
Impact of Income and Industry on New-Onset Diabetes among Employees: A Retrospective Cohort Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
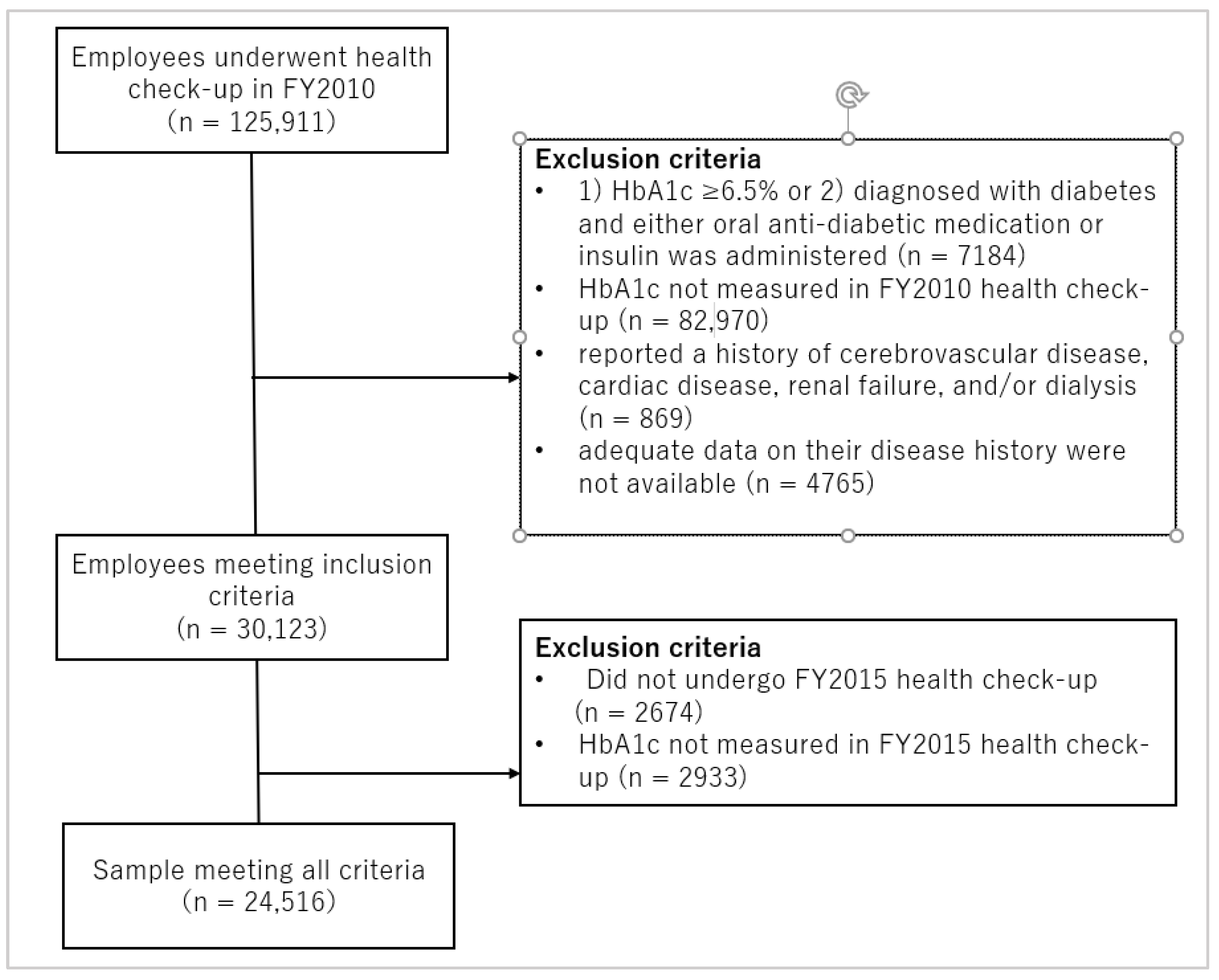
2.2. Study Population
2.3. Definition of Diabetes
2.4. Categorizations of Variables
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. Participant Characteristics
3.2. Odds Ratios and 95% Confidence Intervals for the Onset of Diabetes
3.3. Summary of Research Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kolb, H.; Martin, S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 2017, 15, 131. [Google Scholar] [CrossRef] [PubMed]
- Persson, P.G.; Carlsson, S.; Svanström, L.; Ostenson, C.G.; Efendic, S.; Grill, V. Cigarette smoking, oral moist snuff use and glucose intolerance. J. Intern. Med. 2000, 248, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Lantz, P.M.; House, J.S.; Lepkowski, J.M.; Williams, D.R.; Mero, R.P.; Chen, J. Socioeconomic factors, health behaviors, and mortality: Results from a nationally representative prospective study of US adults. JAMA 1998, 279, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Osler, M. Social class and health behaviour in Danish adults: A longitudinal study. Public Health 1993, 107, 251–260. [Google Scholar] [CrossRef]
- Wagenknecht, L.E.; Perkins, L.L.; Cutter, G.R.; Sidney, S.; Burke, G.L.; Manolio, T.A.; Jacobs, D.R., Jr.; Liu, K.A.; Friedman, G.D.; Hughes, G.H.; et al. Cigarette smoking behavior is strongly related to educational status: The CARDIA study. Prev. Med. 1990, 19, 158–169. [Google Scholar] [CrossRef]
- Agardh, E.E.; Ahlbom, A.; Andersson, T.; Efendic, S.; Grill, V.; Hallqvist, J.; Ostenson, C.G. Explanations of socioeconomic differences in excess risk of type 2 diabetes in Swedish men and women. Diabetes Care 2004, 27, 716–721. [Google Scholar] [CrossRef]
- Nagamine, Y.; Kondo, N.; Yokobayashi, K.; Ota, A.; Miyaguni, Y.; Sasaki, Y.; Tani, Y.; Kondo, K. Socioeconomic Disparity in the Prevalence of Objectively Evaluated Diabetes Among Older Japanese Adults: JAGES Cross-Sectional Data in 2010. J. Epidemiol. 2019, 29, 295–301. [Google Scholar] [CrossRef]
- Robbins, J.M.; Vaccarino, V.; Zhang, H.; Kasl, S.V. Socioeconomic status and type 2 diabetes in African American and non-Hispanic white women and men: Evidence from the Third National Health and Nutrition Examination Survey. Am. J. Public Health 2001, 91, 76–83. [Google Scholar] [CrossRef]
- Smith, B.T.; Lynch, J.W.; Fox, C.S.; Harper, S.; Abrahamowicz, M.; Almeida, N.D.; Loucks, E.B. Life-course socioeconomic position and type 2 diabetes mellitus: The Framingham Offspring Study. Am. J. Epidemiol. 2011, 173, 438–447. [Google Scholar] [CrossRef]
- Tang, M.; Chen, Y.; Krewski, D. Gender-related differences in the association between socioeconomic status and self-reported diabetes. Int. J. Epidemiol. 2003, 32, 381–385. [Google Scholar] [CrossRef]
- Berkman, L.F.; Kawachi, I.; Glymour, M.M. Social epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar] [CrossRef]
- Ervasti, J.; Virtanen, M.; Pentti, J.; Lallukka, T.; Tinghog, P.; Kjeldgard, L.; Mittendorfer-Rutz, E.; Alexanderson, K. Work disability before and after diabetes diagnosis: A nationwide population-based register study in Sweden. Am. J. Public Health 2015, 105, e22–e29. [Google Scholar] [CrossRef] [PubMed]
- Breton, M.C.; Guenette, L.; Amiche, M.A.; Kayibanda, J.F.; Gregoire, J.P.; Moisan, J. Burden of diabetes on the ability to work: A systematic review. Diabetes Care 2013, 36, 740–749. [Google Scholar] [CrossRef] [PubMed]
- Robone, S.; Jones, A.M.; Rice, N. Contractual conditions, working conditions and their impact on health and well-being. Eur. J. Health Econ. 2011, 12, 429–444. [Google Scholar] [CrossRef]
- Schrijvers, C.T.; van de Mheen, H.D.; Stronks, K.; Mackenbach, J.P. Socioeconomic inequalities in health in the working population: The contribution of working conditions. Int. J. Epidemiol. 1998, 27, 1011–1018. [Google Scholar] [CrossRef]
- Brown, S.A.; Garcia, A.A.; Zuniga, J.A.; Lewis, K.A. Effectiveness of workplace diabetes prevention programs: A systematic review of the evidence. Patient Educ. Couns. 2018, 101, 1036–1050. [Google Scholar] [CrossRef] [PubMed]
- Hafez, D.; Fedewa, A.; Moran, M.; O’Brien, M.; Ackermann, R.; Kullgren, J.T. Workplace Interventions to Prevent Type 2 Diabetes Mellitus: A Narrative Review. Curr. Diabetes Rep. 2017, 17, 9. [Google Scholar] [CrossRef] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Anderson, J.M. Achievable cost saving and cost-effective thresholds for diabetes prevention lifestyle interventions in people aged 65 years and older: A single-payer perspective. J. Acad. Nutr. Diet. 2012, 112, 1747–1754. [Google Scholar] [CrossRef]
- Carlsson, S.; Andersson, T.; Talbäck, M.; Feychting, M. Incidence and prevalence of type 2 diabetes by occupation: Results from all Swedish employees. Diabetologia 2020, 63, 95–103. [Google Scholar] [CrossRef]
- Kelsall, H.L.; Fernando, P.H.S.; Gwini, S.M.; Sim, M.R. Cardiovascular Disease and Type 2 Diabetes Risk Across Occupational Groups and Industry in a Statewide Study of an Australian Working Population. J. Occup. Environ. Med. 2018, 60, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Witters, D.; Liu, D. Diabetes Rate Greatest among Transportation Workers. Available online: https://news.gallup.com/poll/214097/diabetes-rate-greatest-among-transportation-workers.aspx. (accessed on 5 March 2021).
- Ministry of Health, Labour and Welfare. Basic Survey on Wage Structure. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00450091&tstat=000001011429 (accessed on 31 December 2021).
- Hiltunen, L.A. Are there associations between socio-economic status and known diabetes in an elderly Finnish population? Cent. Eur. J. Public Health 2005, 13, 187–190. [Google Scholar] [PubMed]
- Rathmann, W.; Haastert, B.; Icks, A.; Giani, G.; Holle, R.; Meisinger, C.; Mielck, A. Sex differences in the associations of socioeconomic status with undiagnosed diabetes mellitus and impaired glucose tolerance in the elderly population: The KORA Survey 2000. Eur. J. Public Health 2005, 15, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Waller, J.; Jarvis, M.J. Sex differences in the association of socioeconomic status with obesity. Am. J. Public Health 2002, 92, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Shon, C. Relationship between socioeconomic status and type 2 diabetes: Results from Korea National Health and Nutrition Examination Survey (KNHANES) 2010-2012. BMJ Open 2014, 4, e005710. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Survey on Employment Trends. Available online: https://www.mhlw.go.jp/toukei/list/9-23-1.html (accessed on 31 December 2021).
- Association, J.H.I. Jigyo Nenpo Heisei 27 Nendo (Annual Report 2015 Fiscal Year). Available online: https://www.kyoukaikenpo.or.jp/g7/cat740/sb7200/sbb7200/270407/ (accessed on 1 March 2021).
- Health Service Bureau, the Ministry of Health. Labour and Welfare. Standard Health Checkup and Counseling Guidance Program (Revised Version). Available online: http://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/kenkou/seikatsu/ (accessed on 15 December 2020).
- Seino, Y.; Nanjo, K.; Tajima, N.; Kadowaki, T.; Kashiwagi, A.; Araki, E.; Ito, C.; Inagaki, N.; Iwamoto, Y.; Kasuga, M.; et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J. Diabetes Investig. 2010, 1, 212–228. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, W.; Miyazaki, S. Diagnosis criteria for obesity and obesity disease. Health Eval. Promot. 2015, 42, 301–306. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications. Japan Standard Industrial Classification. Available online: https://www.soumu.go.jp/toukei_toukatsu/index/seido/sangyo/H25index.htm (accessed on 1 March 2021).
- Ministry of Health, Labour and Welfare. National Health and Nutrition Survey. Available online: https://www.mhlw.go.jp/bunya/kenkou/kenkou_eiyou_chousa.html (accessed on 16 February 2021).
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Schernhammer, E.S.; Sun, Q.; Hu, F.B. Rotating night shift work and risk of type 2 diabetes: Two prospective cohort studies in women. PLoS Med. 2011, 8, e1001141. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Internal Affairs and Communications Labour Force Survey. Available online: https://www.e-stat.go.jp/stat-search/database?page=1&layout=datalist&toukei=00200531&tstat=000000110001&cycle=7&tclass1=000001040276&tclass2=000001040299&tclass3=000001040303&result_page=1&tclass4val=0 (accessed on 17 February 2021).
- Nutbeam, D. Evaluating Health Promotion—Progress, Problems and solutions. Health Promot. Int. 1998, 13, 27–44. [Google Scholar] [CrossRef]
- Ishikawa, H.; Nomura, K.; Sato, M.; Yano, E. Developing a measure of communicative and critical health literacy: A pilot study of Japanese office workers. Health Promot. Int. 2008, 23, 269–274. [Google Scholar] [CrossRef]
- Yokokawa, H.; Yuasa, M.; Sanada, H.; Hisaoka, T.; Fukuda, H. Age- and Sex-Specific Impact of Health Literacy on Healthy Lifestyle Characteristics among Japanese Residents in a Rural Community. Health 2015, 7, 679–688. [Google Scholar] [CrossRef]
- Yokokawa, H.; Fukuda, H.; Yuasa, M.; Sanada, H.; Hisaoka, T.; Naito, T. Association between health literacy and metabolic syndrome or healthy lifestyle characteristics among community-dwelling Japanese people. Diabetol. Metab. Syndr. 2016, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, S.T.; Fransson, E.I.; Heikkilä, K.; Ahola, K.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Dragano, N.; Goldberg, M.; et al. Job strain as a risk factor for type 2 diabetes: A pooled analysis of 124,808 men and women. Diabetes Care 2014, 37, 2268–2275. [Google Scholar] [CrossRef] [PubMed]
- Agardh, E.; Allebeck, P.; Hallqvist, J.; Moradi, T.; Sidorchuk, A. Type 2 diabetes incidence and socio-economic position: A systematic review and meta-analysis. Int. J. Epidemiol. 2011, 40, 804–818. [Google Scholar] [CrossRef]
- Wu, H.; Bragg, F.; Yang, L.; Du, H.; Guo, Y.; Jackson, C.A.; Zhu, S.; Yu, C.; Luk, A.O.Y.; Chan, J.C.N.; et al. Sex differences in the association between socioeconomic status and diabetes prevalence and incidence in China: Cross-sectional and prospective studies of 0.5 million adults. Diabetologia 2019, 62, 1420–1429. [Google Scholar] [CrossRef] [PubMed]
- Papier, K.; Jordan, S.; D’Este, C.; Bain, C.; Peungson, J.; Banwell, C.; Yiengprugsawan, V.; Seubsman, S.A.; Sleigh, A. Incidence and risk factors for type 2 diabetes mellitus in transitional Thailand: Results from the Thai cohort study. BMJ Open 2016, 6, e014102. [Google Scholar] [CrossRef] [PubMed]
- Alterman, T.; Luckhaupt, S.E.; Dahlhamer, J.M.; Ward, B.W.; Calvert, G.M. Prevalence rates of work organization characteristics among workers in the U.S.: Data from the 2010 National Health Interview Survey. Am. J. Ind. Med. 2013, 56, 647–659. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Short sleep duration among workers—United States, 2010. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 281–285.
- Kerkhof, G.A. Shift work and sleep disorder comorbidity tend to go hand in hand. Chronobiol. Int. 2018, 35, 219–228. [Google Scholar] [CrossRef]
- Rajaratnam, S.M.; Howard, M.E.; Grunstein, R.R. Sleep loss and circadian disruption in shift work: Health burden and management. Med. J. Aust. 2013, 199, S11–S15. [Google Scholar] [CrossRef] [PubMed]
- Bonnell, E.K.; Huggins, C.E.; Huggins, C.T.; McCaffrey, T.A.; Palermo, C.; Bonham, M.P. Influences on Dietary Choices during Day versus Night Shift in Shift Workers: A Mixed Methods Study. Nutrients 2017, 9, 193. [Google Scholar] [CrossRef] [PubMed]
- Amani, R.; Gill, T. Shiftworking, nutrition and obesity: Implications for workforce health- a systematic review. Asia Pac. J. Clin. Nutr. 2013, 22, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Survey on Workers Who Changed Jobs. Available online: https://www.mhlw.go.jp/toukei/list/6-18c-r02.html (accessed on 31 December 2021).
- Healthcare Industries Division. Ministry of Economy Trade and Industry. Enhancing Health and Productivity Management. Available online: https://www.meti.go.jp/policy/mono_info_service/healthcare/downloadfiles/180717health-and-productivity-management.pdf (accessed on 1 March 2021).


{kind=link}
| Title | All | Male | Female | |||||||||
| DM+ | Total | pValue | DM+ | Total | pValue | DM+ | Total | pValue | ||||
| n | (%) | n | n | (%) | n | n | (%) | n | ||||
| 773 | (3.2) | 24516 | 620 | (4.0) | 15474 | 153 | (1.7) | 9042 | ||||
| Sex | ||||||||||||
| Male | 620 | (4.0) | 15,474 | <0.001 | ||||||||
| Female | 153 | (1.7) | 9042 | |||||||||
| Age Category | ||||||||||||
| 40–49 | 332 | (2.6) | 12783 | <0.001 | 275 | (3.4) | 8197 | <0.001 | 57 | (1.2) | 4586 | <0.001 |
| 50–59 | 316 | (3.4) | 9307 | 244 | (4.4) | 5585 | 72 | (1.9) | 3722 | |||
| 60–74 | 125 | (5.2) | 2426 | 101 | (6.0) | 1692 | 24 | (3.3) | 734 | |||
| Income Level (USD) Quartile | ||||||||||||
| Q1: <2000 | 187 | (3.0) | 6219 | 0.704 | 87 | (5.4) | 1615 | <0.001 | 100 | (2.2) | 4604 | 0.002 |
| Q2: 2000–2999 | 175 | (3.3) | 5236 | 143 | (4.8) | 2977 | 32 | (1.4) | 2259 | |||
| Q3: 3000–3799 | 214 | (3.1) | 6990 | 201 | (3.6) | 5540 | 13 | (0.9) | 1450 | |||
| Q4: ≥3800 | 197 | (3.2) | 6071 | 189 | (3.5) | 5342 | 8 | (1.1) | 729 | |||
| Hypertension with Medication | ||||||||||||
| Yes | 338 | (5.6) | 6035 | <0.001 | 272 | (6.1) | 4488 | <0.001 | 66 | (4.3) | 1547 | <0.001 |
| No | 435 | (2.4) | 18481 | 348 | (3.2) | 10986 | 87 | (1.2) | 7495 | |||
| Dyslipidemia with Medication | ||||||||||||
| Yes | 448 | (4.8) | 9328 | <0.001 | 352 | (5.4) | 6486 | <0.001 | 96 | (3.4) | 2842 | <0.001 |
| No | 325 | (2.1) | 15187 | 268 | (3.0) | 8987 | 57 | (0.9) | 6200 | |||
| BMI | ||||||||||||
| <25 | 350 | (1.9) | 18423 | <0.001 | 279 | (2.6) | 10912 | <0.001 | 71 | (0.9) | 7511 | <0.001 |
| ≥25 | 423 | (6.9) | 6093 | 341 | (7.5) | 4562 | 82 | (5.4) | 1531 | |||
| Smoking | ||||||||||||
| Yes | 377 | (4.1) | 9257 | <0.001 | 340 | (4.5) | 7634 | 0.005 | 37 | (2.3) | 1623 | 0.043 |
| No | 395 | (2.6) | 15,243 | 279 | (3.6) | 7830 | 116 | (1.6) | 7413 | |||
| Types of Industry | ||||||||||||
| Agriculture, forestry, and fisheries | 4 | (6.3) | 64 | 0.156 | 2 | (6.1) | 33 | 0.547 | 2 | (6.5) | 31 | 0.040 |
| Mining and stone quarrying | 2 | (3.1) | 64 | 0.990 | 2 | (3.4) | 59 | 0.809 | 0 | (0.0) | 5 | 0.769 |
| Construction | 79 | (3.8) | 2077 | 0.076 | 70 | (4.1) | 1699 | 0.801 | 9 | (2.4) | 378 | 0.289 |
| Manufacturing | 156 | (2.9) | 5444 | 0.169 | 133 | (3.3) | 4090 | 0.004 | 23 | (1.7) | 1354 | 0.984 |
| Electricity, gas, heat supply, and water | 5 | (5.1) | 99 | 0.279 | 4 | (5.4) | 74 | 0.539 | 1 | (4.0) | 25 | 0.370 |
| Information and communications | 18 | (2.0) | 880 | 0.945 | 15 | (3.4) | 446 | 0.482 | 3 | (2.2) | 134 | 0.621 |
| Transport and postal services | 130 | (4.7) | 2788 | <0.001 | 126 | (5.0) | 2527 | 0.006 | 4 | (1.5) | 261 | 0.839 |
| Wholesale and retail trade | 167 | (3.5) | 4793 | 0.143 | 123 | (4.4) | 2775 | 0.207 | 44 | (2.2) | 2018 | 0.054 |
| Finance and insurance | 13 | (2.6) | 497 | 0.489 | 9 | (4.3) | 211 | 0.847 | 4 | (1.4) | 286 | 0.696 |
| Real estate and goods rental and leasing | 18 | (4.0) | 454 | 0.318 | 17 | (5.7) | 296 | 0.124 | 1 | (0.6) | 158 | 0.298 |
| Scientific research, professional and technical services | 24 | (3.8) | 630 | 0.339 | 23 | (5.0) | 463 | 0.284 | 1 | (0.6) | 167 | 0.269 |
| Accommodations, food and beverage services | 13 | (3.2) | 402 | 0.926 | 8 | (3.4) | 234 | 0.644 | 5 | (3.0) | 168 | 0.193 |
| Living-related and personal services and entertainment services | 17 | (3.5) | 485 | 0.654 | 12 | (4.4) | 274 | 0.751 | 5 | (2.4) | 211 | 0.440 |
| Education and learning support | 4 | (1.9) | 216 | 0.272 | 4 | (2.7) | 147 | 0.425 | 0 | (0.0) | 69 | 0.274 |
| Medical, health care, and welfare | 55 | (1.6) | 3343 | <0.001 | 20 | (2.5) | 797 | 0.027 | 35 | (1.4) | 2546 | 0.143 |
| Compound services | 0 | (0.0) | 42 | 0.242 | 0 | (0.0) | 19 | 0.373 | 0 | (0.0) | 23 | 0.529 |
| Other services | 55 | (2.8) | 1999 | 0.284 | 47 | (3.8) | 1232 | 0.721 | 8 | (1.0) | 767 | 0.145 |
| Government services | 13 | (2.4) | 539 | 0.319 | 5 | (5.1) | 98 | 0.579 | 8 | (1.8) | 441 | 0.839 |
| Title | Male (n = 15,474) | Female (n = 9042) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||||||
| OR | 95%CI | OR | 95%CI | OR | 95%CI | OR | 95%CI | |||||
| Age Category | ||||||||||||
| 50–59 | 1.32 | 1.10 | 1.57 | 1.26 | 1.05 | 1.52 | 1.57 | 1.10 | 2.22 | 1.11 | 0.76 | 1.61 |
| 60–74 | 1.83 | 1.45 | 2.31 | 1.59 | 1.21 | 2.09 | 2.69 | 1.66 | 4.36 | 1.55 | 0.90 | 2.65 |
| Income Level (USD) Quartile | ||||||||||||
| Q1: <2000 | 1.55 | 1.20 | 2.01 | 1.31 | 0.97 | 1.77 | 2.00 | 0.97 | 4.13 | 1.53 | 0.70 | 3.35 |
| Q2: 2000–2999 | 1.38 | 1.10 | 1.72 | 1.38 | 1.09 | 1.75 | 1.30 | 0.59 | 2.82 | 1.23 | 0.54 | 2.79 |
| Q3: 3000–3799 | 1.03 | 0.84 | 1.26 | 1.07 | 0.87 | 1.32 | 0.82 | 0.34 | 1.98 | 0.88 | 0.35 | 2.20 |
| Hypertension with Medication | ||||||||||||
| Yes | 1.97 | 1.68 | 2.32 | 1.54 | 1.29 | 1.82 | 3.79 | 2.74 | 5.25 | 2.08 | 1.46 | 2.95 |
| Dyslipidemia with Medication | ||||||||||||
| Yes | 1.87 | 1.59 | 2.20 | 1.59 | 1.35 | 1.88 | 3.77 | 2.71 | 5.24 | 2.60 | 1.84 | 3.69 |
| BMI | ||||||||||||
| ≥25 | 3.08 | 2.62 | 3.62 | 2.77 | 2.34 | 3.28 | 5.93 | 4.29 | 8.19 | 4.16 | 2.95 | 5.87 |
| Smoking | ||||||||||||
| Yes | 1.26 | 1.07 | 1.48 | 1.41 | 1.19 | 1.66 | 1.47 | 1.01 | 2.13 | 1.64 | 1.11 | 2.42 |
| Types of Industry | ||||||||||||
| Construction | 1.03 | 0.80 | 1.33 | 1.43 | 0.86 | 2.38 | 1.44 | 0.73 | 2.85 | 1.89 | 0.88 | 4.04 |
| Manufacturing | 0.75 | 0.62 | 0.91 | 1.22 | 0.76 | 1.98 | 1.00 | 0.64 | 1.57 | 0.97 | 0.55 | 1.69 |
| Information and communications | 0.83 | 0.49 | 1.40 | 1.50 | 0.75 | 2.98 | ||||||
| Transport and postal services | 1.32 | 1.08 | 1.62 | 1.46 | 0.89 | 2.38 | 0.90 | 0.33 | 2.45 | 0.88 | 0.30 | 2.56 |
| Wholesale and retail trade | 1.14 | 0.93 | 1.39 | 1.72 | 1.06 | 2.79 | 1.41 | 0.99 | 2.01 | 1.20 | 0.74 | 1.95 |
| Finance and insurance | 1.07 | 0.55 | 2.09 | 1.80 | 0.80 | 4.05 | 0.82 | 0.30 | 2.23 | 1.27 | 0.43 | 3.77 |
| Real estate and goods rental and leasing | 1.47 | 0.90 | 2.42 | 2.07 | 1.06 | 4.04 | ||||||
| Scientific research, professional and technical services | 1.26 | 0.82 | 1.93 | 1.78 | 0.96 | 3.29 | ||||||
| Accommodations, food and beverage services | 0.85 | 0.42 | 1.72 | 1.38 | 0.59 | 3.19 | ||||||
| Living-related and personal services and entertainment services | 1.10 | 0.61 | 1.97 | 1.64 | 0.78 | 3.45 | 1.42 | 0.58 | 3.51 | 1.79 | 0.68 | 4.74 |
| Medical, health care, and welfare | 0.60 | 0.38 | 0.95 | 1.00 | (reference) | 0.75 | 0.52 | 1.10 | 1.00 | (reference) | ||
| Other services | 0.95 | 0.70 | 1.28 | 1.35 | 0.79 | 2.32 | 0.59 | 0.29 | 1.21 | 0.63 | 0.29 | 1.39 |
| Government services | 1.08 | 0.53 | 2.21 | 1.21 | 0.54 | 2.71 | ||||||
| Male (n = 15,474) | Income Level (USD) Quartile | |||||||||||
| Q1 (n = 1615) | Q2 (n = 2977) | Q3 (n = 5540) | Q4 (n = 5,42) | |||||||||
| OR | 95%CI | OR | 95%CI | OR | 95%CI | OR | 95%CI | |||||
| Types of Industry | ||||||||||||
| Construction | 0.82 | 0.25 | 2.67 | 1.70 | 0.47 | 6.15 | 1.16 | 0.43 | 3.09 | 1.86 | 0.78 | 4.44 |
| Manufacturing | 0.41 | 0.13 | 1.26 | 1.41 | 0.42 | 4.70 | 0.86 | 0.33 | 2.22 | 2.24 | 0.99 | 5.05 |
| Information and communications | 1.11 | 0.33 | 3.75 | 2.51 | 0.86 | 7.33 | ||||||
| Transport and postal services | 0.54 | 0.20 | 1.45 | 2.11 | 0.64 | 6.99 | 1.07 | 0.40 | 2.82 | 1.88 | 0.73 | 4.86 |
| Wholesale and retail trade | 0.91 | 0.30 | 2.73 | 1.88 | 0.53 | 6.70 | 1.35 | 0.52 | 3.50 | 2.52 | 1.13 | 5.65 |
| Finance and insurance | 2.32 | 0.76 | 7.05 | |||||||||
| Real estate and goods rental and leasing | 2.21 | 0.42 | 11.56 | 1.81 | 0.49 | 6.62 | 1.71 | 0.43 | 6.76 | |||
| Scientific research, professional and technical services | 2.54 | 0.58 | 11.21 | 1.48 | 0.45 | 4.86 | 2.57 | 0.96 | 6.90 | |||
| Accommodations, food and beverage services | 0.75 | 0.14 | 3.99 | 1.51 | 0.30 | 7.49 | ||||||
| Living-related and personal services and entertainment services | 1.74 | 0.53 | 5.70 | 4.16 | 1.16 | 14.86 | ||||||
| Education and learning support | 1.34 | 0.31 | 5.86 | |||||||||
| Medical, health care, and welfare | 1 | (reference) | 1 | (reference) | 1 | (reference) | 1 | (reference) | ||||
| Other services | 0.63 | 0.20 | 1.98 | 1.11 | 0.29 | 4.32 | 0.70 | 0.23 | 2.11 | 3.10 | 1.29 | 7.47 |
| Female (n = 9042) | Income Level (USD) Quartile | |||||||||||
| Q1 (n = 4604) | Q2 (n = 2259) | Q3 (n = 1450) | Q4 (n = 729) | |||||||||
| OR | 95%CI | OR | 95%CI | OR | 95%CI | OR | 95%CI | |||||
| Types of Industry | ||||||||||||
| Construction | 2.28 | 0.70 | 7.43 | 1.37 | 0.29 | 6.46 | 2.83 | 0.50 | 16.18 | |||
| Manufacturing | 1.29 | 0.59 | 2.81 | 1.36 | 0.49 | 3.77 | ||||||
| Transport and postal services | 1.04 | 0.22 | 4.83 | 1.17 | 0.24 | 5.66 | ||||||
| Wholesale and retail trade | 1.76 | 0.88 | 3.51 | 0.77 | 0.24 | 2.47 | 0.46 | 0.05 | 4.09 | 0.96 | 0.10 | 9.10 |
| Finance and insurance | 1.27 | 0.15 | 10.56 | 1.68 | 0.19 | 14.87 | 0.96 | 0.18 | 5.28 | |||
| Living-related and personal services and entertainment services | 4.04 | 1.34 | 12.18 | |||||||||
| Medical, health care, and welfare | 1 | (reference) | 1 | (reference) | 1 | (reference) | 1 | (reference) | ||||
| Other services | 1.21 | 0.48 | 3.08 | |||||||||
| Government services | 1.42 | 0.51 | 3.95 | 2.35 | 0.49 | 11.28 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishihara, R.; Babazono, A.; Liu, N.; Yamao, R. Impact of Income and Industry on New-Onset Diabetes among Employees: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 1090. https://doi.org/10.3390/ijerph19031090
Ishihara R, Babazono A, Liu N, Yamao R. Impact of Income and Industry on New-Onset Diabetes among Employees: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1090. https://doi.org/10.3390/ijerph19031090
Chicago/Turabian StyleIshihara, Reiko, Akira Babazono, Ning Liu, and Reiko Yamao. 2022. "Impact of Income and Industry on New-Onset Diabetes among Employees: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 3: 1090. https://doi.org/10.3390/ijerph19031090
APA StyleIshihara, R., Babazono, A., Liu, N., & Yamao, R. (2022). Impact of Income and Industry on New-Onset Diabetes among Employees: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 19(3), 1090. https://doi.org/10.3390/ijerph19031090