
The Assessment of Prolonged Inferior Alveolar Nerve Blockade for Postoperative Analgesia in Mandibular Third Molar Surgery by a Perineural Addition of Dexamethasone to 0.5% Ropivacaine: A Randomized Comparison Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Selection
2.1.1. Study Design
2.1.2. Exclusion Criteria
2.2. Techniques of Injections of Local Anesthetics and Dexamethasone
2.3. Wisdom Tooth Surgery
2.4. Summary of Anesthesia and Analgesia Parameters with Defined Outcomes
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
Strengths and Weaknesses of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenquist, J.B.; Nystrom, E. Long-Acting Analgesic or Long-Acting Local Anesthetic in Controlling Immediate Postoperative Pain After Lower Third Molar Surgery. Anesth. Prog. 1987, 34, 6–9. [Google Scholar] [PubMed]
- Shepherd, J.P.; Brickley, M. Surgical removal of third molars. BMJ 1994, 309, 620–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, R.D.; Cohen, B.H. Perioperative pain control. Oral Maxillofac. Surg. Clin. N. Am. 1992, 4, 663–664. [Google Scholar] [CrossRef]
- Fisher, S.E.; Frame, J.W.; Rout, P.G.J.; McEntegart, D.J. Factors affecting the onset and severity of pain following the surgical removal of unilateral impacted mandibular third molar teeth. Br. Dent. J. 1988, 164, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Falci, S.G.M.; Lima, T.C.; Martins, C.C.; dos Santos, C.R.R.; Pinheiro, M.L.P. Preemptive Effect of Dexamethasone in Third-Molar Surgery: A Meta-Analysis. Anesth. Prog. 2017, 64, 136–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjørnsson, G.A.; Haanaes, H.R.; Skoglund, L.A. Ketoprofen 75 mg qid versus acetaminophen 1000 mg qid for 3 days on swelling, pain, and other postoperative events after third-molar surgery. J. Clin. Pharm. 2003, 43, 305–314. [Google Scholar] [CrossRef]
- Mozzati, M.; Gallesio, G.; Russo, A.; Staiti, G.; Mortellaro, C. Third-molar extraction with ultrasound bone surgery: A case-control study. J. Craniofac. Surg. 2014, 25, 856–859. [Google Scholar] [CrossRef]
- Seymour, R.A.; Meechan, J.G.; Blair, G.S. An investigation into post-operative pain after third molar surgery under local analgesia. Br. J. Oral Maxillofac. Surg. 1985, 23, 410–418. [Google Scholar] [CrossRef]
- Burić, N. Ropivacaine as local anesthetic in the surgery of maxillary sinus. Acta Stomatol. Naissi 2003, 19, 167–171. [Google Scholar]
- Buric, N. The assesment of anesthetic efficiacy of ropivacaine in oral surgery. N. Y. State Dent. J. 2006, 72, 36–39. [Google Scholar]
- Tijanic, M.; Buric, N. A randomized anesthethic potency comparison between ropivacaine and bupivacaine on the perioperative regional anesthesia in lower third molar surgery. J. Craniomaxillofac. Surg. 2019, 47, 1652–1660. [Google Scholar] [CrossRef]
- McClellan, K.J.; Faulds, D. Ropivacaine: An update of its use in regional anaesthesia. Drugs 2000, 60, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, J.B.; Wildsmith, J.A.W. Developments in local anaesthesia drugs. Br. J. Anaesth. 2001, 87, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasta, J. Local Anesthetics: Evolving to a New Standard of Care. Pharmacy Practice News. 2013. Available online: http://www.pharmacypracticenews.com/download/SR132_WM.pdf (accessed on 20 January 2022).
- Apfelbaum, J.L.; Chen, C.; Mehta, S.S.; Gan, T.J. Postoperative pain experience: Results from a national survey suggest postoperative pain continues to be undermanaged. Anesth. Analg. 2003, 97, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Polomano, R.C.; Dunwoody, C.J.; Krenzischek, D.A.; Rathmell, J.P. Perspective on pain management in the 21st century. J. Perianesth. Nurs. 2008, 23 (Suppl. S1), S4–S14. [Google Scholar] [CrossRef] [PubMed]
- Covino, B.G.; Vassallo, H.G. Local Anesthetics. Mechanisms of Action and Clinical Use; Grune and Stratton, Inc.: New York, NY, USA, 1976. [Google Scholar]
- Kumar, S.; Palaria, U.; Sinha, A.K.; Punera, D.C.; Pandey, V. Comparative evaluation of ropivacaine and ropivacaine with dexamethasone in supraclavicular brachial plexus block for postoperative analgesia. Anesth. Essays Res. 2014, 8, 202–208. [Google Scholar] [PubMed] [Green Version]
- Møiniche, S.; Jørgensen, H.; Wetterslev, J.; Dahl, J.B. Local Anesthetic Infiltration for Postoperative Pain Relief After Laparoscopy: A Qualitative and Quantitative Systematic Review of Intraperitoneal, Port-Site Infiltration and Mesosalpinx Block. Anesth. Analg. 2000, 90, 899–912. [Google Scholar] [CrossRef]
- Kanazi, G.E.; Aouad, M.T.; Jabbour-Khoury, S.I.; Al Jazzar, M.D.; Alameddine, M.M.; Al-Yaman, R.; Bulbul, M.; Baraka, A.S. Effect of lowdose dexmedetomidine or clonidine on the characteristics of bupivacaine spinal block. Acta Anaesthesiol. Scand. 2006, 50, 222–227. [Google Scholar] [CrossRef]
- Culebras, X.; Van Gessel, E.; Hoffmeyer, P.; Gamulin, Z. Clonidine combined with a long acting local anesthetic does not prolong postoperative analgesia after brachial plexus block but does induce hemodynamic changes. Anesth. Analg. 2001, 92, 199–204. [Google Scholar] [CrossRef]
- Atalay, B.; Onur, O.D. Analgesic and Anti-Inflammatory Effects of Articaine and Perineural Dexamethasone for Mandibular Third Molar Surgery: A Randomized, Double-Blind Study. J. Oral Maxillofac. Surg. 2020, 78, 507–514. [Google Scholar] [CrossRef]
- de Beer, D.A.; Thomas, M.L. Caudal additives in children—Solutions or problems? Br. J. Anaesth. 2003, 90, 487–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansermino, M.; Basu, R.; Vandebeek, C.; Montgomery, C. Nonopioid additives to local anaesthetics for caudal blockade in children: Asystematic review. Paediatr. Anaesth. 2003, 13, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Engelman, E.; Marsala, C. Bayesian enhanced meta-analysis of postoperativeanalgesic efficacyof additives for caudal analgesia in children. Acta Anaesthesiol. Scand. 2012, 56, 817–832. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.O.; Kim, W.K.; Kong, M.H.; Lee, M.K.; Kim, N.S.; Choi, Y.S.; Lim, S.H. No enhancement of sensory and motor blockade by ketamine added to ropivacaine interscalene brachial plexus blockade. Acta Anaesthesiol. Scand. 2002, 46, 821–826. [Google Scholar] [CrossRef]
- Bazin, J.E.; Massoni, C.; Bruelle, P.; Fenies, V.; Groslier, D.; Schoeffler, P. The addition of opioids to local anaesthetics in brachial plexus block: The comparative effects of morphine, buprenorphine and sufentanil. Anaesthesia 1997, 52, 858–862. [Google Scholar] [CrossRef]
- Holte, K.; Werner, U.M.; Lacouture, P.G.; Kehlet, H. Dexamethasone Prolongs Local Analgesia after Subcutaneous Infiltration of Bupivacaine Microcapsules in Human Volunteers. Anesthesiology 2002, 96, 1331–1335. [Google Scholar] [CrossRef] [Green Version]
- Moss, R.; Pfister, J.I.; Kneedler, A.J. Infiltration of Local Anesthetics for Postoperative Analgesia; Pfiedler Enterprises: Aurora, CO, USA, 2015. [Google Scholar]
- De Oliveira, G.S., Jr.; Almeida, M.D.; Benzon, H.T.; Mc Carthy, R.J. Perioperative single dose systemic dexamethasone for postoperative pain: A meta-analysis of randomized controlled trials. Anesthesiology 2011, 115, 575–588. [Google Scholar] [CrossRef] [Green Version]
- Waldron, N.H.; Jones, C.A.; Gan, T.J.; Allen, T.K.; Habib, A.S. Impact of perioperative dexamethasone on postoperative analgesia and sideeffects: Systematic review and meta-analysis. Br. J. Anaesth. 2013, 110, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Aasboe, V.; Raeder, J.C.; Groegaard, B. Betamethasone reduces postoperative pain and nausea after ambulatory surgery. Anesth. Analg. 1998, 87, 913–917. [Google Scholar] [CrossRef]
- Baxendale, B.R.; Vater, M.; Lavery, K.M. Dexamethasone reduces pain and swelling following extraction of third molar teeth. Anaesthesia 1993, 48, 961–964. [Google Scholar] [CrossRef]
- Greaves, M.W. Anti-inflammatory action of corticosteroids. Postgrad. Med. J. 1976, 52, 631–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parrington, S.J.; O’Donnell, D.; Chan, V.W.; Brown-Shreves, D.; Subramanyam, R.; Qu, M.; Brull, R. Dexamethasone added to mepivacaine prolongs the duration of analgesia after supraclavicular brachial plexus blockade. Reg. Anesth. Pain Med. 2010, 35, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Cummings, K.C., 3rd; Napierkowski, D.E.; Parra-Sanchez, I.; Kurz, A.; Dalton, J.E.; Brems, J.J.; Sessler, D.I. Effect of dexamethasone on the duration of interscalene nerve blocks with ropivacaine or bupivacaine. Br. J. Anaesth. 2011, 107, 446–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.; Rodseth, R.; McCartney, C.J. Effects of dexamethasone as a local anaesthetic adjuvant for brachial plexus block: A systematic review and meta-analysis of randomized trials. Br. J. Anaesth. 2014, 112, 427–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, A. Decadron phosphate in the relief of complaints after third molar surgery: A double-blind, controlled trial with bilateral oral surgery. Int. J. Oral Surg. 1985, 14, 235. [Google Scholar] [CrossRef]
- Williams, B.A.; Hough, K.A.; Tsui, B.Y.; Ibinson, J.W.; Gold, M.S.; Gebhart, G.F. Neurotoxicity of adjuvants used in perineural anesthesia and analgesia in comparison with ropivacaine. Reg. Anesth. Pain Med. 2011, 36, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Ma, R.; Wang, X.; Lu, C.; Li, C.; Cheng, Y.; Ding, G.; Liu, L.; Ding, Z. Dexamethasone attenuated bupivacaine-induced neuron injury in vitro through a threonineserine protein kinase B-dependent mechanism. Neuroscience 2010, 167, 329–342. [Google Scholar] [CrossRef]
- Graziani, F.; D’Aiuto, F.; Arduino, P.G.; Tonelli, M.; Gabriele, M. Perioperative dexamethasone reduces post-surgical sequelae of wisdom tooth removal. A split-mouth randomized double-masked clinical trial. Int. J. Oral Maxillofac. Surg. 2006, 35, 241–246. [Google Scholar] [CrossRef]
- Mico-Llorens, J.M.; Satorres-Nieto, M.; Gargallo-Albiol, A.; Arnabat- Domınguez, J.; Berini-Aytes, L.; Gay-Escoda, C. Efficacy of methylprednisolone in controlling complications after impacted lower third molar surgical extraction. Eur. J. Clin. Pharmacol. 2006, 62, 693–698. [Google Scholar] [CrossRef]
- Grossi, G.B.; Maiorana, C.; Garramone, R.A.; Borgonovo, A.; Beretta, M.; Farronato, D.; Santoro, F. Effect of submucosal injection of dexamethasone on postoperative discomfort after third molar surgery: A prospective study. J. Oral Maxillofac. Surg. 2007, 65, 2218–2226. [Google Scholar] [CrossRef]
- Vegas-Bustamante, E.; Micó-Llorens, J.; Gargallo-Albiol, J.; Satorres-Nieto, M.; Berini-Aytes, L.M.; Gay-Escoda, C. Efficacy of methylprednisolone injected into the masseter muscle following the surgical extraction of impacted lower third molars. Int. J. Oral Maxillofac. Surg. 2008, 37, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Gow-Gates, G.A.E. Mandibular conduction anesthesia: A new technique using extraoral landmarks. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 321–328. [Google Scholar] [CrossRef]
- Sisk, A.L. Evaluation of the Akinosi mandibular block technique in oral surgery. J. Oral Maxillofac. Surg. 1986, 44, 113–115. [Google Scholar] [CrossRef]
- Fauel, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statsiscal power analysis programm for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Downie, W.W.; Leatham, P.A.; Rhind, V.M.; Wright, V.; Branco, J.A.; Anderson, J.A. Studies with pain rating scales. Ann. Rheum. Dis. 1978, 37, 378–381. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, S.A. Pain measurement tools for clinical practice and research. AANA J. 1996, 64, 133–140. [Google Scholar]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Tijanić, M.; Burić, K.; Stojanović, S.; Burić, N. Assessment of conduction anesthesia effectiveness using the angulated needle approach for the inferior alveolar nerve block. J. Cranio-Maxillofac. Surg. 2020, 48, 607–615. [Google Scholar] [CrossRef]
- Breivik, E.K.; Björnsson, G.A.; Skovlund, E. A comparison of pain rating scales by sampling from clinical trial data. Clin. J. Pain 2000, 16, 22–28. [Google Scholar] [CrossRef]
- Shrestha, B.R.; Maharjan, K.; Tabedar, S. Supraclavicular brachial plexus block with and without dexamethasone—A comparative study. Randomized Control. Trial. Kathmandu Univ. Med. J. (KUMJ) 2003, 1, 158–160. [Google Scholar]
- Gersema, L.; Baker, K. Use of corticosteroids in oral surgery. J. Oral Maxillofac. Surg. 1992, 50, 270–277. [Google Scholar] [CrossRef]
- Montgomery, M.T.; Hogg, J.P.; Roberts, D.L.; Redding, S.W. The use of glucocorticosteroids to lessen the inflammatory sequelae following third molar surgery. J. Oral Maxillofac. Surg. 1990, 48, 179–187. [Google Scholar] [CrossRef]
- Ustun, Y.; Erdogan, O.; Esen, E.; Karsli, E.D. Comparison of the effects of 2 doses of methylprednisolone on pain, swelling, and trismus after third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2003, 96, 535–539. [Google Scholar] [CrossRef]
- Becker, D.E.; Reed, K.L. Local Anesthetics: Review of Pharmacological Considerations. Anesth. Prog. 2012, 59, 90–102. [Google Scholar] [CrossRef] [Green Version]
- Casati, A.; Fanelli, G.; Aldegheri, G.; Berti, M.; Colnaghi, E.; Cedrati, V.; Torri, G. Interscalene brachial plexus anesthesia with 0.5%, 0.75% or 1% ropivacaine: Double—Blind comparison with 2% mepivacaine. Br. J. Anaest. 1999, 83, 872–875. [Google Scholar] [CrossRef]
- Akerman, B.; Hellbetg, I.B.; Trossvik, C. Primary evaluation of the local anesthetics properties of the amino amide agent ropivacaine (lea 103). Acta Anaesthesiol. Scand. 1988, 32, 571–578. [Google Scholar] [CrossRef]
- Liisanantti, O.; Luukkonen, J.; Rosenberg, P.H. High-dose bupivacaine, levobupivacaine and ropivacaine in axillary brachial plexus block. Acta Anaesthesiol. Scand. 2010, 48, 601–606. [Google Scholar] [CrossRef]
- Kuthiala, G.; Chaudhary, G. Ropivacaine: A review of its pharmacology and clinical use. Indian J. Anaesth 2011, 55, 104–110. [Google Scholar] [CrossRef]
- Messer, E.J.; Keller, J.J. The use of intraoral dexamethasone after extraction of mandibular third molars. Oral Surg. Oral Med. Oral Pathol. 1975, 40, 594–598. [Google Scholar] [CrossRef]
- Beirne, O.R.; Hollander, B. The effect of methylprednisolone on pain, trismus, and swelling after removal of third molars. Oral Surg. Oral Med. Oral Pathol. 1986, 61, 134–138. [Google Scholar] [CrossRef]
- Hargreaves, K.M.; Schmidt, E.A.; Mueller, G.P.; Dionne, R.A. Dexamethasone alters plasma levels of beta-endorphin and postoperative pain. Clin. Pharm. Ther. 1987, 42, 601–607. [Google Scholar] [CrossRef] [PubMed]
- McCormack, K. The spinal actions of nonsteroidal anti-inflammatory drugs and the dissociation between their anti-inflammatory and analgesic effects. Drugs 1994, 47, 28–45. [Google Scholar] [CrossRef] [PubMed]
- Ahlgren, S.C.; Wang, J.F.; Levine, J.D. C-fiber mechanical stimulus response functions are different in inflammatory versus neuropathic hyperalgesia in the rat. Neuroscience 1997, 76, 285–290. [Google Scholar] [CrossRef]
- Honorio, T.B. Epidural Steroids. In Pain Medicine, a Comprehensive Review; Raj, P.P., Ed.; Mosby Publications: St.Louis, MI, USA, 1999; pp. 259–263. [Google Scholar]
- Attardi, B.; Takimoto, K.; Gealy, R. Glucocorticoid induced upregulation of a pituitary K+ channel mRNA in vitro and in vivo. Recept. Channels 1993, 1, 287–293. [Google Scholar] [PubMed]
- Zhang, G.; Liu, Y.; Ruoho, A.E.; Hurley, J.H. Structure of the adenylyl cyclase catalytic core. Nature 1997, 386, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Goppelt-Struebe, M.; Wolter, D.; Resch, K. Glucocorticoids inhibit prostaglandin synthesis not only at the level of phospholipase A2 but also at the level of cyclo-oxygenase/PGE isomerase. Br. J. Pharmacol. 1989, 98, 1287–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, P.H.; Liu, K.; Peng, C.H.; Yang, L.C.; Lin, C.R.; Lu, C.Y. The effect of dexamethasone on postoperative pain and emesis after intrathecal neostigmine. Anesth. Analg. 2001, 92, 228–232. [Google Scholar] [CrossRef]
- Splinter, W.M.; Rhine, E.J. Low-dose ondansetrone with dexamethasone more effectively decreases vomiting after strabismus surgery in children than does high-dose ondansetron. Anesthesiology 1998, 88, 72–75. [Google Scholar] [CrossRef]
- Pathak, R.G.; Anand, P.S.; Rajendra, N.K. Supraclavicular brachial plexus block with and without Dexamethasone—A Comparative Study. Int. J. Sci. Res. Publ. 2012, 12, 1–7. [Google Scholar]
- Neal, J.M.; Rathmell, J.P.; Rowlingson, J.C. Publishing studies that involve ‘Off-label’ use of drugs: Formalizing regional anesthesia and pain medicine’s policy. Reg. Anesth. Pain Med. 2009, 34, 391–392. [Google Scholar] [CrossRef]
- Benzon, H.T.; Gissen, A.J.; Strichartz, G.R.; Avram, M.J.; Covino, B.G. The effect of polyethylene glycol on mammalian nerve impulses. Anesth. Analg. 1987, 66, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Majid, O.W.; Mahmood, W.K. Use of dexamethasone to minimise post-operative sequelae after third molar surgery: Comparison of five different routes of administration. Oral Surg. 2013, 6, 200–208. [Google Scholar] [CrossRef]
- Brković, B.; Andrić, M.; Ćalasan, D.; Milić, M.; Stepić, J.; Vučetić, M.; Brajković, D.; Todorović, T. Efficacy and safety of 1% ropivacaine for postoperative analgesia after lower third molar surgery: A prospective, randomized, double-blinded clinical study. Clin. Oral Investig. 2017, 21, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, D.; Sreekumar, K.; Deshpande, A. Effects of intra-space injection of Twin mix versus intraoral-submucosal, intramuscular, intravenous and per-oral administration of dexamethasone on post-operative sequelae after mandibular impacted third molar surgery: A preliminary clinical comparative study. Oral Maxillofac. Surg. 2014, 18, 293–296. [Google Scholar] [PubMed]
- Kaufman, E.; Goharian, S.; Katz, Y. Adverse Reactions Triggered by Dental Local Anesthetics: A Clinical Survey. Anesth. Prog. 2000, 47, 134–138. [Google Scholar] [PubMed]
- Robertson, W.D. Clinical evaluation of mandibular conduction anesthesia. Gen. Dent. 1979, 27, 49–51. [Google Scholar]
- Donkor, P.; Wong, J.; Punnia-Moorthy, A. An evaluation of the closed mouth mandibular block technigue. Int. J. Oral Maxillofac. Surg. 1990, 19, 216–219. [Google Scholar] [CrossRef]
- Watson, J.E.; Gow-Gates, G.A. Incidence of positive aspiration of the Gow-Gates mandibular block technigue. Anesth. Pain Control. Dent. 1992, 1, 73–76. [Google Scholar]
- Todorović, L.J.; Stajčić, Z.; Petrović, V. Mandibular versus inferior dental anesthesia: Clinical asessment of three different techniques. Int. J. Oral Maxillofac. Surg. 1986, 15, 733–738. [Google Scholar] [CrossRef]
- Simpson, D.; Curran, M.P.; Oldfield, V.; Keating, G.M. Ropivacaine: A review of its use in regional anaesthesia and acute pain management. Drugs 2005, 65, 2675–2717. [Google Scholar] [CrossRef]
- Li, M.; Li, W.; Mei, W.; Tian, Y. Update on the clinical utility and practical use of ropivacaine in Chinese patients. Drug Des. Dev. Ther. 2014, 8, 1269–1276. [Google Scholar]
- Fresenius Kabi: Naropin®(ropivacaine HCl) Injection. 2018. Available online: http://editor.fresenius-kabi.us/PIs/US-PH-Naropin_FK-451112K_Jun_2020-PI.pdf (accessed on 15 November 2021).
- Nickel, A.A., Jr. A retrospective study of parasthesia of the dental alveolar nerves. Anesth. Prog. 1990, 37, 42–45. [Google Scholar] [PubMed]
- Garisto, G.A.; Gaffen, A.S.; Lawrence, H.P.; Tenenbaum, H.C.; Haas, D.A. Occurrence of paresthesia after dental local anesthetic administration in the United States. J. Am. Dent. Assoc. 2010, 141, 836–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, D.A.; Lennon, D. A 21 year retrospective study of reports of paresthesia following local anesthetic administration. J. Can. Dent. Assoc. 1995, 61, 319–330. [Google Scholar]
- Hopman, A.J.; Baart, J.A.; Brand, H.S. Articaine and neurotoxicity: A review. Br. Dent. J. 2017, 223, 501–506. [Google Scholar] [CrossRef]
- Seddon, H.I. Three types of nerve injury. Brain 1943, 66, 237–288. [Google Scholar] [CrossRef]
- Smith, M.H.; Lung, K.E. Nerve injuries after dental injection: A review of the literature. J. Can. Dent. Assoc. 2006, 72, 559–564. [Google Scholar]
- Stojanović, S. Analysis of efficacy of adding dexamethasone to ropivacaine in oral surgery. Acta Stomatol. Naissi 2017, 33, 1754–1762. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Rop + Dex (Group I) N = 15 | Rop (Group II) N = 15 | Bup (Group III) N = 15 | ||||
|---|---|---|---|---|---|---|
| Age | 29.07 ± 7.40 | 24.53 ± 6.22 | 27.58 ± 10.32 | |||
| 95% CI of mean age | 24.97–33.16 | 21.09–27.98 | 21.86–33.29 | |||
| Sex | ||||||
| Male | 7 | 46.7 (%) | 3 | 20.0 (%) | 5 | 33.3 (%) |
| Female | 8 | 53.3 (%) | 12 | 80.0 (%) | 10 | 66.7 (%) |
| Ropivacaine + Dex N = 15 | Ropivacaine N = 15 | Bupivacaine N = 15 | p1 Values | |
|---|---|---|---|---|
| Primary local anesthesia outcomes | ||||
| Duration of anesthesia (min) | 549.73 ± 224.56 b | 277.0 ± 61.52 | 316.47 ± 151.88 a | 0.001 |
| Secondary local anesthesia outcomes | ||||
| Onset time of anesthesia (min) | 4.13 ± 1.30 | 5.40 ± 2.10 | 4.47 ± 1.46 | 0.289 |
| Success of local anesthesia in absolute terms #/%, with additional anesthesia #/% | 14 (93.4%) 1 (6.66%) | 10 (66.7%) 5 (33.33%) | 9 (60%) 6 (40%) | 0.034 2 |
| Amount of anesthesia per patient (mL) | 4.13 | 4.66 | 4.8 | 0.097 |
| The # of patients used analgesics #/% | 10 (66.7%) | 15 (100%/0%) | 13 (86.7%) | 0.052 |
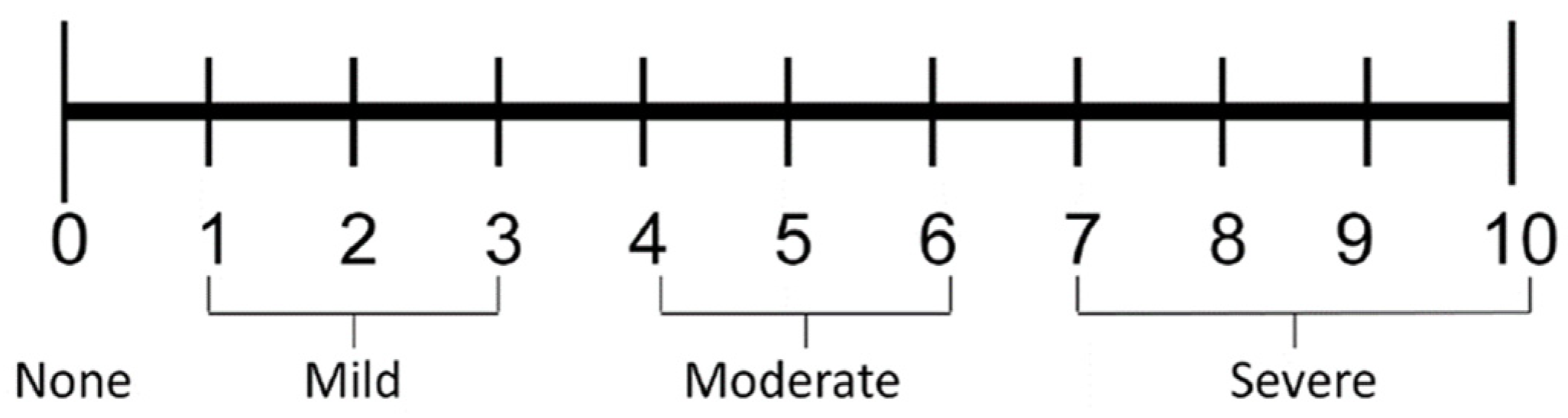
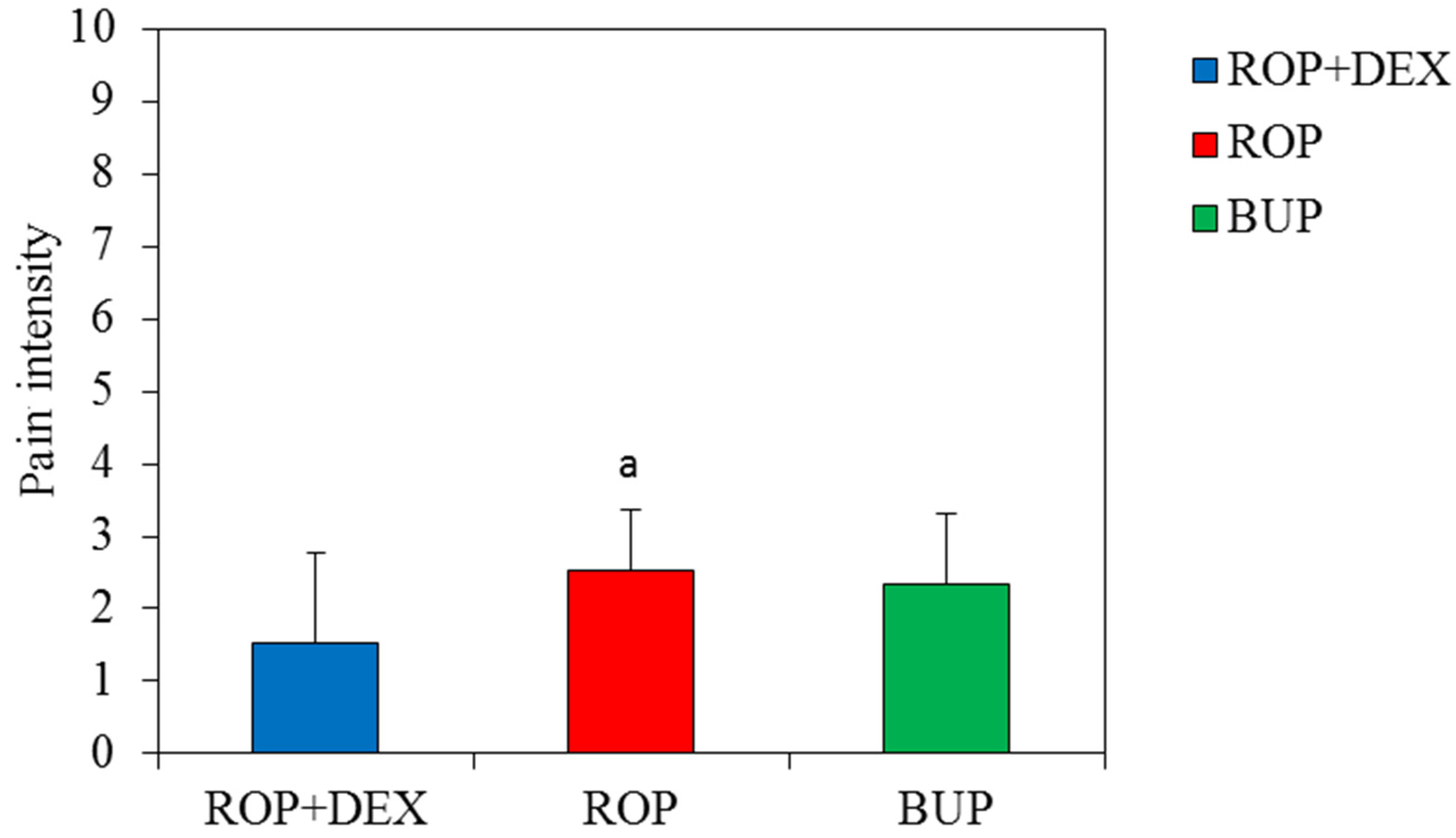
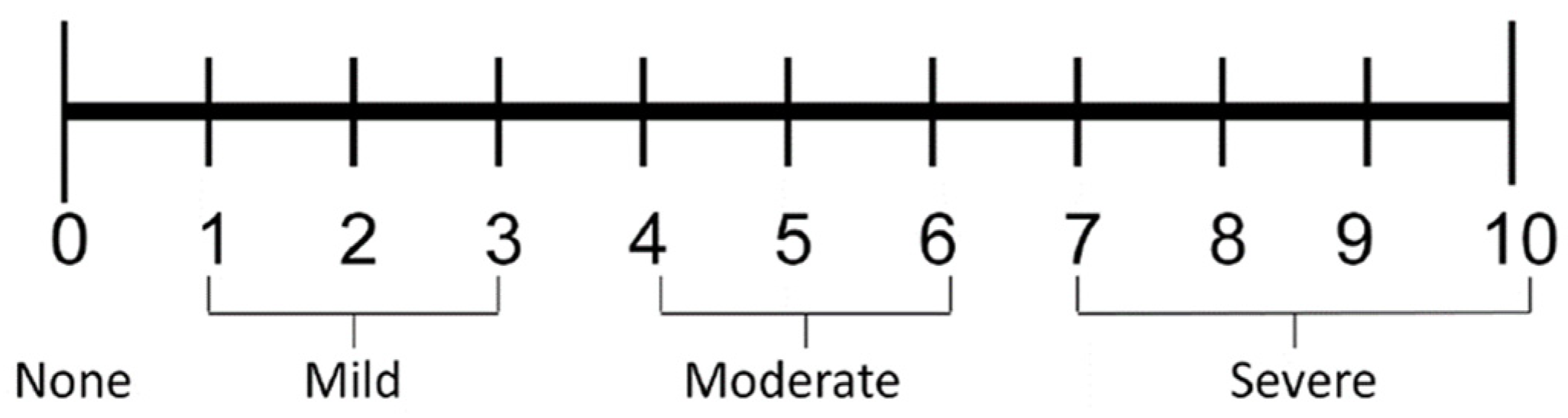
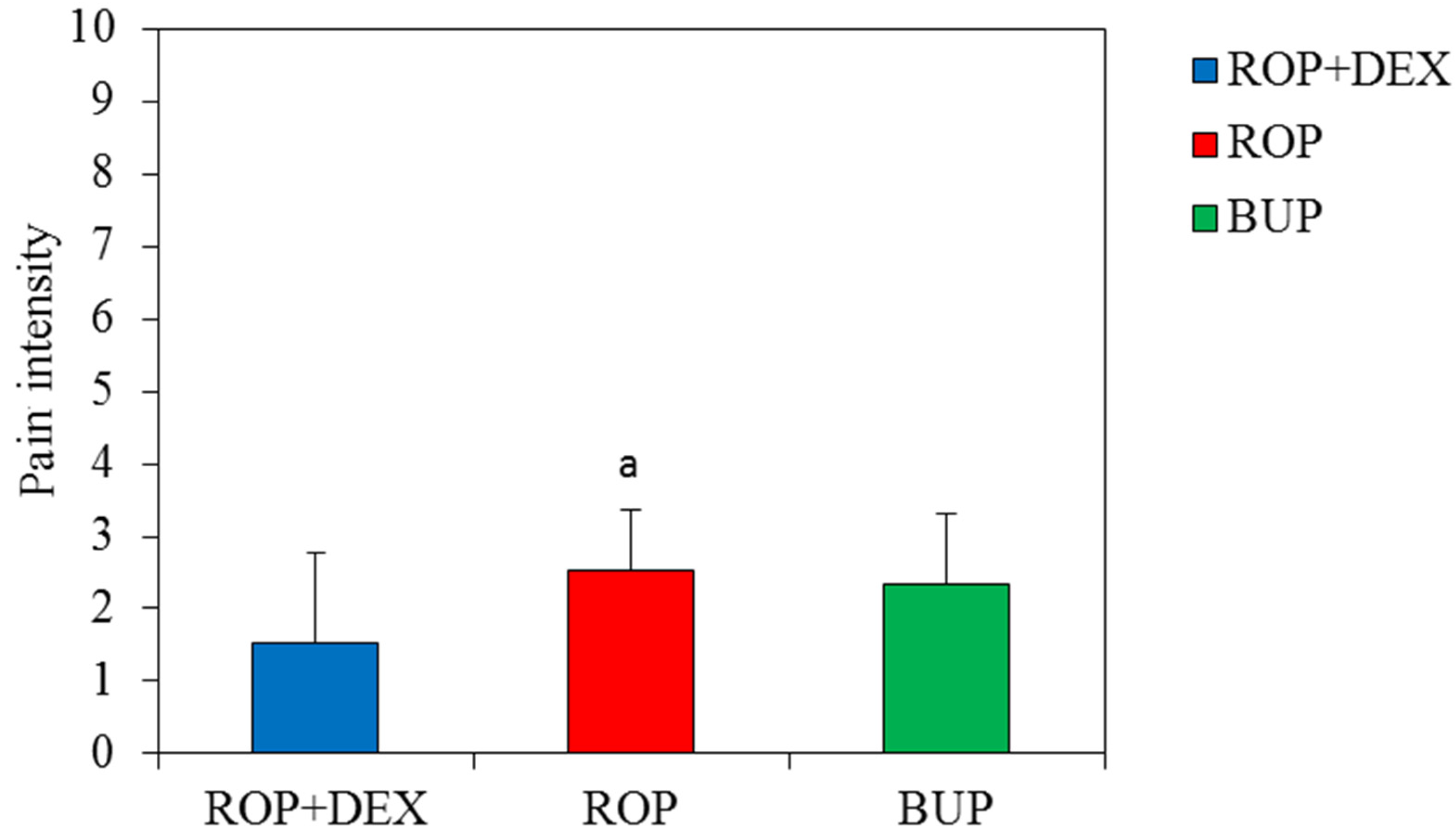
| NRS of pain when the first anlgesics used | 3.70 ± 0.68 | 4.93 ± 0.96 | 4.50 ± 0.76 | 0.004 |
| Duration of analgesia when analgesics used for the first time (min) | 654.9 ± 198.4 b | 345.4 ± 88.0 | 413.7 ± 152.3 | 0.001 |
| # of analgesics during 24 h postoeratively | 1.90 ± 0.57 b | 2.80 ± 0.86 | 2.36 ± 0.84 | 0.027 |
| Dizziness #/% | 1 (2.22%) | 0 (0.0%) | 1 (2.22%) | 1.000 3 |
| Drowiness #/% | 0 (0.0%) | 0 (0.0%) | 1 (2.22%) | 1.000 3 |
| Haematoma #/% | 0 (0.0%) | 1 (2.22%) | 1 (2.22%) | 1.000 3 |
| Positive aspiration #/% | 1 (2.22%) | 0 (0.0%) | 0 (0.0%) | 1.000 3 |
| Transient paresthesia of n.lingualis #/% | 0 (0.0%) | 0 (0.0%) | 1 (2.22%) | 1.000 3 |
| Administered Local Anesthesia Solutions | Achieved Mark | Mean Quality of Achieved Anesthesia | p Value 1 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |||
| GROUP I 0.5% Ropivacaine and 4 mg Dex | 9 | 5 | 1 | 0 | 0 | 0 | 0 | 0 | 1.47 ± 0.38 | 0.037 |
| GROUP II Plain 0.5% Ropivacaine | 3 | 7 | 2 | 2 | 1 | 0 | 0 | 0 | 2.40 ± 1.31 a | |
| GROUP III 0.5% Bupivacaine | 4 | 5 | 4 | 2 | 0 | 0 | 0 | 0 | 2.27 ± 1.00 a | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojanović, S.; Burić, N.; Tijanić, M.; Todorović, K.; Burić, K.; Burić, N.; Jovanović, M.; Bajagić, V. The Assessment of Prolonged Inferior Alveolar Nerve Blockade for Postoperative Analgesia in Mandibular Third Molar Surgery by a Perineural Addition of Dexamethasone to 0.5% Ropivacaine: A Randomized Comparison Study. Int. J. Environ. Res. Public Health 2022, 19, 1324. https://doi.org/10.3390/ijerph19031324
Stojanović S, Burić N, Tijanić M, Todorović K, Burić K, Burić N, Jovanović M, Bajagić V. The Assessment of Prolonged Inferior Alveolar Nerve Blockade for Postoperative Analgesia in Mandibular Third Molar Surgery by a Perineural Addition of Dexamethasone to 0.5% Ropivacaine: A Randomized Comparison Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1324. https://doi.org/10.3390/ijerph19031324
Chicago/Turabian StyleStojanović, Simona, Nikola Burić, Milos Tijanić, Kosta Todorović, Kristina Burić, Nina Burić, Marija Jovanović, and Vukadin Bajagić. 2022. "The Assessment of Prolonged Inferior Alveolar Nerve Blockade for Postoperative Analgesia in Mandibular Third Molar Surgery by a Perineural Addition of Dexamethasone to 0.5% Ropivacaine: A Randomized Comparison Study" International Journal of Environmental Research and Public Health 19, no. 3: 1324. https://doi.org/10.3390/ijerph19031324
APA StyleStojanović, S., Burić, N., Tijanić, M., Todorović, K., Burić, K., Burić, N., Jovanović, M., & Bajagić, V. (2022). The Assessment of Prolonged Inferior Alveolar Nerve Blockade for Postoperative Analgesia in Mandibular Third Molar Surgery by a Perineural Addition of Dexamethasone to 0.5% Ropivacaine: A Randomized Comparison Study. International Journal of Environmental Research and Public Health, 19(3), 1324. https://doi.org/10.3390/ijerph19031324