
Addressing the Social Determinants of Health in South Korea: Moderating Role of mHealth Technologies


Abstract
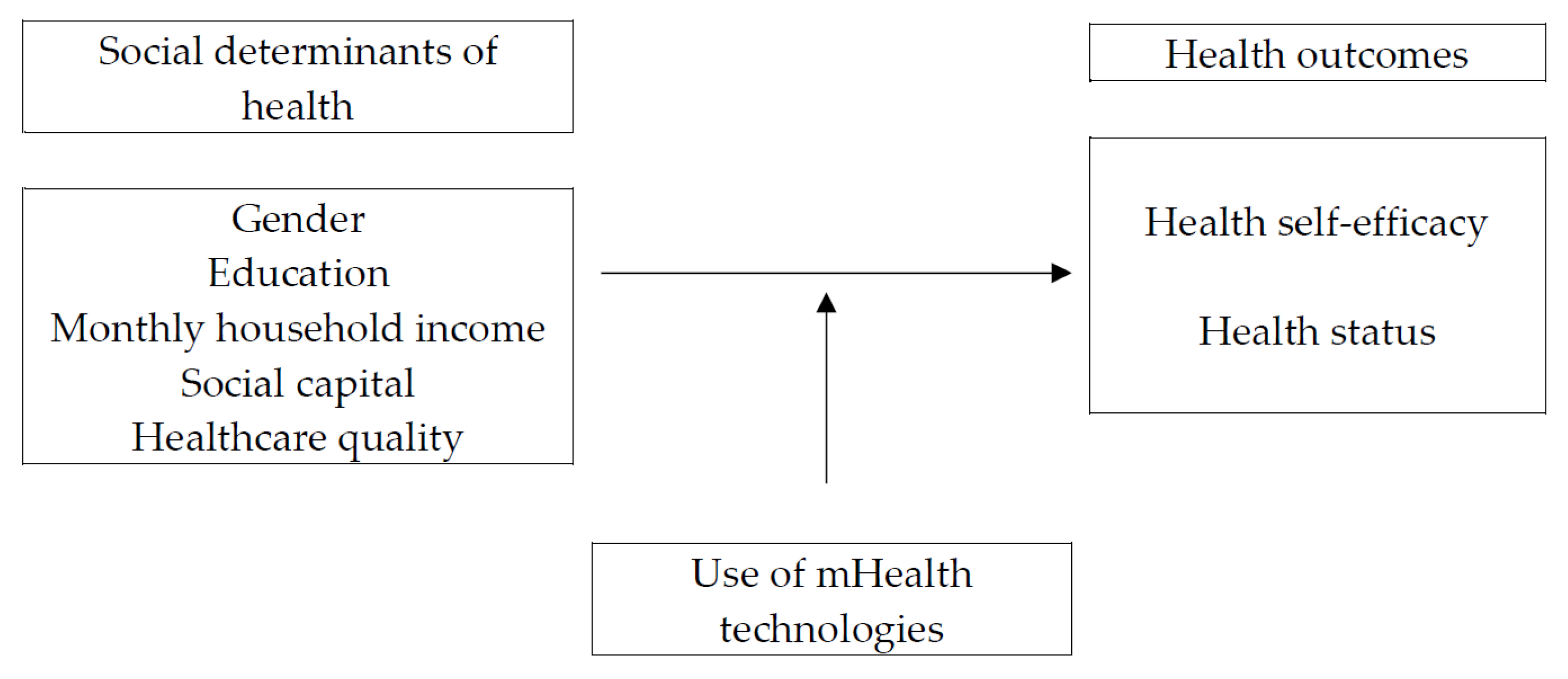
:1. Introduction
2. Materials and Methods
2.1. Data and Participants
2.2. Measures
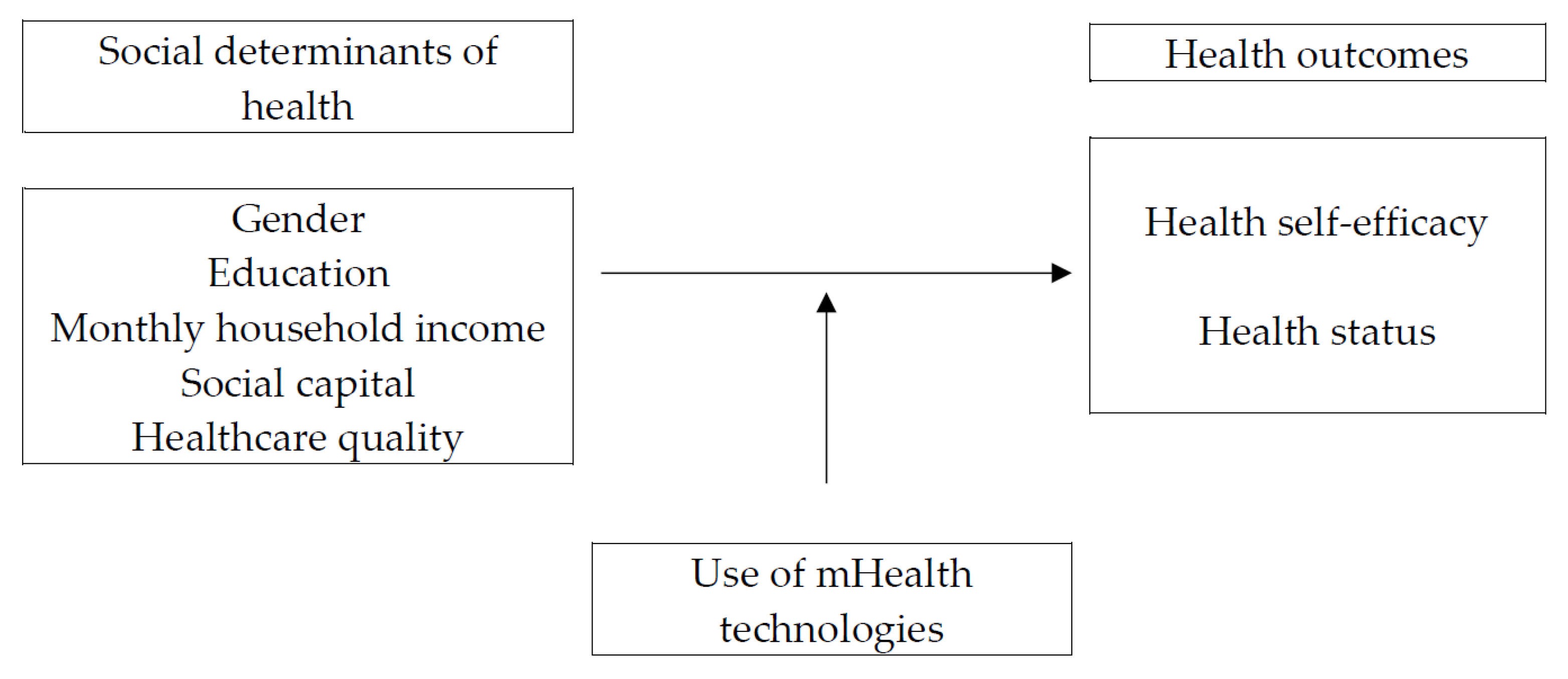
2.2.1. Social Determinants of Health
2.2.2. Use of mHealth Technologies
2.2.3. Health Outcomes
2.3. Statistical Analyses
3. Results
3.1. Effects of Social Determinants on Health Outcomes
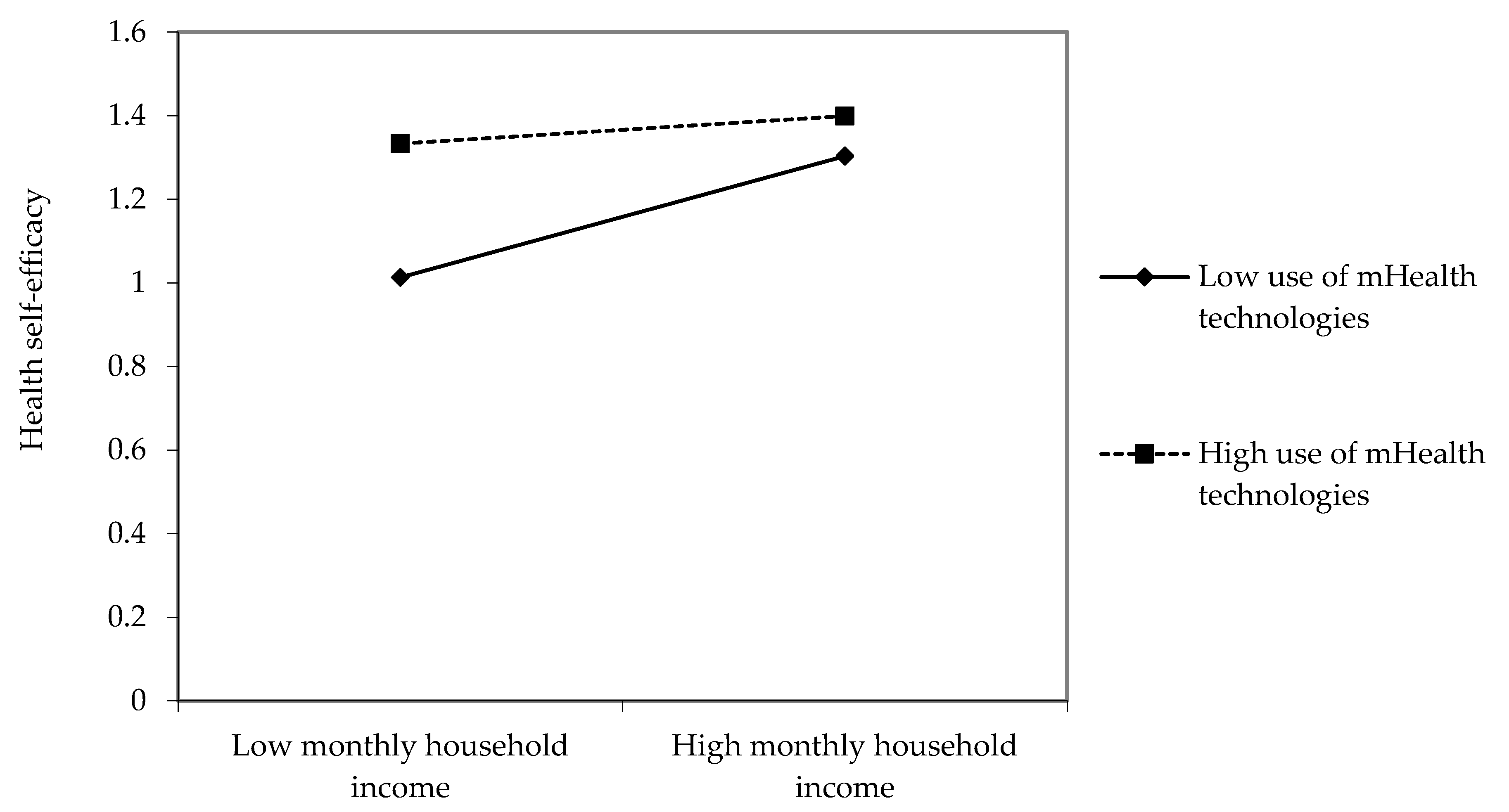
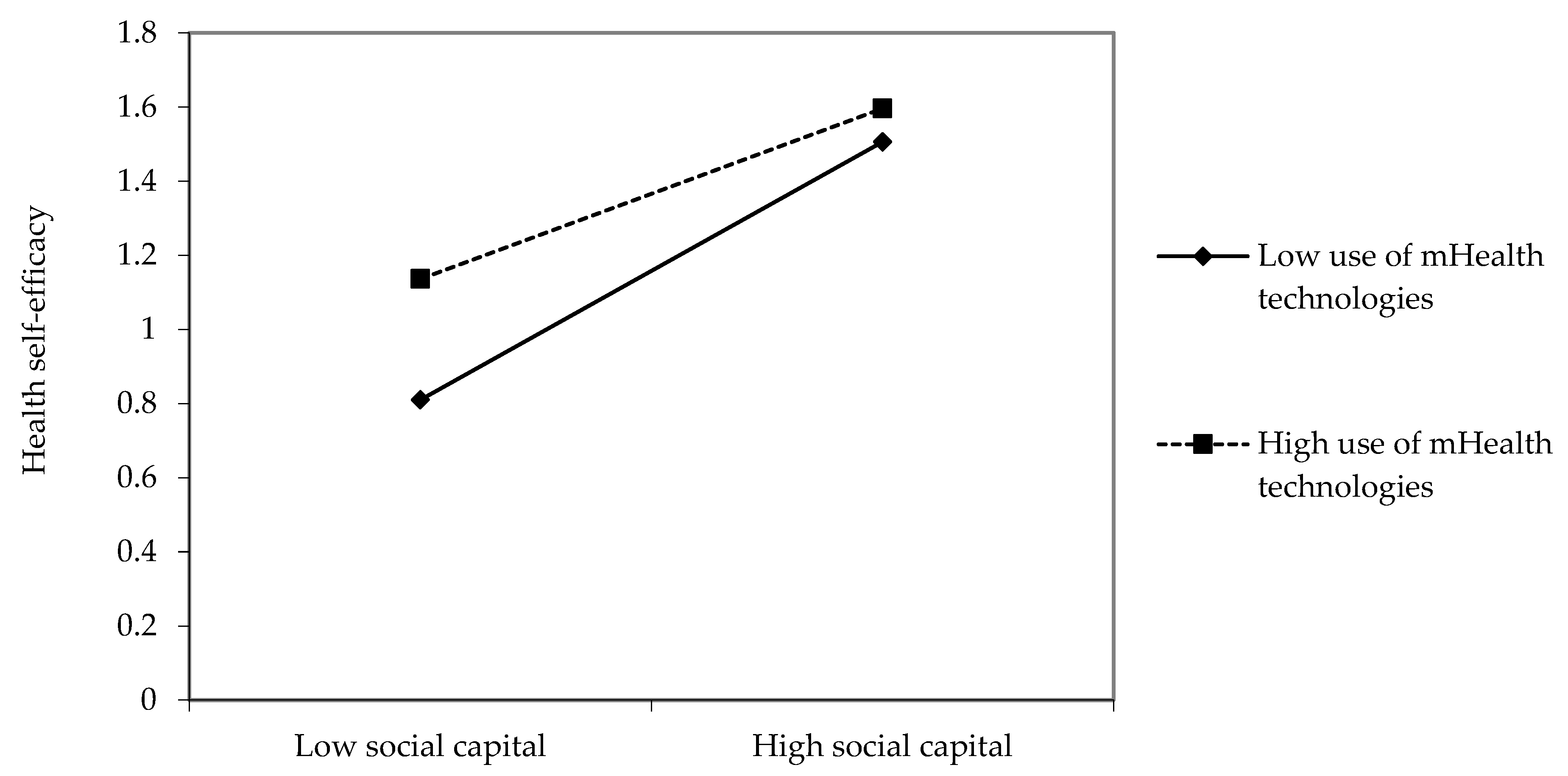
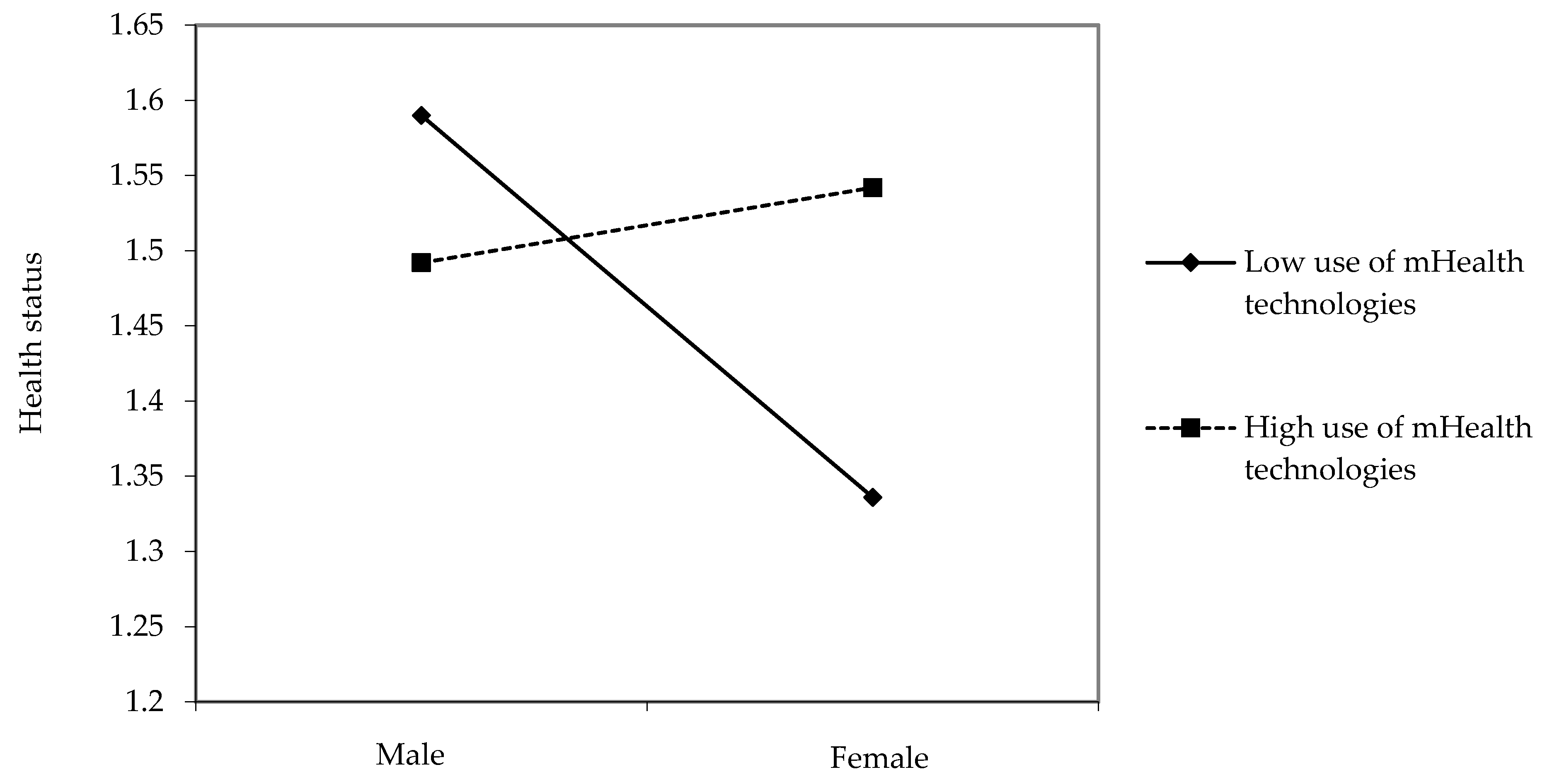
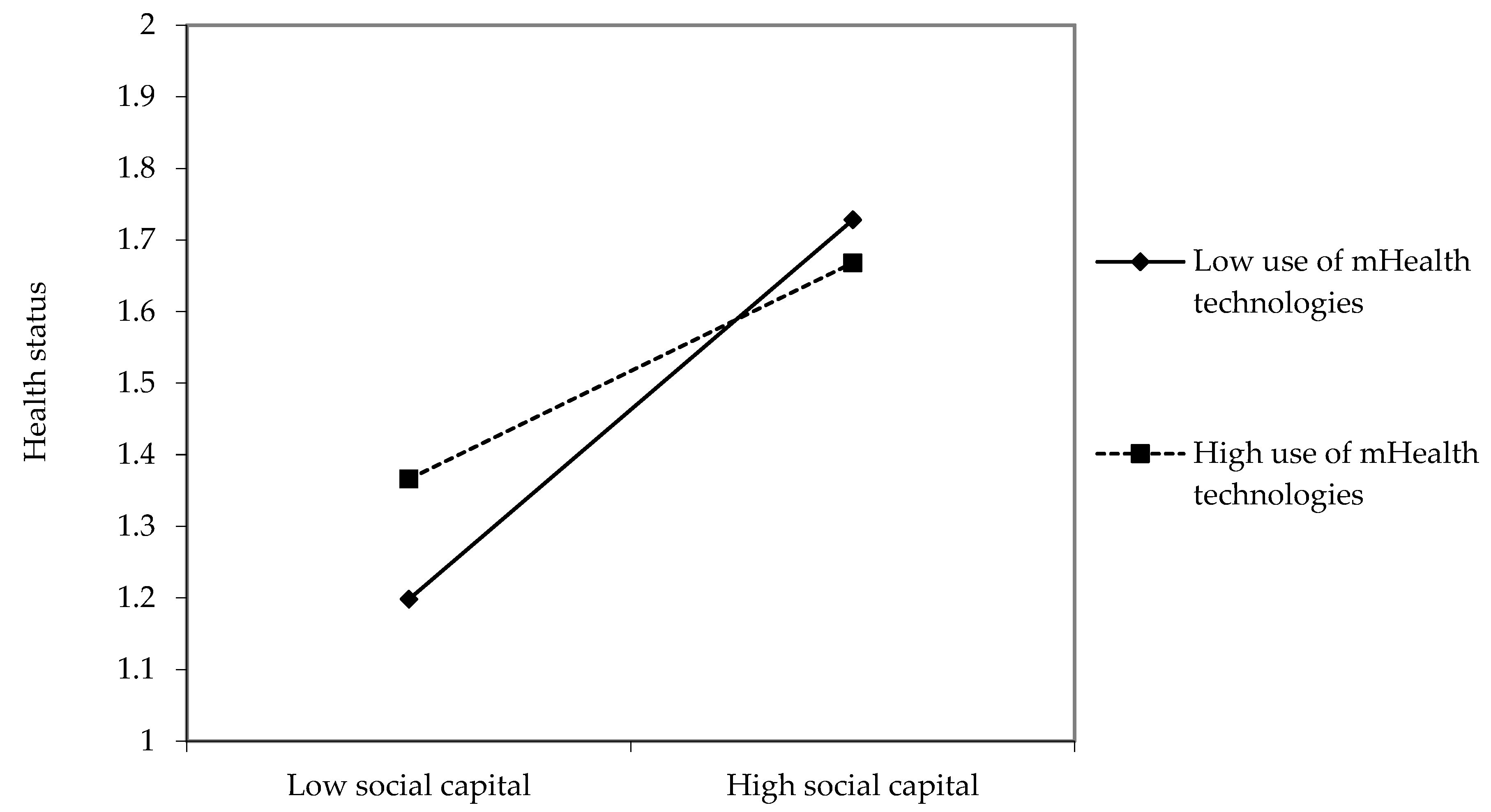
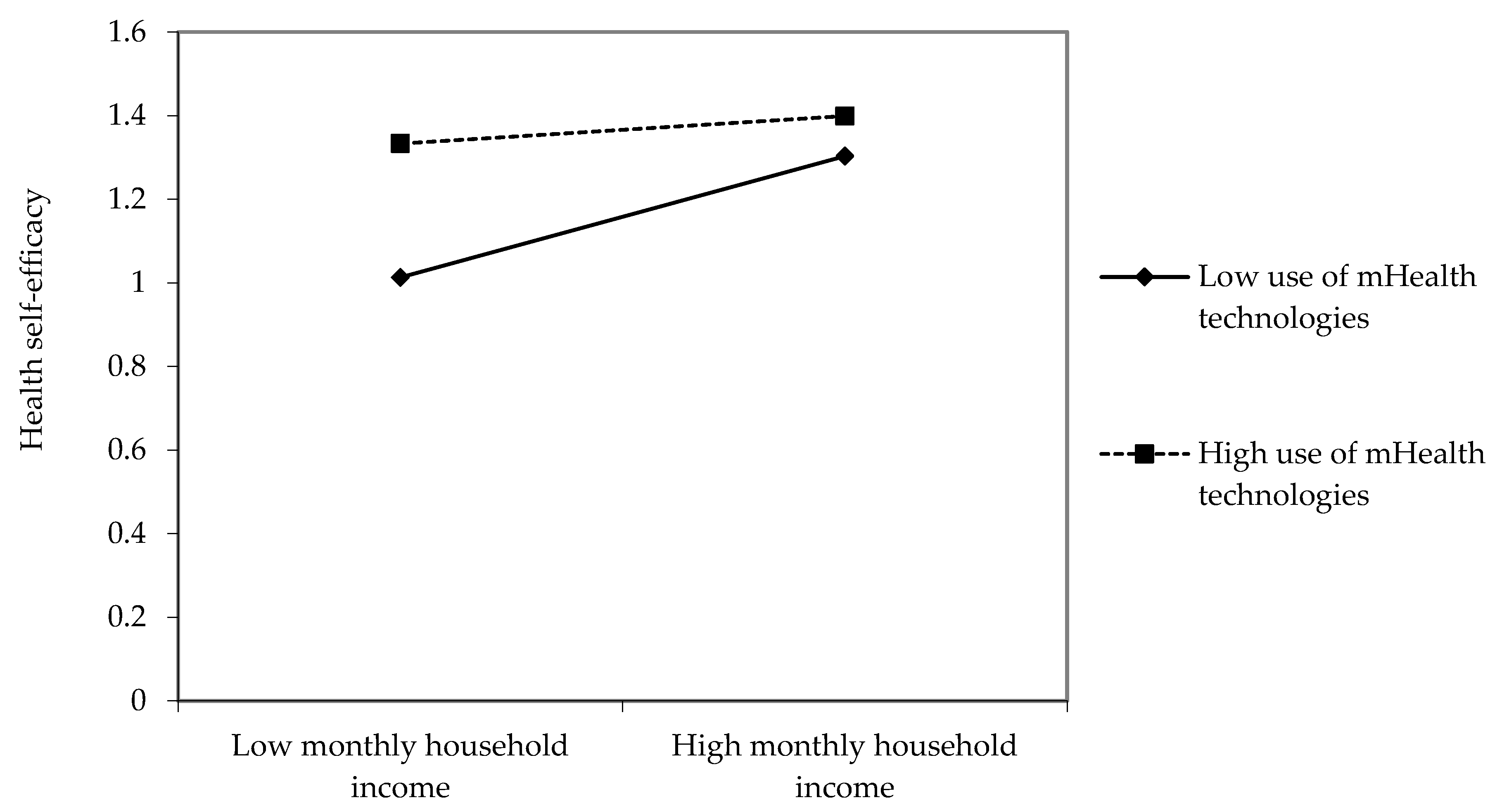
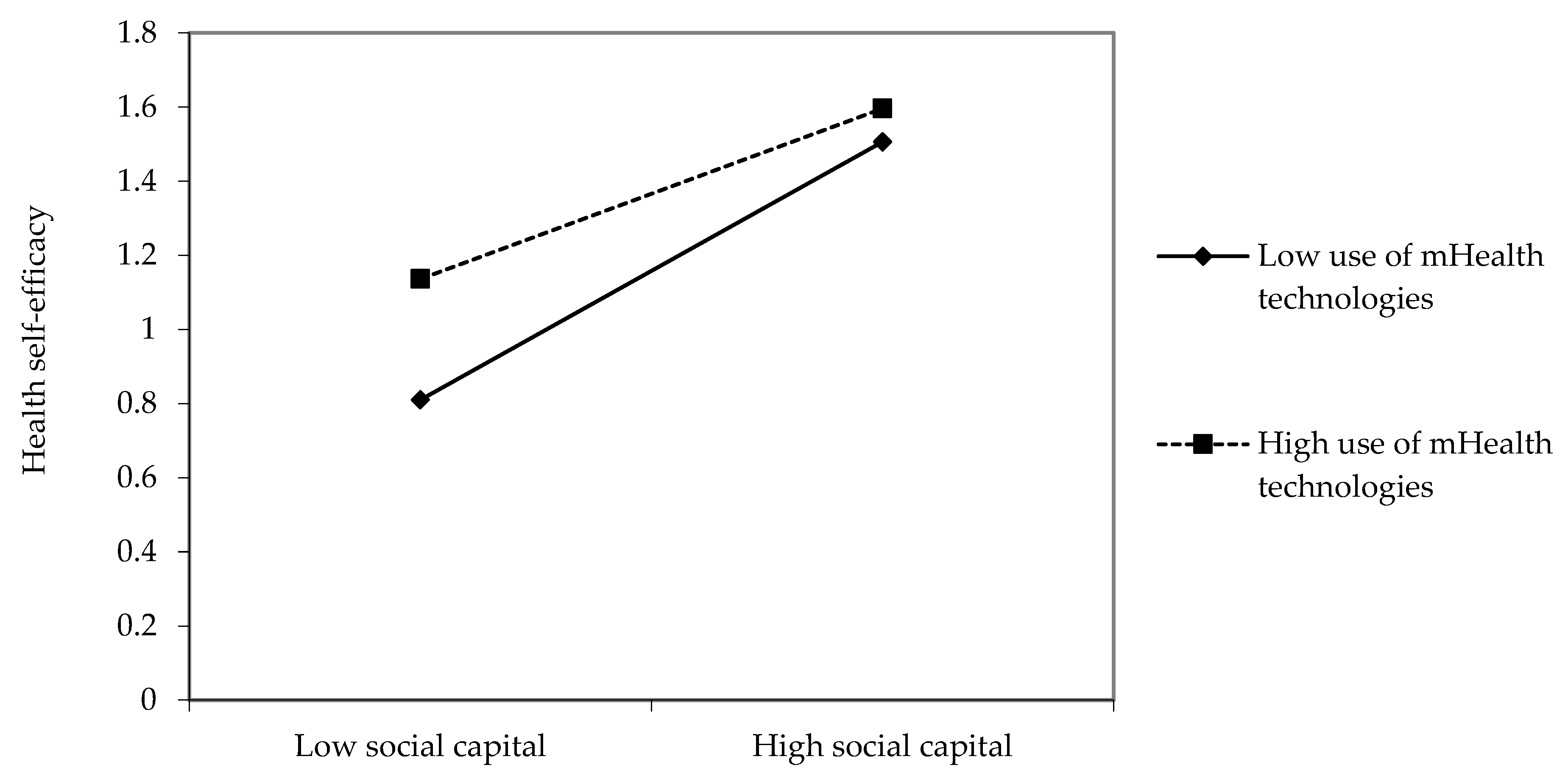
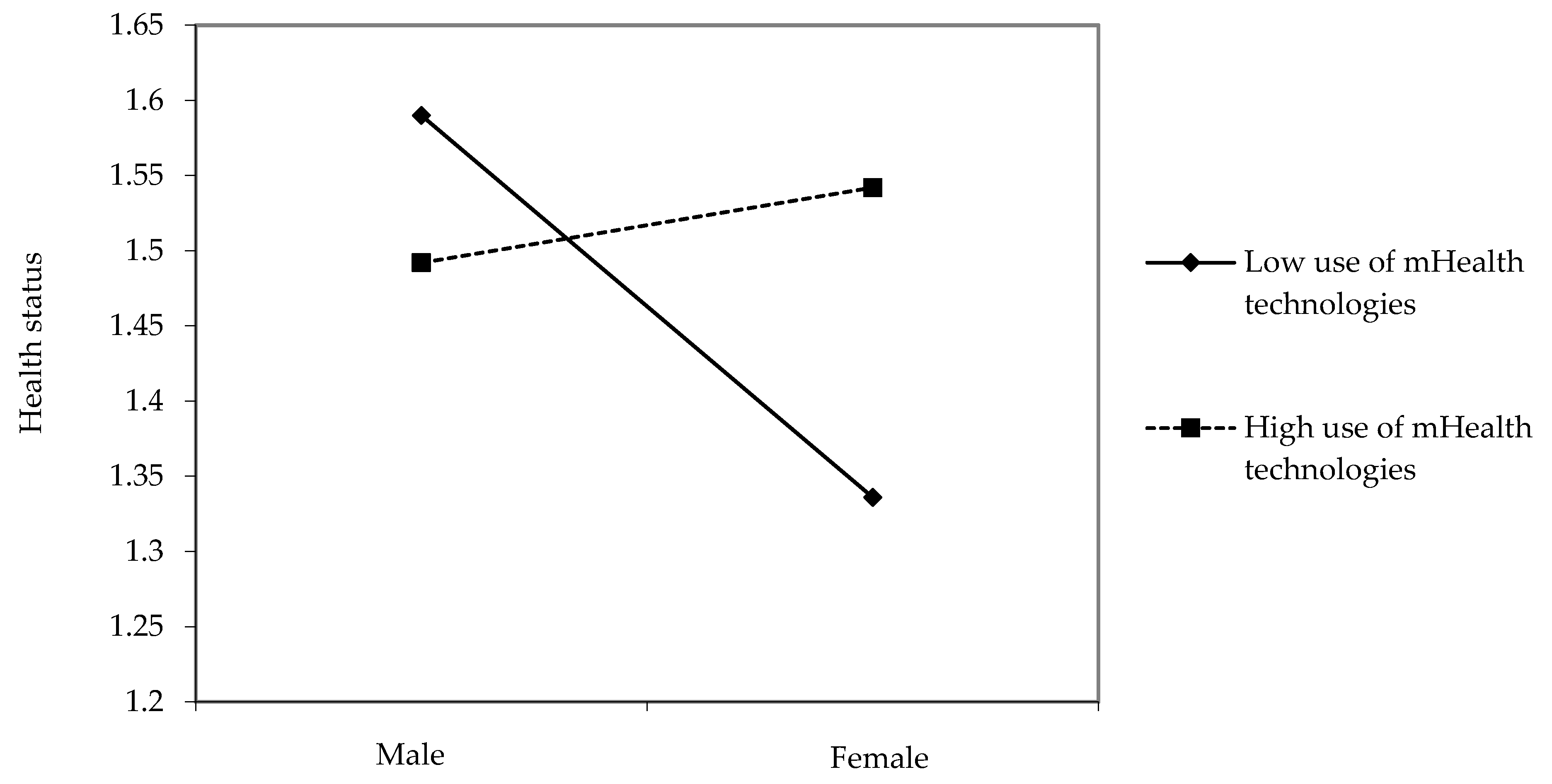
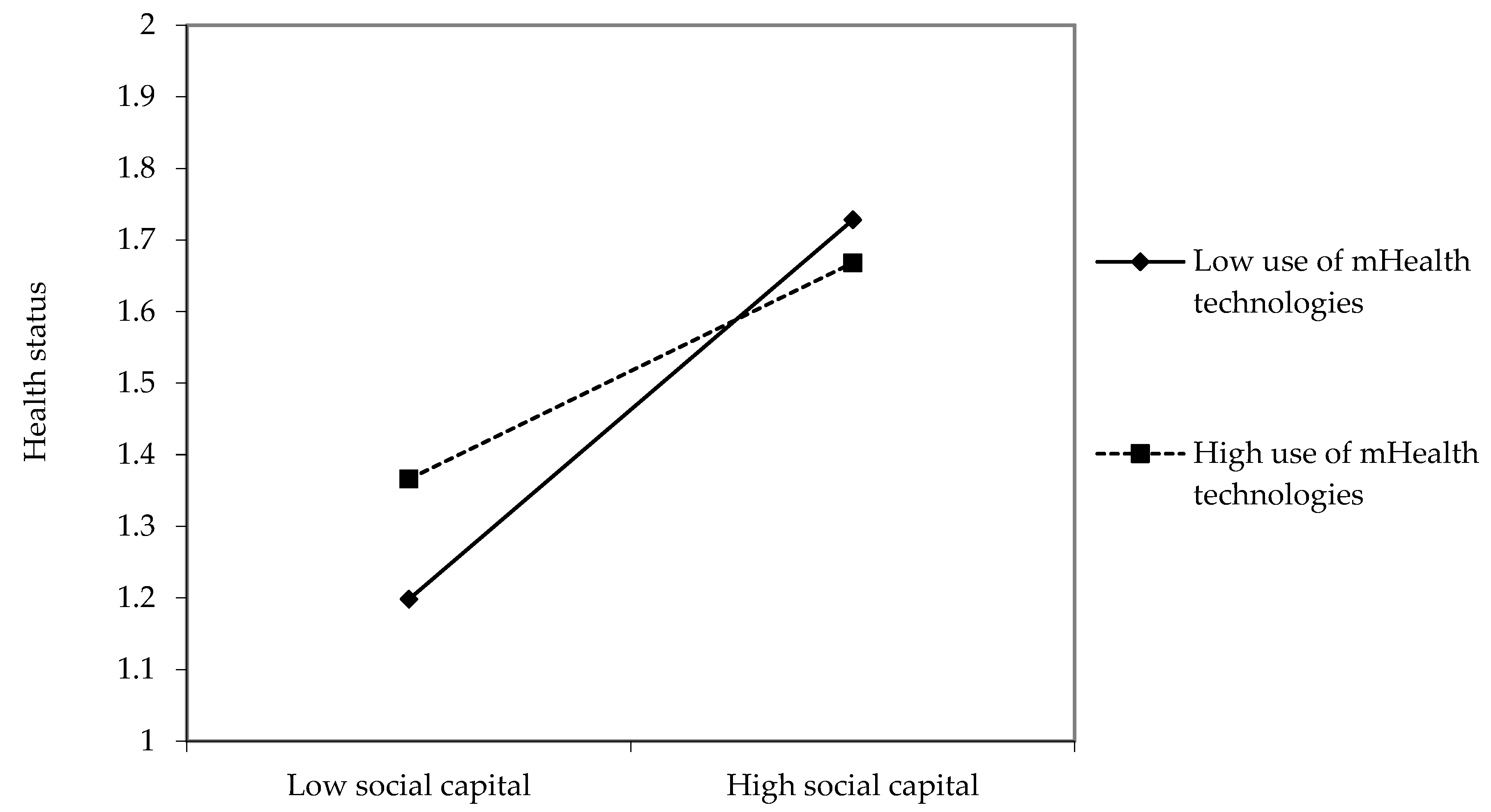
3.2. Moderating Effects of mHealth Technologies Usage
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; Final Report of the Commission on Social Determinants of Health; WHO: Geneva, Switzerland, 2008.
- Samantha, A.; Hinton, E. Beyond health care: The role of social determinants in promoting health and health equity. Health 2019, 20, 219. [Google Scholar]
- Orellano, P.; Quaranta, N.; Reynoso, J.; Balbi, B.; Vasquez, J. Effect of outdoor air pollution on asthma exacerbations in children and adults: Systematic review and multilevel meta-analysis. PLoS ONE 2017, 12, e0174050. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Xue, D.; Liu, Y.; Liu, P.; Chen, H. The relationship between air pollution and depression in China: Is neighbourhood social capital protective? Int. J. Environ. Res. Public Health 2018, 15, 1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adler, N.E.; Stewart, J. Health disparities across the lifespan: Meaning, methods, and mechanisms. Ann. N. Y. Acad. Sci. 2010, 1186, 5–23. [Google Scholar] [CrossRef]
- Kaplan, G.A.; Shema, S.J.; Leite, C.M.A. Socioeconomic determinants of psychological well-being: The role of income, income change, and income sources during the course of 29 years. Ann. Epidemiol. 2008, 18, 531–537. [Google Scholar] [CrossRef] [Green Version]
- Meara, E.R.; Richards, S.; Cutler, D.M. The gap gets bigger: Changes in mortality and life expectancy, by education, 1981–2000. Health Aff. 2008, 27, 350–360. [Google Scholar] [CrossRef] [Green Version]
- Stringhini, S.; Sabia, S.; Shipley, M.; Brunner, E.; Nabi, H.; Kivimaki, M.; Singh-Manoux, A. Association of socioeconomic position with health behaviors and mortality. JAMA 2010, 303, 1159–1166. [Google Scholar] [CrossRef] [Green Version]
- Chin, M.H.; Walters, A.E.; Cook, S.C.; Huang, E.S. Interventions to reduce racial and ethnic disparities in health care. Med. Care Res. Rev. 2007, 64, 7–28. [Google Scholar] [CrossRef] [Green Version]
- Cooper, L.A.; Hill, M.N.; Powe, N.R. Designing and evaluating interventions to eliminate racial and ethnic disparities in health care. J. Gen. Intern. Med. 2002, 17, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Dolan, P. Social support, social justice, and social capital: A tentative theoretical triad for community development. Community Dev. 2008, 39, 112–119. [Google Scholar] [CrossRef]
- El Kefi, S.; Asan, O. How technology impacts communication between cancer patients and their health care providers: A systematic literature review. Int. J. Med. Inform. 2021, 149, 104430. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, T.L.; Goldsmith, D. Social support, social networks, and health. In Handbook of Health Communication; Thompson, T.L., Dorsey, A.M., Miller, K.I., Parrott, R., Eds.; Lawrence Erlbaum: Mahwah, NJ, USA, 2003; pp. 263–284. [Google Scholar]
- Bovier, P.A.; Chamot, E.; Perneger, T.V. Perceived stress, internal resources, and social support as determinants of mental health among young adults. Qual. Life Res. 2004, 13, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Smyth, N.; Siriwardhana, C.; Hotopf, M.; Hatch, S.L. Social networks, social support and psychiatric symptoms: Social determinants and associations within a multicultural community population. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1111–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, R.J.; Williams, J.S.; Egede, L.E. Influence of race, ethnicity and social determinants of health on diabetes outcomes. Am. J. Med. Sci. 2016, 351, 366–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseinpoor, A.R.; Stewart Williams, J.; Amin, A.; Araujo de Carvalho, I.; Beard, J.; Boerma, T.; Kowal, P.; Naidoo, N.; Chatterji, S. Social determinants of self-reported health in women and men: Understanding the role of gender in population health. PLoS ONE 2012, 7, e34799. [Google Scholar]
- Taylor, S.; Field, D. Sociology of Health and Health Care; Blackwell: Oxford, UK, 2007. [Google Scholar]
- Gorman, B.K.; Read, J.N.G. Gender disparities in adult health: An examination of three measures of morbidity. J. Health Soc. Behav. 2006, 47, 95–110. [Google Scholar] [CrossRef]
- McDonough, P.; Walters, V. Gender and health: Reassessing patterns and explanations. Soc. Sci. Med. 2001, 52, 547–559. [Google Scholar] [CrossRef]
- Borrelli, B.; Ritterband, L.M. Special issue on eHealth and mHealth: Challenges and future directions for assessment, treatment, and dissemination. Health Psychol. 2015, 34, 1205–1208. [Google Scholar] [CrossRef]
- Lee, E.; Han, S.; Jo, S.H. Consumer choice of on-demand mHealth app services: Context and contents values using structural equation modeling. Int. J. Med. Inform. 2017, 97, 229–238. [Google Scholar] [CrossRef]
- Krishna, S.; Boren, S.A. Diabetes self-management care via cell phone: A systematic review. J. Diabetes Sci. Technol. 2008, 2, 509–517. [Google Scholar] [CrossRef]
- Neville, R.G.; Charnock Greene, A.; McLeod, J.; Tracey, A.; Surie, J. Mobile phone text messaging can help young people with asthma. Br. Med. J. 2002, 325, 600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vangeepuram, N.; Mayer, V.; Fei, K.; Hanlen-Rosado, E.; Andrade, C.; Wright, S.; Horowitz, C. Smartphone ownership and perspectives on health apps among a vulnerable population in East Harlem, New York. Mhealth 2018, 4, 31. [Google Scholar] [CrossRef] [PubMed]
- Stowell, E.; Lyson, M.C.; Saksono, H.; Wurth, R.C.; Jimison, H.; Pavel, M.; Parker, A.G. Designing and Evaluating mHealth Interventions for Vulnerable Populations: A Systematic Review. In Proceedings of the 2018 CHI Conference on Human Factors in Computing Systems, Montreal, QC, Canada, 21–26 April 2018; pp. 1–17. [Google Scholar]
- Qiao, S.; Li, X.; Stanton, B. Social support and HIV-related risk behaviors: A systematic review of the global literature. AIDS Behav. 2014, 18, 419–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, S.; Peters, A.L.; Agy, C.; Menchine, M. A mobile health intervention for inner city patients with poorly controlled diabetes: Proof-of-concept of the TExT-MED program. Diabetes Technol. Ther. 2012, 14, 492–496. [Google Scholar] [CrossRef]
- Burner, E.; Lam, C.N.; DeRoss, R.; Kagawa-Singer, M.; Menchine, M.; Arora, S. Using mobile health to improve social support for low-income latino patients with diabetes: A mixed-methods analysis of the feasibility trial of TExT-MED + FANS. Diabetes Technol. Ther. 2018, 20, 39–48. [Google Scholar] [CrossRef]
- Bol, N.; Helberger, N.; Weert, J.C. Differences in mobile health app use: A source of new digital inequalities? Inf. Soc. 2018, 34, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Shi, J.; Lee, K.M. The digital divide and seeking health information on smartphones in Asia: Survey study of ten countries. J. Med. Internet Res. 2022, 24, e24086. [Google Scholar] [CrossRef]
- van Deursen, A.; Helsper, E.J. The third-level digital divide: Who benefits most from being online? In Communication and Information Technologies Annual; Robinson, L., Cotton, S.R., Schulz, J., Hale, T.M., Williams, A., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2015; pp. 29–52. [Google Scholar]
- Neter, E.; Brainin, E.; Baron-Epel, O. The third digital divide in the health domain: Is Internet use for health purposes associated with health benefits? In eHealth: Current Evidence, Promises, Perils and Future Directions; Hale, T.M., Chou, W.Y.S., Cotton, S.R., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2018; pp. 153–175. [Google Scholar]
- Chiu, Y.C.; Li, F.Y. Effects of the digital divide on the prevention of food risk in Taiwan. Health Promot. Int. 2021, in press. [Google Scholar] [CrossRef]
- Kumar, D.; Hemmige, V.; Kallen, M.A.; Giordano, T.P.; Arya, M. Mobile phones may not bridge the digital divide: A look at mobile phone literacy in an underserved patient population. Cureus 2019, 11, e4104. [Google Scholar] [CrossRef] [Green Version]
- Hswen, Y.; Viswanath, K. Beyond the hype: Mobile technologies and opportunities to address health disparities. J. Mob. Technol. Med. 2015, 4, 39–40. [Google Scholar] [CrossRef]
- Ben-Zeev, D.; Davis, K.E.; Kaiser, S.; Krzsos, I.; Drake, R.E. Mobile technologies among people with serious mental illness: Opportunities for future services. Adm. Policy Ment. Health 2013, 40, 340–343. [Google Scholar] [CrossRef]
- Viswanath, K.; Nagler, R.H.; Bigman-Galimore, C.A.; McCauley, M.P.; Jung, M.; Ramanadhan, S. The communications revolution and health inequalities in the 21st century: Implications for cancer control. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1701–1708. [Google Scholar] [CrossRef] [Green Version]
- Taylor, K.; Silver, L. Smartphone Ownership is Growing Rapidly around the World, but not always Equally. 2019. Available online: https://www.pewresearch.org/global/2019/02/05/in-emerging-economies-smartphoneadoption-has-grown-more-quickly-among-younger-generations/ (accessed on 10 November 2021).
- Kakihara, M. Mobile Apps in APAC: 2016 Report. Available online: https://www.thinkwithgoogle.com/intl/en-apac/trends-and-insights/mobile-apps-in-apac-2016-report/ (accessed on 13 November 2021).
- Health Information National Trends Survey 5 Cycle 1. Survey Materials. Available online: https://hints.cancer.gov/docs/Instruments/HINTS5_Cycle1_Annotated_Instrument_English.pdf (accessed on 21 November 2021).
- Nelson, D.; Kreps, G.; Hesse, B.; Croyle, R.; Willis, G.; Arora, N.; Rimer, B.; Viswanath, K.V.; Weinstein, N.; Alden, S. The health information national trends survey (HINTS): Development, design, and dissemination. J. Health Commun. 2004, 9, 443–460. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2003. [Google Scholar]
- Lee, S.Y.; Kim, S.J.; Yoo, K.B.; Lee, S.G.; Park, E.C. Gender gap in self-rated health in South Korea compared with the United States. Int. J. Clin. Health Psychol. 2016, 16, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Chun, H.; Khang, Y.H.; Kim, I.H.; Cho, S.I. Explaining gender differences in ill-health in South Korea: The roles of socio-structural, psychosocial, and behavioral factors. Soc. Sci. Med. 2008, 67, 988–1001. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Daskalopoulou, C.; Muniz Terrera, G.; Sanchez Niubo, A.; Rodríguez-Artalejo, F.; Ayuso-Mateos, J.L.; Bobak, M.; Caballero, F.F.; de la Fuente, J.; de la Torre-Luque, A.; et al. Education and wealth inequalities in healthy ageing in eight harmonised cohorts in the ATHLOS consortium: A population-based study. Lancet Public Health 2020, 5, e386–e394. [Google Scholar] [CrossRef]
- Anderson-Lewis, C.; Darville, G.; Mercado, R.E.; Howell, S.; Di Maggio, S. mHealth technology Use and implications in historically underserved and minority populations in the United States: Systematic literature review. JMIR Mhealth Uhealth 2018, 6, e128. [Google Scholar] [CrossRef]
- Blumler, J.G.; Katz, E. The Uses of Mass Communications: Current Perspectives on Gratifications Research; SAGE: Beverly Hills, CA, USA, 1974. [Google Scholar]
- Azevedo, M.R.; Araújo, C.L.P.; Reichert, F.F.; Siqueira, F.V.; da Silva, M.C.; Hallal, P.C. Gender differences in leisure-time physical activity. Int. J. Public Health 2007, 52, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Egli, T.; Bland, H.W.; Melton, B.F.; Czech, D.R. Influence of age, sex, and race on college students’ exercise motivation of physical activity. J. Am. Coll. Health 2011, 59, 399–406. [Google Scholar] [CrossRef]
- Molanorouzi, K.; Khoo, S.; Morris, T. Motives for adult participation in physical activity: Type of activity, age, and gender. BMC Public Health 2015, 15, 66. [Google Scholar] [CrossRef] [Green Version]
- Klenk, S.; Reifegerste, D.; Renatus, R. Gender differences in gratifications from fitness app use and implications for health interventions. Mob. Media Commun. 2017, 5, 178–193. [Google Scholar] [CrossRef] [Green Version]
- Courtenay, W. Key determinants of the health and well-being of men and boys. Int. J. Men’s Health 2003, 2, 1–30. [Google Scholar] [CrossRef]
- Lucivero, F.; Jongsma, K.R. A mobile revolution for healthcare? Setting the agenda for bioethics. J. Med. Ethics 2018, 44, 685–689. [Google Scholar]
- Sama, P.R.; Eapen, Z.J.; Weinfurt, K.P.; Shah, B.R.; Schulman, K.A. An evaluation of mobile health application tools. JMIR Mhealth Uhealth 2014, 2, e3088. [Google Scholar] [CrossRef]
- Anderson, K.; Burford, O.; Emmerton, L. Mobile health apps to facilitate self-care: A qualitative study of user experiences. PLoS ONE 2016, 11, e0156164. [Google Scholar] [CrossRef] [Green Version]
- Denton, M.; Walters, V. Gender differences in structural and behavioral determinants of health: An analysis of the social production of health. Soc. Sci. Med. 1999, 48, 1221–1235. [Google Scholar] [CrossRef]
- Marmot, M.G.; Bosma, H.; Hemingway, H.; Brunner, E.; Stansfeld, S. Contribution of job control and other risk factors to social variations in coronary heart disease incidence. Lancet 1997, 350, 235–239. [Google Scholar] [CrossRef]
- Kim, H.; Goldsmith, J.V.; Sengupta, S.; Mahmood, A.; Powell, M.P.; Bhatt, J.; Chang, C.F.; Bhuyan, S.S. Mobile health application and e-health literacy: Opportunities and concerns for cancer patients and caregivers. J. Cancer Educ. 2019, 34, 3–8. [Google Scholar] [CrossRef]
- Potdar, R.; Thomas, A.; DiMeglio, M.; Mohiuddin, K.; Djibo, D.A.; Laudanski, K.; Dourado, C.M.; Leighton, J.C.; Ford, J.G. Access to internet, smartphone usage, and acceptability of mobile health technology among cancer patients. Support. Care Cancer 2020, 28, 5455–5461. [Google Scholar] [CrossRef]
- Smith, B.; Magnani, J.W. New technologies, new disparities: The intersection of electronic health and digital health literacy. Int. J. Cardiol. 2019, 292, 280–282. [Google Scholar] [CrossRef]
- Abbaspur-Behbahani, S.; Monaghesh, E.; Hajizadeh, A.; Fehresti, S. Application of mobile health to support the elderly during the COVID-19 outbreak: A systematic review. Health Policy Technol. 2022, in press. [Google Scholar] [CrossRef]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc. Sport 2000, 71, 1–14. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants (N = 1187) | |
|---|---|
| Age (years)Mean (SD) | 43.96 (13.13) |
| Gender | |
| Male | 583 (49.1%) |
| Female | 604 (50.9%) |
| Education | |
| High school or less | 258 (21.7%) |
| Some college or associate’s degree | 191 (16.1%) |
| Bachelor’s degree | 634 (53.4%) |
| Graduate degree | 104 (8.8%) |
| Monthly household income | |
| Less than 2.00 million Korean won ($1794 USD) | 121 (10.2%) |
| 2.01–3.00 million Korean won ($2691 USD) | 176 (14.8%) |
| 3.01–4.00 million Korean won ($3587 USD) | 207 (17.4%) |
| 4.01–5.00 million Korean won ($4484 USD) | 218 (18.4%) |
| 5.01–6.00 million Korean won ($5381 USD) | 158 (13.3%) |
| 6.01–7.00 million Korean won ($6278 USD) | 102 (8.6%) |
| 7.01–8.00 million Korean won ($7175 USD) | 80 (6.7%) |
| 8.01 or more Korean won | 125 (10.5%) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Gender | 1.00 | |||||||
| 2. Education | −0.15 *** | 1.00 | ||||||
| 3. Monthly household income | 0.04 | 0.22 *** | 1.00 | |||||
| 4. Social capital | 0.05 | 0.12 *** | 0.18 *** | 1.00 | ||||
| 5. Healthcare quality | −0.05 | 0.02 | 0.04 | 0.26 *** | 1.00 | |||
| 6. Use of mHealth technologies | −0.03 | 0.11 *** | 0.13 *** | 0.15 *** | 0.17 *** | 1.00 | ||
| 7. Health self-efficacy | −0.13 *** | 0.12 *** | 0.14 *** | 0.34 *** | 0.21 *** | 0.18 *** | 1.00 | |
| 8. Health status | −0.05 | 0.12 *** | 0.14 *** | 0.27 *** | 0.25 *** | 0.11 *** | 0.49 *** | 1.00 |
| Health Self–Efficacy | Health Status | |
|---|---|---|
| Block 1. Social determinants of health | ||
| Gender (Male = 0) | −0.14 *** | −0.05 |
| Education | 0.05 | 0.07 * |
| Monthly household income | 0.09 ** | 0.08 ** |
| Social capital | 0.29 *** | 0.21 *** |
| Healthcare quality | 0.12 *** | 0.17 *** |
| ∆R2 (%) | 0.158 *** | 0.120 *** |
| Block 2. Moderator | ||
| Use of mHealth technologies | 0.10 *** | 0.03 |
| ∆R2 (%) | 0.01 *** | 0.001 |
| Block 3. Interactions | ||
| Gender × Use of mHealth technologies | 0.00 | 0.08 ** |
| Education × Use of mHealth technologies | 0.02 | 0.00 |
| Monthly household income × Use of mHealth technologies | −0.06 * | −0.03 |
| Social capital × Use of mHealth technologies | −0.06 * | −0.06 * |
| Healthcare quality × Use of mHealth technologies | 0.03 | 0.01 |
| ∆R2 (%) | 0.008 * | 0.011 * |
| Total ∆R2 (%) | 0.177 *** | 0.132 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, W. Addressing the Social Determinants of Health in South Korea: Moderating Role of mHealth Technologies. Int. J. Environ. Res. Public Health 2022, 19, 1871. https://doi.org/10.3390/ijerph19031871
Yoo W. Addressing the Social Determinants of Health in South Korea: Moderating Role of mHealth Technologies. International Journal of Environmental Research and Public Health. 2022; 19(3):1871. https://doi.org/10.3390/ijerph19031871
Chicago/Turabian StyleYoo, Woohyun. 2022. "Addressing the Social Determinants of Health in South Korea: Moderating Role of mHealth Technologies" International Journal of Environmental Research and Public Health 19, no. 3: 1871. https://doi.org/10.3390/ijerph19031871
APA StyleYoo, W. (2022). Addressing the Social Determinants of Health in South Korea: Moderating Role of mHealth Technologies. International Journal of Environmental Research and Public Health, 19(3), 1871. https://doi.org/10.3390/ijerph19031871