
The Impact of the COVID-19 Pandemic on Israeli Orthodontic Practice: A Clinic’s Activity and Patients’ Attitudes


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Appointment Logs
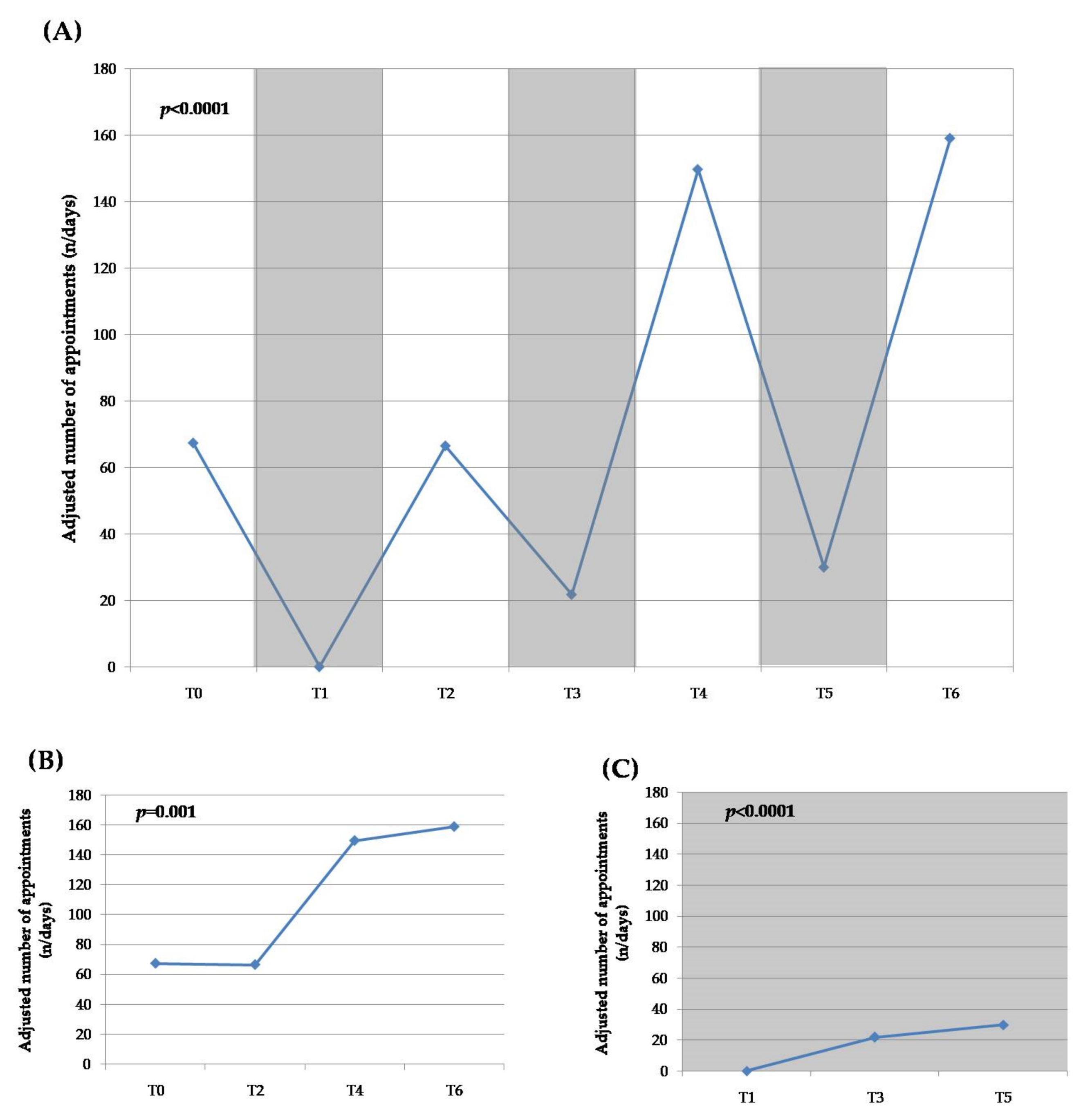
- T0—the pre-pandemic and pre-lockdown situation: 1 January–18 March 2020 (78 days);
- T1—the first lockdown (extreme lockdown): 19 March–7 May 2020 (50 days);
- T2—the first inter-lockdown period: 8 May–17 September 2020 (133 days);
- T3—the second lockdown: 18 September–17 November 2020 (61 days);
- T4—the second inter-lockdown period: 18 November–26 December 2020 (39 days);
- T5—the third lockdown: 27 December 2020–7 February 2021 (43 days);
- T6—the post-lockdown period: 8 February–8 March 2021 (29 days).
- The total number of appointments: a count of all scheduled appointments during the specified period;
- The adjusted number of appointments: the number of scheduled appointments relative to the period duration; this was calculated by dividing the total number of appointments by the number of days for the specified period;
- The number of missed appointments: a count of the missed and canceled appointments by either patients or orthodontists during a specified period;
- The number of emergency visits: the number of unscheduled appointments for a specified period;
- The percentage of missed appointments and emergency visits; they were calculated as the proportion of missed appointments and emergency visits from the total number of appointments in the specified period.
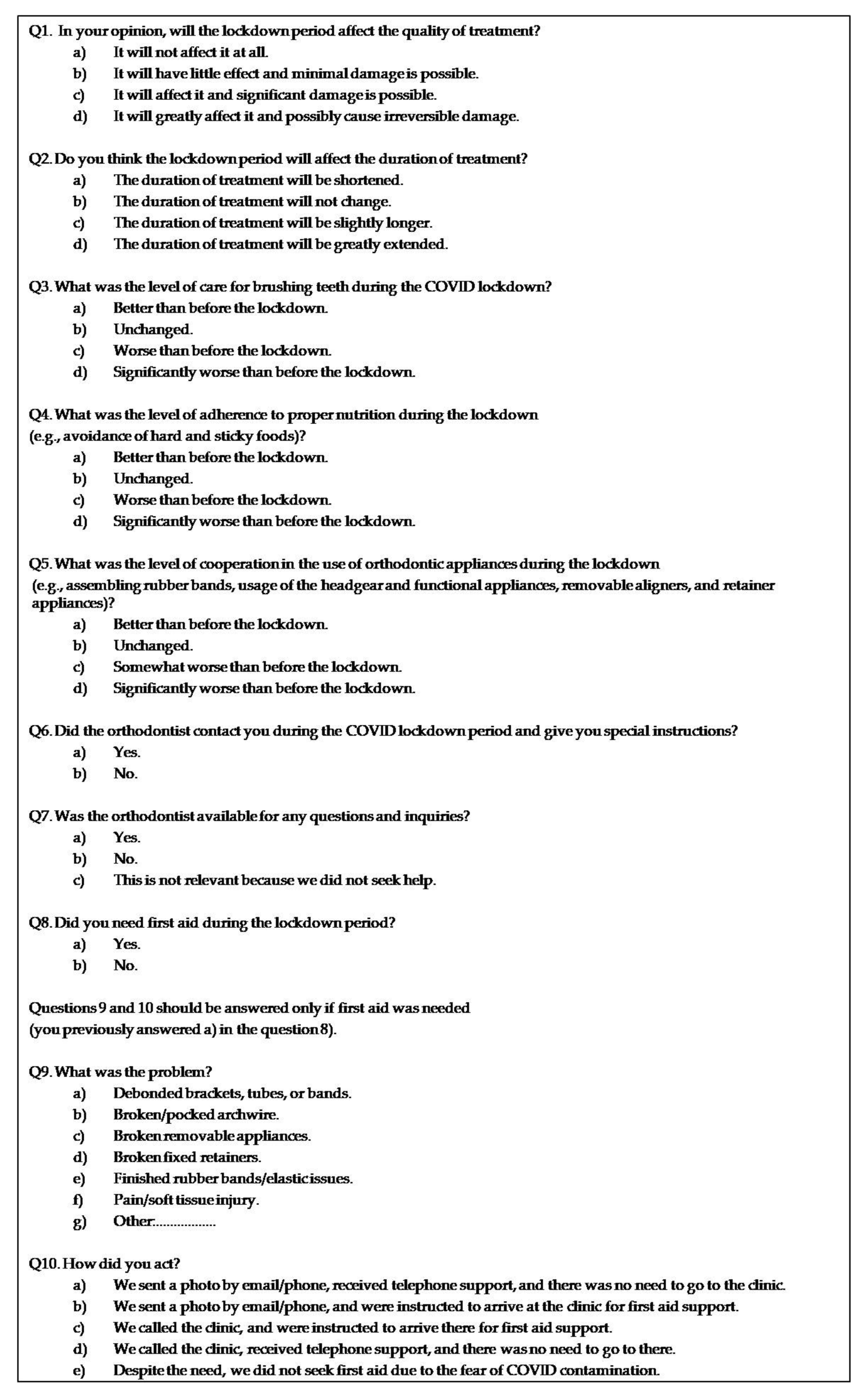
2.3. Questionnaire
2.4. Validation of the Questionnaire
2.5. Statistical Analysis
3. Results
3.1. Appointment Logs
3.2. Questionnaire
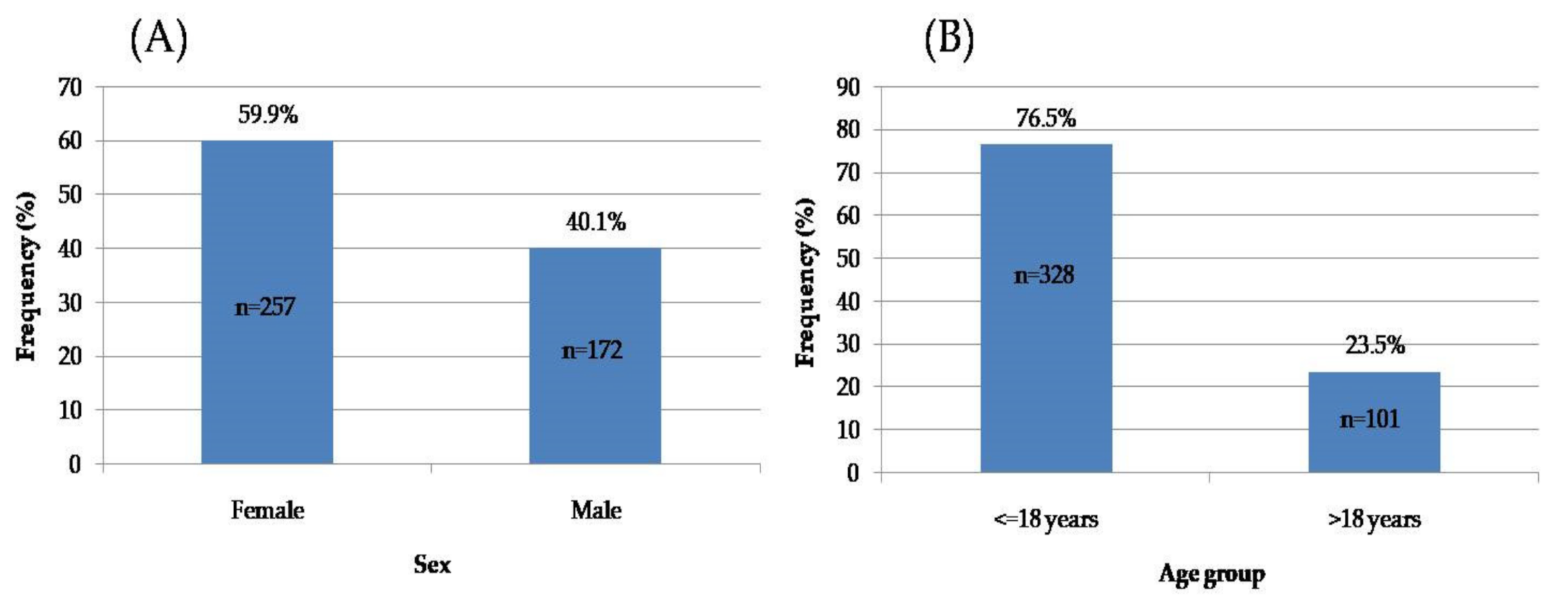
3.2.1. Subjects’ Sex and Age
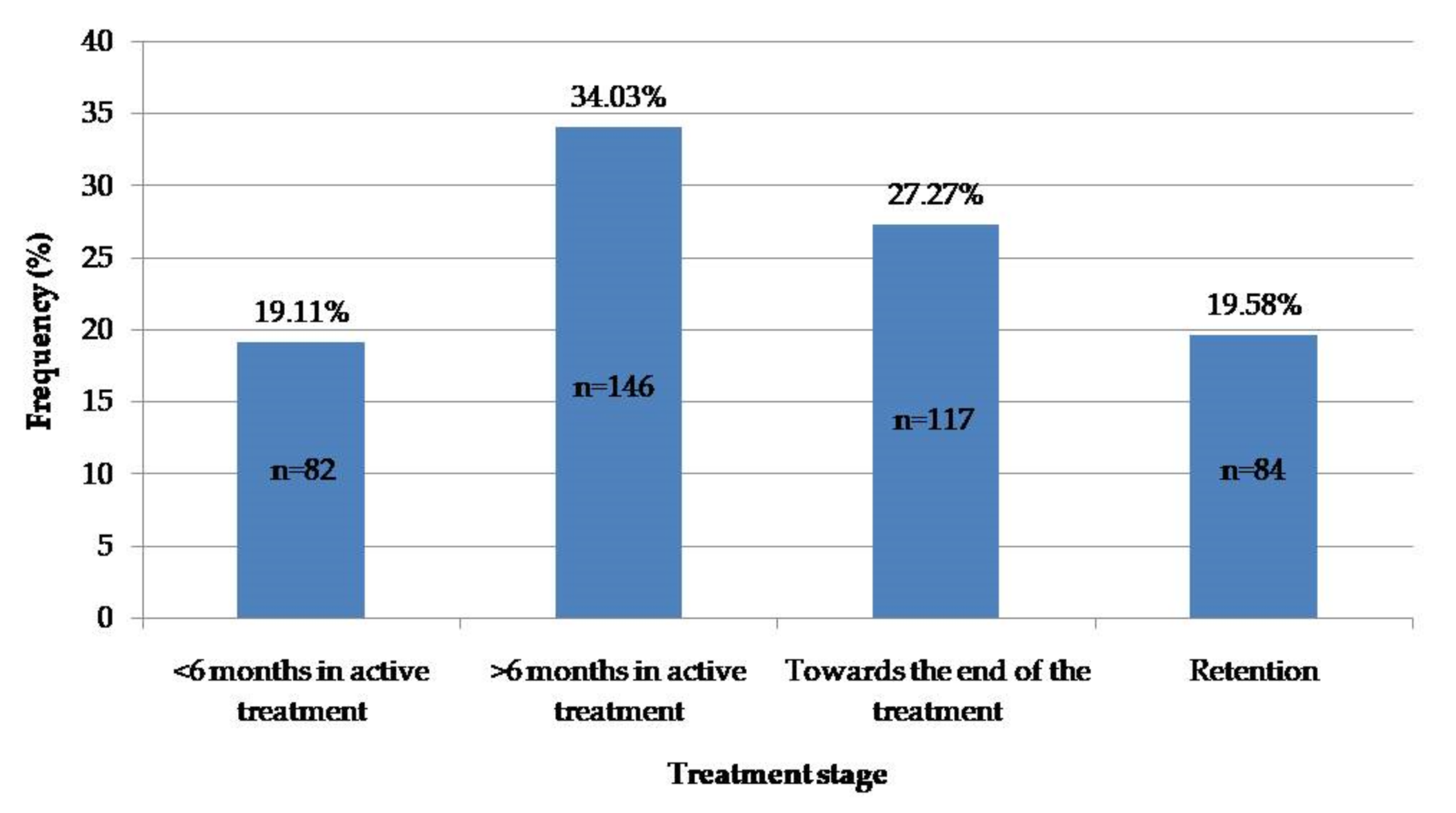
3.2.2. Subjects’ Treatment Stage
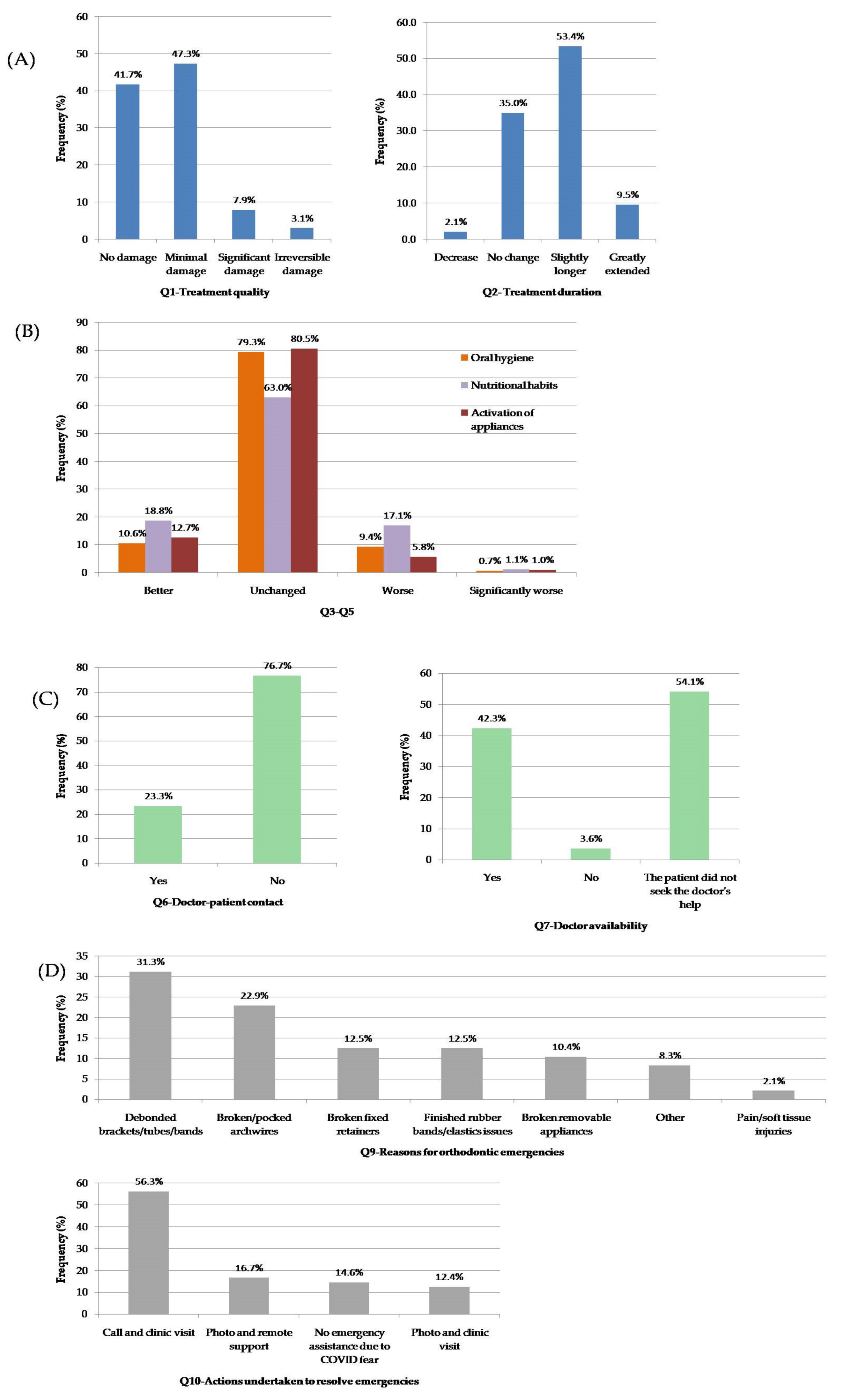
3.2.3. Subjects’ Responses
- Cluster 1 (Q1–Q2): Patients’ concerns and expectations (Figure 5A).
- Cluster 2 (Q3–Q5): Cooperation with the treatment protocol (Figure 5B).
- Cluster 3 (Q6–Q7): Contact with the orthodontist in dental care (Figure 5C).
- Cluster 4 (Q8–10): Emergency issues (Figure 5D).
4. Discussion
4.1. Orthodontic Clinics’ Activity and Patients’ Attitudes
4.2. Orthodontic Emergencies and Doctor Availability
5. Limitations of the Study
6. Conclusions
- Orthodontic clinics were able to operate at their full capacity between periods of lockdowns but needed to adhere to strict measures to reduce the risk of infection to both patients and staff.
- No significant change in the number of missed and canceled appointments was found during the pandemic.
- A majority of orthodontic patients believed that the length and quality of their treatment may be slightly affected due to the pandemic, and a small minority (10%) expected that significant and irreversible damage would occur, in addition to an extended treatment duration.
- The stage of the treatment was associated with patients’ anxieties and expectations; namely, the patients who approached the end of their treatment exhibited greater anxiety regarding the possibility of an extended treatment time.
- A significant increase in the number of orthodontic emergency appointments during lockdowns was not found in the current study.
- The remote monitoring of patients using various telecommunication tools is helpful, but it was found to be insufficient to manage the majority of the treatment emergencies. The main reason for unscheduled appointments was technical issues with an orthodontic appliance, which preferably should be solved by an expert within a clinic.
- Reducing the occurrence of orthodontic emergencies may reduce patients’ fears and may provide patients with greater motivation for improved cooperation during the lockdown period.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Duryea, M.; Huang, G.; Kadioglu, O.; Mah, J.; Palomo, J.M.; Rossouw, E.; Stappert, D.; Stewart, K.; Tufekci, E. COVID-19: What do we know? Am. J. Orthod. Dentofac. Orthop. 2020, 158, e53–e62. [Google Scholar] [CrossRef] [PubMed]
- Falahchai, M.; Babaee Hemmati, Y.; Hasanzade, M. Dental care management during the COVID-19 outbreak. Spec. Care Dentist. 2020, 40, 539–548. [Google Scholar] [CrossRef]
- Dongarwar, D.; Salihu, H.M. COVID-19 pandemic: Marked global disparities in fatalities according to geographic location and universal health care. Int. J. Matern. Child Health AIDS 2020, 9, 213–216. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Alibrahim, H.; Al Madani, A.; Alamri, A.; Bamashmous, M.; Tounsi, A. Fear factor in seeking dental care among Saudis during COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10589. [Google Scholar] [CrossRef]
- Yavan, M. First clinical appointment after the COVID-19 lockdown: Reflections from orthodontic patients and their anxiety levels. Turk. J. Orthod. 2021, 34, 86–92. [Google Scholar] [CrossRef]
- Peloso, R.M.; Pini, N.I.P.; Sundfeld Neto, D.; Mori, A.A.; Oliveira, R.C.G.D.; Valarelli, F.P.; Freitas, K.M.S. How does the quarantine resulting from COVID-19 impact dental appointments and patient anxiety levels? Braz. Oral Res. 2020, 34, e84. [Google Scholar] [CrossRef]
- Cotrin, P.; Peloso, R.M.; Oliveira, R.C.; de Oliveira, R.C.G.; Pini, N.I.P.; Valarelli, F.P.; Freitas, K.M.S. Impact of coronavirus pandemic in appointments and anxiety/concerns of patients regarding orthodontic treatment. Orthod. Craniofac. Res. 2020, 23, 455–461. [Google Scholar] [CrossRef]
- Martina, S.; Amato, A.; Rongo, R.; Caggiano, M.; Amato, M. The perception of COVID-19 among Italian dentists: An orthodontic point of view. Int. J. Environ. Res. Public Health 2020, 17, 4384. [Google Scholar] [CrossRef]
- León-Manco, R.A.; Agudelo-Suárez, A.A.; Armas-Vega, A.; Figueiredo, M.C.; Verdugo-Paiva, F.; Santana-Pérez, Y.; Viteri-García, A. Perceived stress in dentists and dental students of Latin America and the Caribbean during the mandatory social isolation measures for the COVID-19 pandemic: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 5889. [Google Scholar] [CrossRef] [PubMed]
- Mekhemar, M.; Attia, S.; Dörfer, C.; Conrad, J. Dental nurses’ mental health in Germany: A nationwide survey during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 8108. [Google Scholar] [CrossRef] [PubMed]
- Shavit, T.; Sherman, A.; Aisenberg, D. The effects of the COVID-19 crisis on the subjective well-being of the Israeli population-monitored phase by phase. Curr. Psychol. 2021, 12, 6300–6307. [Google Scholar] [CrossRef] [PubMed]
- Lipskaya-Velikovsky, L. COVID-19 isolation in healthy population in Israel: Challenges in daily life, mental health, resilience, and quality of life. Int. J. Environ. Res. Public Health 2021, 18, 999. [Google Scholar] [CrossRef]
- Haklai, Z.; Aburbeh, M.; Goldberger, N.; Gordon, E.S. Excess mortality during the COVID-19 pandemic in Israel, March-November 2020: When, where, and for whom? Isr. J. Health Policy Res. 2021, 10, 17. [Google Scholar] [CrossRef]
- Somekh, I.; Simões, E.A.F.; Somekh, E. Coronavirus disease spread during summer vacation, Israel, 2020. Emerg. Infect. Dis. 2022, 28, 188–191. [Google Scholar] [CrossRef]
- Nir, Y.F.; Levy, Y.; Gutkind, A.; Grossman, E. The effect of the COVID-19 pandemic on patient visits to the emergency department and hospitalizations in medical wards in an Israeli medical center. Isr. J. Health Policy Res. 2021, 10, 62. [Google Scholar]
- Caprioglio, A.; Pizzetti, G.B.; Zecca, P.A.; Fastuca, R.; Maino, G.; Nanda, R. Management of orthodontic emergencies during 2019-NCOV. Prog. Orthod. 2020, 21, 10. [Google Scholar] [CrossRef] [Green Version]
- Turkistani, K.A. Precautions and recommendations for orthodontic settings during the COVID-19 outbreak: A review. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 175–181. [Google Scholar] [CrossRef]
- Saltaji, H.; Sharaf, K.A. COVID-19 and orthodontics-A call for action. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 12–13. [Google Scholar] [CrossRef]
- Carter, A. Can orthodontic care be safely delivered during the COVID-19 pandemic? Recommendations from a literature review. Evid. Based Dent. 2020, 21, 66–67. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.; Parschal, J.; Paquette, D. Proposed clinical guidance for orthodontists and orthodontic staff in the post-COVID-19 environment: A clinician’s perspective. J. Clin. Orthod. 2020, 52, 264–267. [Google Scholar] [PubMed]
- Xiong, X.; Wu, Y.; Fang, X.; Sun, W.; Ding, Q.; Yi, Y.; Huang, Y.; Gong, J.; Liu, J.; Wang, J. Mental distress in orthodontic patients during the coronavirus disease 2019 pandemic. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 824–833.e1. [Google Scholar] [CrossRef] [PubMed]
- Cotrin, P.; Peloso, R.M.; Pini, N.I.P.; Oliveira, R.C.; de Oliveira, R.C.G.; Valarelli, F.P.; Freitas, K.M.S. Urgencies and emergencies in orthodontics during the coronavirus disease 2019 pandemic: Brazilian orthodontists’ experience. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 661–667. [Google Scholar] [CrossRef]
- Turkistani, K.A. Impact of delayed orthodontic care during COVID-19 pandemic: Emergency, disability, and pain. J. World Fed. Orthod. 2020, 9, 106–111. [Google Scholar] [CrossRef]
- Umeh, O.D.; Utomi, I.L.; Isiekwe, I.G.; Aladenika, E.T. Impact of the coronavirus disease 2019 pandemic on orthodontic patients and their attitude to orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e399–e409. [Google Scholar] [CrossRef]
- Natapov, L.; Schwartz, D.; Herman, H.D.; Markovich, D.D.; Yellon, D.; Jarallah, M.; Liphshiz, I.; Carmeli, Y.; Karakis, I. Risk of SARS-CoV-2 transmission following exposure during dental treatment—A national cohort study. J. Dent. 2021, 113, 103791. [Google Scholar] [CrossRef]
- Lucaciu, O.; Boca, A.; Mesaros, A.S.; Petrescu, N.; Aghiorghiesei, O.; Mirica, I.C.; Hosu, I.; Armencea, G.; Bran, S.; Dinu, C.M. Assessing SARS-CoV-2 infection rate among Romanian dental practitioners. Int. J. Environ. Res. Public Health 2021, 18, 4897. [Google Scholar] [CrossRef]
- Krishnan, B.; Raman, R.; Nirupama, C.; Gunasekaran, R.; Asokan, B.K.; Ravi, K. COVID-19–challenge to orthodontic management in virtual era. J. Cont. Orthod. 2020, 4, 16–20. [Google Scholar]
- Valekar, S.; Manikandan, J.; Phaphe, S. COVID-19 lockdown and its impact on orthodontic patients. Int. Dent. J. Stud. Res. 2021, 8, 152–157. [Google Scholar]
- Sangalli, L.; Savoldi, F.; Dalessandri, D.; Bonetti, S.; Gu, M.; Signoroni, A.; Paganelli, C. Effects of remote digital monitoring on oral hygiene of orthodontic patients: A prospective study. BMC Oral Health 2021, 21, 435. [Google Scholar] [CrossRef] [PubMed]
- Quan, S.; Guo, Y.; Zhou, J.; Zhang, G.; Xing, K.; Mei, H.; Li, J. Orthodontic emergencies and mental state of Chinese orthodontic patients during the COVID-19 pandemic. BMC Oral Health 2021, 21, 477. [Google Scholar] [CrossRef] [PubMed]
- Popat, H.; Thomas, K.; Farnell, D.J. Management of orthodontic emergencies in primary care-self-reported confidence of general dental practitioners. Br. Dent. J. 2016, 221, 21–24. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T-Period | Duration (Days) | Appointments (n) | Adjusted Appointments (n/Days) | Missed Appointments (% *) | Emergency Visits (% *) |
|---|---|---|---|---|---|
| T0 | 78 | 5252 | 67.33 | 539 (10.3%) | 238 (4.5%) |
| T1 | 50 | 0 | 0 | 0 | 88 |
| T2 | 133 | 8842 | 66.48 | 813 (9.2%) | 326 (3.7%) |
| T3 | 61 | 1325 | 21.72 | 114 (8.6%) | 58 (4.4%) |
| T4 | 39 | 5836 | 149.64 | 554 (9.5%) | 194 (3.3%) |
| T5 | 43 | 1287 | 29.93 | 129 (10.0%) | 62 (4.8%) |
| T6 | 29 | 4611 | 159.00 | 402 (8.7%) | 158 (3.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sella Tunis, T.; Ratson, T.; Matalon, S.; Abba, M.; Abramson, A.; Davidovitch, M.; Shpack, N. The Impact of the COVID-19 Pandemic on Israeli Orthodontic Practice: A Clinic’s Activity and Patients’ Attitudes. Int. J. Environ. Res. Public Health 2022, 19, 1965. https://doi.org/10.3390/ijerph19041965
Sella Tunis T, Ratson T, Matalon S, Abba M, Abramson A, Davidovitch M, Shpack N. The Impact of the COVID-19 Pandemic on Israeli Orthodontic Practice: A Clinic’s Activity and Patients’ Attitudes. International Journal of Environmental Research and Public Health. 2022; 19(4):1965. https://doi.org/10.3390/ijerph19041965
Chicago/Turabian StyleSella Tunis, Tatiana, Tal Ratson, Shlomo Matalon, Michael Abba, Alex Abramson, Moshe Davidovitch, and Nir Shpack. 2022. "The Impact of the COVID-19 Pandemic on Israeli Orthodontic Practice: A Clinic’s Activity and Patients’ Attitudes" International Journal of Environmental Research and Public Health 19, no. 4: 1965. https://doi.org/10.3390/ijerph19041965
APA StyleSella Tunis, T., Ratson, T., Matalon, S., Abba, M., Abramson, A., Davidovitch, M., & Shpack, N. (2022). The Impact of the COVID-19 Pandemic on Israeli Orthodontic Practice: A Clinic’s Activity and Patients’ Attitudes. International Journal of Environmental Research and Public Health, 19(4), 1965. https://doi.org/10.3390/ijerph19041965