
Social Determinants of Remaining Life Expectancy at Age 60: A District-Level Analysis in Germany


Abstract
1. Introduction
- (1)
- How large are the differences in district-level remaining life expectancy for 60-year-old men and women in Germany?
- (2)
- Is there a specific geographic distribution pattern of areas with high or low remaining life expectancy in Germany (both among men and women)? How similar are the spatial distribution patterns of men’s and women’s remaining life expectancy at age 60?
- (3)
- Which social determinants explain the existing differences in district-level remaining life expectancy of 60-year-old men and women in statistical terms?
2. Data and Methods
2.1. Data
2.2. Methods to Investigate the Research Questions
2.3. Potential Social Determinants of Men’s and Women’s Remaining Life Expectancy at Age 60 at District Level
3. Results
3.1. Remaining Life Expectancy at Age 60 in Germany and in German Districts (2015/17)
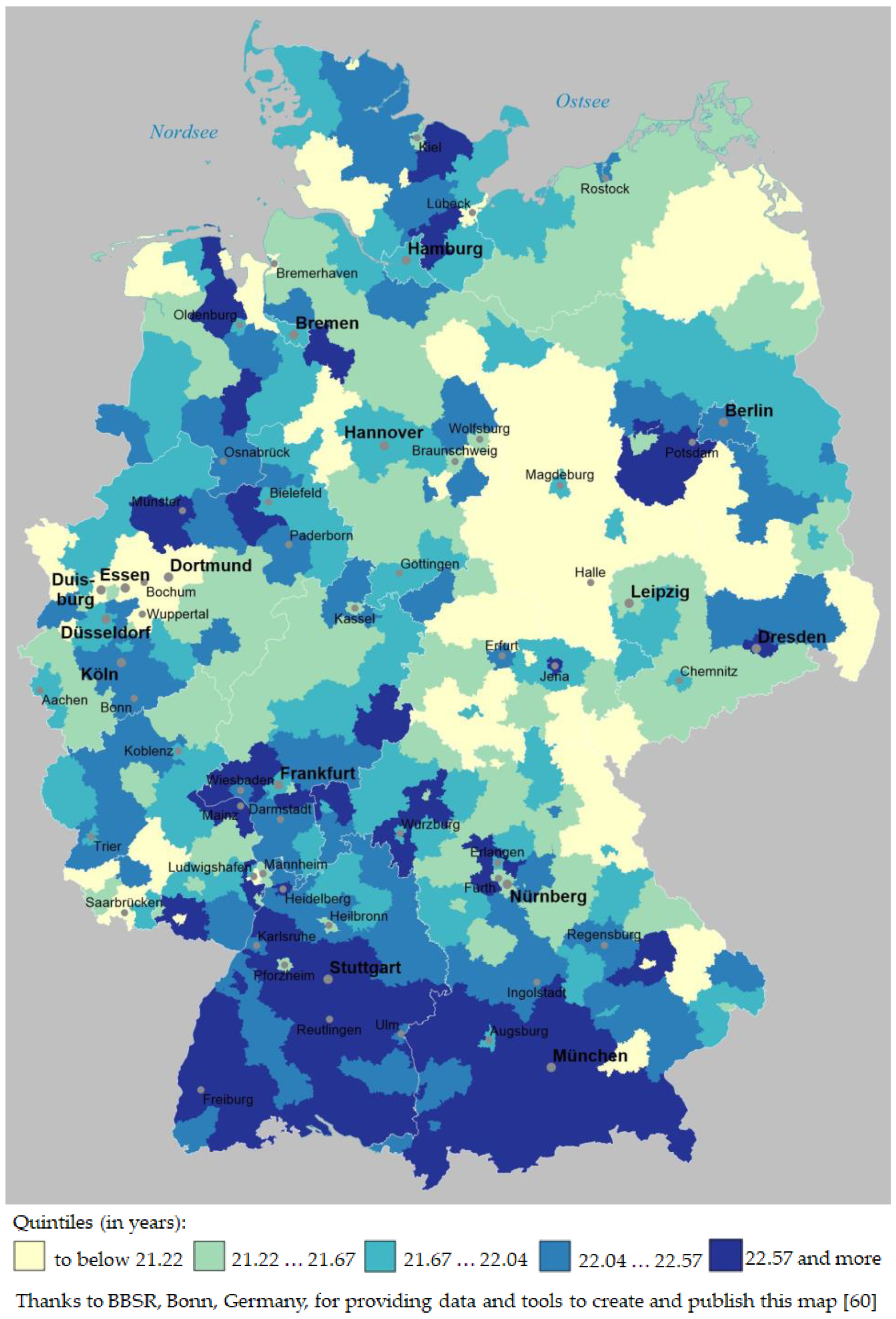
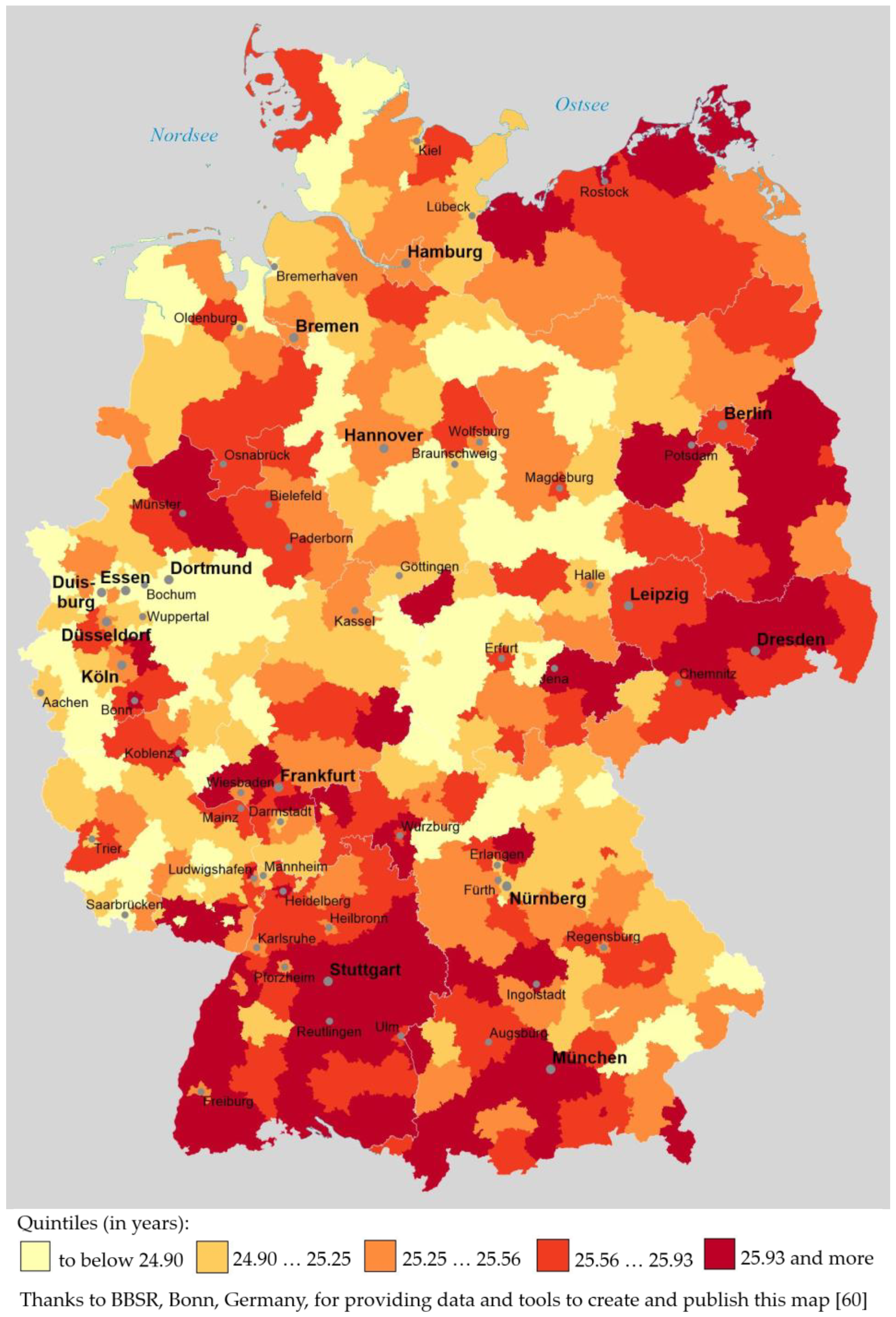
3.2. Geographical Distribution of RLE in German Districts (2015/17), Grouped in RLE Quintiles
3.3. Analyzing Potential Predictors of Men’s and Women’s Remaining Life Expectancy at Age 60 Using Bivariate Regression Analyses
3.4. Analyzing Potential Predictors of Men’s and Women’s Remaining Life Expectancy at Age 60 Using Multivariate Regression Analyses
4. Discussion
4.1. Discussion of the Results That Provide Answers to Research Questions (1) and (2)
4.2. Discussion of the Results That Provide Answers to Research Question (3)
4.2.1. Selection of the Potential Predictors of Remaining Life Expectancy at Old Age
4.2.2. Discussion of the Results of the Bivariate Regression Models
4.2.3. Discussion of the Multiple Regression Models
- (i)
- (ii)
- Only second and third in rank were classic economic predictors: in case of men’s RLE, these indicators were ‘household income’ (ß = 0.27) and ‘unemployment’ (ß = −0.23) and in case of women’s RLE ‘proportion of elder with financial elder support’ (ß = −0.30) and ‘unemployment’ (ß = −0.23).
- (iii)
- Furthermore, variables reflecting the availability of health services or the staffing level of care services for the elder—i.e., indicators (1)–(4) in Table 1—had an at best marginal partial impact on the outcome variables: in case of men’s RLE, only ‘care personnel per 100 persons in need of full inpatient care’ had a very small positive impact (ß = 0.16); in case of women’s RLE, none of those four indicators had a statistically significant partial impact on the target variable.
- (iv)
- Finally, for both men’s and women’s RLE at district level, ‘voter turnout’ had a far smaller association in the multiple regression models than in the bivariate regression models: with regard to men’s RLE, its ß value decreased from 0.67 in the bivariate to 0.15 in the multivariate analysis; for women’s RLE, there was not even a significant partial impact of ‘voter turnout’ in the multiple regression model, whereas in the bivariate model it had been 0.38.
4.3. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Latzitis, N.; Sundmacher, L.; Busse, R. [Regional Differences in Life Expectancy in Germany at County Levels and their Possible Determinants.] Regionale Unterschiede der Lebenserwartung in Deutschland auf Ebene der Kreise und kreisfreien Städte und deren möglichen Determinanten. Gesundheitswesen 2011, 73, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Rau, R.; Schmertmann, C.P. District-Level Life Expectancy in Germany. Dtsch. Arztebl. Int. 2020, 117, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Marmot, M.; Bell, R. Social inequalities in health: A proper concern of epidemiology. Ann. Epidemiol. 2016, 26, 238–240. [Google Scholar] [CrossRef]
- Kim, I.; Kang, H.Y.; Khang, Y.H. Life Expectancy in Areas around Subway Stations in the Seoul Metropolitan Area in Korea, 2008–2017. J. Korean Med. Sci. 2020, 35, e365. [Google Scholar] [CrossRef] [PubMed]
- Luy, M.; Di Giulio, P.; Di Lego, V.; Lazarevič, P.; Sauerberg, M. Life Expectancy: Frequently Used, but Hardly Understood. Gerontology 2020, 66, 95–104. [Google Scholar] [CrossRef]
- Luy, M. [Differential Mortality: The Unequal Distribution of Life Expectancy in Germany]. Differentielle Sterblichkeit: Die Ungleiche Verteilung der Lebenserwartung in Deutschland, Rostock, 2006. Available online: https://www.rostockerzentrum.de/content/publikationen/rz_diskussionpapier_6.pdf (accessed on 14 November 2021).
- Statistisches Bundesamt. [Period Life Tables 2018/20]. Periodensterbetafel 2018/2020. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Sterbefaelle-Lebenserwartung/Publikationen/Downloads-Sterbefaelle/periodensterbetafel-erlaeuterung-5126203207004.html (accessed on 10 December 2021).
- Preston, S.H.; Heuveline, P.; Guillot, M. Demography: Measuring and Modeling Population Processes, [Nachdr.]; Blackwell: Oxford, UK, 2009; ISBN 9781557864512. [Google Scholar]
- Harper, S. Demography: A Very Short Introduction, 1st ed.; Oxford University Press: Oxford, UK, 2018; ISBN 9780198725732. [Google Scholar]
- Morland, P. The Human Tide: How Population Shaped the Modern World, 1st ed.; PublicAffairs: New York, NY, USA, 2019; ISBN 9781541788367. [Google Scholar]
- Lindgren, M. Guessing Life Expectancy for Disasters. Available online: https://www.gapminder.org/documentation/documentation/Gapdoc004%20Guessing%20LEX.pdf (accessed on 10 December 2021).
- Plümper, T.; Neumayer, E. The Unequal Burden of War: The Effect of Armed Conflict on the Gender Gap in Life Expectancy. Int. Org. 2006, 60, 723–754. [Google Scholar] [CrossRef]
- Preston, S.H. The changing relation between mortality and level of economic development. Popul. Stud. 1975, 29, 231–248. [Google Scholar] [CrossRef]
- Cutler, D.; Deaton, A.; Lleras-Muney, A. The Determinants of Mortality. J. Econ. Perspect. 2006, 20, 97–120. [Google Scholar] [CrossRef]
- Wilmoth, J.R. Demography of longevity: Past, present, and future trends. Exp. Gerontol. 2000, 35, 1111–1129. [Google Scholar] [CrossRef]
- Omran, A.R. The epidemiologic transition. A theory of the epidemiology of population change. Milbank Mem. Fund Q. 1971, 49, 509–538. [Google Scholar] [CrossRef] [PubMed]
- Olshansky, S.J.; Ault, A.B. The fourth stage of the epidemiologic transition: The age of delayed degenerative diseases. Milbank Q. 1986, 64, 355–391. [Google Scholar] [CrossRef]
- Omran, A.R. The epidemiologic transition theory. A preliminary update. J. Trop. Pediatric 1983, 29, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Looman, C.W.; Kunst, A.E.; Habbema, J.F.; van der Maas, P.J. Post-1950 mortality trends and medical care: Gains in life expectancy due to declines in mortality from conditions amenable to medical intervention in The Netherlands. Soc. Sci. Med. 1988, 27, 889–894. [Google Scholar] [CrossRef]
- Mackenbach, J.P. Political conditions and life expectancy in Europe, 1900–2008. Soc. Sci. Med. 2013, 82, 134–146. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Hu, Y.; Looman, C.W. Democratization and life expectancy in Europe, 1960–2008. Soc. Sci. Med. 2013, 93, 166–175. [Google Scholar] [CrossRef]
- Trias-Llimós, S.; Bilal, U.; Franco, M.; Blanes, A.; Riffe, T. [Decrease in life expectancy in 2020 and SARS-CoV-2 seroprevalence]. Caídas en la esperanza de vida en 2020 y seroprevalencia del SARS-CoV-2. Gac. Sanit. 2021. [Google Scholar] [CrossRef]
- Aburto, J.M.; Schöley, J.; Kashnitsky, I.; Zhang, L.; Rahal, C.; Missov, T.I.; Mills, M.C.; Dowd, J.B.; Kashyap, R. Quantifying impacts of the COVID-19 pandemic through life-expectancy losses: A population-level study of 29 countries. Int. J. Epidemiol. 2021, dyab207. [Google Scholar] [CrossRef]
- Aburto, J.M.; Kashyap, R.; Schöley, J.; Angus, C.; Ermisch, J.; Mills, M.C.; Dowd, J.B. Estimating the burden of the COVID-19 pandemic on mortality, life expectancy and lifespan inequality in England and Wales: A population-level analysis. J. Epidemiol. Community Health 2021, 75, 735–740. [Google Scholar] [CrossRef]
- Chan, E.Y.S.; Cheng, D.; Martin, J. Impact of COVID-19 on excess mortality, life expectancy, and years of life lost in the United States. PLoS ONE 2021, 16, e0256835. [Google Scholar] [CrossRef]
- Díaz-Olalla, J.M.; Valero-Oteo, I.; Moreno-Vázquez, S.; Blasco-Novalbos, G.; del Moral-Luque, J.A.; Haro-León, A. [Decline in life expectancy in Madrid’s districts in 2020: Its correlation with social determinants]. Caída de la esperanza de vida en distritos de Madrid en 2020: Relación con determinantes sociales. Gac. Sanit. 2021. [Google Scholar] [CrossRef]
- Islam, N.; Jdanov, D.A.; Shkolnikov, V.M.; Khunti, K.; Kawachi, I.; White, M.; Lewington, S.; Lacey, B. Effects of COVID-19 pandemic on life expectancy and premature mortality in 2020: Time series analysis in 37 countries. BMJ 2021, 375, e066768. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Yadav, P.K.; Yadav, N. Impact of COVID-19 on life expectancy at birth in India: A decomposition analysis. BMC Public Health 2021, 21, 1906. [Google Scholar] [CrossRef] [PubMed]
- Andrasfay, T.; Goldman, N. Reductions in US life expectancy from COVID-19 by Race and Ethnicity: Is 2021 a repetition of 2020? medRxiv 2021. [Google Scholar] [CrossRef]
- Kataoka, A.; Fukui, K.; Sato, T.; Kikuchi, H.; Inoue, S.; Kondo, N.; Nakaya, T.; Ito, Y. Geographical socioeconomic inequalities in healthy life expectancy in Japan, 2010–2014: An ecological study. Lancet Reg. Health-West. Pac. 2021, 14, 100204. [Google Scholar] [CrossRef] [PubMed]
- Rashid, T.; Bennett, J.E.; Paciorek, C.J.; Doyle, Y.; Pearson-Stuttard, J.; Flaxman, S.; Fecht, D.; Toledano, M.B.; Li, G.; Daby, H.I.; et al. Life expectancy and risk of death in 6791 communities in England from 2002 to 2019: High-resolution spatiotemporal analysis of civil registration data. Lancet Public Health 2021, 6, e805–e816. [Google Scholar] [CrossRef]
- Laborde, C.; Crouzet, M.; Carrère, A.; Cambois, E. Contextual factors underpinning geographical inequalities in disability-free life expectancy in 100 French départements. Eur. J. Ageing 2021, 18, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Mackenbach, J.P.; van Lenthe, F.J.; Mokdad, A.H.; Murray, C.J.L. Inequalities in Life Expectancy Among US Counties, 1980 to 2014: Temporal Trends and Key Drivers. JAMA Intern. Med. 2017, 177, 1003–1011. [Google Scholar] [CrossRef] [PubMed]
- Roubal, A.M.; Pollock, E.A.; Gennuso, K.P.; Blomme, C.K.; Givens, M.L. Comparative Methodologic and Practical Considerations for Life Expectancy as a Public Health Mortality Measure. Public Health Rep. 2021, 33354921999407. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.-K.; Kang, H.-Y.; Kim, I.; Khang, Y.-H. Spatio-temporal Analysis of District-level Life Expectancy from 2004 to 2017 in Korea. J. Korean Med. Sci. 2020, 36, e8. [Google Scholar] [CrossRef]
- Helmert, U.; Streich, W.; Borgers, D. Regional Differences in Trends in Life Expectancy and the Influence of the Political and Socioeconomic Contexts in Germany. Int. J. Health Serv. 2003, 33, 669–686. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Hoebel, J.; Kroll, L.E. Social differences in mortality and life expectancy in Germany. Current situation and trends. J. Health Monit. 2019, 4, 3–13. [Google Scholar] [CrossRef]
- Federal Ministry for Economic Affairs and Energy. Creating Equivalent Living Conditions in Eastern and Western Germany. Available online: https://www.bmwi.de/Redaktion/EN/Dossier/neue-laender.html (accessed on 13 November 2021).
- Razum, O.; Sauzet, O. Equality in Living Conditions as a Prerequisite for Health Equity. Dtsch. Arztebl. Int. 2020, 117, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Federal Ministry of Justice and Consumer Protection. Basic Law for the Federal Republic of Germany, Article 72 [Concurrent Legislative Powers]. Available online: https://www.gesetze-im-internet.de/englisch_gg/englisch_gg.html#p0326 (accessed on 13 November 2021).
- Bundesministerium der Justiz und für Verbraucherschutz. [Social Code (SGB) Book Five (V)—Statutory Health Insurance—§ 70 Quality, Humanity and Economic Efficiency.] Sozialgesetzbuch (SGB) Fünftes Buch (V)—Gesetzliche Krankenversicherung—§ 70 Qualität, Humanität und Wirtschaftlichkeit. Available online: https://www.gesetze-im-internet.de/sgb_5/__70.html (accessed on 10 December 2021).
- Pickett, K.E.; Wilkinson, R.G. Income inequality and health: A causal review. Soc. Sci. Med. 2015, 128, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Kroll, L.E.; Müters, S.; Lampert, T. [Unemployment and Health. An overview of current research results and data from the 2010 and 2012 German Health Update.] Arbeitslosigkeit und ihre Auswirkungen auf die Gesundheit. Bundesgesundheitsbl 2015, 59, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Kroll, L. [Income Differences in Health and Life Expectancy—Cross-Sectional and Longitudinal Findings of the German Socio-Economic Panel (GSOEP).] Einkommensdifferenzen in der Gesundheit und Lebenserwartung—Quer- und Längsschnittbefunde des Sozio-oekonomischen Panels (SOEP). Gesundheitswesen 2006, 68, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Kroll, L.E.; Kuntz, B.; Hoebel, J. [Health inequalities in Germany and in international comparison: Developments and trends over time.] Gesundheitliche Ungleichheit in Deutschland und im internationalen Vergleich: Zeitliche Entwicklungen und Trends. J. Health Monit. 2018, 3, 2–25. [Google Scholar] [CrossRef]
- Lantz, P.M.; House, J.S.; Lepkowski, J.M.; Williams, D.R.; Mero, R.P.; Chen, J. Socioeconomic factors, health behaviors, and mortality: Results from a nationally representative prospective study of US adults. JAMA 1998, 279, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Le Hoi, V.; Phuc, H.D.; Dung, T.V.; Chuc, N.T.K.; Lindholm, L. Remaining life expectancy among older people in a rural area of Vietnam: Trends and socioeconomic inequalities during a period of multiple transitions. BMC Public Health 2009, 9, 471. [Google Scholar] [CrossRef]
- Moreno, X.; Lera, L.; Moreno, F.; Albala, C. Socioeconomic inequalities in life expectancy and disability-free life expectancy among Chilean older adults: Evidence from a longitudinal study. BMC Geriatr. 2021, 21, 176. [Google Scholar] [CrossRef]
- Babones, S.J. Income inequality and population health: Correlation and causality. Soc. Sci. Med. 2008, 66, 1614–1626. [Google Scholar] [CrossRef] [PubMed]
- Khang, Y.-H.; Bahk, J.; Lim, D.; Kang, H.-Y.; Lim, H.-K.; Kim, Y.-Y.; Park, J.H. Trends in inequality in life expectancy at birth between 2004 and 2017 and projections for 2030 in Korea: Multiyear cross-sectional differences by income from national health insurance data. BMJ Open 2019, 9, e030683. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.G.; Pickett, K. The Spirit Level: Why Equality Is Better for Everyone; Penguin Books: London, UK, 2010; ISBN 0141032367. [Google Scholar]
- Fors, S.; Wastesson, J.W.; Morin, L. Growing Income-Based Inequalities in Old-Age Life Expectancy in Sweden, 2006–2015. Demography 2021, 58, 2117–2138. [Google Scholar] [CrossRef]
- Lampert, T.; Hoebel, J.; Eric Kroll, L.; Luy, M. [Social differences in life expectancy.] Soziale Unterschiede in der Lebenserwartung. Public Health Forum 2018, 26, 325–327. [Google Scholar] [CrossRef]
- Matthews, R.J.; Jagger, C.; Hancock, R.M. Does Socio-economic Advantage Lead to a Longer, Healthier Old Age? Soc. Sci. Med. 2006, 62, 2489–2499. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, G. Socio-ecological Perspective of Older Age Life Expectancy: Income, Gender Inequality, and Financial Crisis in Europe. Glob. Health 2017, 13, 58. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.; Ko, W.; Muhwava, W.; Choi, Y.; Kim, H.; Park, Y.S.; Jambere, G.B.; Cho, Y. Mind the Gaps: Age and Cause Specific Mortality and Life Expectancy in the Older Population of South Korea and Japan. BMC Public Health 2020, 20, 819. [Google Scholar] [CrossRef]
- Federal Institute for Research on Building, Urban Affairs and Spatial Development. The Federal Institute for Research on Building, Urban Affairs and Spatial Development. Available online: https://www.bbsr.bund.de/BBSR/EN/home/_node.html (accessed on 15 November 2021).
- Federal Office for Building and Regional Planning. The Federal Office for Building and Regional Planning. Available online: https://www.bbr.bund.de/BBR/EN/Home/_node.html (accessed on 15 November 2021).
- Bundesinstitut für Bau-, Stadt- und Raumordnung. [INKAR: Indicators and Maps for Spatial and Urban Development]. INKAR: Indikatoren und Karten zur Raum- und Stadtentwicklung. Available online: https://www.inkar.de/ (accessed on 25 November 2021).
- Federal Institute for Research on Building, Urban Affairs and Spatial Development. [Indicators, Spatial and Temporal References (PDF File): INKAR 2019—Indicator Overview]. Indikatoren, Raum- und Zeitbezüge (PDF File): INKAR 2019—Indikatorenübersicht. Available online: https://www.inkar.de/ (accessed on 15 November 2021).
- Statistische Ämter des Bundes und der Länder. [Regional Database Germany]. Regionaldatenbank Deutschland. Available online: https://www.regionalstatistik.de/genesis/online/logon (accessed on 5 December 2021).
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; Sage: London, UK, 2015. [Google Scholar]
- Columbia University, Mailman School of Public Health. Population Health Methods: Geographically Weighted Regression. Available online: https://www.publichealth.columbia.edu/research/population-health-methods/geographically-weighted-regression (accessed on 20 January 2022).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Taylor and Francis: Hoboken, NJ, USA, 2013; ISBN 9780805802832. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Statistische Ämter des Bundes und der Länder. [Regional Atlas of Germany, Theme Area “Health Care and Social Services,” Indicators for “Nursing and Personnel”.] Regionalatlas Deutschland, Themenbereich “Gesundheits- und Sozialwesen”, Indikatoren zu “Pflege und Personal”. Available online: https://www.regionalstatistik.de/genesis//online?operation=table&code=AI014-2&bypass=true&levelindex=0&levelid=1638719323111 (accessed on 5 December 2021).
- Artiga, S.; Hinton, E. Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity. Available online: https://collections.nlm.nih.gov/catalog/nlm:nlmuid-101740257-pdf (accessed on 22 December 2021).
- Moss, N.E. Gender equity and socioeconomic inequality: A framework for the patterning of women’s health. Soc. Sci. Med. 2002, 54, 649–661. [Google Scholar] [CrossRef]
- Maier, W.; Fairburn, J.; Mielck, A. [Regional Deprivation and Mortality in Bavaria. Development of a Community-Based Index of Multiple Deprivation]. Regionale Deprivation und Mortalität in Bayern. Entwicklung eines ‘Index Multipler Deprivation’ auf Gemeindeebene. Gesundheitswesen 2012, 74, 416–425. [Google Scholar] [CrossRef]
- Maier, W.; Schwettmann, L. [Area deprivation in Germany: The ‘German Index of Multiple Deprivation (GIMD)’]. Regionale Deprivation in Deutschland: Der‚ German Index of Multiple Deprivation (GIMD)‘. Public Health Forum 2018, 26, 376–379. [Google Scholar] [CrossRef]
- Hofmeister, C.; Maier, W.; Mielck, A.; Stahl, L.; Breckenkamp, J.; Razum, O. [Regional Deprivation in Germany: Nation-wide Analysis of its Association with Mortality Using the German Index of Multiple Deprivation (GIMD)]. Regionale Deprivation in Deutschland: Bundesweite Analyse des Zusammenhangs mit Mortalität unter Verwendung des ‘German Index of Multiple Deprivation (GIMD)’. Gesundheitswesen 2016, 78, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Kroll, L.E.; Schumann, M.; Hoebel, J.; Lampert, T. [Regional Differences in Health—Development of a Socioeconomic Deprivation Index for Germany]. Regionale Unterschiede in der Gesundheit—Entwicklung Eines Sozioökonomischen Deprivationsindex für Deutschland, 2017. Available online: https://edoc.rki.de/handle/176904/2648.2 (accessed on 15 December 2021).
- Blakely, T.A.; Kennedy, B.P.; Kawachi, I. Socioeconomic inequality in voting participation and self-rated health. Am. J. Public Health 2001, 91, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Couture, J.; Breux, S. The differentiated effects of health on political participation. Eur. J. Public Health 2017, 27, 599–604. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Denny, K.; Doyle, O. Analysing the relationship between voter turnout and health in Ireland. Ir. Med. J. 2007, 100, 56–58. [Google Scholar]
- Denny, K.J.; Doyle, O.M. “… Take up thy bed, and vote.” Measuring the relationship between voting behaviour and indicators of health. Eur. J. Public Health 2007, 17, 400–401. [Google Scholar] [CrossRef]
- Islam, M.K.; Merlo, J.; Kawachi, I.; Lindström, M.; Burström, K.; Gerdtham, U.-G. Does it really matter where you live? A panel data multilevel analysis of Swedish municipality-level social capital on individual health-related quality of life. Health Econ. Policy Law 2006, 1, 209–235. [Google Scholar] [CrossRef]
- Kim, D.; Kawachi, I. A multilevel analysis of key forms of community- and individual-level social capital as predictors of self-rated health in the United States. J. Urban Health 2006, 83, 813–826. [Google Scholar] [CrossRef]
- Murayama, H.; Fujiwara, Y.; Kawachi, I. Social Capital and Health: A Review of Prospective Multilevel Studies. J. Epidemiol. 2012, 22, 179–187. [Google Scholar] [CrossRef]
- Macinko, J.; Starfield, B. The utility of social capital in research on health determinants. Milbank Q. 2001, 79, 387–427. [Google Scholar] [CrossRef]
- Nowatzki, N.R. Income Inequality and Health: A Theoretical Quagmire. In Redistributing Health: New Directions in Population Health Research in Canada, 2nd ed.; McIntosh, T., Jeffery, B., Muhajarine, N., Eds.; University of Regina Press: Regina, SK, Canada, 2010; pp. 35–52. [Google Scholar]
- Atkinson, M.D.; Fowler, A. Social Capital and Voter Turnout: Evidence from Saint’s Day Fiestas in Mexico. Br. J. Political Sci. 2014, 44, 41–59. [Google Scholar] [CrossRef]
- Luy, M. Causes of Male Excess Mortality: Insights from Cloistered Populations. Popul. Dev. Rev. 2003, 29, 647–676. [Google Scholar] [CrossRef]
- Luy, M.; Gast, K. Do women live longer or do men die earlier? Reflections on the causes of sex differences in life expectancy. Gerontology 2014, 60, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Kolip, P.; Lange, C. Gender inequality and the gender gap in life expectancy in the European Union. Eur. J. Public Health 2018, 28, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Hossin, M.Z. The male disadvantage in life expectancy: Can we close the gender gap? Int. Health 2021, 13, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M. Social Determinants of Health and Related Inequalities: Confusion and Implications. Front. Public Health 2019, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Balfour, R.; Bell, R.; Marmot, M. Social determinants of mental health. Int. Rev. Psychiatry 2014, 26, 392–407. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Kennedy, B.P. Health and social cohesion: Why care about income inequality? BMJ 1997, 314, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I.; Kennedy, B.P. Income inequality and health: Pathways and mechanisms. Health Serv. Res. 1999, 34, 215–227. [Google Scholar]
- Haan, P.; Stichnoth, H.; Blömer, M.; Buslei, H.; Geyer, J.; Krolage, C.; Müller, K.-U. [Development of Old-Age Poverty until 2036. Trends, Risk Groups and Policy Scenarios]. Entwicklung der Altersarmut bis 2036: Trends, Risikogruppen und Politikszenarien. Available online: https://www.bertelsmann-stiftung.de/de/publikationen/publikation/did/entwicklung-der-altersarmut-bis-2036/ (accessed on 5 December 2021).
- OECD. Pensions at a Glance 2019; OECD: Paris, France, 2019; ISBN 9789264787919. [Google Scholar]
- Luy, M.; Caselli, G. The Impact of a Migration-Caused Selection Effect on Regional Mortality Differences in Italy and Germany; Rostock Center for the Study of Demographic Change: Rostock, Germany, 2008. [Google Scholar]
- Luy, M.; Zannella, M.; Wegner-Siegmundt, C.; Minagawa, Y.; Lutz, W.; Caselli, G. The impact of increasing education levels on rising life expectancy: A decomposition analysis for Italy, Denmark, and the USA. Genus 2019, 75, 11. [Google Scholar] [CrossRef]
- Shkolnikov, V.M.; Andreev, E.M.; Jasilionis, D.; Leinsalu, M.; Antonova, O.I.; Mckee, M. The changing relation between education and life expectancy in central and eastern Europe in the 1990s. J. Epidemiol. Community Health 2006, 60, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.P.; Leon, J.; Smith Greenaway, E.G.; Collins, J.; Movit, M. The education effect on population health: A reassessment. Popul. Dev. Rev. 2011, 37, 307–332. [Google Scholar] [CrossRef] [PubMed]
- Montez, J.K.; Hummer, R.A.; Hayward, M.D. Educational attainment and adult mortality in the United States: A systematic analysis of functional form. Demography 2012, 49, 315–336. [Google Scholar] [CrossRef] [PubMed]
- Montez, J.K.; Brooks, J.D. Educational attainment and adult health. In Handbook of Aging and the Social Sciences, 9th ed.; Ferraro, K.F., Carr, D., Freedman, V.A., Idler, E.L., Eds.; Academic Press An Imprint of Elsevier: London, UK; San Diego, CA, USA; Cambridge, MA, USA; Oxford, UK, 2021; pp. 83–98. ISBN 9780128159705. [Google Scholar]
- Welsh, J.; Bishop, K.; Booth, H.; Butler, D.; Gourley, M.; Law, H.D.; Banks, E.; Canudas-Romo, V.; Korda, R.J. Inequalities in life expectancy in Australia according to education level: A whole-of-population record linkage study. Int. J. Equity Health 2021, 20, 178. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Lee, H. Marked Disparities in Life Expectancy by Education, Poverty Level, Occupation, and Housing Tenure in the United States, 1997–2014. Int. J. Matern. Child Health 2021, 10, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Woolf, S.H.; Johnson, R.E.; Phillips, R.L.; Philipsen, M. Giving everyone the health of the educated: An examination of whether social change would save more lives than medical advances. Am. J. Public Health 2007, 97, 679–683. [Google Scholar] [CrossRef] [PubMed]
- Shkolnikov, V.M.; Andreev, E.M.; Jdanov, D.A.; Jasilionis, D.; Kravdal, Ø.; Vågerö, D.; Valkonen, T. Increasing Absolute Mortality Disparities by Education in Finland, Norway and Sweden, 1971–2000. J. Epidemiol. Community Health 2012, 66, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.M.; Spittel, M.L.; Zeno, T.L. Educational Attainment and Life Expectancy. Policy Insights Behav. Brain Sci. 2014, 1, 189–194. [Google Scholar] [CrossRef]
- Solé-Auró, A.; Martín, U.; Domínguez Rodríguez, A. Educational Inequalities in Life and Healthy Life Expectancies among the 50-Plus in Spain. Int. J. Environ. Res. Public Health 2020, 17, 3558. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Indicator No. | Indicator Name | Definition [61,67] | Mean | SD | Range |
|---|---|---|---|---|---|
| (1) | Primary-care physicians per 100,000 inhabitants | Primary-care physicians (in German: “Hausärzte”) per 100,000 inhabitants | 61.36 | 26.11 | 8.4–164.9 |
| (2) | Hospital beds per 1000 inhabitants | Hospital beds per 1000 inhabitants | 6.35 | 3.89 | 0.00–29.59 |
| (3) | Care personnel per 100 persons in need of outpatient care services | Care personnel per 100 persons in need of outpatient care services | 46.31 | 12.56 | 24.6–156.2 |
| (4) | Care personnel per 100 persons in need of full inpatient care | Care personnel in nursing homes per 100 persons in need of full inpatient care | 93.82 | 11.96 | 68.1–132.4 |
| (5) | GDP (gross domestic product) per capita | GDP in 1000€ per inhabitant | 37.09 | 16.05 | 16.4–172.4 |
| (6) | Household income | Average disposable household income (in €) per inhabitant per month | 1872.56 | 215.76 | 1365–3242 |
| (7) | Proportion of employees without vocational qualification | Employees (subject to social security contributions) at place of residence without vocational qualification per 100 employees (subject to social security contributions) at place of residence | 6.93 | 1.80 | 2.9–12.2 |
| (8) | Proportion of employees with academic degree | Employees (subject to social insurance contributions) at place of residence with academic degree per 100 employees (subject to social security contributions) at place of residence | 7.76 | 3.45 | 2.9–23.0 |
| (9) | Unemployment | Unemployed or job-seeking persons per 1000 inhabitants at working age | 44.24 | 19.22 | 12.2–106.3 |
| (10) | Proportion of people with Hartz-IV support | Employable and non-employable persons entitled to German Social Code II-based welfare benefits (“Hartz-IV support”) per 100 inhabitants < 65 years | 8.13 | 4.46 | 1.5–24.9 |
| (11) | Proportion of elder with financial elder support | Persons > 64 years receiving basic income support per 1000 inhabitants > 64 years | 22.37 | 14.63 | 3.0–82.1 |
| (12) | Voter turnout | Voter turnout (in %) in the 2017 federal elections | 75.08 | 3.79 | 63.1–84.1 |
| Indicator/Predictor Name | ß (Standardized Regression Coefficient) | p Value of ß |
|---|---|---|
| Primary-care physicians per 100,000 inhabitants | −0.07 | 0.168 |
| Hospital beds per 1000 inhabitants | −0.15 | 0.004 |
| Care personnel per 100 persons in need of outpatient care services | 0.14 | 0.005 |
| Care personnel per 100 persons in need of full inpatient care | 0.22 | <0.001 |
| GDP (gross domestic product) per capita | 0.15 | 0.003 |
| Household income | 0.63 | <0.001 |
| Proportion of employees without vocational qualification | 0.12 | 0.013 |
| Proportion of employees with academic degree | 0.41 | <0.001 |
| Unemployment | −0.60 | <0.001 |
| Proportion of people with Hartz-IV support | −0.56 | <0.001 |
| Proportion of elder with financial elder support | −0.10 | 0.045 |
| Voter turnout | 0.67 | <0.001 |
| Indicator/Predictor | ß (Standardized Regression Coefficient) | p Value of ß |
|---|---|---|
| Primary-care physicians per 100,000 inhabitants | −0.01 | 0.913 |
| Hospital beds per 1000 inhabitants | −0.10 | 0.055 |
| Care personnel per 100 persons in need of outpatient care services | 0.14 | 0.005 |
| Care personnel per 100 persons in need of full inpatient care | −0.00 | 0.981 |
| GDP (gross domestic product) per capita | 0.12 | 0.022 |
| Household income | 0.35 | <0.001 |
| Proportion of employees without vocational qualification | −0.14 | 0.006 |
| Proportion of employees with academic degree | 0.40 | <0.001 |
| Unemployment | −0.37 | <0.001 |
| Proportion of people with Hartz-IV support | −0.35 | <0.001 |
| Proportion of elder with financial elder support | −0.19 | <0.001 |
| Voter turnout | 0.38 | <0.001 |
| Indicator/Predictor | ß (Standardized Regression Coefficient) | p Value of ß |
|---|---|---|
| Primary-care physicians per 100,000 inhabitants | - | n.s. |
| Hospital beds per 1000 inhabitants | - | n.s. |
| Care personnel per 100 persons in need of outpatient care services | - | n.s. |
| Care personnel per 100 persons in need of full inpatient care | 0.16 | <0.001 |
| GDP (gross domestic product) per capita | −0.13 | 0.005 |
| Household income | 0.27 | <0.001 |
| Proportion of employees without vocational qualification | - | n.s. |
| Proportion of employees with academic degree | 0.42 | <0.001 |
| Unemployment | −0.23 | <0.001 |
| Proportion of elder with financial elder support | −0.09 | 0.050 |
| Voter turnout | 0.15 | 0.014 |
| Indicator/Predictor | ß (Standardized Regression Coefficient) | p Value of ß |
|---|---|---|
| Primary-care physicians per 100,000 inhabitants | - | n.s. |
| Hospital beds per 1000 inhabitants | - | n.s. |
| Care personnel per 100 persons in need of outpatient care services | - | n.s. |
| Care personnel per 100 persons in need of full inpatient care | - | n.s. |
| GDP (gross domestic product) per capita | - | n.s. |
| Household income | - | n.s. |
| Proportion of employees without vocational qualification | - | n.s. |
| Proportion of employees with academic degree | 0.51 | <0.001 |
| Unemployment | −0.23 | <0.001 |
| Proportion of elder with financial elder support | −0.30 | <0.001 |
| Voter turnout | - | n.s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siegel, A.; Schug, J.F.; Rieger, M.A. Social Determinants of Remaining Life Expectancy at Age 60: A District-Level Analysis in Germany. Int. J. Environ. Res. Public Health 2022, 19, 1530. https://doi.org/10.3390/ijerph19031530
Siegel A, Schug JF, Rieger MA. Social Determinants of Remaining Life Expectancy at Age 60: A District-Level Analysis in Germany. International Journal of Environmental Research and Public Health. 2022; 19(3):1530. https://doi.org/10.3390/ijerph19031530
Chicago/Turabian StyleSiegel, Achim, Jonas F. Schug, and Monika A. Rieger. 2022. "Social Determinants of Remaining Life Expectancy at Age 60: A District-Level Analysis in Germany" International Journal of Environmental Research and Public Health 19, no. 3: 1530. https://doi.org/10.3390/ijerph19031530
APA StyleSiegel, A., Schug, J. F., & Rieger, M. A. (2022). Social Determinants of Remaining Life Expectancy at Age 60: A District-Level Analysis in Germany. International Journal of Environmental Research and Public Health, 19(3), 1530. https://doi.org/10.3390/ijerph19031530