
Health and Economic Impact of Atrial Fibrillation of Workers in Italy: Social Security Benefits

 ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis by Classification of Profession
3.2. Territorial Analysis: Distribution by Region of Residence
3.3. Estimated Number of Beneficiaries and Social Security Costs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Camp, G. Cardiovascular disease prevention. Acta Clin. Belg. 2014, 69, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Vio, R.; Proietti, R. Stroke, Dementia, and Atrial Fibrillation: From Pathophysiologic Association to Pharmacological Implications. Medicina 2020, 56, 227. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, M.M.; Borchini, R. Atrial fibrillation: An additional cardiovascular detrimental effect of stress at work? Eur. J. Prev. Cardiol. 2018, 25, 1140–1141. [Google Scholar] [CrossRef] [PubMed]
- Zimetbaum, P. Atrial Fibrillation. Ann. Intern. Med. 2017, 166, ITC33–ITC48. [Google Scholar] [CrossRef]
- Camm, A.J. Atrial fibrillation and risk. Clin. Cardiol. 2012, 35, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Vizzardi, E.; Curnis, A.; Latini, M.G.; Salghetti, F.; Rocco, E.; Lupi, L.; Rovetta, R.; Quinzani, F.; Bonadei, I.; Bontempi, L.; et al. Risk factors for atrial fibrillation recurrence: A literature review. J. Cardiovasc. Med. 2014, 15, 235–253. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Rago, A.; Proietti, R.; Di Meo, F.; Antonio Papa, A.; Calabrò, P.; D’Onofrio, A.; Nigro, G.; AlTurki, A. Efficacy and safety of the target-specific oral anticoagulants for stroke prevention in atrial fibrillation: The real-life evidence. Ther. Adv. Drug Saf. 2017, 8, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Russo, S.; Mariani, T.T.; Migliorini, R.; Marcellusi, A.; Mennini, F.S. The economic burden of musculoskeletal disorders on the Italian social security pension system estimated by a Monte Carlo simulation. Reumatismo 2015, 67, 45–56. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Coppeta, L.; Somma, G.; Ippoliti, L.; Ferrari, C.; D’Alessandro, I.; Pietroiusti, A.; Trabucco Aurilio, M. Contact Screening for Healthcare Workers Exposed to Patients with COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 9082. [Google Scholar] [CrossRef] [PubMed]
- Coppeta, L.; Ferrari, C.; Iannuzzi, I.; D’Alessandro, I.; Balbi, O.; Pietroiusti, A.; Trabucco Aurilio, M. Rubella Immunity among Italian Female Healthcare Workers: A Serological Study. Int. J. Environ. Res. Public Health 2020, 17, 7992. [Google Scholar] [CrossRef] [PubMed]
- Rapporto ISTAT. Il Futuro Demografico del Paese. Previsioni Regionali della Popolazione Residente al 2065. Available online: https://www.istat.it/it/files//2018/05/previsioni_demografiche.pdf (accessed on 2 August 2021).
- Grattan, E.; Jeffcoate, G.O. Medical factors and road accidents. Br. Med. J. 1968, 1, 75–79. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kivimäki, M.; Jokela, M.; Nyberg, S.T.; Singh-Manoux, A.; Fransson, E.I.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Casini, A.; et al. Long working hours and risk of coronary heart disease and stroke: A systematic review and meta-analysis of published and unpublished data for 603,838 individuals. Lancet 2015, 386, 1739–1746. [Google Scholar] [CrossRef]
- Lee, W.; Lee, J.; Kim, H.R.; Lee, Y.M.; Lee, D.W.; Kang, M.Y. The combined effect of long working hours and individual risk factors on cardiovascular disease: An interaction analysis. J. Occup. Health 2021, 63, e12204. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Kim, H.R.; Myong, J.P.; Choi, J.; Hong, Y.C.; Kang, M.Y. Does working long hours increase the risk of cardiovascular disease for everyone? J. Occup. Health 2019, 61, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Bolcato, M.; Sanavio, M.; Rodriguez, D.; Aprile, A. Proposal for the Application of a Quality Indicator to Medico-legal Consultations in the Field of Medical Liability. Curr. Pharm. Biotechnol. 2021, 22, 1994–2000. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
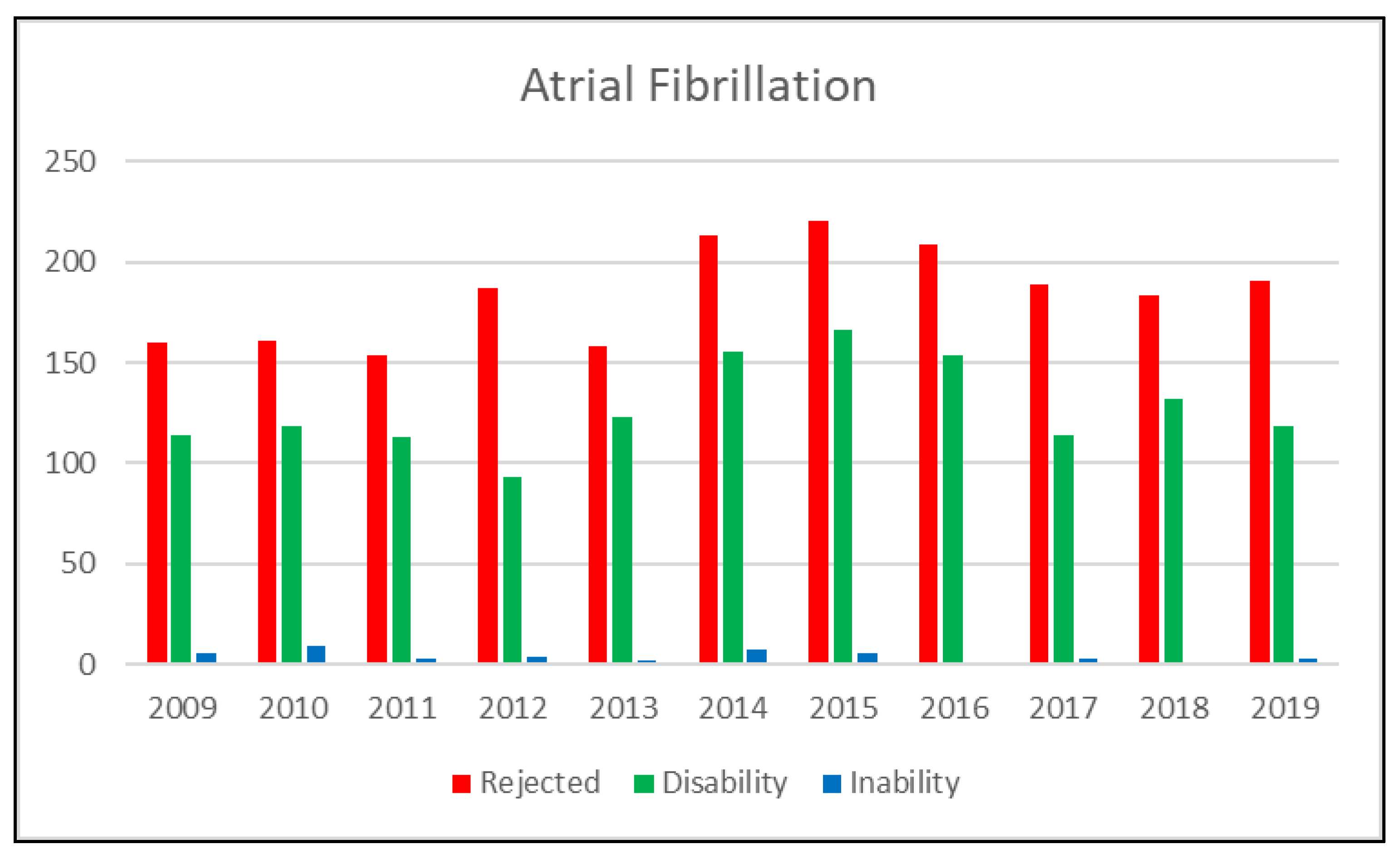
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | Total | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Atrial Fibrillation | Rejected | 160 | 161 | 154 | 187 | 158 | 213 | 220 | 209 | 189 | 183 | 191 | |
| Disability | 114 | 118 | 113 | 93 | 123 | 155 | 166 | 154 | 114 | 132 | 118 | ||
| Inability | 5 | 9 | 3 | 4 | 2 | 7 | 5 | 1 | 3 | 1 | 3 | ||
| Total | 279 | 288 | 270 | 284 | 283 | 375 | 391 | 364 | 306 | 316 | 312 | 3468 |
| Classification of Profession | Values % |
|---|---|
| I—Legislators, top management, and entrepreneurs | 3.0% |
| II—Intellectual, scientific, and highly specialized professions | 0.9% |
| III—Technical professions | 3.2% |
| IV—Clerical support workers | 4.6% |
| V—Skilled professions in business activities and services | 11.3% |
| VI—Craftsmen, skilled workers, and farmers | 35.1% |
| VII—Plant Operators, stationary and mobile machine operators, and vehicle drivers | 14.5% |
| VIII—Unskilled professions | 27.4% |
| Region | 2009 | 2019 | Average 2009–2019 |
|---|---|---|---|
| Piedmont | 4.5% | 0.8% | 2.4% |
| Valle d’Aosta | 0.0% | 40.8% | 27.2% |
| Liguria | 4.8% | 1.2% | 3.2% |
| Lombardy | 1.1% | 0.5% | 1.0% |
| Trentino-Alto Adige | 0.0% | 1.5% | 3.0% |
| Venice | 1.4% | 0.0% | 1.2% |
| Friuli-Venezia Giulia | 3.0% | 5.9% | 4.0% |
| Emilia-Romagna | 1.2% | 3.3% | 2.6% |
| Tuscany | 3.4% | 1.9% | 2.6% |
| Umbria | 6.3% | 14.5% | 12.3% |
| Marche | 1.2% | 2.4% | 4.7% |
| Lazio | 3.1% | 2.8% | 3.5% |
| Abruzzo | 6.2% | 7.6% | 6.3% |
| Molise | 0.0% | 20.7% | 18.8% |
| Campania | 9.8% | 9.1% | 9.1% |
| Puglia | 8.5% | 10.4% | 11.1% |
| Basilicata | 20.0% | 11.9% | 12.9% |
| Calabria | 13.1% | 12.3% | 12.7% |
| Sicily | 4.6% | 5.0% | 7.2% |
| Sardinia | 7.7% | 6.4% | 9.9% |
| Year | Total Beneficiaries | Average Annual Amounts | ||
|---|---|---|---|---|
| IA | IP | IA | IP | |
| 2009 | 366,728 | 81,138 | € 7835 | € 12,174 |
| 2019 | 446,326 | 84,183 | € 9593 | € 13,717 |
| Media 2009–2019 | 392,913 | 84,106 | € 8765 | € 13,063 |
| IA | IP | Total | ||||
|---|---|---|---|---|---|---|
| Beneficiaries | Costs | Beneficiaries | Costs | Beneficiaries | Costs | |
| 2009 | 951 | EUR 7,454,031 | 46 | EUR 562,071 | 998 | EUR 8,016,102 |
| 2019 | 1028 | EUR 9,864,371 | 38 | EUR 527,431 | 1067 | EUR 10,391,802 |
| AVERAGE | 1060 | EUR 9,331,781 | 44 | EUR 10,391,802 | 1103 | EUR 9,900,870 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trabucco Aurilio, M.; Mennini, F.S.; Nardone, C.; Piccioni, A.; Bolcato, M.; Russo, V.; Sciannamea, V.; Migliorini, R.; Coppeta, L.; Magrini, A. Health and Economic Impact of Atrial Fibrillation of Workers in Italy: Social Security Benefits. Int. J. Environ. Res. Public Health 2022, 19, 1883. https://doi.org/10.3390/ijerph19031883
Trabucco Aurilio M, Mennini FS, Nardone C, Piccioni A, Bolcato M, Russo V, Sciannamea V, Migliorini R, Coppeta L, Magrini A. Health and Economic Impact of Atrial Fibrillation of Workers in Italy: Social Security Benefits. International Journal of Environmental Research and Public Health. 2022; 19(3):1883. https://doi.org/10.3390/ijerph19031883
Chicago/Turabian StyleTrabucco Aurilio, Marco, Francesco Saverio Mennini, Claudia Nardone, Andrea Piccioni, Matteo Bolcato, Vincenzo Russo, Valerio Sciannamea, Raffaele Migliorini, Luca Coppeta, and Andrea Magrini. 2022. "Health and Economic Impact of Atrial Fibrillation of Workers in Italy: Social Security Benefits" International Journal of Environmental Research and Public Health 19, no. 3: 1883. https://doi.org/10.3390/ijerph19031883
APA StyleTrabucco Aurilio, M., Mennini, F. S., Nardone, C., Piccioni, A., Bolcato, M., Russo, V., Sciannamea, V., Migliorini, R., Coppeta, L., & Magrini, A. (2022). Health and Economic Impact of Atrial Fibrillation of Workers in Italy: Social Security Benefits. International Journal of Environmental Research and Public Health, 19(3), 1883. https://doi.org/10.3390/ijerph19031883