
A Cross-Sectional Study of Exposure Factors Associated with Seropositivity for SARS-CoV-2 Antibodies during the Second Epidemic Wave among a Sample of the University of Corsica (France)

 , , , , , , ,
, , , , , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Timeline
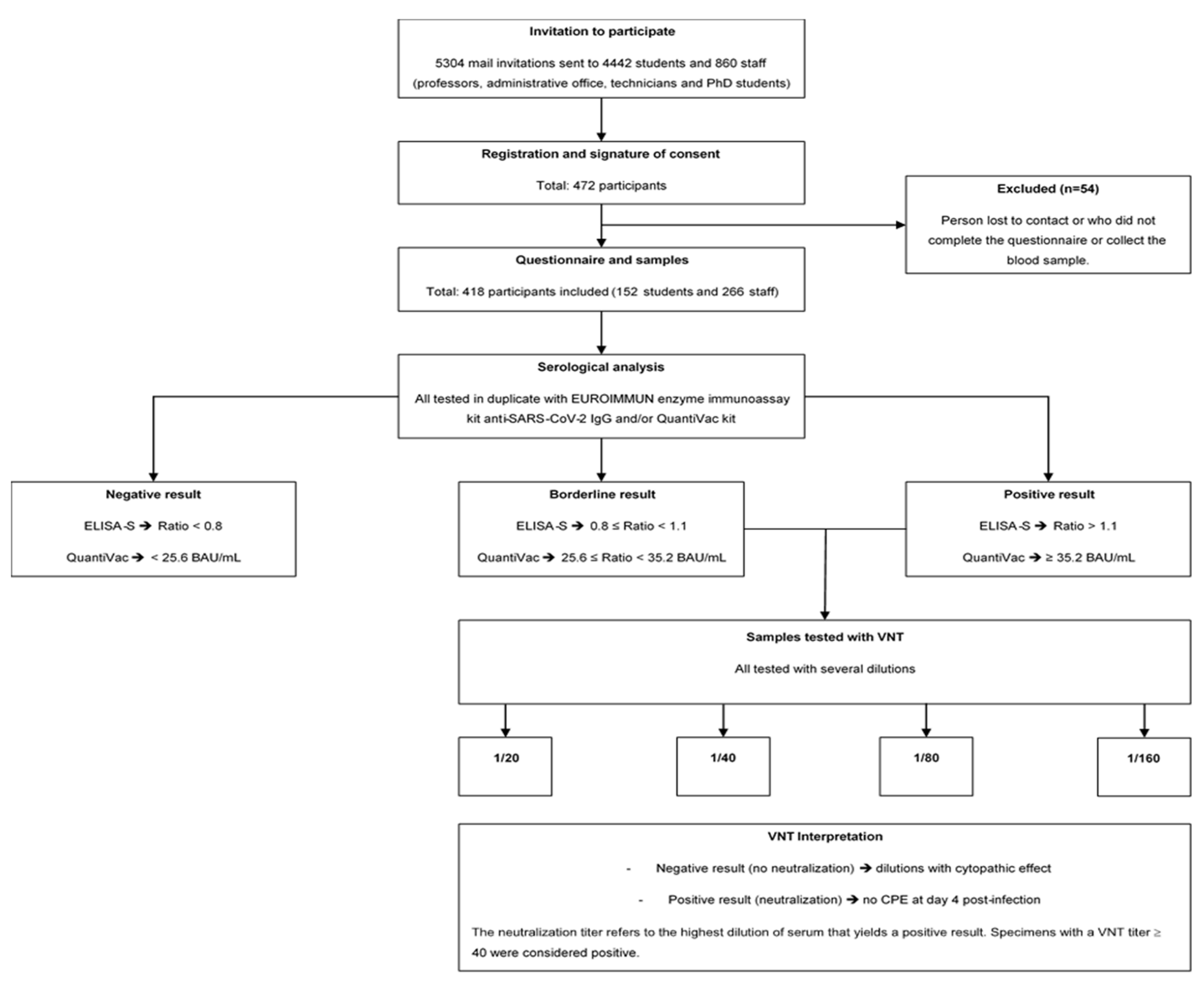
2.2. Study Design
2.3. Participants
2.4. Outcomes
2.5. Serological Analysis
2.6. Statistical Analysis
2.6.1. Sample-Size Calculation
2.6.2. Analysis of Seroprevalence and Epidemiological Factors
2.7. Ethics
3. Results
3.1. Sociodemographic Data Description
3.2. Symptoms and SARS-CoV-2 History
3.3. Seroprevalence of IgG Antibodies against SARS-CoV-2
3.4. Quantitative Results
3.5. Seroneutralization Results
3.6. Sociobehavioral Characteristics of the Population
3.7. Association between Factors and Seropositivity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wood, G. There’s No Simple Way to Reopen Universities. Available online: https://www.theatlantic.com/ideas/archive/2020/04/colleges-are-weighing-costs-reopening-fall/610759/ (accessed on 24 November 2021).
- Vasold, K.L.; Deere, S.J.; Pivarnik, J.M. Club and Intramural Sports Participation and College Student Academic Success. Recreat. Sports J. 2019, 43, 55–66. [Google Scholar] [CrossRef]
- Gostin, L.O.; Wiley, L.F. Governmental Public Health Powers during the COVID-19 Pandemic: Stay-at-Home Orders, Business Closures, and Travel Restrictions. JAMA 2020, 323, 2137. [Google Scholar] [CrossRef] [PubMed]
- Renault, V.; Humblet, M.-F.; Parisi, G.; Donneau, A.-F.; Bureau, F.; Gillet, L.; Fontaine, S.; Saegerman, C. The First Random Observational Survey of Barrier Gestures against COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 9972. [Google Scholar] [CrossRef]
- Tilley, K.; Ayvazyan, V.; Martinez, L.; Nanda, N.; Kawaguchi, E.S.; O’Gorman, M.; Conti, D.; Gauderman, W.J.; Van Orman, S. A Cross-Sectional Study Examining the Seroprevalence of Severe Acute Respiratory Syndrome Coronavirus 2 Antibodies in a University Student Population. J. Adolesc. Health 2020, 67, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Tuells, J.; Egoavil, C.M.; Pena Pardo, M.A.; Montagud, A.C.; Montagud, E.; Caballero, P.; Zapater, P.; Puig-Barberá, J.; Hurtado-Sanchez, J.A. Seroprevalence Study and Cross-Sectional Survey on COVID-19 for a Plan to Reopen the University of Alicante (Spain). Int. J. Environ. Res. Public Health 2021, 18, 1908. [Google Scholar] [CrossRef] [PubMed]
- Araújo, A.A.d.S.; Quintans-Júnior, L.J.; Schimieguel, D.M.; Corrêa, C.B.; de Moura, T.R.; Cavalcante, R.C.M.; Grespan, R.; Cerqueira-Meneses, D.d.V.; Barreto-Alves, J.A.; Martins-Filho, P.R. Seroprevalence of SARS-CoV-2 Antibodies in Low-Income University Students. EXCLI J. 2021, 20, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.R.K.; Srinivasan, S.; Herzog, C.M.; Gontu, A.; Bharti, N.; Small, M.; Rogers, C.J.; Schade, M.M.; Kuchipudi, S.V.; Kapur, V.; et al. SARS-CoV-2 Seroprevalence in a University Community: A Longitudinal Study of the Impact of Student Return to Campus on Infection Risk Among Community Members. medRxiv 2021. 2021.02.17.21251942. [Google Scholar] [CrossRef]
- Tsitsilonis, O.E.; Paraskevis, D.; Lianidou, E.; Pierros, V.; Akalestos, A.; Kastritis, E.; Moutsatsou, P.; Scorilas, A.; Sphicopoulos, T.; Terpos, E.; et al. Seroprevalence of Antibodies against SARS-CoV-2 among the Personnel and Students of the National and Kapodistrian University of Athens, Greece: A Preliminary Report. Life 2020, 10, 214. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological Memory to SARS-CoV-2 Assessed for up to 8 Months after Infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Gallian, P.; Pastorino, B.; Morel, P.; Chiaroni, J.; Ninove, L.; de Lamballerie, X. Lower Prevalence of Antibodies Neutralizing SARS-CoV-2 in Group O French Blood Donors. Antivir. Res. 2020, 181, 104880. [Google Scholar] [CrossRef]
- Capai, L.; Ayhan, N.; Masse, S.; Canarelli, J.; Priet, S.; Simeoni, M.-H.; Charrel, R.; de Lamballerie, X.; Falchi, A. Seroprevalence of SARS-CoV-2 IgG Antibodies in Corsica (France), April and June 2020. J. Clin. Med. 2020, 9, 3569. [Google Scholar] [CrossRef] [PubMed]
- Sergent, E.S.G. Calculateurs Épidémiologiques Epitools. Ausvet. Available online: https://epitools.ausvet.com.au/ (accessed on 22 November 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2006; Available online: https://www.eea.europa.eu/data-and-maps/indicators/oxygen-consuming-substances-in-rivers/r-development-core-team-2006 (accessed on 22 November 2021).
- Capai, L.; Masse, S.; Fourié, T.; Decarreaux, D.; Canarelli, J.; Simeoni, M.-H.; Amroun, A.; Mohammed-Ali, S.; Saba Villarroel, P.M.; de Lamballerie, X.; et al. Impact of the Second Epidemic Wave of SARS-CoV-2: Increased Exposure of Young People. Front. Public Health 2021, 9, 715192. [Google Scholar] [CrossRef] [PubMed]
- Vusirikala, A.; Whitaker, H.; Jones, S.; Tessier, E.; Borrow, R.; Linley, E.; Hoschler, K.; Baawuah, F.; Ahmad, S.; Andrews, N.; et al. Seroprevalence of SARS-CoV-2 Antibodies in University Students: Cross-Sectional Study, December 2020, England. J. Infect. 2021, 83, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Chia, P.Y.; Coleman, K.K.; Tan, Y.K.; Ong, S.W.X.; Gum, M.; Lau, S.K.; Lim, X.F.; Lim, A.S.; Sutjipto, S.; Lee, P.H.; et al. Detection of Air and Surface Contamination by SARS-CoV-2 in Hospital Rooms of Infected Patients. Nat. Commun. 2020, 11, 2800. [Google Scholar] [CrossRef] [PubMed]
- Alsaïdi, I.; De Sousa Santos, F.; Plard, B.; Janvier, E.; Tinland, A.; Hafni, A.; Mosnier, E. Factors Associated with SARS-CoV2 Infection and Care Pathways among the Most Vulnerable Populations Living in Marseille: A Case Control Study. BMC Public Health 2021, 21, 1704. [Google Scholar] [CrossRef]
- van den Broek-Altenburg, E.M.; Atherly, A.J.; Diehl, S.A.; Gleason, K.M.; Hart, V.C.; MacLean, C.D.; Barkhuff, D.A.; Levine, M.A.; Carney, J.K. Jobs, Housing, and Mask Wearing: Cross-Sectional Study of Risk Factors for COVID-19. JMIR Public Health Surveill 2021, 7, e24320. [Google Scholar] [CrossRef]
- Galmiche, S.; Charmet, T.; Schaeffer, L.; Paireau, J.; Grant, R.; Chény, O.; Platen, C.V.; Maurizot, A.; Blanc, C.; Dinis, A.; et al. Exposures Associated with SARS-CoV-2 Infection in France: A Nationwide Online Case-Control Study. Lancet Reg. Health–Europe 2021, 7, 100148. [Google Scholar] [CrossRef]
- Wei, J.-T.; Liu, Y.-X.; Zhu, Y.-C.; Qian, J.; Ye, R.-Z.; Li, C.-Y.; Ji, X.-K.; Li, H.-K.; Qi, C.; Wang, Y.; et al. Impacts of Transportation and Meteorological Factors on the Transmission of COVID-19. Int. J. Hyg. Environ. Health 2020, 230, 113610. [Google Scholar] [CrossRef]
- Fang, L.-Q.; De Vlas, S.J.; Feng, D.; Liang, S.; Xu, Y.-F.; Zhou, J.-P.; Richardus, J.H.; Cao, W.-C. Geographical Spread of SARS in Mainland China. Trop. Med. Int. Health 2009, 14, 14–20. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; de Larrea, N.F.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A Nationwide, Population-Based Seroepidemiological Study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Cho, J.H.; Lee, M.H.; Kim, Y.J.; Park, C.-S. The Diagnostic Value of Detecting Sudden Smell Loss among Asymptomatic COVID-19 Patients in Early Stage: The Possible Early Sign of COVID-19. Auris Nasus Larynx 2020, 47, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Robbiani, D.F.; Gaebler, C.; Muecksch, F.; Lorenzi, J.C.C.; Wang, Z.; Cho, A.; Agudelo, M.; Barnes, C.O.; Gazumyan, A.; Finkin, S.; et al. Convergent Antibody Responses to SARS-CoV-2 in Convalescent Individuals. Nature 2020, 584, 437–442. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.; Zhang, J.; Zeng, M.; Yun, Q.; Guo, W.; Zheng, Y.; Zhao, S.; Wang, M.H.; Yang, Z. Epidemiological Parameters of COVID-19: Case Series Study. J. Med. Internet Res. 2020, 22, e19994. [Google Scholar] [CrossRef]
- Zhang, H.; Hong, C.; Zheng, Q.; Zhou, P.; Zhu, Y.; Zhang, Z.; Bi, Q.; Ma, T. A Multi-Family Cluster of COVID-19 Associated with Asymptomatic and Pre-Symptomatic Transmission in Jixi City, Heilongjiang, China, 2020. Emerg. Microbes Infect. 2020, 9, 2509–2514. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | Overall, n = 418 1 | Academic Population | p-Value 2 | |
|---|---|---|---|---|
| Student, n = 152 1 | University Staff, n = 266 1 | |||
| Mean age (min; max) | 33.8 (17; 64) | 21.5 (17; 44) | 40.8 (20; 64) | <0.001 |
| Age group | <0.001 | |||
| <20 years | 54 (13%) | 54 (36%) | 0 (0%) | |
| [20–29 years] | 143 (34%) | 91 (60%) | 52 (20%) | |
| [30–39 years] | 82 (20%) | 4 (2%) | 78 (29%) | |
| [40–49 years] | 73 (17%) | 3 (2%) | 70 (26%) | |
| >50 years | 66 (16%) | 0 (0%) | 66 (25%) | |
| Gender Female | 271 (65%) | 97 (64%) | 174 (65%) | 0.742 |
| Education level | <0.001 | |||
| High school level and under | 75 (18%) | 49 (32%) | 26 (10%) | |
| Bachelor’s degree | 134 (32%) | 75 (49%) | 59 (22%) | |
| Master’s degree | 122 (29%) | 28 (18%) | 94 (35%) | |
| Over master’s degree | 87 (21%) | 0 (0%) | 87 (33%) | |
| Accommodation type | <0.001 | |||
| Halls of residence | 28 (7.1%) | 28 (22%) | 0 (0%) | |
| Apartment | 223 (57%) | 83 (65%) | 140 (53%) | |
| House | 141 (36%) | 17 (13%) | 124 (47%) | |
| Unknown | 26 | 24 | 2 | |
| Residential district * | <0.001 | |||
| Corte | 184 (44%) | 23 (15%) | 161 (61%) | |
| Corte/Elsewhere | 137 (33%) | 95 (62%) | 42 (16%) | |
| Elsewhere | 97 (23%) | 34 (22%) | 63 (24%) | |
| Chronic diseases ** | 117 (28%) | 34 (22%) | 83 (31%) | 0.048 |
| Unknown | 2 | 0 | 2 | |
| COVID-19 symptoms at any time since January 2020 *** | 149 (36%) | 66 (43%) | 83 (31%) | 0.012 |
| Case contact since January 2020 | 109 (26%) | 50 (33%) | 59 (22%) | 0.016 |
| Confirmed SARS-CoV-2 cases since January 2020 (self-report) | 27 (6.5%) | 11 (7.2%) | 16 (6.0%) | 0.62 |
| COVID-19 symptoms of SARS-CoV-2 confirmed cases | 22 (5.3%) | 9 (5.9%) | 13 (4.9%) | 0.6 |
| Serological status (ELISA-S) | 0.57 | |||
| Presence Ac IgG-S Adjusted according to test sensitivity and specificity | 49 (11.7%) 49 (12.8%) | 16 (10.5%) 16 (11.5%) | 33 (12.4%) 33 (13.5%) | |
| Characteristic | Reported No Symptoms at Any Time Since 1 January 2020 | Reported Experiencing Symptoms at Any Time Since 1 January 2020 | p-Value 1 |
|---|---|---|---|
| Positive ELISA-S (n = 49) | 18 (36.7%) | 31 (63.3%) | <0.001 |
| Positive RT-qPCR/ antigen test (n = 27) | 5 (18.5%) | 22 (81.5%) | <0.001 |
| Positive RT-qPCR and positive ELISA-S (n = 19) | 3 (15.8%) | 16 (84.2%) | <0.001 |
| Characteristic | Overall, n = 49 1 | Seroneutralization Results | p-Value 2 | |
|---|---|---|---|---|
| Negative, n = 34 1 | Positive, n = 15 1 | |||
| Function | 0.20 | |||
| Student | 16 (33%) | 9 (26%) | 7 (47%) | |
| University staff | 33 (67%) | 25 (74%) | 8 (53%) | |
| Mean age (years) | 32.20 (12.5) | 33.53 (12.2) | 29.20 (13.1) | 0.13 |
| Gender | 0.60 | |||
| Female | 30 (61%) | 20 (59%) | 10 (67%) | |
| Symptoms since January 2020 | 0.024 | |||
| Asymptomatic | 18 (37%) | 16 (47%) | 2 (13%) | |
| Symptomatic | 31 (63%) | 18 (53%) | 13 (87%) | |
| Mean quantification (BAU/mL) Unknown | 108.0 (85.5) 11 | 73.6 (52.1) 11 | 160.9 (100.5) 0 | 0.002 |
| Positive COVID-19 test since January 2020 | 19 (39%) | 6 (18%) | 13 (87%) | <0.001 |
| Characteristic | Description of Selected Variables (Univariate Analysis) | Effect of Selected Variables (Multivariate Analysis) | ||||
|---|---|---|---|---|---|---|
| Overall, n = 390 1 | ELISA Results | p-Value 2 | Odds Ratio [95% CI] | p-Value 2 | ||
| Negative, n = 342 1 | Positive, n = 48 1 | |||||
| Residential lifestyle | 0.10 | 0.018 | ||||
| Elsewhere | 86 (22%) | 81 (55%) | 5 (10%) | - | - | |
| Corte/Elsewhere | 123 (32%) | 107 (31%) | 16 (33%) | 1.80 [0.64–5.87] | 0.300 | |
| Corte | 181 (46%) | 154 (45%) | 27 (56%) | 3.74 [1.40–12.00] | 0.014 | |
| Accommodation type | 0.016 | 0.028 | ||||
| Apartment | 222 (57%) | 186(54%) | 36 (75%) | - | - | |
| House | 140 (36%) | 131 (38%) | 9 (19%) | 0.36 [0.15–0.77] | 0.013 | |
| University residence | 28 (7%) | 25 (8%) | 3 (6%) | 0.64 [0.14–2.08] | 0.500 | |
| Use of public transportation/carpooling | 154 (39%) | 131 (38%) | 23 (48%) | 0.200 | 2.00 [1.01–4.02] | 0.048 |
| Case contact since January 2020 | 97 (25%) | 77 (23%) | 20 (42%) | 0.004 | 2.32 [1.20–4.40] | 0.012 |
| Acute respiratory infection | 67 (16%) | 47 (13%) | 20 (41%) | <0.001 | 3.05 [1.43–6.43] | 0.005 |
| Loss of smell | 20 (4.8%) | 6 (1.6%) | 14 (29%) | <0.001 | 16.4 [5.87–50.7] | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Decarreaux, D.; Sevila, J.; Masse, S.; Capai, L.; Fourié, T.; Saba Villarroel, P.M.; Amroun, A.; Nurtop, E.; Vareille, M.; Pouquet, M.; et al. A Cross-Sectional Study of Exposure Factors Associated with Seropositivity for SARS-CoV-2 Antibodies during the Second Epidemic Wave among a Sample of the University of Corsica (France). Int. J. Environ. Res. Public Health 2022, 19, 1953. https://doi.org/10.3390/ijerph19041953
Decarreaux D, Sevila J, Masse S, Capai L, Fourié T, Saba Villarroel PM, Amroun A, Nurtop E, Vareille M, Pouquet M, et al. A Cross-Sectional Study of Exposure Factors Associated with Seropositivity for SARS-CoV-2 Antibodies during the Second Epidemic Wave among a Sample of the University of Corsica (France). International Journal of Environmental Research and Public Health. 2022; 19(4):1953. https://doi.org/10.3390/ijerph19041953
Chicago/Turabian StyleDecarreaux, Dorine, Julie Sevila, Shirley Masse, Lisandru Capai, Toscane Fourié, Paola Mariela Saba Villarroel, Abdennour Amroun, Elif Nurtop, Matthieu Vareille, Marie Pouquet, and et al. 2022. "A Cross-Sectional Study of Exposure Factors Associated with Seropositivity for SARS-CoV-2 Antibodies during the Second Epidemic Wave among a Sample of the University of Corsica (France)" International Journal of Environmental Research and Public Health 19, no. 4: 1953. https://doi.org/10.3390/ijerph19041953
APA StyleDecarreaux, D., Sevila, J., Masse, S., Capai, L., Fourié, T., Saba Villarroel, P. M., Amroun, A., Nurtop, E., Vareille, M., Pouquet, M., Blanchon, T., de Lamballerie, X., Charrel, R., & Falchi, A. (2022). A Cross-Sectional Study of Exposure Factors Associated with Seropositivity for SARS-CoV-2 Antibodies during the Second Epidemic Wave among a Sample of the University of Corsica (France). International Journal of Environmental Research and Public Health, 19(4), 1953. https://doi.org/10.3390/ijerph19041953