
Do Sleep Disturbances Improve Following Psychoanalytic Psychotherapy for Adolescent Depression?



Abstract
:1. Introduction
2. Materials and Methods
2.1. The First Experimental Study of Transference Work—In Teenagers (FEST-IT)
2.1.1. Patient Material
2.1.2. Treatment and Therapists
2.1.3. Evaluation
2.2. Ethics
2.3. Measures in the Present Study
2.3.1. Symptom Checklist 90 Revised (SCL-90-R)
2.3.2. Beck Depression Inventory (BDI-II)
2.4. Statistics
Missing Data
3. Results
3.1. Descriptive Statistics of Sleep Problems at Baseline
3.2. Correlation between Depression and Sleep
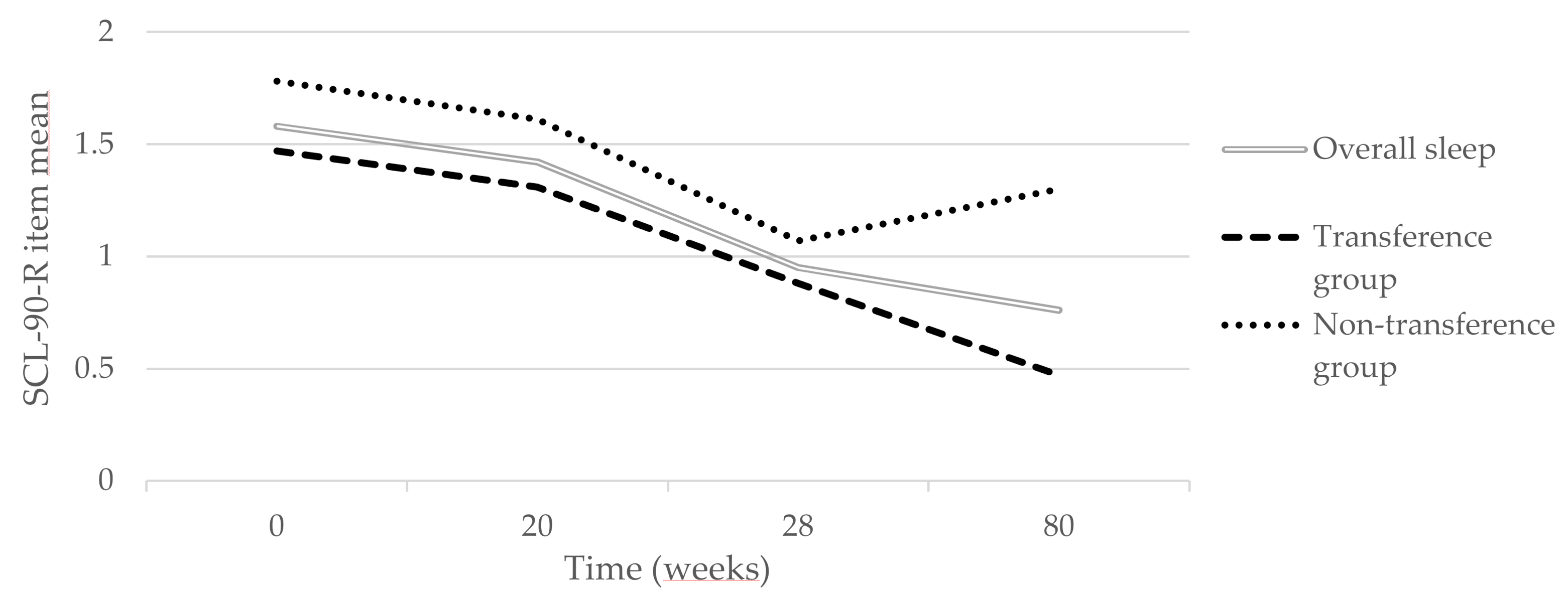
3.3. Change Trajectories for the Two Treatment Groups
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reynolds, S.; Orchard, F.; Midgley, N.; Kelvin, R.; Goodyer, I.; The IMPACT consortium. Do sleep disturbances in depressed adolescents improve following psychological treatment for depression? J. Affect. Disord. 2020, 262, 205–210. [Google Scholar] [CrossRef]
- Orchard, F.; Pass, L.; Marshall, T.; Reynolds, S. Clinical characteristics of adolescents referred for treatment of depressive disorders. Child Adolesc. Ment. Health 2017, 22, 61–68. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Pub: Arlington, TX, USA, 2013. [Google Scholar]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Nutt, D.; Wilson, S.; Paterson, L. Sleep disorders as core symptoms of depression. Dialogues Clin. Neurosci. 2008, 10, 329–336. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR, 4th ed.; American Psychiatric Press: Washington, DC, USA, 2000. [Google Scholar]
- Tsuno, N.; Besset, A.; Ritchie, K. Sleep and depression. J. Clin. Psychiatry 2005, 66, 1254–1269. [Google Scholar] [CrossRef] [PubMed]
- Asarnow, L.D.; Mirchandaney, R. Sleep and Mood Disorders Among Youth. Child Adolesc. Psychiatr. Clin. N. Am. 2021, 30, 251–268. [Google Scholar] [CrossRef]
- Lovato, N.; Gradisar, M. A meta-analysis and model of the relationship between sleep and depression in adolescents: Recommendations for future research and clinical practice. Sleep Med. Rev. 2014, 18, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Buysse, D.J.; Gentzler, A.L.; Kiss, E.; Mayer, L.; Kapornai, K.; Vetro, A.; Kovacs, M. Insomnia and hypersomnia associated with depressive phenomenology and comorbidity in childhood depression. Sleep 2007, 30, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, C.; Andrade, B.; Campisi, S.C.; Wong, M.; Zhao, H.; Jing, X.; Aitken, M.; Bonato, S.; Haltigan, J.; Wang, W.; et al. Association Between Disturbed Sleep and Depression in Children and Youths: A Systematic Review and Meta-analysis of Cohort Studies. JAMA Netw. Open 2021, 4, e212373. [Google Scholar] [CrossRef]
- Freeman, D.; Sheaves, B.; Waite, F.; Harvey, A.G.; Harrison, P.J. Sleep disturbance and psychiatric disorders. Lancet Psychiatry 2020, 7, 628–637. [Google Scholar] [CrossRef]
- Urrila, A.S.; Karlsson, L.; Kiviruusu, O.; Pelkonen, M.; Strandholm, T.; Marttunen, M. Sleep complaints among adolescent outpatients with major depressive disorder. Sleep Med. 2012, 13, 816–823. [Google Scholar] [CrossRef]
- Goodyer, I.M.; Reynolds, S.; Barrett, B.; Byford, S.; Dubicka, B.; Hill, J.; Holland, F.; Kelvin, R.; Midgley, N.; Roberts, C.; et al. Cognitive behavioural therapy and short-term psychoanalytical psychotherapy versus a brief psychosocial intervention in adolescents with unipolar major depressive disorder (IMPACT): A multicentre, pragmatic, observer-blind, randomised controlled superiority trial. Lancet Psychiatry 2017, 4, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Ulberg, R.; Hummelen, B.; Hersoug, A.G.; Midgley, N.; Hoglend, P.A.; Dahl, H.J. The first experimental study of transference work-in teenagers (FEST-IT): A multicentre, observer- and patient-blind, randomised controlled component study. BMC Psychiatry 2021, 21, 106. [Google Scholar] [CrossRef]
- Ulberg, R.; Hersoug, A.G.; Hoglend, P. Treatment of adolescents with depression: The effect of transference interventions in a randomized controlled study of dynamic psychotherapy. Trials 2012, 13, 159. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33, quiz 34–57. [Google Scholar]
- Pfohl, B.; Blum, N.; Zimmerman, M. Structured Interview for DSM-IV Personality: Sidp-IV; American Psychiatric Pub: Washington, DC, USA, 1997. [Google Scholar]
- Aas, I.H. Guidelines for rating Global Assessment of Functioning (GAF). Ann. Gen. Psychiatry 2011, 10, 2. [Google Scholar] [CrossRef]
- Ness, E.; Dahl, H.J.; Tallberg, P.; Amlo, S.; Hoglend, P.; Thoren, A.; Egeland, J.; Ulberg, R. Assessment of dynamic change in psychotherapy with asdolescents. Child Adolesc. Psychiatry Ment. Health 2018, 12, 39. [Google Scholar] [CrossRef] [PubMed]
- Midgley, N.; Rhode, M.; Rustin, M.; Hughes, C.; Cregeen, S. IMPACT Group: Short-Term Psychoanalytic Psychotherapy (STPP) for Adolescents with Moderate or Severe Depression: A Treatment Manual; IMPACT Trial Office: Cambridge, UK, 2010. [Google Scholar]
- Ulberg, R. Psykodynamisk korttidspsykoterapi med ungdom: STPP. Mellanrummet 2008, 19, 135–144. [Google Scholar]
- Derogatis, L. SCL-90-R: Administration, scoring & procedures manual-II for the (revised) version and other instruments of the psychopathology rating scale series. Clin. Psychom. Res. 1992, 1–16. Available online: https://books.google.com.sg/books/about/SCL_90_R_Administration_Scoring_and_Proc.html?id=PRUBPAAACAAJ&redir_esc=y (accessed on 23 December 2021).
- Rytila-Manninen, M.; Frojd, S.; Haravuori, H.; Lindberg, N.; Marttunen, M.; Kettunen, K.; Therman, S. Psychometric properties of the Symptom Checklist-90 in adolescent psychiatric inpatients and age- and gender-matched community youth. Child Adolesc. Psychiatry Ment. Health 2016, 10, 23. [Google Scholar] [CrossRef]
- Siqveland, J.; Moum, T.; Leiknes, K. Psychometric Assessment of the Norwegian Version of the Symptom Checklist 90 Revised (SCL-90-R); Folkehelseinstituttet: Oslo, Norway, 2016; ISBN 978-82-8082-788-3. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories-IA and -II in psychiatric outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.P.; Gorenstein, C. Psychometric properties of the Beck Depression Inventory-II: A comprehensive review. Braz. J. Psychiatry 2013, 35, 416–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis; John Wiley & Sons: New York, NY, USA, 2012; Volume 998. [Google Scholar]
- Owens, J.; Adolescent Sleep Working, G.; Committee on, A. Insufficient sleep in adolescents and young adults: An update on causes and consequences. Pediatrics 2014, 134, e921–e932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradisar, M.; Gardner, G.; Dohnt, H. Recent worldwide sleep patterns and problems during adolescence: A review and meta-analysis of age, region, and sleep. Sleep Med. 2011, 12, 110–118. [Google Scholar] [CrossRef]
- Mayers, A.G.; Grabau, E.A.; Campbell, C.; Baldwin, D.S. Subjective sleep, depression and anxiety: Inter-relationships in a non-clinical sample. Hum. Psychopharmacol. 2009, 24, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Lorenzo-Luaces, L. Heterogeneity in the prognosis of major depression: From the common cold to a highly debilitating and recurrent illness. Epidemiol. Psychiatr. Sci. 2015, 24, 466–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keers, R.; Uher, R. Gene-environment interaction in major depression and antidepressant treatment response. Curr. Psychiatry Rep. 2012, 14, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Hazell, P. Updates in treatment of depression in children and adolescents. Curr. Opin. Psychiatry 2021, 34, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Philips, B.; Falkenstrom, F. What Research Evidence Is Valid for Psychotherapy Research? Front. Psychiatry 2020, 11, 625380. [Google Scholar] [CrossRef] [PubMed]
- Ness, E. Measuring Psychodynamic Process and Change in Psychoterapy. Ph.D Thesis, Faculty of Medicine, University of Oslo, Oslo, Norway, 2019. [Google Scholar]
- Armitage, R.; Hoffmann, R.F. Sleep EEG, depression and gender. Sleep Med. Rev. 2001, 5, 237–246. [Google Scholar] [CrossRef]
- Kanstrup, M.; Holmstrom, L.; Ringstrom, R.; Wicksell, R.K. Insomnia in paediatric chronic pain and its impact on depression and functional disability. Eur. J. Pain 2014, 18, 1094–1102. [Google Scholar] [CrossRef]
- Yilmaz, E.; Sedky, K.; Bennett, D.S. The relationship between depressive symptoms and obstructive sleep apnea in pediatric populations: A meta-analysis. J. Clin. Sleep Med. 2013, 9, 1213–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, T.; Broglia, E.; Pushpakumar, D.; Lodhi, T.; Taheri, S. An investigation into the strength of the association and agreement levels between subjective and objective sleep duration in adolescents. PLoS ONE 2013, 8, e72406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Austad, S.B.; Follesø, H.S. Setting the Rest Interval in Actigraphy—A Systematic Review and Development of a Novel Manual. Master‘s Thesis, Norwegian University of Science and Technology (NTNU), Trondheim, Norway, 2018. [Google Scholar]
- Gupta, P.; Sagar, R.; Mehta, M. Subjective sleep problems and sleep hygiene among adolescents having depression: A case-control study. Asian J. Psychiatr. 2019, 44, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.N.; Rowe, H.; Repa, L.M.; Fowler, K.; Zhou, E.S.; Grandner, M.A. A decade’s difference: 10-year change in insomnia symptom prevalence in Canada depends on sociodemographics and health status. Sleep Health 2018, 4, 160–165. [Google Scholar] [CrossRef]
- Gregory, A.M.; Sadeh, A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med. Rev. 2012, 16, 129–136. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Transference Work Group (n = 39) | Non-Transference Work Group (n = 30) | |||
|---|---|---|---|---|
| N | % | N | % | |
| Female gender | 33 | 84.6 | 24 | 80.0 |
| Axis I diagnosis | ||||
| Depressive disorder | 39 | 100.0 | 30 | 100.0 |
| Prevalence of one or more comorbid diagnoses | 18 | 46.2 | 16 | 53.3 |
| Social phobia | 7 | 17.9 | 3 | 10.0 |
| Panic disorder | 2 | 5.1 | 4 | 13.3 |
| Agoraphobia | 5 | 12.8 | 3 | 10.0 |
| PTSD | 1 | 2.6 | 1 | 3.3 |
| Mean (N = 39) | (SD) | Mean (N = 30) | (SD) | |
| Age | 17.3 | 0.7 | 17.3 | 0.7 |
| BDI | 28.5 | 9.5 | 28.8 | 8.3 |
| GAF 1 | 59.6 | 5.5 | 59.2 | 5.0 |
| MADRS * | 20.8 | 4.5 | 24.0 | 6.1 |
| GSI | 1.2 | 0.4 | 1.6 | 0.6 |
| Axis II diagnoses as measured with SIDP-IV (PD criteria) | 13.5 | 9.0 | 12.4 | 7.8 |
| Trouble Falling Asleep | Restless or Disturbed Sleep | Early Morning Awakening | |
|---|---|---|---|
| Not at all | 17.6 | 31.3 | 58.8 |
| A little bit | 10.3 | 16.4 | 13.2 |
| Moderately | 23.5 | 19.4 | 13.2 |
| Quite a bit | 22.1 | 19.4 | 7.4 |
| Extremely | 26.1 | 13.4 | 7.4 |
| Trouble Falling Asleep | Restless or Disturbed Sleep | Early Morning Awakening | ||||
|---|---|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | Mean | (SD) | |
| Transference work group (n = 39) | 2.07 | 1.54 | 1.54 | 1.41 | 1.05 | 1.45 |
| Non-transference work group (n = 29) | 2.59 | 1.21 | 1.86 | 1.48 | 0.72 | 1.06 |
| Number of Sleep Symptoms | Baseline (0 Weeks) n = 68 | Session 20 (20 Weeks) n = 37 | End of Treatment (28 Weeks) n = 58 | Follow-Up (80 Weeks) n = 46 |
|---|---|---|---|---|
| 0 | 5.9 | 16.2 | 20.7 | 37 |
| >0–1 | 28.0 | 35.1 | 34.5 | 26 |
| >1–2 | 35.3 | 29.7 | 32.8 | 22 |
| >2–3 | 19.1 | 10.8 | 12.0 | 15 |
| >3–4 | 7.4 | 8.1 | 0 | 0 |
| Sleep Difficulties | Estimate | SE | CI (95%) | t-Value | F-Value | p |
|---|---|---|---|---|---|---|
| From baseline to post-treatment | ||||||
| Time1 a | −0.15 | 0.05 | −0.26 to −0.05 | −2.8 | 15.9 | 0.005 |
| Time1 × treatment b | −0.05 | 0.07 | −0.20 to 0.09 | −0.74 | 0.5 | 0.460 |
| Posttreatment to one-year follow-up | ||||||
| Time2 a | −0.07 | 0.04 | −0.14 to 0.006 | −1.8 | 1.1 | 0.069 |
| Time2 × treatment b | 0.08 | 0.06 | −0.04 to 0.20 | 1.3 | 1.7 | 0.185 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schønning, T.; Dahl, H.-S.J.; Hummelen, B.; Ulberg, R. Do Sleep Disturbances Improve Following Psychoanalytic Psychotherapy for Adolescent Depression? Int. J. Environ. Res. Public Health 2022, 19, 1790. https://doi.org/10.3390/ijerph19031790
Schønning T, Dahl H-SJ, Hummelen B, Ulberg R. Do Sleep Disturbances Improve Following Psychoanalytic Psychotherapy for Adolescent Depression? International Journal of Environmental Research and Public Health. 2022; 19(3):1790. https://doi.org/10.3390/ijerph19031790
Chicago/Turabian StyleSchønning, Thea, Hanne-Sofie Johnsen Dahl, Benjamin Hummelen, and Randi Ulberg. 2022. "Do Sleep Disturbances Improve Following Psychoanalytic Psychotherapy for Adolescent Depression?" International Journal of Environmental Research and Public Health 19, no. 3: 1790. https://doi.org/10.3390/ijerph19031790
APA StyleSchønning, T., Dahl, H.-S. J., Hummelen, B., & Ulberg, R. (2022). Do Sleep Disturbances Improve Following Psychoanalytic Psychotherapy for Adolescent Depression? International Journal of Environmental Research and Public Health, 19(3), 1790. https://doi.org/10.3390/ijerph19031790