
Chronic Pain and Its Association with Depressive Symptoms and Renal Function in Hypertensive Patients

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Assessment of Chronic Pain
2.3. Assessment of Depressive Symptoms
2.4. Laboratory Measurements
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Laboratory Parameters of the Study Population
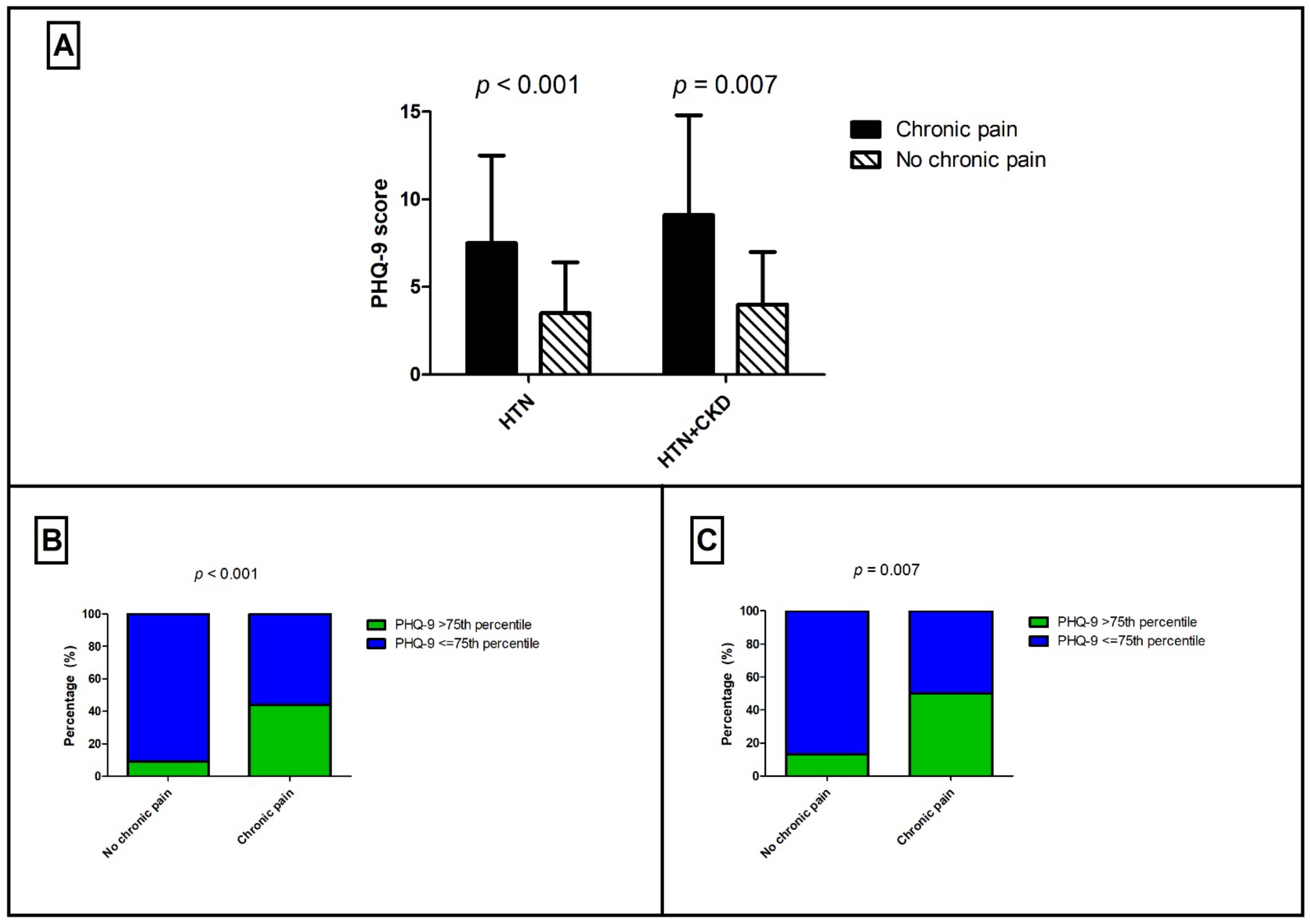
3.3. Determinants of Chronic Pain in Hypertension
3.4. Chronic Pain in Patients with Impaired Renal Function
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef] [PubMed]
- Woo, A.K. Depression and Anxiety in Pain. Rev. Pain 2010, 4, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chobufo, M.D.; Gayam, V.; Soluny, J.; Rahman, E.U.; Enoru, S.; Foryoung, J.B.; Agbor, V.N.; Dufresne, A.; Nfor, T. Prevalence and control rates of hypertension in the USA: 2017–2018. Int. J. Cardiol. Hypertens. 2020, 6, 100044. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.K.; Chang, T.I.; Cushman, W.C.; Furth, S.L.; Ix, J.H.; Pecoits-Filho, R.; Perkovic, V.; Sarnak, M.J.; Tobe, S.W.; Tomson, C.R.V.; et al. Blood pressure in chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 95, 1027–1036. [Google Scholar] [CrossRef]
- Bruck, K.; Stel, V.S.; Gambaro, G.; Hallan, S.; Volzke, H.; Arnlov, J.; Kastarinen, M.; Guessous, I.; Vinhas, J.; Stengel, B.; et al. CKD Prevalence Varies across the European General Population. J. Am. Soc. Nephrol. 2016, 27, 2135–2147. [Google Scholar] [CrossRef]
- Bello, A.K.; Ronksley, P.E.; Tangri, N.; Kurzawa, J.; Osman, M.A.; Singer, A.; Grill, A.; Nitsch, D.; Queenan, J.A.; Wick, J.; et al. Prevalence and Demographics of CKD in Canadian Primary Care Practices: A Cross-sectional Study. Kidney Int. Rep. 2019, 4, 561–570. [Google Scholar] [CrossRef] [Green Version]
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Davison, S.N.; Rathwell, S.; Ghosh, S.; George, C.; Pfister, T.; Dennett, L. The Prevalence and Severity of Chronic Pain in Patients with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Can. J. Kidney Health Dis. 2021, 8, 2054358121993995. [Google Scholar] [CrossRef]
- Pham, P.C.; Khaing, K.; Sievers, T.M.; Pham, P.M.; Miller, J.M.; Pham, S.V.; Pham, P.A.; Pham, P.T. 2017 update on pain management in patients with chronic kidney disease. Clin. Kidney J. 2017, 10, 688–697. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Homan, T.D.; Bordes, S.; Cichowski, E. Physiology, Pulse Pressure; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Wong, E.L.Y.; Xu, R.H.; Cheung, A.W.L. Health-related quality of life among patients with hypertension: Population-based survey using EQ-5D-5L in Hong Kong SAR, China. BMJ Open 2019, 9, e032544. [Google Scholar] [CrossRef] [Green Version]
- Zheng, E.; Xu, J.; Xu, J.; Zeng, X.; Tan, W.J.; Li, J.; Zhao, M.; Liu, B.; Liu, R.; Sui, M.; et al. Health-Related Quality of Life and Its Influencing Factors for Elderly Patients With Hypertension: Evidence From Heilongjiang Province, China. Front. Public Health 2021, 9, 654822. [Google Scholar] [CrossRef]
- Wong, E.L.Y.; Xu, R.H.; Cheung, A.W.L. Health-related quality of life in elderly people with hypertension and the estimation of minimally important difference using EQ-5D-5L in Hong Kong SAR, China. Eur. J. Health Econ. 2020, 21, 869–879. [Google Scholar] [CrossRef]
- Fraser, S.D.; Barker, J.; Roderick, P.J.; Yuen, H.M.; Shardlow, A.; Morris, J.E.; McIntyre, N.J.; Fluck, R.J.; McIntyre, C.W.; Taal, M.W. Health-related quality of life, functional impairment and comorbidity in people with mild-to-moderate chronic kidney disease: A cross-sectional study. BMJ Open 2020, 10, e040286. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Arroll, B.; Goodyear-Smith, F.; Crengle, S.; Gunn, J.; Kerse, N.; Fishman, T.; Falloon, K.; Hatcher, S. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann. Fam. Med. 2010, 8, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Parlapani, E.; Holeva, V.; Voitsidis, P.; Blekas, A.; Gliatas, I.; Porfyri, G.N.; Golemis, A.; Papadopoulou, K.; Dimitriadou, A.; Chatzigeorgiou, A.F.; et al. Psychological and Behavioral Responses to the COVID-19 Pandemic in Greece. Front. Psychiatry 2020, 11, 821. [Google Scholar] [CrossRef]
- Siarava, E.; Hyphantis, T.; Katsanos, A.H.; Pelidou, S.H.; Kyritsis, A.P.; Markoula, S. Depression and quality of life in patients with epilepsy in Northwest Greece. Seizure 2019, 66, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Shrestha, P.L.; Shrestha, P.A.; Vivo, R.P. Epidemiology of comorbidities in patients with hypertension. Curr. Opin. Cardiol. 2016, 31, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Ventura, H.O.; Lavie, C.J. Impact of comorbidities in hypertension. Curr. Opin. Cardiol. 2016, 31, 374–375. [Google Scholar] [CrossRef] [PubMed]
- Sacco, M.; Meschi, M.; Regolisti, G.; Detrenis, S.; Bianchi, L.; Bertorelli, M.; Pioli, S.; Magnano, A.; Spagnoli, F.; Giuri, P.G.; et al. The relationship between blood pressure and pain. J. Clin. Hypertens. 2013, 15, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Al-Ghamdi, S.; Shubair, M.M.; El-Metwally, A.; Alsalamah, M.; Alshahrani, S.M.; Al-Khateeb, B.F.; Bahkali, S.; Aloudah, S.M.; Al-Zahrani, J.; Almigbal, T.H.; et al. The relationship between chronic pain, prehypertension, and hypertension. A population-based cross-sectional survey in Al-Kharj, Saudi Arabia. Postgrad. Med. 2021, 133, 345–350. [Google Scholar] [CrossRef]
- Bartley, E.J.; Fillingim, R.B. Sex differences in pain: A brief review of clinical and experimental findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Mathew, R.O.; Bettinger, J.J.; Wegrzyn, E.L.; Fudin, J. Pharmacotherapeutic considerations for chronic pain in chronic kidney and end-stage renal disease. J. Pain Res. 2016, 9, 1191–1195. [Google Scholar] [CrossRef] [Green Version]
- Han, B.; Compton, W.M. Prescription Opioids for Pain Management in Patients on Dialysis. J. Am. Soc. Nephrol. 2017, 28, 3432–3434. [Google Scholar] [CrossRef]
- Lambourg, E.; Colvin, L.; Guthrie, G.; Murugan, K.; Lim, M.; Walker, H.; Boon, G.; Bell, S. The prevalence of pain among patients with chronic kidney disease using systematic review and meta-analysis. Kidney Int. 2021, 100, 636–649. [Google Scholar] [CrossRef]
- Davison, S.N. Pain, analgesics, and safety in patients with CKD. Clin. J. Am. Soc. Nephrol. 2015, 10, 350–352. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Li, Y.; Chen, L.; Chen, P.; Hu, Y. Prevalence of Depression in Patients with Hypertension: A Systematic Review and Meta-Analysis. Medicine 2015, 94, e1317. [Google Scholar] [CrossRef]
- Rubio-Guerra, A.F.; Rodriguez-Lopez, L.; Vargas-Ayala, G.; Huerta-Ramirez, S.; Serna, D.C.; Lozano-Nuevo, J.J. Depression increases the risk for uncontrolled hypertension. Exp. Clin. Cardiol. 2013, 18, 10–12. [Google Scholar]
- DeMoss, D.S.; Teigen, K.J.; Claassen, C.A.; Fisk, M.J.; Blair, S.E.; Bakre, S.A.; Hurd, C.L.; Rush, A.J. Association between depression and hypertension using classic and revised blood pressure thresholds. Fam. Pract. 2020, 37, 616–622. [Google Scholar] [CrossRef]
- Hamam, M.S.; Kunjummen, E.; Hussain, M.S.; Nasereldin, M.; Bennett, S.; Miller, J. Anxiety, Depression, and Pain: Considerations in the Treatment of Patients with Uncontrolled Hypertension. Curr. Hypertens. Rep. 2020, 22, 106. [Google Scholar] [CrossRef]
- Miller, L.R.; Cano, A. Comorbid chronic pain and depression: Who is at risk? J. Pain 2009, 10, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Santoro, D.; Satta, E.; Messina, S.; Costantino, G.; Savica, V.; Bellinghieri, G. Pain in end-stage renal disease: A frequent and neglected clinical problem. Clin. Nephrol. 2013, 79 (Suppl. 1), S2–S11. [Google Scholar] [CrossRef]
- Al-Jabi, S.W.; Sous, A.; Jorf, F.; Taqatqa, M.; Allan, M.; Sawalha, L.; Lubadeh, E.; Zyoud, S.H.; Sweileh, W.M. Depression in patients treated with haemodialysis: A cross-sectional study. Lancet 2018, 391 (Suppl. 2), S41. [Google Scholar] [CrossRef]
- Samoudi, A.F.; Marzouq, M.K.; Samara, A.M.; Zyoud, S.H.; Al-Jabi, S.W. The impact of pain on the quality of life of patients with end-stage renal disease undergoing hemodialysis: A multicenter cross-sectional study from Palestine. Health Qual. Life Outcomes 2021, 19, 39. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Total Patients (N = 158) | Patients with eGFR < 60 (N = 47) | Patients with eGFR ≥ 60 (N = 111) | p |
|---|---|---|---|---|
| Sociodemographic and Clinical characteristics | ||||
| Age, years | 55.2 (SD: 13.7) | 58.3 (SD: 13.8) | 53.8 (SD: 13.4) | 0.07 |
| Male Sex | 94 (59.5%) | 27 (57.4%) | 67 (60.4%) | 0.73 |
| BMI, kg/m2 | 28.9 (SD: 4.8) | 28.1 (SD: 3.9) | 29.3 (SD: 5.1) | 0.22 |
| Obesity | 41 (35.3%) | 11 (31.4%) | 30 (37.0%) | 0.23 |
| Diabetes mellitus | 17 (13.1%) | 8 (19.5%) | 9 (10.1%) | 0.14 |
| Cardiovascular disease | 10 (7.7%) | 4 (9.8%) | 6 (6.7%) | 0.55 |
| SBP, mmHg | 131 (SD: 15) | 130 (SD: 16) | 131 (SD: 15) | 0.62 |
| DBP, mmHg | 87 (SD: 10) | 86 (SD: 9) | 87 (SD: 10) | 0.68 |
| PP, mmHg | 44 (SD: 12) | 44 (SD: 13) | 44 (SD: 12) | 0.79 |
| Depressive Symptoms | ||||
| Depression score (PHQ-9) | 5.2 (SD: 4.4) | 6.5 (SD: 5.2) | 4.7 (SD: 4.0) | 0.02 |
| PHQ-9 above 75th percentile | 38 (24.5%) | 14 (31.1%) | 24 (21.8%) | 0.22 |
| Parameters | Chronic Pain (N = 70) | No Chronic Pain (N = 88) | p |
|---|---|---|---|
| Clinical characteristics | |||
| Age, years | 58.7 (SD: 14.6) | 52.4 (SD: 12.3) | 0.004 |
| Male Sex | 30 (42.9%) | 64 (72.7%) | <0.001 |
| BMI, kg/m2 | 29.6 (SD: 5.3) | 28.4 (SD: 4.4) | 0.19 |
| Obesity | 21 (41.2%) | 20 (30.8%) | 0.24 |
| Diabetes mellitus | 11 (19.6%) | 6 (8.1%) | 0.053 |
| eGFR < 60 mL/min/1.73 m2 | 23 (32.9%) | 24 (27.3%) | 0.45 |
| Cardiovascular disease | 3 (5.4%) | 7 (9.5%) | 0.39 |
| Psychometric characteristics | |||
| Depression (PHQ-9) | 7.5 (SD: 5.0) | 3.5 (SD: 2.9) | <0.001 |
| PHQ-9 above 75th percentile | 30 (44.1%) | 8 (9.2%) | <0.001 |
| Parameter | Odds Ratio | 95% Confidence Interval | p |
|---|---|---|---|
| Age | 1.03 | 0.99–1.07 | 0.12 |
| Female sex | 2.87 | 1.13–7.33 | 0.03 |
| Diabetes mellitus | 2.20 | 0.60–8.02 | 0.23 |
| Hemoglobin | 0.78 | 0.57–1.06 | 0.10 |
| eGFRCKD-EPI | 0.99 | 0.97–1.01 | 0.40 |
| PHQ-9 score > 75th percentile | 4.91 | 1.30–18.5 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalaitzidis, R.G.; Theofilis, P.; Touchantzidou, K.; Vordoni, A.; Siamopoulos, K.C.; Skapinakis, P. Chronic Pain and Its Association with Depressive Symptoms and Renal Function in Hypertensive Patients. Int. J. Environ. Res. Public Health 2022, 19, 1899. https://doi.org/10.3390/ijerph19031899
Kalaitzidis RG, Theofilis P, Touchantzidou K, Vordoni A, Siamopoulos KC, Skapinakis P. Chronic Pain and Its Association with Depressive Symptoms and Renal Function in Hypertensive Patients. International Journal of Environmental Research and Public Health. 2022; 19(3):1899. https://doi.org/10.3390/ijerph19031899
Chicago/Turabian StyleKalaitzidis, Rigas G., Panagiotis Theofilis, Kalliopi Touchantzidou, Aikaterini Vordoni, Kostas C. Siamopoulos, and Petros Skapinakis. 2022. "Chronic Pain and Its Association with Depressive Symptoms and Renal Function in Hypertensive Patients" International Journal of Environmental Research and Public Health 19, no. 3: 1899. https://doi.org/10.3390/ijerph19031899
APA StyleKalaitzidis, R. G., Theofilis, P., Touchantzidou, K., Vordoni, A., Siamopoulos, K. C., & Skapinakis, P. (2022). Chronic Pain and Its Association with Depressive Symptoms and Renal Function in Hypertensive Patients. International Journal of Environmental Research and Public Health, 19(3), 1899. https://doi.org/10.3390/ijerph19031899