
The Promise of Digital Self-Management: A Reflection about the Effects of Patient-Targeted e-Health Tools on Self-Management and Wellbeing

{kind=link}
{kind=link}
Abstract
:1. Introduction
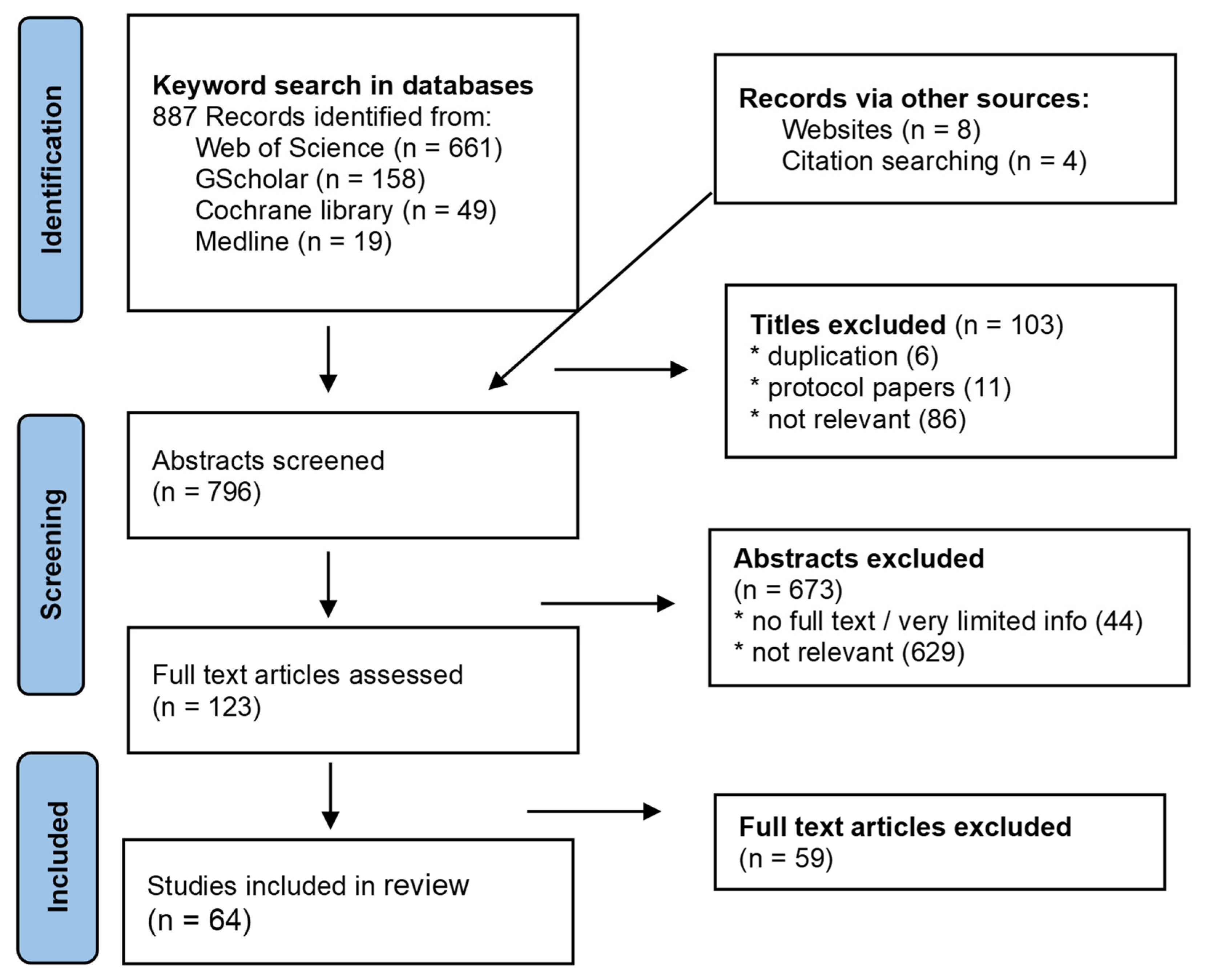
2. Materials and Methods
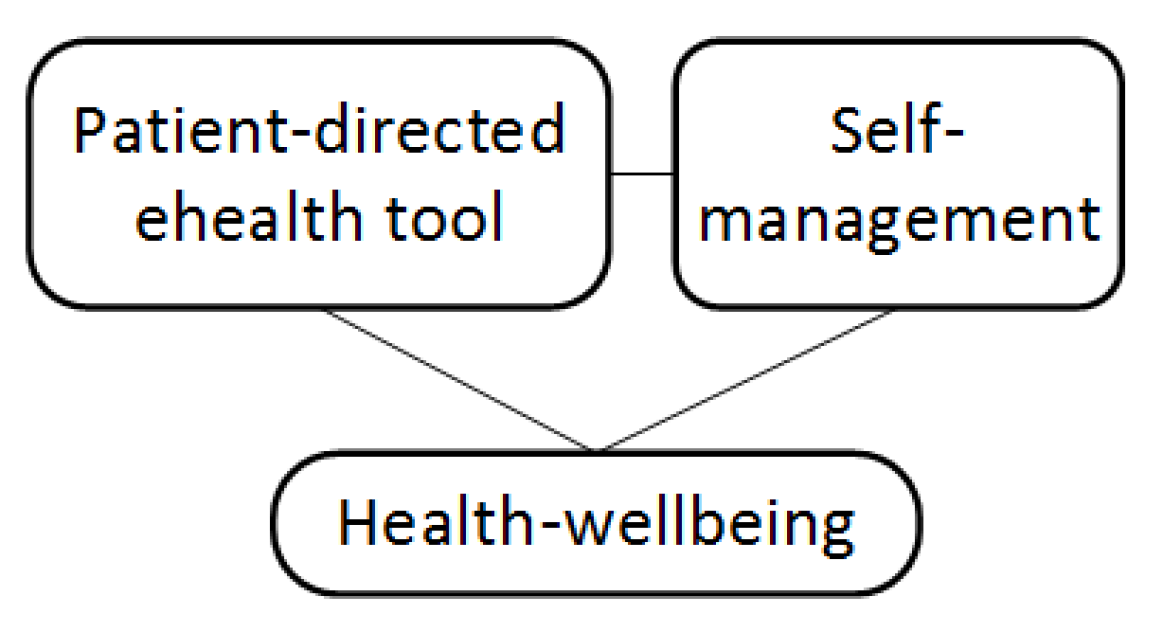
2.1. Conceptual Framework
2.2. Study Selection
3. Results
3.1. The Relationship between Patient-Directed e-Health Tools and Self-Management
3.2. The Relationship between Self-Management and Wellbeing
3.3. The Relationship between Patient-Directed e-Health Tools and Wellbeing
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Topol, E. The Patient Eill See You Now: The Future of Medicine Is in Your Hands; Basic Books: New York, NY, USA, 2015. [Google Scholar]
- Finoulst, M. Dokter Google; Houtekiet: Assenede, Belgium, 2020. [Google Scholar]
- Talboom-Kamp, E.; Tossaint-Schoenmakers, R.; Goedhart, A.; Versluis, A.; Kasteleyn, M. Patients’ attitudes toward an online patient portal for communicating laboratory test results: Real-world study using the ehealth impact questionnaire. J. Med. Internet Res. 2020, 22, e17060. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Digital Health. A Digital (R)evolution: Introducing the Lancet Digital Health. Lancet Digit. Health 2019, 1, e1. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, R.C.; Bornkessel, A.S. Digital Social Networks and Health. Circulation 2013, 127, 1829–1836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient self-management of chronic disease in primary care. JAMA J. Am. Med. Assoc. 2002, 288, 2469–2475. [Google Scholar] [CrossRef]
- Coster, S.; Norman, I. Cochrane reviews of educational and self-management interventions to guide nursing practice: A review. Int. J. Nurs. Stud. 2009, 46, 508–528. [Google Scholar] [CrossRef]
- Lorig, K.; Ritter, P.L.; Plant, K. A disease-specific self-help program compared with a generalized chronic disease self-help program for arthritis patients. Arthritis Rheum. 2005, 53, 950–957. [Google Scholar] [CrossRef]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [Green Version]
- Palmer, M.J.; Machiyama, K.; Woodd, S.; Gubijev, A.; Barnard, S.; Russell, S.; Perel, P.; Free, C. Mobile phone-based interventions for improving adherence to medication prescribed for the primary prevention of cardiovascular disease in adults. Cochrane Database Syst. Rev. 2021, 3, CD012675. [Google Scholar] [CrossRef]
- Stephanie, L.; Sharma, R.S. Digital health eco-systems: An epochal review of practice-oriented research. Int. J. Inf. Manag. 2020, 53, 102032. [Google Scholar] [CrossRef]
- Sharon, T. When digital health meets digital capitalism, how many common goods are at stake? Big Data Soc. 2018, 5, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lupton, D. The digitally engaged patient: Self-monitoring and self-care in the digital health era. Soc. Theory Health 2013, 11, 256–270. [Google Scholar] [CrossRef]
- Singh, K.; Meyer, S.R.; Westfall, J.M. Consumer-Facing Data, Information, and Tools: Self-Management of Health in the Digital Age. Health Aff. 2019, 38, 352–358. [Google Scholar] [CrossRef]
- Morrissey, E.C.; Casey, M.; Glynn, L.G.; Walsh, J.C.; Molloy, G.J. Smartphone apps for improving medication adherence in hypertension: Patients’ perspectives. Patient Prefer. Adherence 2018, 12, 813–822. [Google Scholar] [CrossRef] [Green Version]
- Adams, K.; Greiner, A.; Corrigan, J. The 1st Annual Crossing the Quality Chasm Summit: A Focus on Communities; National Academies Press (US): Washington, DC, USA, 2004. [Google Scholar]
- Ryan, R.M.; Huta, V.; Deci, E.L. Living Well: A Self Determination Theory Perspective on Eudaimonia. J. Happiness Stud. 2008, 9, 139–170. [Google Scholar] [CrossRef]
- Arcury, T.A.; Sandberg, J.C.; Melius, K.P.; Quandt, S.A.; Leng, X.; Latulipe, C.; Miller, D.P., Jr.; Smith, D.A.; Bertoni, A.G. Older Adult Internet Use and eHealth Literacy. J. Appl. Gerontol. 2020, 39, 141–150. [Google Scholar] [CrossRef]
- Meppelink, C.S.; Smit, E.G.; Diviani, N.; van Weert, J.C.M. Health Literacy and Online Health Information Processing: Unraveling the Underlying Mechanisms. J. Health Commun. 2016, 21, 109–120. [Google Scholar] [CrossRef] [Green Version]
- Wulfovich, S.; Fiordelli, M.; Rivas, H.; Concepcion, W.; Wac, K. ‘I Must Try Harder’: Design Implications for Mobile Apps and Wearables Contributing to Self-Efficacy of Patients with Chronic Conditions. Front. Psychol. 2019, 10, 2388. [Google Scholar] [CrossRef] [Green Version]
- King, C.E.; Sarrafzadeh, M. A Survey of Smartwatches in Remote Health Monitoring. J. Healthc. Inform. Res. 2018, 2, 1–24. [Google Scholar] [CrossRef]
- Hixson, J.D.; Braverman, L. Digital tools for epilepsy: Opportunities and barriers. Epilepsy Res. 2020, 162. [Google Scholar] [CrossRef]
- Johnson, A.J.; Palit, S.; Terry, E.L.; Thompson, O.J.; Powell-Roach, K.; Dyal, B.W.; Ansell, M.; Booker, S.Q. Managing osteoarthritis pain with smart technology: A narrative review. Rheumatol. Adv. Pract. 2021, 5. [Google Scholar] [CrossRef]
- Lalloo, C.; Shah, U.; Birnie, K.A.; Davies-Chalmers, C.; Rivera, J.; Stinson, J.; Campbell, F. Commercially Available Smartphone Apps to Support Postoperative Pain Self-Management: Scoping Review. JMIR mHealth uHealth 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Ter Huurne, E.D.; Postel, M.G.; de Haan, H.A.; van der Palen, J.; DeJong, C.A.J. Treatment dropout in web-based cognitive behavioral therapy for patients with eating disorders. Psychiatry Res. 2017, 247, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Sorkin, D.H.; Janio, E.A.; Eikey, E.V.; Schneider, M.; Davis, K.; Schueller, S.M.; Stadnick, N.A.; Zheng, K.; Neary, M.; Safani, D.; et al. Rise in Use of Digital Mental Health Tools and Technologies in the United States During the COVID-19 Pandemic: Survey Study. J. Med. Internet Res. 2021, 23, e26994. [Google Scholar] [CrossRef] [PubMed]
- Hixson, J. Use of a Digital Self-Management Platform for Improving Access in Epilepsy Patients. Neurology 2016, 86. Available online: https://n.neurology.org/content/86/16_Supplement/I14.004 (accessed on 10 January 2022).
- Algeo, N.; Hunter, D.; Cahill, A.; Dickson, C.; Adams, J. Usability of a digital self-management website for people with osteoarthritis: A UK patient and public involvement study. Int. J. Ther. Rehabil. 2017, 24, 78–82. [Google Scholar] [CrossRef]
- Merchant, R.; Inamdar, R.; Henderson, K.; Barrett, M.A.; van Sickle, D. Digital Health Intervention for Asthma: Patient Perception of Usability and Value for Self-Management. Am. J. Respir. Crit. Care Med. 2017, 195, A3326. [Google Scholar]
- Tendedez, H.; Ferrario, M.A.; McNaney, R.; Whittle, J. Respiratory Self-Care: Identifying Current Challenges and Future Potentials for Digital Technology to Support People with Chronic Respiratory Conditions. In Proceedings of the 13th EAI International Conference on Pervasive Computing Technologies for Healthcare (PervasiveHealth), Trento, Italy, 20–23 May 2019; pp. 129–138. [Google Scholar] [CrossRef] [Green Version]
- Svendsen, M.J.; Wood, K.W.; Kyle, J.; Cooper, K.; Rasmussen, C.D.N.; Sandal, L.F.; Stochkendahl, M.J.; Mair, F.S.; Nicholl, B.I. Barriers and facilitators to patient uptake and utilisation of digital interventions for the self-management of low back pain: A systematic review of qualitative studies. BMJ Open 2020, 10, e038800. [Google Scholar] [CrossRef]
- Neal, D.; van den Berg, F.; Planting, C.; Ettema, T.; Dijkstra, K.; Finnema, E.; Dröes, R.M. Can Use of Digital Technologies by People with Dementia Improve Self-Management and Social Participation? A Systematic Review of Effect Studies. J. Clin. Med. 2021, 10, 604. [Google Scholar] [CrossRef]
- Hamideh, D.; Nebeker, C. The Digital Health Landscape in Addiction and Substance Use Research: Will Digital Health Exacerbate or Mitigate Health Inequities in Vulnerable Populations? Curr. Addict. Rep. 2020, 7, 317–332. [Google Scholar] [CrossRef]
- Lau, S.C.L.; Bhattacharjya, S.; Fong, M.W.; Nicol, G.E.; Lenze, E.J.; Baum, C.; Hardi, A.; Wong, A.W. Effectiveness of theory-based digital self-management interventions for improving depression, anxiety, fatigue and self-efficacy in people with neurological disorders: A systematic review and meta-analysis. J. Telemed. Telecare 2020. [Google Scholar] [CrossRef]
- Adesina, N.; Dogan, H.; Green, S.; Tsofliou, F. Dietary digital tools to support self-management of gestational diabetes mellitus: A systematic literature review. Proc. Nutr. Soc. 2021, 80. [Google Scholar] [CrossRef]
- Scott, I.A.; Scuffham, P.; Gupta, D.; Harch, T.M.; Borchi, J.; Richards, B. Going digital: A narrative overview of the effects, quality and utility of mobile apps in chronic disease self-management. Aust. Health Rev. 2020, 44, 62–82. [Google Scholar] [CrossRef]
- Nkhom, D.; Soko, C.J.; Bowrin, P.; Iqbal, U. Digital Health Interventions for Diabetes Self-Management Education/Support in Type 1 & 2 Diabetes Mellitus. Stud. Health Technol. Inform. 2020, 270, 1263–1264. [Google Scholar]
- Berry, N.; Lobban, F.; Bucci, S. A qualitative exploration of service user views about using digital health interventions for self-management in severe mental health problems. BMC Psychiatry 2019, 19, 35. [Google Scholar] [CrossRef] [Green Version]
- Baltaxe, E.; Czypionka, T.; Kraus, M.; Reiss, M.; Askildsen, J.E.; Grenković, R.; Lindén, T.S.; Pitter, J.G.; Rutten-van Molken, M.; Solans, O.; et al. Digital health transformation of integrated care in Europe: An overarching content analysis of 17 integrated care programmes. J. Med. Internet Res. 2019, 21, e14956. [Google Scholar] [CrossRef] [Green Version]
- Li, L.C.; Townsend, A.F.; Badley, E.M. Self-management interventions in the digital age: New approaches to support people with rheumatologic conditions. Best Pract. Res. Clin. Rheumatol. 2012, 26, 321–333. [Google Scholar] [CrossRef]
- Villalobos, N.; Vela, F.S.; Hernandez, L.M. Digital Healthcare Intervention to Improve Self-Management for Patients with Type 2 Diabetes: A Scoping Review. J. Sci. Innov. Med. 2020, 3, 1–11. [Google Scholar] [CrossRef]
- Tran, J.; Tran, R.; White, J.R. Smartphone-based glucose monitors and applications in the management of diabetes: An overview of 10 salient ‘apps’ and a novel smartphone-connected blood glucose monitor. Clin. Diabetes 2012, 30, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Radhakrishnan, K.; Baranowski, T.; Julien, C.; Thomaz, E.; Kim, M. Role of Digital Games in Self-Management of Cardiovascular Diseases: A Scoping Review. Games Health J. 2019, 8, 65–73. [Google Scholar] [CrossRef]
- Lagan, S.; Ramakrishnan, A.; Lamont, E.; Ramakrishnan, A.; Frye, M.; Torous, J. Digital health developments and drawbacks: A review and analysis of top-returned apps for bipolar disorder. Int. J. Bipolar Disord. 2020, 8. [Google Scholar] [CrossRef]
- The Lancet Infectious Diseases. The COVID-19 infodemic. Lancet Infect. Dis. 2020, 20, 875. [Google Scholar] [CrossRef]
- Wagner, T.; Lindstadt, C.; Jeon, Y.; Mackert, M. Implantable Medical Device Website Efficacy in Informing Consumers Weighing Benefits/Risks of Health Care Options. J. Health Commun. 2016, 21, 121–126. [Google Scholar] [CrossRef]
- Liang, J.; Xian, D.; Liu, X.; Fu, J.; Zhang, X.; Tang, B.; Lei, J. Usability study of mainstream wearable fitness devices: Feature analysis and system usability scale evaluation. JMIR mHealth uHealth 2018, 6, e11066. [Google Scholar] [CrossRef] [Green Version]
- Lorig, K.; Holman, H. Self-management education: History, definition, outcomes, and mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef]
- Dineen-Griffin, S.; Garcia-Cardenas, V.; Williams, K.; Benrimoj, S.I. Helping patients help themselves: A systematic review of self-management support strategies in primary health care practice. PLoS ONE 2019, 14, e0220116. [Google Scholar] [CrossRef] [Green Version]
- O’Connell, S.; McCarthy, V.J.C.; Savage, E. Frameworks for self-management support for chronic disease: A cross-country comparative document analysis. BMC Health Serv. Res. 2018, 18, 583. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Dobransky, P. From Being Ashamed to Being Empowered. Psychol. Today 2010. Available online: https://www.psychologytoday.com/us/blog/the-urban-scientist/201005/being-ashamed-being-empowered (accessed on 28 January 2021).
- Sennet, R. Shame Is the Key; New York Times: New York, NY, USA, 1978; p. 4. [Google Scholar]
- Archer, A. Shame and diabetes self-management. Pract. Diabetes 2014, 31, 102–106. [Google Scholar] [CrossRef]
- Parikh, N.S.; Parker, R.M.; Nurss, J.R.; Baker, D.W.; Williams, M.V. Shame and health literacy: The unspoken connection. Patient Educ. Couns. 1996, 27, 33–39. [Google Scholar] [CrossRef]
- Ellis, J.; Boger, E.; Latter, S.; Kennedy, A.; Jones, F.; Foster, C.; Demain, S. Conceptualisation of the ‘good’ self-manager: A qualitative investigation of stakeholder views on the self-management of long-term health conditions. Soc. Sci. Med. 2017, 176, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devisch, I. Ziek van Gezondheid; De Bezige Bij: Gent, Belgium, 2013. [Google Scholar]
- Mak, W.W.S.; Cheung, R.Y.M.; Law, R.W.; Woo, J.; Li, P.C.K.; Chung, R.W.Y. Examining attribution model of self-stigma on social support and psychological well-being among people with HIV+/AIDS. Soc. Sci. Med. 2007, 64, 1549–1559. [Google Scholar] [CrossRef] [PubMed]
- Turan, J.M.; Elafros, M.A.; Logie, C.H.; Banik, S.; Turan, B.; Crockett, K.B.; Pescosolido, B.; Murray, S.M. Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Med. 2019, 17, 7. [Google Scholar] [CrossRef] [Green Version]
- Peacock, M.; Bissell, P.; Owen, J. Shaming Encounters: Reflections on Contemporary Understandings of Social Inequality and Health. Sociology 2014, 48, 387–402. [Google Scholar] [CrossRef]
- Lopdrup-Hjort, T.; Gudman-Hoyer, M.; Bramming, P.; Pedersen, M. Editorial: Governing work though self-management. Ephemer. Theory Polit. Organ. 2011, 11, 97–104. Available online: www.ephemeraweb.org (accessed on 28 January 2021).
- Svensson, T.; Müssener, U.; Alexandersson, K. Pride, empowerment and return to work: On the significance of positive social emotions in the rehabilitation of sickness absentees. Work 2006, 27, 57–65. [Google Scholar]
- Allen, C.; Vassilev, I.; Kennedy, A.; Rogers, A. Long-Term Condition Self-Management Support in Online Communities: A Meta-Synthesis of Qualitative Papers. J. Med. Internet Res. 2016, 18, e5260. [Google Scholar] [CrossRef]
- Karim, F.; Oyewande, A.; Abdalla, L.F.; Ehsanullah, R.C.; Khan, S. Social Media Use and Its Connection to Mental Health: A Systematic Review. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Daker-White, G.; Rogers, A. What is the potential for social networks and support to enhance future telehealth interventions for people with a diagnosis of schizophrenia: A critical interpretive synthesis. BMC Psychiatry 2013, 13, 279. [Google Scholar] [CrossRef] [Green Version]
- Allen, C.; Vassilev, I.; Kennedy, A.; Rogers, A. The work and relatedness of ties mediated online in supporting long-term condition self-management. Sociol. Health Illn. 2020, 42, 579–595. [Google Scholar] [CrossRef]
- Lee, K.; Hoti, K.; Hughes, J.D.; Emmerton, L.M. Consumer use of ‘Dr Google’: A survey on health information-seeking behaviors and navigational needs. J. Med. Internet Res. 2015, 17, e288. [Google Scholar] [CrossRef]
- Ebeling, M.F.E. Patient disempowerment through the commercial access to digital health records. Health 2019, 23, 385–400. [Google Scholar] [CrossRef]
- Nundy, S.; Patel, K.K.; Sendak, M. Accelerating Digital Health to Achieve Equitable Delivery of the COVID-19 Vaccine. Health Aff. Blogs 2021. [Google Scholar] [CrossRef]
- Weiner, J.P. Doctor-patient communication in the e-health era. Isr. J. Health Policy Res. 2012, 1, 33. [Google Scholar] [CrossRef] [Green Version]
- Parish, M.N.; Fazio, S.; Chan, S.; Yellowlees, P.M. Managing Psychiatrist-Patient Relationships in the Digital Age: A Summary Review of the Impact of Technology-Enabled Care on Clinical Processes and Rapport. Curr. Psychiatry Rep. 2017, 19. [Google Scholar] [CrossRef]
- Malone, M.; Mathes, L.; Dooley, J.; While, A.E. Health information seeking and its effect on the doctor-patient digital divide. J. Telemed. Telecare 2005, 11, 25–28. [Google Scholar] [CrossRef]
- Kerr, C.; Murray, E.; Noble, L.; Morris, R.; Bottomley, C.; Stevenson, F.; Patterson, D.; Peacock, R.; Turner, I.; Jackson, K.; et al. The Potential of Web-Based Interventions for Heart Disease Self-Management: A Mixed Methods Investigation. J. Med. Internet Res. 2010, 12, 66–80. [Google Scholar] [CrossRef] [PubMed]
- Belliger, A.; Krieger, D.J. The digital transformation of health care. In Knowledge Management in Digital Change; North, K., Maier, R., Haas, O., Eds.; Springer: Cham, Switzerland, 2018; pp. 311–326. [Google Scholar]
- Morgan, H. ‘Pushed’ self-tracking using digital technologies for chronic health condition management: A critical interpretive synthesis. Digit. Health 2016, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korteweg, L. Huisartsenzorg 2030: Van praktijk naar platform? Huisarts Wet. 2020, 63, 65–66. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Olmen, J. The Promise of Digital Self-Management: A Reflection about the Effects of Patient-Targeted e-Health Tools on Self-Management and Wellbeing. Int. J. Environ. Res. Public Health 2022, 19, 1360. https://doi.org/10.3390/ijerph19031360
van Olmen J. The Promise of Digital Self-Management: A Reflection about the Effects of Patient-Targeted e-Health Tools on Self-Management and Wellbeing. International Journal of Environmental Research and Public Health. 2022; 19(3):1360. https://doi.org/10.3390/ijerph19031360
Chicago/Turabian Stylevan Olmen, Josefien. 2022. "The Promise of Digital Self-Management: A Reflection about the Effects of Patient-Targeted e-Health Tools on Self-Management and Wellbeing" International Journal of Environmental Research and Public Health 19, no. 3: 1360. https://doi.org/10.3390/ijerph19031360
APA Stylevan Olmen, J. (2022). The Promise of Digital Self-Management: A Reflection about the Effects of Patient-Targeted e-Health Tools on Self-Management and Wellbeing. International Journal of Environmental Research and Public Health, 19(3), 1360. https://doi.org/10.3390/ijerph19031360