
Effects of Urban Landscape and Sociodemographic Characteristics on Heat-Related Health Using Emergency Medical Service Incidents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Heat-Related Health Data
2.3. Heat Exposure Assessment
2.4. Urban Landscape and Sociodemographic Characteristics
2.5. Statistical Analysis
3. Results
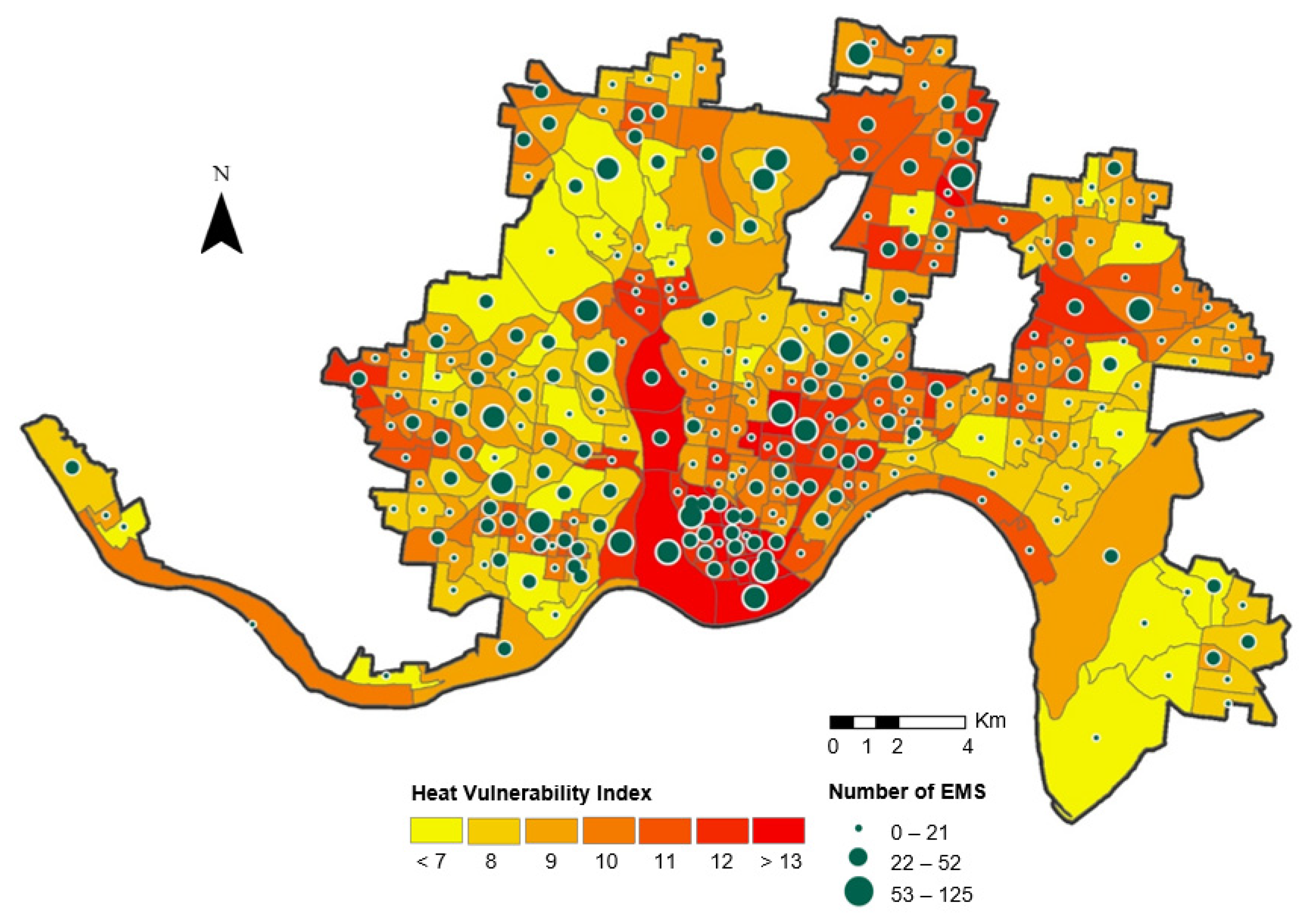
3.1. Summary Statistics for Heat-Related EMS and Neighborhood Characteristics
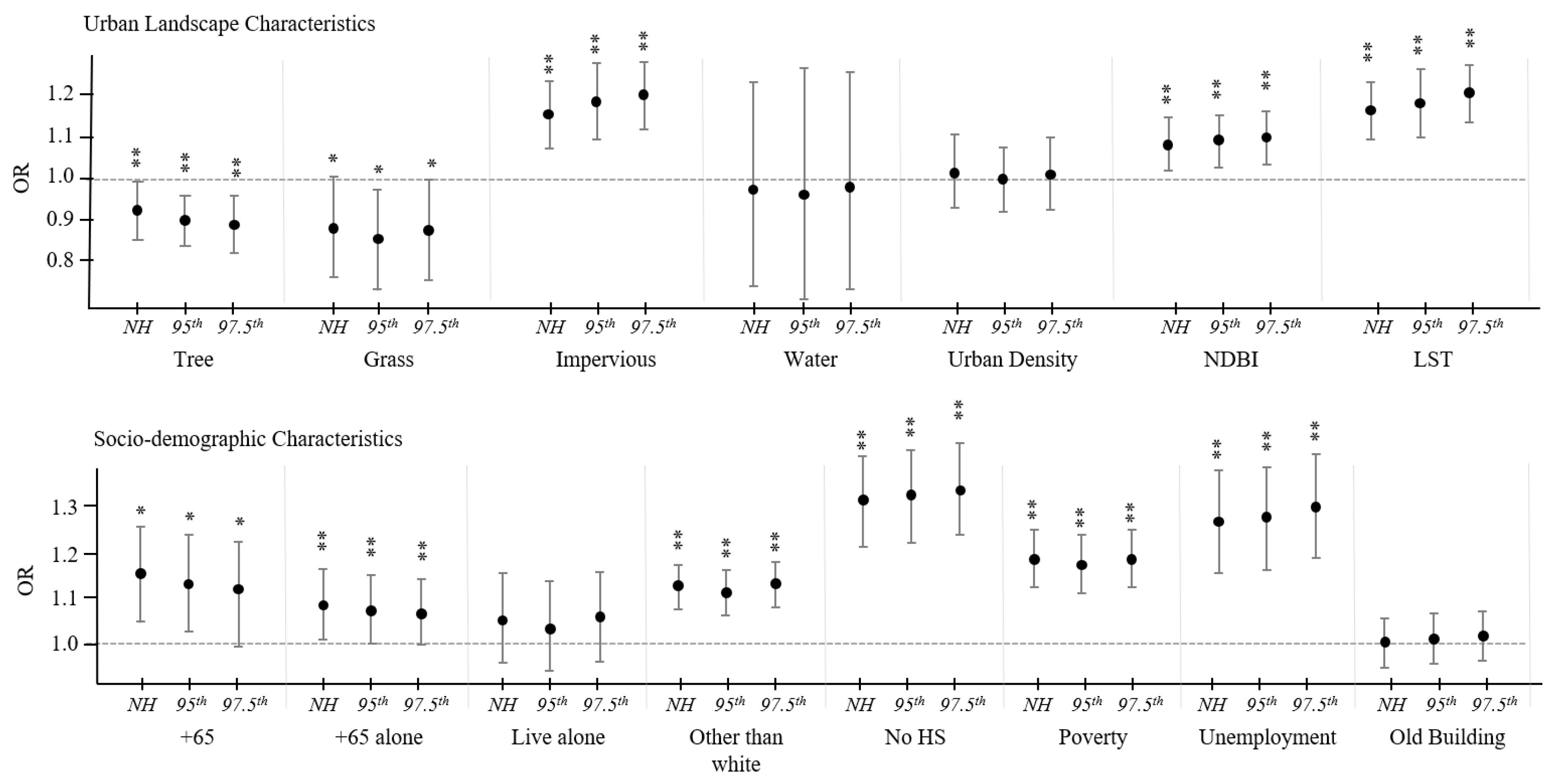
3.2. Neighborhood Effects on Heat-Related EMS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Luber, G.; McGeehin, M. Climate change and extreme heat events. Am. J. Prev. Med. 2008, 35, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.A.; Vanos, J.K.; Kenny, N.A.; Brown, R.D. The relationship between neighbourhood tree canopy cover and heat-related ambulance calls during extreme heat events in Toronto, Canada. Urban For. Urban Green. 2016, 20, 180–186. [Google Scholar] [CrossRef] [Green Version]
- Johnson, B.E.; Shifferd, J. Who lives where: A comprehensive population taxonomy of cities, suburbs, exurbs, and rural areas in the united states. Geogr. Bull. 2016, 57, 25–40. [Google Scholar]
- Dang, T.N.; Van, D.Q.; Kusaka, H.; Seposo, X.T.; Honda, Y. Green Space and Deaths Attributable to the Urban Heat Island Effect in Ho Chi Minh City. Am. J. Public Health 2018, 108, S137–S143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limaye, V.S.; Vargo, J.; Harkey, M.; Holloway, T.; Patz, J.A. Climate Change and Heat-Related Excess Mortality in the Eastern USA. EcoHealth 2018, 15, 485–496. [Google Scholar] [CrossRef]
- Romeo Upperman, C.; Parker, J.; Jiang, C.; He, X.; Murtugudde, R.; Sapkota, A. Frequency of Extreme Heat Event as a Surrogate Exposure Metric for Examining the Human Health Effects of Climate Change. PLoS ONE 2015, 10, e0144202. [Google Scholar] [CrossRef]
- Tan, J.; Zheng, Y.; Tang, X.; Guo, C.; Li, L.; Song, G.; Zhen, X.; Yuan, D.; Kalkstein, A.J.; Li, F.; et al. The urban heat island and its impact on heat waves and human health in Shanghai. Int. J. Biometeorol. 2010, 54, 75–84. [Google Scholar] [CrossRef]
- Vaidyanathan, A.; Malilay, J.; Schramm, P.; Saha, S. Heat-Related Deaths—United States 2004–2018. Morb. Mortal. Wkly. Rep. 2020, 69, 729–734. [Google Scholar] [CrossRef]
- Golden, J.S.; Hartz, D.; Brazel, A.; Luber, G.; Phelan, P. A biometeorology study of climate and heat-related morbidity in Phoenix from 2001 to 2006. Int. J. Biometeorol. 2008, 52, 471–480. [Google Scholar] [CrossRef]
- Meehl, G.A.; Tebaldi, C. More intense, more frequent, and longer lasting heat waves in the 21st century. Science 2004, 305, 994–997. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Wang, X.; Thatcher, M.; Barnett, G.; Kachenko, A.; Prince, R. Urban vegetation for reducing heat related mortality. Environ. Pollut. 2014, 192, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Lai, D.; Liu, W.; Gan, T.; Liu, K.; Chen, Q. A review of mitigating strategies to improve the thermal environment and thermal comfort in urban outdoor spaces. Sci. Total Environ. 2019, 661, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Santos Nouri, A.; Costa, J.P.; Santamouris, M.; Matzarakis, A. Approaches to outdoor thermal comfort thresholds through public space design: A review. Atmosphere 2018, 9, 108. [Google Scholar] [CrossRef] [Green Version]
- Peng, J.; Xie, P.; Liu, Y.; Ma, J. Urban thermal environment dynamics and associated landscape pattern factors: A case study in the Beijing metropolitan region. Remote Sens. Environ. 2016, 173, 145–155. [Google Scholar] [CrossRef]
- Kim, E.J.; Kim, H. Effect modification of individual- and regional-scale characteristics on heat wave-related mortality rates between 2009 and 2012 in Seoul, South Korea. Sci. Total Environ. 2017, 595, 141–148. [Google Scholar] [CrossRef]
- Gronlund, C.J.; Berrocal, V.J.; White-Newsome, J.L.; Conlon, K.C.; O’neill, M.S. Vulnerability to extreme heat by socio-demographic characteristics and area green space among the elderly in Michigan 1990–2007. Environ. Res. 2015, 136, 449–461. [Google Scholar] [CrossRef] [Green Version]
- Harlan, S.L.; Declet-Barreto, J.H.; Stefanov, W.L.; Petitti, D.B. Neighborhood effects on heat deaths: Social and environmental predictors of vulnerability in Maricopa County, Arizona. Environ. Health Perspect. 2013, 121, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.L.; Baumann, L.M.; Romero, K.; Combe, J.M.; Gomez, A.; Gilman, R.H.; Cabrera, L.; Gonzalvez, G.; Hansel, N.N.; Wise, R.; et al. Effect of urbanisation on asthma, allergy and airways inflammation in a developing country setting. Thorax 2011, 66, 1051–1057. [Google Scholar] [CrossRef] [Green Version]
- Kovats, R.S.; Hajat, S. Heat stress and public health: A critical review. Annu. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef]
- Lloyd-Sherlock, P. Population ageing in developed and developing regions: Implications for health policy. Soc. Sci. Med. 2000, 51, 887–895. [Google Scholar] [CrossRef]
- Epstein, Y.; Moran, D.S. Thermal comfort and the heat stress indices. Ind. Health 2006, 44, 388–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayak, S.; Shrestha, S.; Kinney, P.; Ross, Z.; Sheridan, S.; Pantea, C.; Hsu, W.; Muscatiello, N.; Hwang, S. Development of a heat vulnerability index for New York State. Public Health 2018, 161, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.P.; Stanforth, A.; Lulla, V.; Luber, G. Developing an applied extreme heat vulnerability index utilizing socioeconomic and environmental data. Appl. Geogr. 2012, 35, 23–31. [Google Scholar] [CrossRef]
- Xu, Y.; Dadvand, P.; Barrera-Gómez, J.; Sartini, C.; Marí-Dell’Olmo, M.; Borrell, C.; Medina-Ramón, M.; Sunyer, J.; Basagaña, X. Differences on the effect of heat waves on mortality by sociodemographic and urban landscape characteristics. J. Epidemiol. Community Health 2013, 67, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Ostro, B.D. A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. Am. J. Epidemiol. 2008, 168, 632–637. [Google Scholar] [CrossRef]
- Kenney, W.L. Decreased cutaneous vasodilation in aged skin: Mechanisms, consequences and interventions. J. Therm. Biol. 2001, 26, 263–271. [Google Scholar] [CrossRef]
- Vanos, J.K.; Kalkstein, L.S.; Sanford, T.J. Detecting synoptic warming trends across the US Midwest and implications to human health and heat-related mortality. Int. J. Climatol. 2015, 35, 85–96. [Google Scholar]
- Madrigano, J.; Ito, K.; Johnson, S.; Kinney, P.L.; Matte, T. A Case-Only Study of Vulnerability to Heat Wave-Related Mortality in New York City (2000-2011). Environ. Health Perspect. 2015, 123, 672–678. [Google Scholar] [CrossRef]
- Steadman, R.G. A universal scale of apparent temperature. J. Appl. Meteorol. Climatol. 1984, 23, 1674–1687. [Google Scholar] [CrossRef]
- Cheng, J.; Xu, Z.; Zhao, D.; Xie, M.; Zhang, H.; Wang, S.; Su, H. The burden of extreme heat and heatwave on emergency ambulance dispatches: A time-series study in Huainan, China. Sci. Total Environ. 2016, 571, 27–33. [Google Scholar] [CrossRef]
- Krehl, A.; Siedentop, S.; Taubenböck, H.; Wurm, M. A comprehensive view on urban spatial structure: Urban density patterns of German city regions. ISPRS Int. J. Geo-Inf. 2016, 5, 76. [Google Scholar] [CrossRef] [Green Version]
- Angel, S.; Franco, S.A.; Liu, Y.; Blei, A.M. The shape compactness of urban footprints. Prog. Plan. 2020, 139, 100429. [Google Scholar] [CrossRef]
- Burton, E. Measuring urban compactness in UK towns and cities. Environ. Plan. B Plan. Des. 2002, 29, 219–250. [Google Scholar] [CrossRef]
- Parr, J.B. The regional economy, spatial structure and regional urban systems. Reg. Stud. 2014, 48, 1926–1938. [Google Scholar] [CrossRef]
- Avdan, U.; Jovanovska, G. Algorithm for automated mapping of land surface temperature using LANDSAT 8 satellite data. J. Sens. 2016, 2016, 1480307. [Google Scholar] [CrossRef] [Green Version]
- Reid, C.E.; O’Neill, M.S.; Gronlund, C.J.; Brines, S.J.; Brown, D.; Diez-Roux, A.V.; Schwartz, J. Mapping community determinants of heat vulnerability. Environ. Health Perspect. 2009, 117, 1730–1736. [Google Scholar] [CrossRef]
- Ver Hoef, J.M.; Boveng, P.L. Quasi-Poisson vs. negative binomial regression: How should we model overdispersed count data? Ecology 2007, 88, 2766–2772. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, J.M.; Lattimore, P.K. Count Models in Criminology. In Handbook of Quantitative Criminology; Springer: Berlin/Heidelberg, Germany, 2010; pp. 683–698. [Google Scholar]
- Berk, R.; MacDonald, J.M. Overdispersion and Poisson regression. J. Quant. Criminol. 2008, 24, 269–284. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Shephard, R.J. Habitual physical activity and health in the elderly: The Nakanojo Study. Geriatr. Gerontol. Int. 2010, 10, S236–S243. [Google Scholar] [CrossRef]
- Priyadarsini, R.; Hien, W.N.; David, C.K.W. Microclimatic modeling of the urban thermal environment of Singapore to mitigate urban heat island. Sol. Energy 2008, 82, 727–745. [Google Scholar] [CrossRef]
- Son, J.Y.; Lane, K.J.; Lee, J.-T.; Bell, M.L. Urban vegetation and heat-related mortality in Seoul, Korea. Environ. Res. 2016, 151, 728–733. [Google Scholar] [CrossRef] [Green Version]
- Zanobetti, A.; O’Neill, M.S.; Gronlund, C.J.; Schwartz, J.D. Susceptibility to mortality in weather extremes: Effect modification by personal and small area characteristics in a multi-city case-only analysis. Epidemiol. 2013, 24, 809–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Review Article: Vulnerability to Heat-related Mortality: A Systematic Review, Meta-analysis, and Meta-regression Analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [CrossRef] [PubMed]
- Hendel, M.; Azos-Diaz, K.; Tremeac, B. Behavioral adaptation to heat-related health risks in cities. Energy Build. 2017, 152, 823–829. [Google Scholar] [CrossRef]
- Bergstrand, K.; Mayer, B.; Brumback, B.; Zhang, Y. Assessing the relationship between social vulnerability and community resilience to hazards. Soc. Indic. Res. 2015, 122, 391–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, B.E.; Hallisey, E.J.; Adams, E.; Lavery, A. Measuring community vulnerability to natural and anthropogenic hazards: The Centers for Disease Control and Prevention’s Social Vulnerability Index. J. Environ. Health 2018, 80, 34–36. [Google Scholar] [PubMed]
- Gronlund, C.J. Racial and socioeconomic disparities in heat-related health effects and their mechanisms: A review. Curr. Epidemiol. Rep. 2014, 1, 165–173. [Google Scholar] [CrossRef]
- Klinenberg, E. Heat Wave: A Social Autopsy of Disaster in Chicago; University of Chicago Press: Chicago, IL, USA, 2015. [Google Scholar]
- Sampson, N.R.; Gronlund, C.J.; Buxton, M.A.; Catalano, L.; White-Newsome, J.L.; Conlon, K.C.; O’Neill, M.S.; McCormick, S.; Parker, E.A. Staying cool in a changing climate: Reaching vulnerable populations during heat events. Glob. Environ. Chang. 2013, 23, 475–484. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Category | Variable | Abbreviation | Mean | SD | Min | Max |
|---|---|---|---|---|---|---|
| Heat-related Morbidity | Normal heat days daily EMS | NH | 48.78 | 37.20 | 2.50 | 275.50 |
| 95th extreme heat days daily EMS | 95th EH | 23.00 | 17.03 | 0.00 | 125.00 | |
| 97.5th extreme heat days daily EMS | 97.5th EH | 9.88 | 8.51 | 0.00 | 54.00 | |
| Urban Landscape | Percent of tree cover | Tree | 34.48 | 16.50 | 2.94 | 84.38 |
| Percent of grass area | Grass | 21.33 | 6.91 | 1.07 | 52.28 | |
| Percent of impervious surface | Imper | 41.00 | 17.72 | 5.48 | 92.34 | |
| Percent of water area | Water | 0.64 | 2.68 | 0.00 | 23.33 | |
| Population density (urban density) | Dense | 9.27 | 5.97 | 0.23 | 32.41 | |
| Average of NDBI * (built-up) | NDBI | −0.11 | 0.04 | −0.20 | 0.02 | |
| Average of LST ** | LST | 22.89 | 1.52 | 18.40 | 26.50 | |
| Socio-demographic | Percent of over 65 years of age | +65 | 12.93 | 8.76 | 0.68 | 47.53 |
| Percent of over 65 years of age and living alone | 65+ alone | 43.39 | 24.95 | 2.27 | 97.28 | |
| Percent of living alone | Live alone | 19.89 | 11.66 | 1.13 | 74.18 | |
| Percent of non-white | Non white | 51.47 | 29.19 | 3.32 | 97.95 | |
| Percent of no high school diploma | No HS | 13.45 | 11.39 | 0.23 | 61.29 | |
| Percent below the poverty line | Poverty | 26.04 | 19.45 | 0.18 | 86.23 | |
| Percent of unemployment | Unemployment | 10.05 | 10.00 | 0.48 | 64.41 | |
| Percent of building before 1939 | Old Building | 43.01 | 25.06 | 1.05 | 95.83 | |
| Confounding Variables | Population | - | 188 | 246 | 19 | 2781 |
| Size of block group | - | 1085 | 553 | 155 | 4405 |
| Variable | Urban Landscape | Socio-Demographic | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tree | Grass | Imper | Water | Dense | LST | NDBI | +65 | 65+ Alone | Live Alone | Non White | No HS | Poverty | Unemployment | Old Building | |
| Tree | 1 | ||||||||||||||
| Grass | 0.079 | 1 | |||||||||||||
| Impervious | −0.856 ** | −0.426 ** | 1 | ||||||||||||
| Water | −0.059 | −0.024 | −0.160 ** | 1 | |||||||||||
| Density | −0.367 ** | −0.137 * | 0.493 ** | −0.290 ** | 1 | ||||||||||
| LST | −0.897 ** | −0.367 ** | 0.923 ** | 0.033 | 0.326 ** | 1 | |||||||||
| NDBI | −0.906 ** | −0.183 ** | 0.900 ** | −0.062 | 0.458 ** | 0.897 ** | 1 | ||||||||
| 65+ | 0.044 | 0.186 ** | −0.128 * | 0.047 | −0.310 ** | −0.105 | −0.062 | 1 | |||||||
| 65+ alone | −0.138 * | −0.044 | 0.144 * | −0.060 | 0.144 * | 0.147 * | 0.149 * | 0.091 | 1 | ||||||
| Live alone | −0.026 | −0.114 | 0.111 | −0.141 * | 0.080 | 0.053 | 0.048 | 0.125 * | 0.082 | 1 | |||||
| Non white | −0.103 | 0.146 * | 0.094 | −0.204 ** | 0.059 | 0.163 ** | 0.153 ** | 0.036 | 0.100 | 0.003 | 1 | ||||
| No HS | 0.001 | −0.056 | −0.023 | 0.045 | −0.114 | 0.088 | −0.017 | −0.033 | 0.053 | −0.019 | 0.426 ** | 1 | |||
| Poverty | −0.094 | −0.043 | 0.095 | −0.055 | 0.098 | 0.159 ** | 0.080 | −0.192 ** | 0.065 | −0.048 | 0.453 ** | 0.514 ** | 1 | ||
| Unemployment | −0.093 | −0.122 * | 0.128 * | −0.023 | 0.135 * | 0.181 ** | 0.092 | −0.243 ** | 0.124 * | −0.054 | 0.519 ** | 0.638 ** | 0.600 ** | 1 | |
| Old Building | −0.244 ** | −0.268 ** | 0.318 ** | 0.045 | 0.105 | 0.274 ** | 0.254 ** | −0.174 ** | −0.101 | −0.022 | −0.173 ** | −0.012 | 0.003 | −0.044 | 1 |
| Category | Variable | Model 1 (Normal Heat) | Model 2 (EH 95th) | Model 3 (EH 97.5th) | |||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||
| Urban landscape | Grass area | 0.847 ** | 0.755–0.951 | 0.839 ** | 0.750–0.940 | 0.861 ** | 0.765–0.972 |
| Impervious surface | 1.120 ** | 1.065–1.177 | 1.141 ** | 1.087–1.198 | 1.157 ** | 1.099–1.219 | |
| Socio-demographic | Age > 65 years | 1.320 ** | 1.209–1.441 | 1.300 ** | 1.194–1.415 | 1.277 ** | 1.166–1.399 |
| Age > 65 living alone | 1.016 | 0.982–1.051 | 1.012 | 0.980–1.045 | 1.009 | 0.975–1.044 | |
| Race other than white | 1.070 ** | 1.033–1.109 | 1.069 ** | 1.033–1.107 | 1.081 ** | 1.042–1.121 | |
| No HS diploma | 1.084 | 1.021–1.152 | 1.130 ** | 1.035–1.234 | 1.119 * | 1.018–1.229 | |
| <Poverty line | 1.083 ** | 0.987–1.189 | 1.056 | 0.996–1.120 | 1.044 | 0.982–1.111 | |
| Unemployment | 1.099 | 0.999–1.208 | 1.111 | 1.014–1.217 | 1.141 ** | 1.038–1.255 | |
| Confounding variable | Area | 1.109 ** | 1.080–1.138 | 1.105 ** | 1.077–1.134 | 1.109 ** | 1.079–1.140 |
| Population | exposure | - | exposure | - | exposure | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Brown, R.D. Effects of Urban Landscape and Sociodemographic Characteristics on Heat-Related Health Using Emergency Medical Service Incidents. Int. J. Environ. Res. Public Health 2022, 19, 1287. https://doi.org/10.3390/ijerph19031287
Lee K, Brown RD. Effects of Urban Landscape and Sociodemographic Characteristics on Heat-Related Health Using Emergency Medical Service Incidents. International Journal of Environmental Research and Public Health. 2022; 19(3):1287. https://doi.org/10.3390/ijerph19031287
Chicago/Turabian StyleLee, Kanghyun, and Robert D. Brown. 2022. "Effects of Urban Landscape and Sociodemographic Characteristics on Heat-Related Health Using Emergency Medical Service Incidents" International Journal of Environmental Research and Public Health 19, no. 3: 1287. https://doi.org/10.3390/ijerph19031287
APA StyleLee, K., & Brown, R. D. (2022). Effects of Urban Landscape and Sociodemographic Characteristics on Heat-Related Health Using Emergency Medical Service Incidents. International Journal of Environmental Research and Public Health, 19(3), 1287. https://doi.org/10.3390/ijerph19031287