
Gender and Social Inequalities in Awareness of Coronary Artery Disease in European Countries

 , ,
, ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Participant Characteristics
3.2. Awareness of Heart Disease
3.3. Warning Signs of a Heart Attack and Calls to Emergency Services
3.4. Perceived Risk Factors and Heart Disease Prevention Strategies
3.5. At-Risk Individuals and Medical History
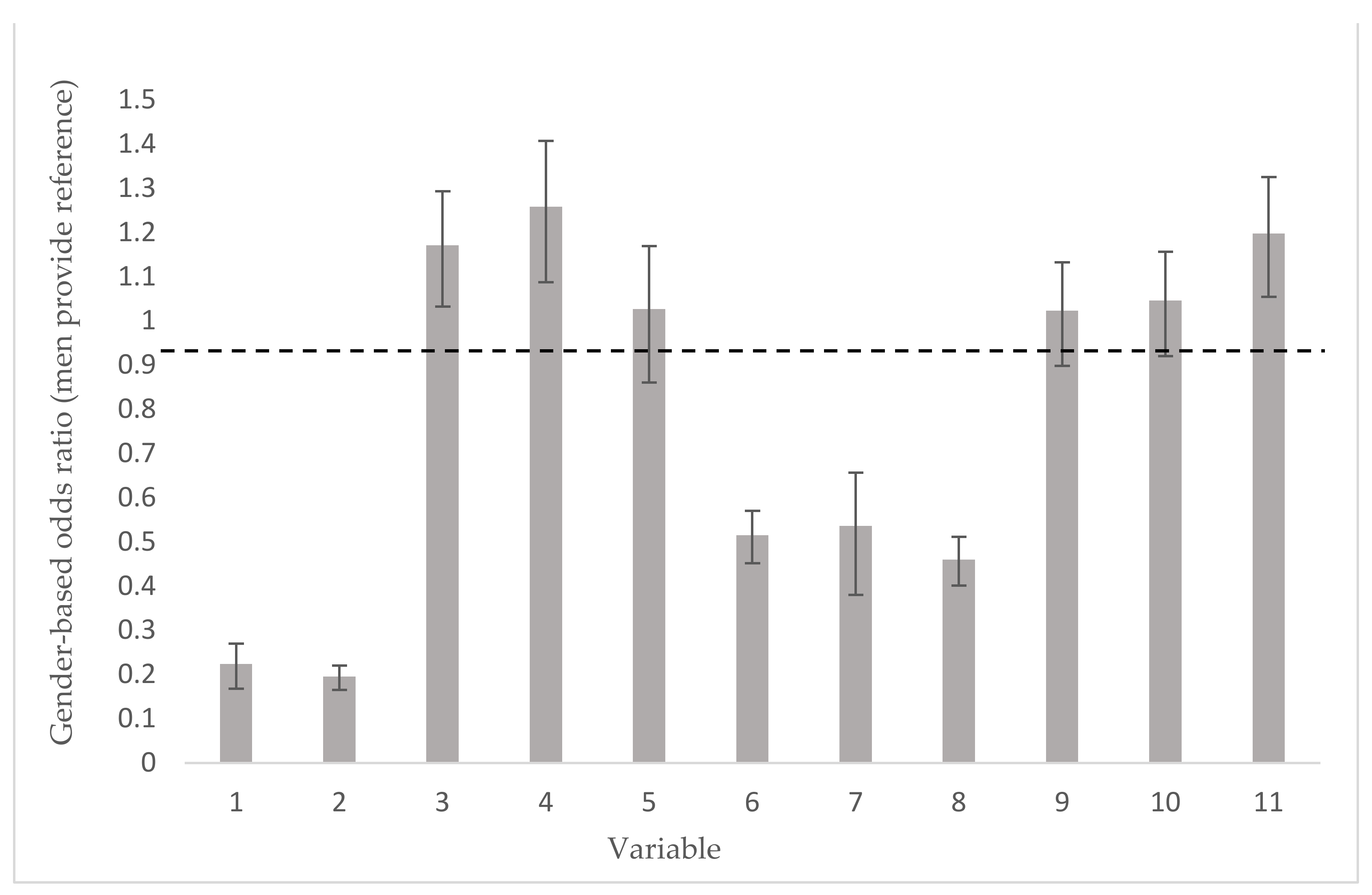
3.6. Key Awareness Indicators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- Eurostat Cardiovascular Diseases Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Cardiovascular_diseases_statistics (accessed on 11 October 2021).
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable risk factors, cardiovascular disease, and mortality in 155,722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2019, 395, 795–808. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. NICE Impact: Cardiovascular Disease Prevention. Available online: https://www.nice.org.uk/media/default/about/what-we-do/into-practice/measuring-uptake/nice-impact-cardiovascular-disease-prevention.pdf (accessed on 10 September 2021).
- Oertelt-Prigione, S.; Seeland, U.; Kendel, F.; Rücke, M.; Flöel, A.; Gaissmaier, W.; Heim, C.; Schnabel, R.; Stangl, V.; Regitz-Zagrosek, V. Cardiovascular risk factor distribution and subjective risk estimation in urban women—The BEFRI Study: A randomized cross-sectional study. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.; Heeley, E.; Chalmers, J.; Chow, C.K. Inaccurate risk perceptions contribute to treatment gaps in secondary prevention of cardiovascular disease. Intern. Med. J. 2015, 46, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, F.D.; Chen, Y.; Di Santo, P.; Simard, T.; Motazedian, P.; Hibbert, B. Association Between Self-Reported Potentially Modifiable Cardiac Risk Factors and Perceived Need to Improve Physical Health: A Population-Based Study. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef]
- Nehme, Z.; Andrew, E.; Bernard, S.; Patsamanis, H.; Cameron, P.; Bray, J.; Meredith, I.T.; Smith, K. Impact of a public awareness campaign on out-of-hospital cardiac arrest incidence and mortality rates. Eur. Heart J. 2016, 38, 1666–1673. [Google Scholar] [CrossRef]
- Mosca, L.; Mochari, H.; Christian, A.; Berra, K.; Taubert, K.; Mills, T.; Burdick, K.A.; Simpson, S.L. National Study of Women’s Awareness, Preventive Action, and Barriers to Cardiovascular Health. Circulation 2006, 113, 525–534. [Google Scholar] [CrossRef]
- Mosca, L.; Hammond, G.; Greenberger, H.M.; Towfighi, A.; Albert, M.A. Fifteen-Year Trends in Awareness of Heart Disease in Women. Circulation 2013, 127, 1254–1263. [Google Scholar] [CrossRef]
- Naylor-Wardle, J.; Rowland, B.; Kunadian, V. Socioeconomic status and cardiovascular health in the COVID-19 pandemic. Heart 2021, 107, 358–365. [Google Scholar] [CrossRef]
- Münzel, T.; Miller, M.R.; Sørensen, M.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Reduction of environmental pollutants for prevention of cardiovascular disease: It’s time to act. Eur. Heart J. 2020, 41, 3989–3997. [Google Scholar] [CrossRef]
- EUGenMed, T.; Cardiovascular Clinical Study Group; Regitz-Zagrosek, V.; Oertelt-Prigione, S.; Prescott, E.; Franconi, F.; Gerdts, E.; Foryst-Ludwig, A.; Maas, A.H.; Kautzky-Willer, A.; et al. Gender in cardiovascular diseases: Impact on clinical manifestations, management, and outcomes. Eur. Heart J. 2015, 37, 24–34. [Google Scholar] [CrossRef]
- McDonnell, L.A.; Pipe, A.L.; Westcott, C.; Perron, S.; Younger-Lewis, D.; Elias, N.; Nooyen, J.; Reid, R.D. Perceived vs Actual Knowledge and Risk of Heart Disease in Women: Findings From a Canadian Survey on Heart Health Awareness, Attitudes, and Lifestyle. Can. J. Cardiol. 2014, 30, 827–834. [Google Scholar] [CrossRef]
- Bolívar Muñoz, J.; Martínez Cassinello, R.; Mateo Rodríguez, I.; Torres Ruiz, J.M.; Pascual Martínez, N.; Rosell-Ortiz, F.; Reina Toral, A.; Martín Castro, C.; Daponte Codina, A. Actuación de los pacientes ante un síndrome coronario agudo: Diferencias desde una perspectiva de género. Emergencias 2013, 25, 23–30. [Google Scholar]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardio-vascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Erhardt, L.; Hobbs, F.D.R. Public perceptions of cardiovascular risk in five European countries: The react survey. Int. J. Clin. Pr. 2002, 56, 638–644. [Google Scholar]
- Cushman, M.; Shay, C.M.; Howard, V.J.; Jiménez, M.C.; Lewey, J.; McSweeney, J.C.; Newby, L.K.; Poudel, R.; Reynolds, H.R.; Rexrode, K.M.; et al. Ten-Year Differences in Women’s Awareness Related to Coronary Heart Disease: Results of the 2019 American Heart Association National Survey: A Special Report From the American Heart Association. Circulation 2021, 143, e239–e248. [Google Scholar] [CrossRef]
- Mata, J.; Frank, R.; Gigerenzer, G. Symptom recognition of heart attack and stroke in nine European countries: A representative survey. Health Expect. 2012, 17, 376–387. [Google Scholar] [CrossRef]
- Mahajan, S.; Valero-Elizondo, J.; Khera, R.; Desai, N.R.; Blankstein, R.; Blaha, M.J.; Virani, S.S.; Kash, B.A.; Zoghbi, W.A.; Krumholz, H.M.; et al. Variation and Disparities in Awareness of Myocardial Infarction Symptoms Among Adults in the United States. JAMA Netw. Open 2019, 2, e1917885. [Google Scholar] [CrossRef]
- Intas, G.; Tsolakoglou, J.; Stergiannis, P.; Chalari, E.; Fildissis, G. Do Greek citizens have minimum knowledge about heart attack ? A survey. Health Sci. J. 2015, 9, 1–7. [Google Scholar]
- Park, K.S. Factors affecting awareness of myocardial infarction symptoms among the general public. Epidemiology Health 2020, 42, e2020032. [Google Scholar] [CrossRef]
- Birnbach, B.; Höpner, J.; Mikolajczyk, R. Cardiac symptom attribution and knowledge of the symptoms of acute myocardial infarction: A systematic review. BMC Cardiovasc. Disord. 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, S.; Baldwin, T.; Tahir, M.; Choudhry, O.; Senior, A.; Greenfield, S. Public knowledge of the symptoms of myocardial infarction: A street survey in Birmingham, England. Fam. Pract. 2011, 29, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Merz, C.N.B.; Shaw, L.J.; Reis, S.; Bittner, V.; Kelsey, S.F.; Olson, M.; Johnson, B.D.; Pepine, C.J.; Mankad, S.; Sharaf, B.L.; et al. Insights From the NHLBI-Sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study: Part II: Gender Differences in Presentation, Diagnosis, and Outcome With Regard to Gender-Based Pathophysiology of Atherosclerosis and Macrovascular and Microvascular Coronary Disease. J. Am. Coll. Cardiol. 2006, 47, S21–S29. [Google Scholar] [CrossRef]
- Van Oosterhout, R.E.M.; De Boer, A.R.; Maas, A.H.E.M.; Rutten, F.H.; Bots, M.L.; Peters, S.A.E. Sex Differences in Symptom Presentation in Acute Coronary Syndromes: A Systematic Review and Meta-analysis. J. Am. Heart Assoc. 2020, 9, e014733. [Google Scholar] [CrossRef]
- Fang, J.; Luncheon, C.; Ayala, C.; Odom, E.; Loustalot, F. Awareness of heart attack symptoms and response among adults—United States, 2008, 2014, and 2017. Morb. Mortal. Wkly. Rep. 2019, 68, 101. [Google Scholar] [CrossRef]
- Kopeć, G.; Sobien, B.; Podolec, M.; Dziedzic, H.; Zarzecka, J.; Loster, B.; Pajak, A.; Podolec, P. Knowledge of a patient-dependant phase of acute myocardial infarction in Polish adults: The role of physician’s advice. Eur. J. Public Health 2010, 21, 603–608. [Google Scholar] [CrossRef][Green Version]
- Albarqouni, L.; Smenes, K.; Meinertz, T.; Schunkert, H.; Fang, X.; Ronel, J.; Ladwig, K.-H. Patients’ knowledge about symptoms and adequate behaviour during acute myocardial infarction and its impact on delay time. Patient Educ. Couns. 2016, 99, 1845–1851. [Google Scholar] [CrossRef]
- Garrido, D.; Petrova, D.; Catena, A.; Ramírez-Hernández, J.A.; Garcia-Retamero, R. Recognizing a Heart Attack: Patients’ Knowledge of Cardiovascular Risk Factors and Its Relation to Prehospital Decision Delay in Acute Coronary Syndrome. Front. Psychol. 2020, 11, 2056. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Young, L. Social Determinants of Myocardial Infarction Risk and Survival: A Systematic Review. Eur. J. Cardiovasc. Res. 2020, 2020, 1–12. [Google Scholar] [CrossRef]
- Keller, A.; Litzelman, K.; Wisk, L.E.; Maddox, T.; Cheng, E.R.; Creswell, P.D.; Witt, W.P. Does the perception that stress affects health matter? The association with health and mortality. Health Psychol. 2012, 31, 677–684. [Google Scholar] [CrossRef]
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Kim, H.-S.; Lee, H.; Kim, K.; Park, H.-K.; Park, K.-S.; Kang, G.W.; Shin, H.-Y.; Kim, R.B.; Oh, G.-J.; Seo, J.H.; et al. The General Public’s Awareness of Early Symptoms of and Emergency Responses to Acute Myocardial Infarction and Related Factors in South Korea: A National Public Telephone Survey. J. Epidemiology 2016, 26, 233–241. [Google Scholar] [CrossRef]
- Cainzos-Achirica, M.; Blaha, M.J. Cardiovascular risk perception in women: True unawareness or risk miscalculation? BMC Med. 2015, 13, 1–4. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Gawlinski, A. Rationale and design of the Cardiac Hospitalization Atherosclerosis Management Program at the University of California Los Angeles. Am. J. Cardiol. 2000, 85, 10–17. [Google Scholar] [CrossRef]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Smith, G.D.; Himmelfarb, C.D.; Lauer, M.S.; Lockwood, D.W.; et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef]
- Vogel, B.; Acevedo, M.; Appelman, Y.; Merz, C.N.B.; Chieffo, A.; A Figtree, G.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.H.E.M.; et al. The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Lichtman, J.H.; Leifheit-Limson, E.C.; Watanabe, E.; Allen, N.B.; Garavalia, B.; Garavalia, L.S.; Spertus, J.A.; Krumholz, H.M.; Curry, L.A. Symptom Recognition and Healthcare Experiences of Young Women With Acute Myocardial Infarction. Circ. Cardiovasc. Qual. Outcomes 2015, 8, S31–S38. [Google Scholar] [CrossRef]
- Leifheit-Limson, E.C.; D’Onofrio, G.; Daneshvar, M.; Geda, M.; Bueno, H.; Spertus, J.A.; Krumholz, H.M.; Lichtman, J.H. Sex Differences in Cardiac Risk Factors, Perceived Risk, and Health Care Provider Discussion of Risk and Risk Modification Among Young Patients With Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2015, 66, 1949–1957. [Google Scholar] [CrossRef]
- Long, T.; Taubenheim, A.M.; Wayman, J.; Temple, S.; Ruoff, B.A. The Heart Truth: Using the Power of Branding and Social Marketing to Increase Awareness of Heart Disease in Women. Soc. Mark. Q. 2008, 14, 3–29. [Google Scholar] [CrossRef]
- Kouvari, M.; Souliotis, K.; Yannakoulia, M.; Panagiotakos, D.B. Cardiovascular Diseases in Women: Policies and Practices around the Globe to Achieve Gender Equity in Cardiac Health. Risk Manag. Healthc Policy. 2020, 13, 2079–2094. [Google Scholar] [CrossRef]
- Salmi, L.-R.; Barsanti, S.; Bourgueil, Y.; Daponte, A.; Piznal, E.; Ménival, S.; Leleu, H.; Jusot, F.; Saton, M.-O.; Kovacs, Z.; et al. Interventions addressing health inequalities in European regions: The AIR project. Health Promot. Int. 2015, 32, 430–441. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Male | Female | Overall | ||||
|---|---|---|---|---|---|---|
| Characteristic | N | % | N | % | N | % |
| Gender | 1252 | 47.8 | 1357 | 52.2 | 2609 | 100 |
| Age | ||||||
| 25–44 years | 425 | 34.0 | 469 | 34.6 | 895 | 34.3 |
| 45–64 years | 514 | 41.0 * | 513 | 37.8 * | 1027 | 39.4 |
| 65 and over | 313 | 25.0 * | 374 | 27.6 * | 687 | 26.3 |
| Missing | 0 | 0 | 0 | |||
| Health status | ||||||
| Very good | 261 | 20.8 | 280 | 20.6 | 541 | 20.7 |
| Good | 637 | 50.9 | 686 | 50.5 | 1323 | 50.7 |
| Fair | 272 | 21.8 * | 325 | 23.9 * | 597 | 22.9 |
| Bad | 65 | 5.2 * | 52 | 3.8 * | 117 | 4.5 |
| Very bad | 17 | 1.3 | 14 | 1.0 | 31 | 1.2 |
| Missing | 0 | 0 | 0 | |||
| Marital status | ||||||
| Single | 252 | 20.2 | 170 | 12.6 | 422 | 16.2 |
| Married/living together | 860 | 69.1 * | 894 | 66.1 * | 1754 | 67.5 |
| Divorced/separated | 70 | 5.6 ** | 132 | 9.8 ** | 203 | 7.8 |
| Widow | 63 | 5.1 ** | 157 | 11.6 ** | 220 | 8.5 |
| Missing | 0 | 0 | 0 | |||
| Education | ||||||
| Compulsory or less | 725 | 58.8 ** | 860 | 64.5 ** | 1584 | 61.7 |
| Higher education | 509 | 41.2 ** | 473 | 35.5 ** | 982 | 38.3 |
| Missing | 19 | 1.4 | 24 | 1.7 | 43 | 1.6 |
| Relative socioeconomic status | ||||||
| High | 521 | 45.9 ** | 435 | 36.6 ** | 956 | 41.1 |
| Low | 614 | 54.1 ** | 752 | 63.4 ** | 1366 | 58.9 |
| Missing | 117 | 9.3 | 170 | 12.5 | 287 | 11.0 |
| Health insurance | ||||||
| Has health coverage | 1219 | 97.4 * | 1337 | 98.5 * | 2556 | 98.0 |
| Don’t know/No answer | 12 | 1.0 | 10 | 0.7 | 22 | 0.8 |
| Medical history | ||||||
| Has suffered from a heart attack | 83 | 6.7 ** | 54 | 4.0 ** | 137 | 5.3 |
| Don’t know/No answer | 1 | 0.1 | 1 | 0.1 | 2 | 0.1 |
| Has been diagnosed with a cardiovascular disease (other than heart attack) | 148 | 12.0 ** | 120 | 8.9 ** | 268 | 10.3 |
| Don’t know/No answer | 13 | 1.0 | 6 | 0.4 | 19 | 0.7 |
| Close relative or friend has had a heart attack | 731 | 58.7 * | 843 | 62.5 * | 1575 | 60.7 |
| Don’t know/No answer | 15 | 1.2 | 14 | 1.0 | 29 | 1.1 |
| Close relative or friend has had another severe cardiovascular disease (different from a heart attack: myocardial infarction or angina pectoris) | 502 | 40.9 * | 589 | 44.2 * | 1090 | 42.6 |
| Don’t know/No answer | 44 | 3.5 | 41 | 3.0 | 85 | 3.3 |
| Have you ever taken a screening test to know about your risk of being affected by cardiovascular disease? | 645 | 52.0 ** | 472 | 35.2 ** | 1134 | 43.2 |
| Don’t know/No answer | 13 | 1.0 | 14 | 1.0 | 27 | 1.0 |
| High Education | Low Education | High SES | Low SES | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |||||||||||
| Characteristic | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % |
| Leading health issue (affecting your gender) | ||||||||||||||||||||
| Cancer in general | 250 | 22.8 * | 235 | 19.9 * | 119 | 26.4 xx | 76 | 18.2 | 131 | 20.3 xx | 159 | 21.0 | 116 | 22.3 | 71 | 16.4 †† | 133 | 21.7 | 151 | 20.1 †† |
| Lung cancer | 19 | 1.8 * | 1 | 0.1 * | 7 | 1.6 | 1 | 0.1 | 12 | 2.0 | 0 | 0.1 | 8 | 1.7 | 0 | 0.0 | 11 | 1.9 | 1 | 0.1 |
| Breast cancer | 266 | 22.5 | 92 | 22.2 | 174 | 22.9 | 74 | 17.2 †† | 192 | 25.7 †† | ||||||||||
| Diabetes | 30 | 2.8 | 28 | 2.4 | 12 | 2.8 | 12 | 2.9 | 18 | 2.8 | 16 | 2.2 | 14 | 2.7 | 13 | 2.9 | 16 | 2.8 | 15 | 2.1 |
| Heart disease/Heart attack | 210 | 19.2 ** | 50 | 4.2 ** | 88 | 19.7 | 25 | 5.9 †† | 122 | 19.2 | 25 | 3.4 †† | 118 | 22.7 xx | 28 | 6.7 †† | 87 | 14.2 xx | 22 | 3.0 †† |
| Obesity | 109 | 10.0 * | 69 | 5.8 * | 54 | 12.0 xx | 31 | 6.8 †† | 55 | 8.8 xx | 38 | 4.7 †† | 57 | 11.2 xx | 39 | 9.0 †† | 52 | 8.5 xx | 26 | 3.4 †† |
| Don’t know/No answer | 157 | 12.5 | 174 | 12.8 | 65 | 12.8 | 53 | 11.3 | 86 | 11.9 | 115 | 13.4 | 54 | 10.3 | 37 | 8.4 | 86 | 14.0 | 100 | 13.3 |
| Leading cause of death (affecting your gender) | ||||||||||||||||||||
| Accidental death | 31 | 2.7 * | 5 | 0.4 * | 9 | 1.9 xx | 3 | 0.8 †† | 22 | 3.3 xx | 2 | 0.2 †† | 16 | 3.3 | 3 | 0.9 †† | 15 | 2.8 | 2 | 0.3 †† |
| Cancer in general | 260 | 22.9 * | 573 | 49.1 * | 101 | 21.4 | 202 | 48.7 | 159 | 23.7 | 371 | 49.2 | 100 | 19.1 xx | 218 | 50.1 | 146 | 23.8 xx | 355 | 47.4 |
| Lung cancer | 42 | 3.7 * | 13 | 1.1 * | 6 | 1.2 xx | 0 | 0.0 †† | 36 | 5.2 xx | 13 | 1.8 †† | 7 | 1.4 xx | 1 | 0.1 †† | 29 | 4.7 xx | 11 | 1.4 †† |
| Breast cancer | 199 | 17.0 | 72 | 17.1 | 127 | 16.7 | 68 | 15.7 | 129 | 17.1 | ||||||||||
| Heart disease/Heart attack | 565 | 49.9 ** | 192 | 16.5 ** | 259 | 55.5 xx | 75 | 18.1 | 306 | 46.1 xx | 117 | 15.6 | 301 | 59.4 xx | 83 | 19.7 †† | 264 | 44.2 xx | 109 | 15.2 †† |
| Stroke | 58 | 5.1 | 56 | 4.8 | 17 | 3.8 xx | 17 | 4.2 | 41 | 6.1 xx | 39 | 5.3 | 18 | 3.7 xx | 13 | 2.9†† | 40 | 6.9 xx | 43 | 6.0 †† |
| Don’t know/No answer | 121 | 9.7 | 189 | 13.9 | 42 | 8.3 | 52 | 11.0 | 73 | 10.0 | 132 | 15.3 | 48 | 9.3 | 62 | 14.3 | ||||
| What are the warning signs that you associate with having a heart attack? | ||||||||||||||||||||
| Chest pain (discomfort and sharp pain) | 759 | 60.6 ** | 779 | 57.4 ** | 334 | 65.6 xx | 305 | 64.4 †† | 418 | 57.6 xx | 467 | 54.3 †† | 340 | 65.3 xx | 288 | 66.3 †† | 345 | 56.2 xx | 399 | 53.0 †† |
| Radiation of pain | 532 | 42.5 ** | 659 | 48.6 ** | 221 | 43.5 | 246 | 52.0† | 303 | 41.8 | 405 | 47.1 † | 237 | 45.4 xx | 241 | 55.4 †† | 234 | 38.1 xx | 338 | 45.0 †† |
| Dyspnea (shortness of breath) | 219 | 17.5 * | 268 | 19.7 * | 97 | 19.1 | 96 | 20.4 | 122 | 16.8 | 169 | 19.7 | 111 | 21.3 xx | 111 | 25.6 †† | 89 | 14.5 xx | 129 | 17.2 †† |
| Nausea | 66 | 5.3 ** | 171 | 12.6 ** | 36 | 7.0 xx | 68 | 14.4 | 29 | 4.0 xx | 102 | 11.9 | 36 | 7.0 xx | 42 | 9.7 † | 22 | 3.6 xx | 102 | 13.6† |
| Sweating | 110 | 8.8 ** | 55 | 4.1 ** | 51 | 10.1 | 22 | 4.6 | 59 | 8.1 | 31 | 3.6 | 58 | 11.1 xx | 17 | 3.9 | 39 | 6.4 xx | 33 | 4.4 |
| Unusual fatigue | 60 | 4.8 | 64 | 4.7 | 18 | 3.6 x | 29 | 6.2 † | 42 | 5.8 x | 34 | 4.0 † | 20 | 3.9 x | 20 | 4.7 | 36 | 5.8 x | 38 | 5.1 |
| Dizziness | 180 | 14.4 * | 160 | 11.8 * | 95 | 18.6 xx | 59 | 12.4 | 85 | 11.8 xx | 99 | 11.5 | 77 | 14.7 | 56 | 12.8 | 88 | 14.4 | 91 | 12.1 |
| Generalized weakness | 83 | 6.7 * | 62 | 4.6 * | 38 | 7.4 | 22 | 4.7 | 45 | 6.3 | 40 | 4.7 | 33 | 6.3 | 22 | 5.0 | 45 | 7.4 | 39 | 5.2 |
| Palpitations | 100 | 8.0 * | 138 | 10.1 * | 45 | 8.9 | 48 | 10.1 | 52 | 7.2 | 84 | 9.8 | 35 | 6.8 x | 48 | 11.1 | 58 | 9.4 x | 79 | 10.5 |
| Don’t know/No answer | 305 | 24.4 | 140 | 10.3 | 109 | 21.4 | 35 | 7.5 | 188 | 25.9 | 104 | 12.1 | 105 | 20.1 | 22 | 5.1 | 174 | 28.4 | 97 | 12.9 |
| Knows the main symptoms | 205 | 16.3 | 208 | 15.4 | 97 | 19.1 xx | 96 | 20.4 †† | 105 | 14.5 xx | 108 | 12.6 †† | 102 | 19.6 xx | 89 | 20.5 †† | 86 | 14.0 xx | 102 | 13.6 †† |
| If you thought you were experiencing a heart attack, what is the first thing you would do? | ||||||||||||||||||||
| Take an aspirin | 10 | 0.8 | 16 | 1.2 | 6 | 1.2 | 7 | 1.4 | 4 | 0.6 | 6 | 0.7 | 7 | 1.3 xx | 3 | 0.7 | 2 | 0.4 xx | 10 | 1.3 |
| Go to a hospital | 117 | 9.3 | 135 | 9.9 | 39 | 7.6 xx | 37 | 7.8 †† | 78 | 10.8 xx | 96 | 11.2 †† | 39 | 7.4 xx | 31 | 7.2 †† | 72 | 11.7 xx | 94 | 12.5 †† |
| Call a doctor | 187 | 15.0 * | 227 | 16.7 * | 68 | 13.4 xx | 51 | 10.8 †† | 117 | 16.1 xx | 166 | 19.3 †† | 77 | 14.8 | 59 | 13.5 †† | 91 | 14.9 | 149 | 19.8 †† |
| Call emergency medical services (112) | 681 | 54.4 * | 781 | 57.6 * | 298 | 58.6 xx | 317 | 67.1†† | 376 | 51.8 xx | 458 | 53.3 †† | 286 | 54.8 | 281 | 64.7 †† | 327 | 53.3 | 390 | 51.9 †† |
| Call your spouse or a family member | 109 | 8.7 * | 94 | 6.9 * | 51 | 10.1 xx | 36 | 7.6 | 57 | 7.9 xx | 56 | 6.5 | 49 | 9.4 | 33 | 7.5 | 52 | 8.4 | 47 | 6.3 |
| Other | 119 | 9.5 * | 71 | 5.2 * | 43 | 8.5 | 21 | 4.5 | 68 | 9.4 | 50 | 5.8 | 60 | 11.6 xx | 24 | 5.5 | 47 | 7.7 xx | 38 | 5.0 |
| Don’t know | 28 | 2.2 | 33 | 2.5 | 3 | 0.5 xx | 4 | 0.8 †† | 25 | 3.4 xx | 28 | 3.3 †† | 4 | 0.7 xx | 4 | 1.0 †† | 23 | 3.7 xx | 24 | 3.2 †† |
| Call emergency services versus all other options | 681 | 54.4 * | 781 | 57.6 * | 299 | 58.7 xx | 318 | 67.2 †† | 376 | 51.8 xx | 458 | 53.3 †† | 286 | 54.8 | 281 | 64.7 †† | 327 | 53.3 | 390 | 51.9 †† |
| High Education | Low Education | High SES | Low SES | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |||||||||||
| Characteristic | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % |
| Main risk factors for suffering cardiovascular disease | ||||||||||||||||||||
| High blood pressure | 142 | 11.4 ** | 251 | 18.5 ** | 81 | 16.0 xx | 109 | 23.0 †† | 60 | 8.3 xx | 141 | 16.4 †† | 67 | 18.8 | 58 | 13.4 †† | 75 | 17.8 | 65 | 8.7 †† |
| Cholesterol (low good cholesterol or high bad cholesterol) | 74 | 5.9 ** | 142 | 10.4 ** | 46 | 9.1 xx | 64 | 13.5 †† | 28 | 3.9 xx | 74 | 8.6 †† | 37 | 11.0 | 32 | 7.4 †† | 37 | 9.4 | 29 | 3.8 †† |
| Family history of heart disease or stroke | 128 | 10.2 ** | 211 | 15.6 ** | 65 | 12.8 xx | 108 | 22.8 †† | 62 | 8.6xx | 97 | 11.3 †† | 69 | 18.7 x | 50 | 11.6 † | 59 | 13.4 x | 64 | 8.5† |
| Smoking habit | 794 | 63.4 * | 812 | 59.8 * | 322 | 63.2 | 300 | 63.4 † | 455 | 62.7 | 499 | 58.0 † | 369 | 60.4x | 304 | 69.8†† | 351 | 48.9 xx | 429 | 57.0 †† |
| Drinking alcohol | 598 | 47.8 ** | 376 | 27.7 ** | 231 | 45.4 | 134 | 28.3 | 354 | 48.8 | 237 | 27.5 | 258 | 37.0 x | 147 | 50.6† | 262 | 32.0 x | 229 | 45.3 † |
| Diabetes | 46 | 3.6 ** | 99 | 7.3 ** | 29 | 5.8 xx | 41 | 8.7 † | 17 | 2.3 xx | 58 | 6.7 † | 22 | 6.3 | 20 | 4.5† | 24 | 5.7 | 21 | 3.0† |
| Unhealthy diet habits | 489 | 39.1 | 544 | 40.1 | 223 | 43.8 xx | 225 | 47.6 †† | 259 | 35.7 xx | 311 | 36.2 †† | 230 | 44.2 x | 181 | 41.5 † | 221 | 36.0 xx | 272 | 36.2 † |
| Not exercising | 537 | 42.9 * | 542 | 40.0 * | 277 | 54.5 xx | 236 | 49.9 †† | 258 | 35.6xx | 296 | 34.4 †† | 254 | 48.7 x | 226 | 51.9 †† | 200 | 32.5 xx | 262 | 34.9 †† |
| Obesity | 394 | 31.4 ** | 501 | 36.9 ** | 182 | 35.8 xx | 187 | 39.6 † | 210 | 28.9 xx | 296 | 34.4 † | 207 | 39.8 x | 187 | 43.1 †† | 153 | 24.9 xx | 162 | 21.6 †† |
| Stress | 804 | 64.2 | 847 | 62.4 | 313 | 61.4x | 313 | 66.2 † | 473 | 65.3 x | 529 | 61.5 † | 353 | 67.7 | 288 | 66.3 | 403 | 65.6 | 475 | 63.1 |
| Other | 95 | 7.6 ** | 226 | 16.7 ** | 35 | 6.9 | 89 | 18.9 † | 59 | 8.2 | 134 | 15.6† | 35 | 10.2 x | 51 | 11.7 | 60 | 15.0 x | 105 | 13.9 |
| Don’t know | 143 | 11.4 | 72 | 5.3 | 40 | 7.8 | 14 | 3.0 | 103 | 14.2 | 52 | 6.0 | 30 | 5.8 | 7 | 1.7 | 103 | 16.8 | 47 | 6.2 |
| Preventive actions | ||||||||||||||||||||
| Eating more fruit and vegetables | 544 | 43.4 * | 626 | 46.3 * | 211 | 41.5 | 178 | 37.6 †† | 324 | 44.7 | 437 | 50.8†† | 212 | 40.6 | 201 | 46.1 | 273 | 44.4 | 365 | 48.6 |
| Physical activity | 846 | 67.6 | 891 | 65.9 | 362 | 71.2x | 339 | 71.6 †† | 481 | 66.3 x | 543 | 63.1 †† | 389 | 74.7 xx | 309 | 71.0 †† | 395 | 64.4 xx | 483 | 64.2 †† |
| Regular medical check-ups | 351 | 28.1 * | 409 | 30.3 * | 126 | 24.8 x | 152 | 32.1 | 220 | 30.3x | 249 | 29.0 | 135 | 25.9 x | 120 | 27.5 † | 191 | 31.1 x | 237 | 31.5 † |
| Keep a healthy weight | 472 | 37.7 * | 478 | 35.3 * | 215 | 42.2 xx | 187 | 39.5 †† | 247 | 34.0 xx | 278 | 32.3 †† | 212 | 40.7 x | 161 | 37.0 | 213 | 34.7 x | 255 | 33.9 |
| Not smoking | 636 | 50.8 ** | 638 | 47.2 ** | 269 | 52.8 | 245 | 51.8 †† | 360 | 49.6 | 378 | 44.0 †† | 276 | 53.0 x | 223 | 51.3 †† | 289 | 47.0 x | 316 | 42.0 †† |
| Improve stress management | 334 | 26.7 ** | 321 | 23.8 ** | 145 | 28.4 x | 121 | 25.5 | 180 | 24.8 x | 200 | 23.4 | 148 | 28.5 | 120 | 27.5 †† | 161 | 26.3 | 157 | 20.9 †† |
| Hypertension control | 275 | 22.0 ** | 374 | 27.7 ** | 99 | 19.4 x | 130 | 27.4 | 171 | 23.6 x | 237 | 27.6 | 106 | 20.3 | 107 | 24.7 † | 136 | 22.2 | 217 | 28.8 † |
| Taking vitamins | 18 | 1.4 * | 30 | 2.2 * | 6 | 1.2 | 7 | 1.4 † | 9 | 1.3 | 23 | 2.7† | 1 | 0.2 xx | 8 | 1.8 | 14 | 2.3 xx | 22 | 2.9 |
| Taking antioxidants | 12 | 0.9 | 15 | 1.1 | 4 | 0.7 | 5 | 1.1 | 8 | 1.1 | 10 | 1.2 | 2 | 0.4 x | 5 | 1.1 | 9 | 1.4 x | 10 | 1.3 |
| Hormone replacement therapy | 4 | 0.3 | 3 | 0.2 | 0 | 0.0x | 0 | 0.0 † | 4 | 0.5 x | 3 | 0.4 † | 1 | 0.1 | 1 | 0.1 | 2 | 0.4 | 1 | 0.1 |
| Diabetes control | 117 | 9.3 * | 108 | 8.0* | 44 | 8.6 | 28 | 6.0 † | 73 | 10.0 | 77 | 8.9 † | 39 | 7.5 x | 21 | 4.9 †† | 61 | 9.9 x | 74 | 9.9†† |
| Don’t know | 13 | 1.1 | 10 | 0.7 | 4 | 0.8 | 1 | 0.2 † | 9 | 1.3 | 9 | 1.0 † | 2 | 0.3x | 3 | 0.7 | 10 | 1.7 x | 3 | 0.4 |
| Individuals who are most at risk of suffering from cardiovascular disease | ||||||||||||||||||||
| Men have more heart diseases than women | 960 | 80.2 ** | 892 | 69.9 ** | 417 | 82.0 x | 339 | 74.7 †† | 542 | 78.8 x | 553 | 67.0 †† | 443 | 85.1 xx | 312 | 71.7 | 461 | 75.0 xx | 517 | 68.8 |
| Don’t know/No answer | 55 | 4.4 | 81 | 6.0 | 29 | 5.7 | 24 | 5.0 | 26 | 3.6 | 54 | 6.3 | 24 | 4.7 | 14 | 3.3 | 21 | 3.4 | 44 | 5.8 |
| Men that are highly stressed executive professionals are more prone to heart attacks | 1059 | 85.7 | 1151 | 86.2 | 436 | 85.6 | 406 | 85.8 | 621 | 85.7 | 740 | 86.1 | 450 | 86.4 | 378 | 86.9 | 533 | 86.8 | 650 | 86.4 |
| Don’t know/No answer | 15 | 1.2 | 22 | 1.6 | 9 | 1.7 | 1 | 0.2 | 7 | 0.9 | 22 | 2.5 | 5 | 0.9 | 1 | 0.1 | 10 | 1.6 | 15 | 2.0 |
| Young women, under 50, do not have heart attacks | 310 | 25.7** | 274 | 20.8 ** | 109 | 21.8 xx | 100 | 21.3 | 201 | 28.4 xx | 174 | 20.6 | 126 | 24.1 x | 78 | 17.9 † | 176 | 28.7 x | 165 | 21.9 † |
| Don’t know/No answer | 46 | 3.7 | 35 | 2.6 | 22 | 4.3 | 4 | 0.9 | 25 | 3.5 | 32 | 3.7 | 18 | 3.4 | 1 | 0.1 | 23 | 3.8 | 27 | 3.6 |
| In women the probability of heart disease increases after menopause | 667 | 65.2** | 830 | 69.1 ** | 288 | 68.4 x | 320 | 75.1 †† | 379 | 63.3 x | 510 | 65.8 †† | 298 | 63.1 | 308 | 70.7 | 369 | 66.3 | 506 | 67.3 |
| Don’t know/No answer | 230 | 18.4 | 156 | 11.5 | 112 | 22.0 | 50 | 10.6 | 112 | 15.5 | 106 | 12.3 | 97 | 18.6 | 38 | 8.7 | 109 | 17.8 | 85 | 11.3 |
| Only women who adopt behaviors and lifestyles of men will have heart disease | 290 | 24.7 * | 301 | 22.9 * | 99 | 20.5 xx | 64 | 13.7 †† | 191 | 27.9 xx | 237 | 27.9 †† | 122 | 23.5 x | 72 | 16.6 †† | 167 | 27.2 x | 199 | 26.5 †† |
| Don’t know/No answer | 78 | 6.2 | 46 | 3.4 | 30 | 5.8 | 15 | 3.1 | 48 | 6.6 | 31 | 3.6 | 22 | 4.3 | 2 | 0.4 | 47 | 7.7 | 34 | 4.5 |
| Only women which have brought up children will have heart disease | 55 | 4.6 | 54 | 4.0 | 13 | 2.6 xx | 7 | 1.5 †† | 42 | 6.1 xx | 45 | 5.2 †† | 21 | 4.0 | 7 | 1.7 †† | 28 | 4.6 | 43 | 5.7 †† |
| Don’t know/No answer | 70 | 5.6 | 31 | 2.3 | 21 | 4.2 | 7 | 1.5 | 30 | 4.2 | 25 | 2.9 | 18 | 3.4 | 1 | 0.1 | 31 | 5.0 | 23 | 3.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daponte-Codina, A.; Knox, E.C.; Mateo-Rodriguez, I.; Seims, A.; Regitz-Zagrosek, V.; Maas, A.H.E.M.; White, A.; Barnhoorn, F.; Rosell-Ortiz, F. Gender and Social Inequalities in Awareness of Coronary Artery Disease in European Countries. Int. J. Environ. Res. Public Health 2022, 19, 1388. https://doi.org/10.3390/ijerph19031388
Daponte-Codina A, Knox EC, Mateo-Rodriguez I, Seims A, Regitz-Zagrosek V, Maas AHEM, White A, Barnhoorn F, Rosell-Ortiz F. Gender and Social Inequalities in Awareness of Coronary Artery Disease in European Countries. International Journal of Environmental Research and Public Health. 2022; 19(3):1388. https://doi.org/10.3390/ijerph19031388
Chicago/Turabian StyleDaponte-Codina, Antonio, Emily C. Knox, Inmaculada Mateo-Rodriguez, Amanda Seims, Vera Regitz-Zagrosek, Angela H. E. M. Maas, Alan White, Floris Barnhoorn, and Fernando Rosell-Ortiz. 2022. "Gender and Social Inequalities in Awareness of Coronary Artery Disease in European Countries" International Journal of Environmental Research and Public Health 19, no. 3: 1388. https://doi.org/10.3390/ijerph19031388
APA StyleDaponte-Codina, A., Knox, E. C., Mateo-Rodriguez, I., Seims, A., Regitz-Zagrosek, V., Maas, A. H. E. M., White, A., Barnhoorn, F., & Rosell-Ortiz, F. (2022). Gender and Social Inequalities in Awareness of Coronary Artery Disease in European Countries. International Journal of Environmental Research and Public Health, 19(3), 1388. https://doi.org/10.3390/ijerph19031388