cognition and Language as Measured by the BSID-II MDI (n = 10)
3.2.2. Other Measure of Cognition, Including Attention, Executive Function, and Memory (n = 13)
3.2.3. Motor Function, Fine, and Gross (n = 23)
3.2.4. Communication and Language Development (n = 11)
3.2.5. Social Development (n = 5)
3.2.6. General or Composite Measures of Neurodevelopmental Functioning (n = 11)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Included Studies

{kind=link}
| Study (Year) | Reference | Country | Study Design | Exposure | Timing of Exposure | Outcome 1 | Timing of Outcome | Sample Size 2 | High Quality 3 |
| Barbone et al. (2019) | [61] | Italy, Slovenia, Croatia, Greece | Prospective | Hair Whole blood Umbilical cord | 20 weeks—delivery 20 weeks—delivery At delivery | Bayley-III | 18 months | 628–1086 | Yes |
| Boucher et al. (2014) | [55] | Canada | Prospective | Umbilical cord | At delivery | FTII, A-not-B test, BSID-II | 6.5, 11 months | 94 | Yes |
| Castriotta et al. (2020) | [62] | Italy | Prospective | Umbilical cord | 20–32 weeks gestation | Bayley-III cognitive | 40 months | 323 | No |
| Daniels et al. (2004) | [74] | United Kingdom | Prospective | Umbilical cord | At delivery | MCDI, DDST | 15, 18 months | 1054 | Yes |
| Davidson et al. (2008) | [50] | Republic of Seychelles | Prospective | Hair | At delivery | BSID-II | 9, 30 months | 225–228 | No |
| Freire et al. (2018) | [68] | Spain | Prospective | Placenta | At delivery | MSCA | 48-60 months | 302 | No |
| Golding et al. (2016) | [76] | United Kingdom | Prospective | Whole blood | 11 weeks gestation | Modified DDST | 6, 18, 30, 42 months | 2394–2721 | No |
| Hu et al. (2016) | [73] | China | Prospective | Whole blood Umbilical cord | At delivery | GDS | 12 months | 410 | Yes |
| Jedrychowski et al. (2007) | [56] | Poland | Prospective | Umbilical cord | At delivery | BSID-II | 12, 24, 36 months | 270–374 | No |
| Kim S et al. (2008) | [57] | South Korea | Prospective | Whole blood Umbilical cord | At delivery | BSID-II, SMS | 13-24 months | 49–118 | No |
| Kim Y et al. (2018) | [48] | South Korea | Prospective | Whole blood Whole blood Umbilical cord | 12–20 weeks gestation 28–42 weeks gestation At delivery | BSID-II | 6, 12, 24, 36 months | 414–790 | Yes |
| Lederman et al. (2008) | [58] | USA | Prospective | Umbilical cord | At delivery | BSID-II, WPPSI-R | 12, 24, 36, 48 months | 107-132 | No |
| Lin et al. (2013) | Taiwan | Prospective | Umbilical cord | At delivery | CDIIT | 24 months | 230 | No | |
| Llop et al. (2012) | [59] | Spain | Prospective | Umbilical cord | At delivery | BSID-II | 14 months | 1683 | Yes |
| Marques et al. (2009) | [45] | Brazil | Prospective | Hair | At delivery | GDS | 6, 36, 60 months | 82 | No |
| Nisevic et al. (2019) | [63] | Croatia, Italy | Prospective | Umbilical cord | At delivery | Bayley-III | 18 months | 257 | Yes |
| Nyanza et al. (2020) | [46] | Tanzania | Prospective | Whole blood | 16–27 weeks gestation | MDAT | 6–12 months | 429 | No |
| Oken et al. (2005) | [70] | USA | Prospective | Hair | At delivery | VRM | 6 months | 135 | No |
| Oken et al. (2008) | [69] | USA | Prospective | Erythrocyte | 2nd trimester | PPVT, WRAVMA | 36 months | 341 | Yes |
| Polanska et al. (2013) | [49] | Poland | Prospective | Hair | 30–34 weeks gestation | Bayley-III | 12–24 months | 303 | No |
| Prpic et al. (2017) | [72] | Croatia | Prospective | Umbilical cord | At delivery | Bayley-III | 18 months | 135 | Yes |
| Rothenberg et al. (2016) | [44] | China | Prospective | Whole blood Hair | At delivery | BSID-II | 12 months | 270 | Yes |
| Shah-Kulkarni et al. (2020) | [53] | South Korea | Prospective | Whole blood Whole blood Umbilical cord | 12–20 weeks gestation > 28 weeks gestation At delivery | K-BSID-II | 6 months | 321-467 | No |
| SnojTratnik et al. (2017) | [64] | Slovenia, Croatia | Prospective | Hair Umbilical cord | 34 weeks gestation/at delivery At delivery | Bayley-III | 16–20 months | 280–357 | No |
| Strain et al. (2015) | [54] | Republic of Seychelles | Prospective | Hair | At delivery | BSID-II, CDI | 20 months | 1241–1265 | No |
| Suzuki et al. (2010) | [43] | Japan | Prospective | Hair | At delivery | NBAS | 3 days | 498 | Yes |
| Tatsuta et al. (2014) | [67] | Japan | Prospective | Umbilical cord | At delivery | K-ABC | 42 months | 287 | No |
| Tatsuta et al. (2017) | [71] | Japan | Prospective | Umbilical cord | At delivery | BSID-II, KSPD | 18 months | 566 | Yes |
| Valent et al. (2013) | [65] | Italy | Prospective | Hair Umbilical cord | 20–22 weeks gestationAt delivery | Bayley-III | 18 months | 271–505 | Yes |
| Wang et al. (2019) | [66] | China | Prospective | Umbilical cord | At delivery | NBNA Bayley-III | 3 days18 months | 172–265 | No |
| Wu et al. (2014) | [75] | China | Prospective | Umbilical cord | At delivery | NBNA | 3 days | 418 | No |
| Xu et al. (2016) | [47] | USA | Prospective | Whole blood Umbilical cord | 16 weeks—delivery At delivery | NNNS | 5 weeks | 344 | Yes |
References
- Tierney, A.L.; Nelson, C.A., 3rd. Brain Development and the Role of Experience in the Early Years. Zero Three 2009, 30, 9–13. [Google Scholar] [PubMed]
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the “First 1000 Days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, S.P.; Wachs, T.D.; Meeks Gardner, J.; Lozoff, B.; Wasserman, G.A.; Pollitt, E.; Carter, J.A. Child development: Risk factors for adverse outcomes in developing countries. Lancet 2007, 369, 145–157. [Google Scholar] [CrossRef]
- Fitzgerald, E.; Hor, K.; Drake, A.J. Maternal influences on fetal brain development: The role of nutrition, infection and stress, and the potential for intergenerational consequences. Early Hum. Dev. 2020, 150, 105190. [Google Scholar] [CrossRef]
- Bernhoft, R.A. Mercury toxicity and treatment: A review of the literature. J. Environ. Public Health 2012, 2012, 460508. [Google Scholar] [CrossRef]
- Syversen, T.; Kaur, P. The toxicology of mercury and its compounds. J. Trace Elem. Med. Biol. 2012, 26, 215–226. [Google Scholar] [CrossRef]
- Oliveira, C.S.; Nogara, P.A.; Ardisson-Araújo, D.M.P.; Aschner, M.; Rocha, J.B.T.; Dórea, J.G. Neurodevelopmental Effects of Mercury. Adv. Neurotoxicol. 2018, 2, 27–86. [Google Scholar] [CrossRef]
- Mason, R.P.; Choi, A.L.; Fitzgerald, W.F.; Hammerschmidt, C.R.; Lamborg, C.H.; Soerensen, A.L.; Sunderland, E.M. Mercury biogeochemical cycling in the ocean and policy implications. Environ. Res. 2012, 119, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Ascher, D.B.; Myung, Y.; Lamborg, C.H.; Hallam, S.J.; Gionfriddo, C.M.; Holt, K.E.; Moreau, J.W. Mercury methylation by metabolically versatile and cosmopolitan marine bacteria. ISME J. 2021, 15, 1810–1825. [Google Scholar] [CrossRef] [PubMed]
- Munson, K.M.; Lamborg, C.H.; Boiteau, R.M.; Saito, M.A. Dynamic mercury methylation and demethylation in oligotrophic marine water. Biogeosciences 2018, 15, 6451–6460. [Google Scholar] [CrossRef] [Green Version]
- Balshaw, S.; Edwards, J.; Daughtry, B.; Ross, K. Mercury in seafood: Mechanisms of accumulation and consequences for consumer health. Rev. Environ. Health 2007, 22, 91–113. [Google Scholar] [CrossRef] [PubMed]
- United Nations Environment Programme. Global Mercury Assessment 2018; UN: Geneva, Switzerland, 2019. [Google Scholar]
- Sunderland, E.M.; Krabbenhoft, D.P.; Moreau, J.W.; Strode, S.A.; Landing, W.M. Mercury sources, distribution, and bioavailability in the North Pacific Ocean: Insights from data and models. Glob. Biogeochem. Cycles 2009, 23, GB2010. [Google Scholar] [CrossRef] [Green Version]
- Hong, Y.-S.; Kim, Y.-M.; Lee, K.-E. Methylmercury exposure and health effects. J. Prev. Med. Public Health 2012, 45, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Bradley, M.A.; Barst, B.D.; Basu, N. A Review of Mercury Bioavailability in Humans and Fish. Int. J. Environ. Res. Public Health 2017, 14, 169. [Google Scholar] [CrossRef] [Green Version]
- Tong, M.; Yu, J.; Liu, M.; Li, Z.; Wang, L.; Yin, C.; Ren, A.; Chen, L.; Jin, L. Total mercury concentration in placental tissue, a good biomarker of prenatal mercury exposure, is associated with risk for neural tube defects in offspring. Environ. Int. 2021, 150, 106425. [Google Scholar] [CrossRef]
- Chen, Z.; Myers, R.; Wei, T.; Bind, E.; Kassim, P.; Wang, G.; Ji, Y.; Hong, X.; Caruso, D.; Bartell, T.; et al. Placental transfer and concentrations of cadmium, mercury, lead, and selenium in mothers, newborns, and young children. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 537–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aschner, M.; Aschner, J.L. Mercury neurotoxicity: Mechanisms of blood-brain barrier transport. Neurosci. Biobehav. Rev. 1990, 14, 169–176. [Google Scholar] [CrossRef]
- Sakamoto, M.; Chan, H.M.; Domingo, J.L.; Koriyama, C.; Murata, K. Placental transfer and levels of mercury, selenium, vitamin E, and docosahexaenoic acid in maternal and umbilical cord blood. Environ. Int. 2018, 111, 309–315. [Google Scholar] [CrossRef]
- Aberg, B.; Ekman, L.; Falk, R.; Greitz, U.; Persson, G.; Snihs, J.O. Metabolism of Methyl Mercury (203Hg) Compounds in Man. Arch. Environ. Health Int. J. 1969, 19, 478–484. [Google Scholar] [CrossRef]
- Jo, S.; Woo, H.D.; Kwon, H.-J.; Oh, S.-Y.; Park, J.-D.; Hong, Y.-S.; Pyo, H.; Park, K.S.; Ha, M.; Kim, H.; et al. Estimation of the Biological Half-Life of Methylmercury Using a Population Toxicokinetic Model. Int. J. Environ. Res. Public Health 2015, 12, 9054. [Google Scholar] [CrossRef] [Green Version]
- Vohr, B.R.; Poggi Davis, E.; Wanke, C.A.; Krebs, N.F. Neurodevelopment: The Impact of Nutrition and Inflammation During Preconception and Pregnancy in Low-Resource Settings. Pediatrics 2017, 139, S38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellinger, D.C. Environmental chemical exposures and neurodevelopmental impairments in children. Pediatr. Med. 2018, 1, 1–13. [Google Scholar] [CrossRef]
- Rand, M.D.; Caito, S.W. Variation in the biological half-life of methylmercury in humans: Methods, measurements and meaning. Biochim. Biophys. Acta (BBA) Gen. Subj. 2019, 1863, 129301. [Google Scholar] [CrossRef] [PubMed]
- Jafari, T.; Rostampour, N.; Fallah, A.A.; Hesami, A. The association between mercury levels and autism spectrum disorders: A systematic review and meta-analysis. J. Trace Elem. Med. Biol. 2017, 44, 289–297. [Google Scholar] [CrossRef]
- Choi, A.L.; Cordier, S.; Weihe, P.; Grandjean, P. Negative confounding in the evaluation of toxicity: The case of methylmercury in fish and seafood. Crit. Rev. Toxicol. 2008, 38, 877–893. [Google Scholar] [CrossRef] [Green Version]
- Mazahery, H.; Stonehouse, W.; Delshad, M.; Kruger, M.C.; Conlon, C.A.; Beck, K.L.; von Hurst, P.R. Relationship between Long Chain n-3 Polyunsaturated Fatty Acids and Autism Spectrum Disorder: Systematic Review and Meta-Analysis of Case-Control and Randomised Controlled Trials. Nutrients 2017, 9, 155. [Google Scholar] [CrossRef] [Green Version]
- Madore, C.; Leyrolle, Q.; Lacabanne, C.; Benmamar-Badel, A.; Joffre, C.; Nadjar, A.; Layé, S. Neuroinflammation in Autism: Plausible Role of Maternal Inflammation, Dietary Omega 3, and Microbiota. Neural Plast. 2016, 2016, 3597209. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.A. The first 1000 days: A critical period of nutritional opportunity and vulnerability. Nutr. Diet. 2020, 77, 295–297. [Google Scholar] [CrossRef]
- Holmes, P.; James, K.A.; Levy, L.S. Is low-level environmental mercury exposure of concern to human health? Sci. Total Environ. 2009, 408, 2. [Google Scholar] [CrossRef]
- Clarkson, T.W.; Jayesh, V.B.; Ballatori, N. Mechanisms of mercury disposition in the body. Am. J. Ind. Med. 2007, 50, 10. [Google Scholar] [CrossRef]
- Persson, M.; Fagt, S.; Nauta, M.J. Personalised fish intake recommendations: The effect of background exposure on optimisation. Br. J. Nutr. 2018, 120, 946–957. [Google Scholar] [CrossRef] [Green Version]
- Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 March 2021).
- Lederer, D.J.; Bell, S.C.; Branson, R.D.; Chalmers, J.D.; Marshall, R.; Maslove, D.M.; Ost, D.E.; Punjabi, N.M.; Schatz, M.; Smyth, A.R.; et al. Control of Confounding and Reporting of Results in Causal Inference Studies. Guidance for Authors from Editors of Respiratory, Sleep, and Critical Care Journals. Ann. Am. Thorac. Soc. 2018, 16, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin-Lun Hung, G.; Hahn, J.; Alamiri, B.; Buka, S.L.; Goldstein, J.M.; Laird, N.; Nelson, C.A.; Smoller, J.W.; Gilman, S.E. Socioeconomic disadvantage and neural development from infancy through early childhood. Int. J. Epidemiol. 2015, 44, 1889–1899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, S.; Ha, M.; Hwang, S.-S.; Son, M.; Kwon, H.-J. Disparities in Children’s Blood Lead and Mercury Levels According to Community and Individual Socioeconomic Positions. Int. J. Environ. Res. Public Health 2015, 12, 6232–6248. [Google Scholar] [CrossRef] [Green Version]
- Wehby, G.L.; Prater, K.; McCarthy, A.M.; Castilla, E.E.; Murray, J.C. The Impact of Maternal Smoking during Pregnancy on Early Child Neurodevelopment. J. Hum. Cap. 2011, 5, 207–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaxiola-Robles, R.; Bentzen, R.; Zenteno-Savín, T.; Labrada-Martagón, V.; Castellini, J.M.; Celis, A.; O’Hara, T.; Méndez-Rodríguez, L.C. Marine diet and tobacco exposure affects mercury concentrations in pregnant women (I) from Baja California Sur, Mexico. Toxicol. Rep. 2014, 1, 1123–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avella-Garcia, C.B.; Julvez, J. Seafood Intake and Neurodevelopment: A Systematic Review. Curr. Environ. Health Rep. 2014, 1, 46–77. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.-W.; Gwak, J.-I.; Park, Y.-H. The Effect of Smoking and Second-Hand Smoking on the Concentration of Mercury, Lead and Cadmium in the Blood: Based on the Fifth Korea National Health and Nutrition Examination Survey. Korean J. Fam. Pract. 2016, 6, 44–48. [Google Scholar] [CrossRef]
- Næss, S.; Kjellevold, M.; Dahl, L.; Nerhus, I.; Midtbø, L.K.; Bank, M.S.; Rasinger, J.D.; Markhus, M.W. Effects of seafood consumption on mercury exposure in Norwegian pregnant women: A randomized controlled trial. Environ. Int. 2020, 141, 105759. [Google Scholar] [CrossRef]
- Sharp, M.; DeMauro, S.B. Counterbalanced Comparison of the BSID-II and Bayley-III at Eighteen to Twenty-two Months Corrected Age. J. Dev. Behav. Pediatr. 2017, 38, 322–329. [Google Scholar] [CrossRef]
- Suzuki, K.; Nakai, K.; Sugawara, T.; Nakamura, T.; Ohba, T.; Shimada, M.; Hosokawa, T.; Okamura, K.; Sakai, T.; Kurokawa, N.; et al. Neurobehavioral effects of prenatal exposure to methylmercury and PCBs, and seafood intake: Neonatal behavioral assessment scale results of Tohoku study of child development. Environ. Res. 2010, 110, 699–704. [Google Scholar] [CrossRef]
- Rothenberg, S.E.; Yu, X.; Liu, J.; Biasini, F.J.; Hong, C.; Jiang, X.; Nong, Y.; Cheng, Y.; Korrick, S.A. Maternal methylmercury exposure through rice ingestion and offspring neurodevelopment: A prospective cohort study. Int. J. Hyg. Environ. Health 2016, 219, 832–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, R.C.; Dórea, J.G.; Bernardi, J.V.; Bastos, W.R.; Malm, O. Prenatal and postnatal mercury exposure, breastfeeding and neurodevelopment during the first 5 years. Cogn. Behav. Neurol. 2009, 22, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Nyanza, E.C.; Bernier, F.P.; Martin, J.W.; Manyama, M.; Hatfield, J.; Dewey, D. Effects of prenatal exposure and co-exposure to metallic or metalloid elements on early infant neurodevelopmental outcomes in areas with small-scale gold mining activities in Northern Tanzania. Environ. Int. 2021, 149, 106104. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Khoury, J.C.; Sucharew, H.; Dietrich, K.; Yolton, K. Low-level gestational exposure to mercury and maternal fish consumption: Associations with neurobehavior in early infancy. Neurotoxicol. Teratol. 2016, 54, 61–67. [Google Scholar] [CrossRef]
- Kim, Y.; Ha, E.-H.; Park, H.; Ha, M.; Kim, Y.; Hong, Y.-C.; Lee, E.J.; Kim, H.; Chang, N.; Kim, B.-N. Prenatal mercury exposure, fish intake and neurocognitive development during first three years of life: Prospective cohort mothers and Children’s environmental health (MOCEH) study. Sci. Total Environ. 2018, 615, 1192–1198. [Google Scholar] [CrossRef]
- Polanska, K.; Hanke, W.; Sobala, W.; Trzcinka-Ochocka, M.; Ligocka, D.; Brzeznicki, S.; Strugala-Stawik, H.; Magnus, P. Developmental Effects of Exposures to Environmental Factors: The Polish Mother and Child Cohort Study. Biomed. Res. Int. 2013, 2013, 629716. [Google Scholar] [CrossRef]
- Davidson, P.W.; Strain, J.J.; Myers, G.J.; Thurston, S.W.; Bonham, M.P.; Shamlaye, C.F.; Stokes-Riner, A.; Wallace, J.M.; Robson, P.J.; Duffy, E.M.; et al. Neurodevelopmental effects of maternal nutritional status and exposure to methylmercury from eating fish during pregnancy. Neurotoxicology 2008, 29, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.C.; Chen, Y.C.; Su, F.C.; Lin, C.M.; Liao, H.F.; Hwang, Y.H.; Hsieh, W.S.; Jeng, S.F.; Su, Y.N.; Chen, P.C. In utero exposure to environmental lead and manganese and neurodevelopment at 2 years of age. Environ. Res 2013, 123, 52–57. [Google Scholar] [CrossRef]
- Johnson, S.; Marlow, N. Developmental screen or developmental testing? Early Hum. Dev. 2006, 82, 173–183. [Google Scholar] [CrossRef]
- Shah-Kulkarni, S.; Lee, S.; Jeong, K.S.; Hong, Y.-C.; Park, H.; Ha, M.; Kim, Y.; Ha, E.-H. Prenatal exposure to mixtures of heavy metals and neurodevelopment in infants at 6 months. Environ. Res. 2020, 182, 109122. [Google Scholar] [CrossRef] [PubMed]
- Strain, J.J.; Yeates, A.J.; van Wijngaarden, E.; Thurston, S.W.; Mulhern, M.S.; McSorley, E.M.; Watson, G.E.; Love, T.M.; Smith, T.H.; Yost, K.; et al. Prenatal exposure to methyl mercury from fish consumption and polyunsaturated fatty acids: Associations with child development at 20 mo of age in an observational study in the Republic of Seychelles. Am. J. Clin. Nutr. 2015, 101, 530–537. [Google Scholar] [CrossRef] [Green Version]
- Boucher, O.; Muckle, G.; Jacobson, J.L.; Carter, R.C.; Kaplan-Estrin, M.; Ayotte, P.; Dewailly, É.; Jacobson, S.W. Domain-specific effects of prenatal exposure to PCBs, mercury, and lead on infant cognition: Results from the Environmental Contaminants and Child Development Study in Nunavik. Environ. Health Perspect. 2014, 122, 310–316. [Google Scholar] [CrossRef] [Green Version]
- Jedrychowski, W.; Perera, F.; Jankowski, J.; Rauh, V.; Flak, E.; Caldwell, K.L.; Jones, R.L.; Pac, A.; Lisowska-Miszczyk, I. Fish consumption in pregnancy, cord blood mercury level and cognitive and psychomotor development of infants followed over the first three years of life: Krakow epidemiologic study. Environ. Int. 2007, 33, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Eom, S.; Kim, H.J.; Lee, J.J.; Choi, G.; Choi, S.; Kim, S.; Kim, S.Y.; Cho, G.; Kim, Y.D.; et al. Association between maternal exposure to major phthalates, heavy metals, and persistent organic pollutants, and the neurodevelopmental performances of their children at 1 to 2years of age- CHECK cohort study. Sci. Total Environ. 2018, 624, 377–384. [Google Scholar] [CrossRef]
- Lederman, S.A.; Jones, R.L.; Caldwell, K.L.; Rauh, V.; Sheets, S.E.; Tang, D.; Viswanathan, S.; Becker, M.; Stein, J.L.; Wang, R.Y.; et al. Relation between cord blood mercury levels and early child development in a World Trade Center cohort. Environ. Health Perspect. 2008, 116, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Llop, S.; Guxens, M.; Murcia, M.; Lertxundi, A.; Ramon, R.; Riano, I.; Rebagliato, M.; Ibarluzea, J.; Tardon, A.; Sunyer, J.; et al. Prenatal exposure to mercury and infant neurodevelopment in a multicenter cohort in Spain: Study of potential modifiers. Am. J. Epidemiol. 2012, 175, 451–465. [Google Scholar] [CrossRef] [Green Version]
- Yi, Y.G.; Sung, I.Y.; Yuk, J.S. Comparison of Second and Third Editions of the Bayley Scales in Children with Suspected Developmental Delay. Ann. Rehabil. Med. 2018, 42, 313–320. [Google Scholar] [CrossRef] [Green Version]
- Barbone, F.; Rosolen, V.; Mariuz, M.; Parpinel, M.; Casetta, A.; Sammartano, F.; Ronfani, L.; Vecchi Brumatti, L.; Bin, M.; Castriotta, L.; et al. Prenatal mercury exposure and child neurodevelopment outcomes at 18 months: Results from the Mediterranean PHIME cohort. Int. J. Hyg. Environ. Health 2019, 222, 9–21. [Google Scholar] [CrossRef]
- Castriotta, L.; Rosolen, V.; Biggeri, A.; Ronfani, L.; Catelan, D.; Mariuz, M.; Bin, M.; Brumatti, L.V.; Horvat, M.; Barbone, F. The role of mercury, selenium and the Se-Hg antagonism on cognitive neurodevelopment: A 40-month follow-up of the Italian mother-child PHIME cohort. Int. J. Hyg. Environ. Health 2020, 230, 113604. [Google Scholar] [CrossRef]
- Nišević, J.R.; Prpić, I.; Kolić, I.; Baždarić, K.; Tratnik, J.S.; Prpić, I.; Mazej, D.; Špirić, Z.; Barbone, F.; Horvat, M. Combined prenatal exposure to mercury and LCPUFA on newborn’s brain measures and neurodevelopment at the age of 18 months. Environ. Res. 2019, 178, 108682. [Google Scholar] [CrossRef] [PubMed]
- Snoj Tratnik, J.; Falnoga, I.; Trdin, A.; Mazej, D.; Fajon, V.; Miklavčič, A.; Kobal, A.B.; Osredkar, J.; Sešek Briški, A.; Krsnik, M.; et al. Prenatal mercury exposure, neurodevelopment and apolipoprotein E genetic polymorphism. Environ. Res. 2017, 152, 375–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valent, F.; Mariuz, M.; Bin, M.; Little, D.; Mazej, D.; Tognin, V.; Tratnik, J.; McAfee, A.J.; Mulhern, M.S.; Parpinel, M.; et al. Associations of prenatal mercury exposure from maternal fish consumption and polyunsaturated fatty acids with child neurodevelopment: A prospective cohort study in Italy. J. Epidemiol. 2013, 23, 360–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Wu, W.; Li, H.; Cao, L.; Wu, M.; Liu, J.; Gao, Z.; Zhou, C.; Liu, J.; Yan, C. Relation of prenatal low-level mercury exposure with early child neurobehavioral development and exploration of the effects of sex and DHA on it. Environ. Int. 2019, 126, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Tatsuta, N.; Nakai, K.; Murata, K.; Suzuki, K.; Iwai-Shimada, M.; Kurokawa, N.; Hosokawa, T.; Satoh, H. Impacts of prenatal exposures to polychlorinated biphenyls, methylmercury, and lead on intellectual ability of 42-month-old children in Japan. Environ. Res. 2014, 133, 321–326. [Google Scholar] [CrossRef]
- Freire, C.; Amaya, E.; Gil, F.; Fernández, M.F.; Murcia, M.; Llop, S.; Andiarena, A.; Aurrekoetxea, J.; Bustamante, M.; Guxens, M.; et al. Prenatal co-exposure to neurotoxic metals and neurodevelopment in preschool children: The Environment and Childhood (INMA) Project. Sci. Total Environ. 2018, 621, 340–351. [Google Scholar] [CrossRef]
- Oken, E.; Radesky, J.S.; Wright, R.O.; Bellinger, D.C.; Amarasiriwardena, C.J.; Kleinman, K.P.; Hu, H.; Gillman, M.W. Maternal Fish Intake during Pregnancy, Blood Mercury Levels, and Child Cognition at Age 3 Years in a US Cohort. Am. J. Epidemiol. 2008, 167, 1171–1181. [Google Scholar] [CrossRef]
- Oken, E.; Wright, R.O.; Kleinman, K.P.; Bellinger, D.; Amarasiriwardena, C.J.; Hu, H.; Rich-Edwards, J.W.; Gillman, M.W. Maternal fish consumption, hair mercury, and infant cognition in a U.S. Cohort. Environ. Health Perspect. 2005, 113, 1376–1380. [Google Scholar] [CrossRef]
- Tatsuta, N.; Murata, K.; Iwai-Shimada, M.; Yaginuma-Sakurai, K.; Satoh, H.; Nakai, K. Psychomotor Ability in Children Prenatally Exposed to Methylmercury: The 18-Month Follow-Up of Tohoku Study of Child Development. Tohoku J. Exp. Med. 2017, 242, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Prpic, I.; Milardovic, A.; Vlasic-Cicvaric, I.; Spiric, Z.; Radic Nisevic, J.; Vukelic, P.; Snoj Tratnik, J.; Mazej, D.; Horvat, M. Prenatal exposure to low-level methylmercury alters the child’s fine motor skills at the age of 18 months. Environ. Res. 2017, 152, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Chen, L.; Wang, C.; Zhou, Y.; Zhang, Y.; Wang, Y.; Shi, R.; Gao, Y.; Tian, Y. Prenatal low-level mercury exposure and infant neurodevelopment at 12 months in rural northern China. Environ. Sci. Pollut. Res. Int. 2016, 23, 12050–12059. [Google Scholar] [CrossRef] [PubMed]
- Daniels, J.L.; Longnecker, M.P.; Rowland, A.S.; Golding, J. Fish intake during pregnancy and early cognitive development of offspring. Epidemiology 2004, 15, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Ying, T.; Shen, Z.; Wang, H. Effect of low-level prenatal mercury exposure on neonate neurobehavioral development in China. Pediatr. Neurol. 2014, 51, 93–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golding, J.; Gregory, S.; Iles-Caven, Y.; Hibbeln, J.; Emond, A.; Taylor, C.M. Associations between prenatal mercury exposure and early child development in the ALSPAC study. Neurotoxicology 2016, 53, 215–222. [Google Scholar] [CrossRef] [Green Version]
- Valko, M.; Morris, H.; Cronin, M.T. Metals, toxicity and oxidative stress. Curr. Med. Chem. 2005, 12, 1161–1208. [Google Scholar] [CrossRef] [Green Version]
- Chapman, L.; Chan, H.M. The influence of nutrition on methyl mercury intoxication. Environ. Health Perspect. 2000, 108, 29–56. [Google Scholar] [CrossRef] [Green Version]
- Philibert, A.; Fillion, M.; Mergler, D. Mercury exposure and premature mortality in the Grassy Narrows First Nation community: A retrospective longitudinal study. Lancet Planet. Health 2020, 4, e141–e148. [Google Scholar] [CrossRef]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sørensen, N.; Dahl, R.; Jørgensen, P.J. Cognitive Deficit in 7-Year-Old Children with Prenatal Exposure to Methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Taylor, C.M.; Golding, J.; Emond, A.M. Lead, cadmium and mercury levels in pregnancy: The need for international consensus on levels of concern. J. Dev. Orig. Health Dis. 2014, 5, 16–30. [Google Scholar] [CrossRef]
- Rice, D.C.; Schoeny, R.; Mahaffey, K. Methods and rationale for derivation of a reference dose for methylmercury by the US EPA. Risk Anal. Int. J. 2003, 23, 107–115. [Google Scholar] [CrossRef]
- Rice, D.C. The US EPA reference dose for methylmercury: Sources of uncertainty. Environ. Res. 2004, 95, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Mahaffey, K.R.; Clickner, R.P.; Bodurow, C.C. Blood organic mercury and dietary mercury intake: National Health and Nutrition Examination Survey, 1999 and 2000. Environ. Health Perspect. 2004, 112, 562–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhibshi, E. Subclinical neurotoxicity of mercury: A behavioural, molecular mechanisms and therapeutic perspective. Res. J. Pharm. Biol. Chem. Sci. 2012, 3, 34–42. [Google Scholar]
- Taylor, C.M.; Emmett, P.M.; Emond, A.M.; Golding, J. A review of guidance on fish consumption in pregnancy: Is it fit for purpose? Public Health Nutr. 2018, 21, 2149–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saavedra, S.; Fernández-Recamales, Á.; Sayago, A.; Cervera-Barajas, A.; González-Domínguez, R.; Gonzalez-Sanz, J.D. Impact of dietary mercury intake during pregnancy on the health of neonates and children: A systematic review. Nutr. Rev. 2022, 80, 317–328. [Google Scholar] [CrossRef]
- Hibbeln, J.R.; Spiller, P.; Brenna, J.T.; Golding, J.; Holub, B.J.; Harris, W.S.; Kris-Etherton, P.; Lands, B.; Connor, S.L.; Myers, G.; et al. Relationships between seafood consumption during pregnancy and childhood and neurocognitive development: Two systematic reviews. Prostaglandins Leukot. Essent. Fat. Acids 2019, 151, 14–36. [Google Scholar] [CrossRef] [Green Version]
- Grandjean, P.; Budtz-Jørgensen, E.; Jørgensen, P.J.; Weihe, P. Umbilical cord mercury concentration as biomarker of prenatal exposure to methylmercury. Environ. Health Perspect. 2005, 113, 905–908. [Google Scholar] [CrossRef] [Green Version]
- Kozikowska, I.; Binkowski, Ł.J.; Szczepańska, K.; Sławska, H.; Miszczuk, K.; Śliwińska, M.; Łaciak, T.; Stawarz, R. Mercury concentrations in human placenta, umbilical cord, cord blood and amniotic fluid and their relations with body parameters of newborns. Environ. Pollut. 2013, 182, 256–262. [Google Scholar] [CrossRef]
| Include | Exclude |
|---|---|
| 1. Study of total mercury, inorganic, organic, or methylmercury compounds. | 1. Studies other compounds including ethylmercury. |
| 2. Measures mercury in pregnant women. | 2. Measures mercury in other populations. |
| 3. Measures mercury concentrations in biological samples: blood (whole, erythrocyte, plasma, serum), urine, cord blood/tissue, placenta, or hair. | 3. Uses any other measure of mercury exposure. |
| 4. Measures neurodevelopmental functioning (i.e.: cognition, attention, memory, intelligence, fine/gross motor development, receptive/expressive language ability, communicative ability, social development, or overall neurodevelopment) in children aged 0 to 5 years old. | 4. Measures neurodevelopmental functioning in older children or adults, or only measures diagnoses or symptoms of neurodevelopmental disorders. |
| 5. Reports association between mercury and neurodevelopmental functioning | 5. Does not report associations between mercury and specified outcomes. |
| 6. Study reports results from multivariable analysis methods. | 6. Study reports results only from univariable methods such as correlations or t-tests. |
| Abbreviation | Name | n |
|---|---|---|
| A-not-B | A-not-B test | 1 |
| BSID-II | Bayley Scales of Infant and Toddler Development—Second Edition | 9 |
| Bayley-III/BSID-III | Bayley Scales of Infant and Toddler Development—Third Edition | 8 |
| CDI | MacArthur-Bates Communicative Development Inventories | 1 |
| CDIIT | Comprehensive Developmental Inventory for Infants and Toddlers | 1 |
| DDST | Denver Developmental Screening Test | 1 |
| DDST (modified) | Modified version of the Denver Developmental Screening Test | 1 |
| FTII | Fagan Test of Infant Intelligence | 1 |
| GDS | Gesell developmental schedules | 2 |
| K-ABC | Kaufman Assessment Battery for Children | 1 |
| K-BSID-II | Korean adapted version of Bayley Scales of Infant and Toddler Development II | 1 |
| KSPD | Kyoto Scale of Psychological Development | 1 |
| MCDI | MacArthur Communicative Development Inventory | 1 |
| MDAT | Malawi Developmental Assessment Tool | 1 |
| MSCA | McCarthy Scales of Children’s Abilities | 1 |
| NBAS | Neonatal Behavioral Assessment Scale | 1 |
| NBNA | Neonatal Behavioral Neurological Assessment | 2 |
| NNNS | NICU Network Neurobehavioral Scale | 1 |
| PPVT | Peabody Picture Vocabulary Test | 1 |
| SMS | Social Maturity Scale (Vineland) | 1 |
| VRM | Visual recognition memory | 1 |
| WPPSI-R | Wechsler Preschool and Primary Scales of Intelligence-Revised | 2 |
| WRAVMA | Wide Range Assessment of Visual Motor Abilities | 1 |
| Country | n 1 | n 1 | |
|---|---|---|---|
| Brazil | 1 | Republic of Seychelles | 2 |
| Canada | 1 | Slovenia | 2 |
| China | 4 | South Korea | 3 |
| Croatia | 4 | Spain | 2 |
| Greece | 1 | Taiwan | 1 |
| Italy | 4 | Tanzania | 1 |
| Japan | 3 | United Kingdom | 2 |
| Poland | 2 | USA | 4 |
| Mercury source (all maternal) | n | Mercury analysis | n |
| Whole blood | 10 | Atomic absorption spectroscopy (AAS) | 3 |
| Erythrocyte | 1 | Cold vapour atomic absorption spectrometry (CVAAS) | 22 |
| Hair | 10 | Inductively coupled plasma mass spectrometry (ICP-DRC-MS) | 1 |
| Placenta | 1 | Inductively coupled plasma mass spectrometry (ICP-MS) | 4 |
| Umbilical cord | 21 |
| Study | n | Exposure | Units | Outcome | Time of Outcome | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Boucher et al. (2014) | 87 | Umbilical cord | Ln μg/L | BSID-II: MDI | 11 months | 0.08 | −0.15 to 0.33 | |
| Kim Y et al. (2018) | 595 | Umbilical cord | μg/L | BSID-II: MDI | 12 months | −0.04 | −0.39 to 0.32 | 0.85 |
| Kim Y et al. (2018) | 523 | Umbilical cord | μg/L | BSID-II: MDI | 24 months | −0.03 | −0.36 to 0.3 | 0.87 |
| Kim Y et al. (2018) | 438 | Umbilical cord | μg/L | BSID-II: MDI | 36 months | 0.17 | −0.26 to 0.6 | 0.43 |
| Kim Y et al. (2018) | 662 | Umbilical cord | μg/L | BSID-II: MDI | 6 months | −0.03 | −0.27 to 0.21 | 0.8 |
| Kim Y et al. (2018) | 763 | Whole blood (early pregnancy) | μg/L | BSID-II: MDI | 12 months | −0.32 | −0.89 to 0.26 | 0.28 |
| Kim Y et al. (2018) | 614 | Whole blood (late pregnancy) | μg/L | BSID-II: MDI | 12 months | −0.07 | −0.69 to 0.55 | 0.82 |
| Kim Y et al. (2018) | 686 | Whole blood (early pregnancy) | μg/L | BSID-II: MDI | 24 months | −0.06 | −0.63 to 0.51 | 0.83 |
| Kim Y et al. (2018) | 564 | Whole blood (late pregnancy) | μg/L | BSID-II: MDI | 24 months | −0.46 | −1.03 to 0.12 | 0.12 |
| Kim Y et al. (2018) | 557 | Whole blood (early pregnancy) | μg/L | BSID-II: MDI | 36 months | −0.28 | −0.89 to 0.32 | 0.36 |
| Kim Y et al. (2018) | 460 | Whole blood (late pregnancy) | μg/L | BSID-II: MDI | 36 months | −0.25 | −0.88 to 0.38 | 0.43 |
| Kim Y et al. (2018) | 847 | Whole blood (early pregnancy) | μg/L | BSID-II: MDI | 6 months | −0.41 | −0.81 to −0.003 | 0.048 |
| Kim Y et al. (2018) | 689 | Whole blood (late pregnancy) | μg/L | BSID-II: MDI | 6 months | −0.13 | −0.56 to 0.29 | 0.54 |
| Llop et al. (2012) | 1683 | Umbilical cord | Ln µg/L | BSID-II: MDI | 14 months | 0.16 | −0.12 to 0.45 | |
| Rothenberg et al. (2016) | 270 | Hair | Ln μg/g | BSID-II: MDI | 12 months | −4.9 | −9.7 to −0.1 |
| Study | n | Exposure | Units | Outcome | Time of Outcome | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Barbone et al. (2019) | 1083 | Hair | ng/g | Bayley-III: Cognitive composite | 18 months | 0.2 | −0.29 to 0.69 | |
| Barbone et al. (2019) | 829 | Umbilical cord | ng/g | Bayley-III: Cognitive composite | 18 months | 0.13 | −0.39 to 0.64 | |
| Barbone et al. (2019) | 636 | Whole blood | ng/g | Bayley-III: Cognitive composite | 18 months | −0.09 | −0.61 to 0.43 | |
| Boucher et al. (2014) | 77 | Umbilical cord | ln μg/L | A-not-B: 2 correct | 11 months | −0.25 | −0.46 to 0.00 | |
| Boucher et al. (2014) | 77 | Umbilical cord | ln μg/L | A-not-B: 3 correct | 11 months | −0.22 | −0.45 to 0.03 | |
| Boucher et al. (2014) | 73 | Umbilical cord | ln μg/L | Perseverative errors | 11 months | −0.21 | −0.53 to 0.09 | |
| Boucher et al. (2014) | 89 | Umbilical cord | ln μg/L | FTII: Novelty preference | 6.5 months | 0.0 | −0.19 to 0.19 | |
| Boucher et al. (2014) | 89 | Umbilical cord | ln μg/L | FTIII: Fixation duration | 6.5 months | 0.13 | −0.03 to 0.29 | |
| Lin et al. (2013) | 230 | Umbilical cord | Hg ≥ 19.78 μg/L | CDIIT: Cognitive | 24 months | 0.09 | NS | |
| Nisevic et al. (2019) | 257 | Umbilical cord | μg/L | Bayley-III: Cognitive composite | 18 months | 0.14 | 0.34 | |
| Oken et al. (2008) | 341 | Erythrocyte | ng/g | WRAVMA matching | 36 months | −0.2 | −0.6 to 0.2 | |
| Valent et al. (2013) | 505 | Hair | Ln ng/g | Bayley-III: Cognitive composite | 18 months | −0.002 | 0.99 | |
| Valent et al. (2013) | 378 | Umbilical cord | Ln ng/g | Bayley-III: Cognitive composite | 18 months | 0.05 | 0.92 | |
| Xu et al. (2016) | 270 | Umbilical cord | μg/L | NNNS: Attention | 5 weeks | 0.12 | 0.23 | |
| Xu et al. (2016) | 344 | Whole blood | μg/L | NNNS: Attention | 5 weeks | 0.15 | 0.22 |
| Study | n | Exposure | Units | Outcome | Time of Outcome | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Barbone et al. (2019) | 1082 | Hair | ng/g | Bayley-III: Fine Motor scale | 18 months | −0.03 | −0.11 to 0.06 | |
| Barbone et al. (2019) | 1081 | Hair | ng/g | Bayley-III: Gross Motor scale | 18 months | −0.01 | −0.07 to 0.05 | |
| Barbone et al. (2019) | 1083 | Hair | ng/g | Bayley-III: Motor development | 18 months | −0.12 | −0.47 to 0.22 | |
| Barbone et al. (2019) | 635 | Umbilical cord | ng/g | Bayley-III: Gross Motor scale | 18 months | −0.02 | −0.08 to 0.05 | |
| Barbone et al. (2019) | 892 | Umbilical cord | ng/g | Bayley-III: Motor development | 18 months | −0.11 | −0.47 to 0.25 | |
| Barbone et al. (2019) | 636 | Whole blood | ng/g | Bayley-III: Fine Motor scale | 18 months | 0.05 | −0.04 to 0.15 | |
| Barbone et al. (2019) | 890 | Whole blood | ng/g | Bayley-III: Gross Motor scale | 18 months | −0.03 | −0.09 to 0.03 | |
| Barbone et al. (2019) | 636 | Whole blood | ng/g | Bayley-III: Motor development | 18 months | 0.11 | −0.25 to 0.48 | |
| Boucher et al. (2014) | 87 | Umbilical cord | ln μg/L | BSID-II: PDI | 11 months | 0.01 | −0.24 to 0.25 | |
| Hu et al. (2016) | 410 | Umbilical cord | Ln μg/L | GDS: Fine motor domain | 12 months | −2.62 | −7.78 to 2.55 | |
| Hu et al. (2016) | 410 | Umbilical cord | Ln μg/L | GDS: Gross motor domain | 12 months | 1.95 | −3.08 to 6.98 | |
| Hu et al. (2016) | 410 | Whole blood | Ln μg/L | GDS: Fine motor domain | 12 months | 2.69 | −3.37 to 8.74 | |
| Hu et al. (2016) | 410 | Whole blood | Ln μg/L | GDS: Gross motor domain | 12 months | 3.26 | −2.72 to 9.24 | |
| Kim Y et al. (2018) | 595 | Umbilical cord | μg/L | BSID-II: PDI | 12 months | 0.14 | −0.23 to 0.52 | 0.45 |
| Kim Y et al. (2018) | 523 | Umbilical cord | μg/L | BSID-II: PDI | 24 months | 0.16 | −0.17 to 0.48 | 0.34 |
| Kim Y et al. (2018) | 438 | Umbilical cord | μg/L | BSID-II: PDI | 36 months | −0.13 | −0.55 to 0.27 | 0.53 |
| Kim Y et al. (2018) | 662 | Umbilical cord | μg/L | BSID-II: PDI | 6 months | −0.2 | −0.45 to 0.15 | 0.33 |
| Kim Y et al. (2018) | 763 | Whole blood (early pregnancy) | μg/L | BSID-II: PDI | 12 months | 0.3 | −0.31 to 0.91 | 0.34 |
| Kim Y et al. (2018) | 614 | Whole blood (late pregnancy) | μg/L | BSID-II: PDI | 12 months | 0.27 | −0.38 to 0.93 | 0.41 |
| Kim Y et al. (2018) | 686 | Whole blood (early pregnancy) | μg/L | BSID-II: PDI | 24 months | −0.17 | −0.74 to 0.4 | 0.56 |
| Kim Y et al. (2018) | 564 | Whole blood (late pregnancy) | μg/L | BSID-II: PDI | 24 months | −0.09 | −0.67 to 0.48 | 0.75 |
| Kim Y et al. (2018) | 557 | Whole blood (early pregnancy) | μg/L | BSID-II: PDI | 36 months | −0.11 | −0.7 to 0.47 | 0.70 |
| Kim Y et al. (2018) | 460 | Whole blood (late pregnancy) | μg/L | BSID-II: PDI | 36 months | −0.58 | −1.19 to 0.03 | 0.06 |
| Kim Y et al. (2018) | 847 | Whole blood (early pregnancy) | μg/L | BSID-II: PDI | 6 months | −0.55 | −1.05 to −0.05 | 0.03 |
| Kim Y et al. (2018) | 689 | Whole blood (late pregnancy) | μg/L | BSID-II: PDI | 6 months | −0.27 | −0.78 to 0.25 | 0.31 |
| Llop et al. (2012) | 1683 | Umbilical cord | Ln µg/L | BSID-II: PDI | 14 months | −0.05 | −0.79 to 0.68 | |
| Nisevic et al. (2019) | 257 | Umbilical cord | μg/L | Bayley-III: Fine Motor scale | 18 months | −0.07 | 0.78 | |
| Nisevic et al. (2019) | 257 | Umbilical cord | μg/L | Bayley-III: Gross Motor scale | 18 months | 0.08 | 0.71 | |
| Nisevic et al. (2019) | 257 | Umbilical cord | μg/L | Bayley-III: Motor development | 18 months | 0.01 | 0.92 | |
| Oken et al. (2008) | 341 | Erythrocyte | ng/g | WRAVMA drawing | 36 months | 0.1 | −0.2 to 0.4 | |
| Oken et al. (2008) | 341 | Erythrocyte | ng/g | WRAVMA pegboard | 36 months | 0.03 | −0.3 to 0.3 | |
| Rothenberg et al. (2016) | 270 | Hair | Ln μg/g | BSID-II: PDI | 12 months | −2.7 | −8.3 to 2.9 | |
| Tatsuta et al. (2017) | 566 | Umbilical cord | Ln ng/g | BSID-II: PDI | 18 months | −0.12 | 0.009 | |
| Valent et al. (2013) | 505 | Hair | Ln ng/g | Bayley-III: Motor development | 18 months | −0.19 | 0.62 | |
| Valent et al. (2013) | 378 | Umbilical cord | Ln ng/g | Bayley-III: Motor development | 18 months | 0.16 | 0.68 | |
| Xu et al. (2016) | 270 | Umbilical cord | μg/L | NNNS: Asymmetry (Male) | 5 weeks | 0.1 | 0.36 | |
| Xu et al. (2016) | 270 | Umbilical cord | μg/L | NNNS: Asymmetry (Female) | 5 weeks | 0.07 | 0.4 | |
| Xu et al. (2016) | 270 | Umbilical cord | μg/L | NNNS: Handling | 5 weeks | −0.02 | 0.35 | |
| Xu et al. (2016) | 344 | Whole blood | μg/L | NNNS: Asymmetry (Male) | 5 weeks | −0.13 | 0.3 | |
| Xu et al. (2016) | 344 | Whole blood (Female) | μg/L | NNNS: Asymmetry (Female) | 5 weeks | 0.08 | 0.43 | |
| Xu et al. (2016) | 344 | Whole blood | μg/L | NNNS: Handling | 5 weeks | −0.001 | 0.98 |
| Study | n | Exposure | Units | Outcome | Time of Outcome | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Barbone et al. (2019) | 1272 | Hair | ng/g | Bayley-III: Expressive Communication scale | 18 months | 0.04 | −0.06 to 0.13 | |
| Barbone et al. (2019) | 1086 | Hair | ng/g | Bayley-III: Language composite | 18 months | 0.55 | 0.05 to 1.05 | |
| Barbone et al. (2019) | 1075 | Hair | ng/g | Bayley-III: Receptive Communication scale | 18 months | 0.12 | 0.02 to 0.22 | |
| Barbone et al. (2019) | 1070 | Umbilical cord | ng/g | Bayley-III: Expressive Communication scale | 18 months | 0.01 | −0.09 to 0.11 | |
| Barbone et al. (2019) | 896 | Umbilical cord | ng/g | Bayley-III: Language composite | 18 months | 0.25 | −0.29 to 0.78 | |
| Barbone et al. (2019) | 887 | Umbilical cord | ng/g | Bayley-III: Receptive Communication scale | 18 months | 0.12 | −0.08 to 0.32 | |
| Barbone et al. (2019) | 727 | Whole blood | ng/g | Bayley-III: Expressive Communication scale | 18 months | 0.13 | −0.22 to 0.48 | |
| Barbone et al. (2019) | 628 | Whole blood | ng/g | Bayley-III: Receptive Communication scale | 18 months | −0.02 | −0.12 to 0.08 | |
| Daniels et al. (2004) | 1054 | Umbilical cord | μg/g | MCDI: Vocabulary Comprehension | 15 months | 6.1 | 0.8 | |
| Daniels et al. (2004) | 1054 | Umbilical cord | μg/g | DDST: Language | 18 months | 0.1 | 0.9 | |
| Hu et al. (2016) | 410 | Umbilical cord | Ln μg/L | GDS: Language domain | 12 months | 2.17 | −1.88 to 6.21 | |
| Hu et al. (2016) | 410 | Whole blood | Ln μg/L | GDS: Language domain | 12 months | 1.92 | −3.61 to 7.46 | |
| Nisevic et al. (2019) | 257 | Umbilical cord | μg/L | Bayley-III: Language composite | 18 months | −0.05 | 0.74 | |
| Oken et al. (2008) | 341 | Erythrocyte | ng/g | PPVT | 36 months | −0.4 | −0.8 to −0.1 | |
| Valent et al. (2013) | 505 | Hair | Ln ng/g | Bayley-III: Language composite | 18 months | 0.85 | 0.11 | |
| Valent et al. (2013) | 378 | Umbilical cord | Ln ng/g | Bayley-III: Language composite | 18 months | 0.41 | 0.46 |
| Study | n | Exposure | Units | Outcome | Time of Outcome | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Daniels et al. (2004) | 1054 | Umbilical cord | μg/g | MCDI: Social activity | 15 months | −0.2 | 0.9 | |
| Daniels et al. (2004) | 1054 | Umbilical cord | μg/g | DDST: Social Activity | 18 months | 0.5 | 0.8 | |
| Hu et al. (2016) | 410 | Umbilical cord | Ln μg/L | GDS: Social domain | 12 months | 4.06 | 0.51 to 7.62 | |
| Hu et al. (2016) | 410 | Whole blood | Ln μg/L | GDS: Social domain | 12 months | 0.74 | −5.77 to 4.31 | |
| Valent et al. (2013) | 505 | Hair | Ln ng/g | Bayley-III: Social-emotional | 18 months | 1.77 | 0.11 | |
| Valent et al. (2013) | 378 | Umbilical cord | Ln ng/g | Bayley-III: Social-emotional | 18 months | −0.07 | 0.95 |
| Study | n | Exposure | Units | Outcome | Time of Outcome | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Daniels et al. (2004) | 1054 | Umbilical cord | μg/g | DDST: Total | 18 months | 0.4 | 0.9 | |
| Golding et al. (2016) | 2643 | Whole blood | μg/L | DDST-II | 18 months | 0.49 | 0.1 to 0.88 | 0.01 |
| Golding et al. (2016) | 2452 | Whole blood | μg/L | DDST-II | 30 months | 0.23 | −0.08 to 0.53 | 0.15 |
| Golding et al. (2016) | 2394 | Whole blood | μg/L | DDST-II | 32 months | 0.43 | 0.08 to 0.78 | 0.02 |
| Golding et al. (2016) | 2721 | Whole blood | μg/L | DDST-II | 6 months | 0.51 | 0.05 to 1 | 0.03 |
| Hu et al. (2016) | 410 | Umbilical cord | Ln μg/L | GDS: Adaptive domain | 12 months | 4.22 | 0.77 to 7.67 | |
| Hu et al. (2016) | 410 | Whole blood | Ln μg/L | GDS: Adaptive domain | 12 months | 0.65 | −4.3 to 5.59 | |
| Oken et al. (2008) | 341 | Erythrocyte | ng/g | WRAVMA total | 36 months | −0.06 | −0.4 to 0.2 | |
| Suzuki et al. (2010) | 498 | Hair | μg/g | NBAS | 3 days | −0.12 | <0.05 | |
| Valent et al. (2013) | 362 | Hair | Ln ng/g | Bayley-III: Adaptive behaviour | 18 months | 0.55 | 0.56 | |
| Valent et al. (2013) | 271 | Umbilical cord | Ln ng/g | Bayley-III: Adaptive behaviour | 18 months | −0.57 | −0.15 to 0.33 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dack, K.; Fell, M.; Taylor, C.M.; Havdahl, A.; Lewis, S.J. Prenatal Mercury Exposure and Neurodevelopment up to the Age of 5 Years: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 1976. https://doi.org/10.3390/ijerph19041976
Dack K, Fell M, Taylor CM, Havdahl A, Lewis SJ. Prenatal Mercury Exposure and Neurodevelopment up to the Age of 5 Years: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(4):1976. https://doi.org/10.3390/ijerph19041976
Chicago/Turabian StyleDack, Kyle, Matthew Fell, Caroline M. Taylor, Alexandra Havdahl, and Sarah J. Lewis. 2022. "Prenatal Mercury Exposure and Neurodevelopment up to the Age of 5 Years: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 4: 1976. https://doi.org/10.3390/ijerph19041976
APA StyleDack, K., Fell, M., Taylor, C. M., Havdahl, A., & Lewis, S. J. (2022). Prenatal Mercury Exposure and Neurodevelopment up to the Age of 5 Years: A Systematic Review. International Journal of Environmental Research and Public Health, 19(4), 1976. https://doi.org/10.3390/ijerph19041976