
The Association between Serum Uric Acid Levels and 10-Year Cardiovascular Disease Risk in Non-Alcoholic Fatty Liver Disease Patients

 ,
,
Abstract
:1. Introduction
2. Methods
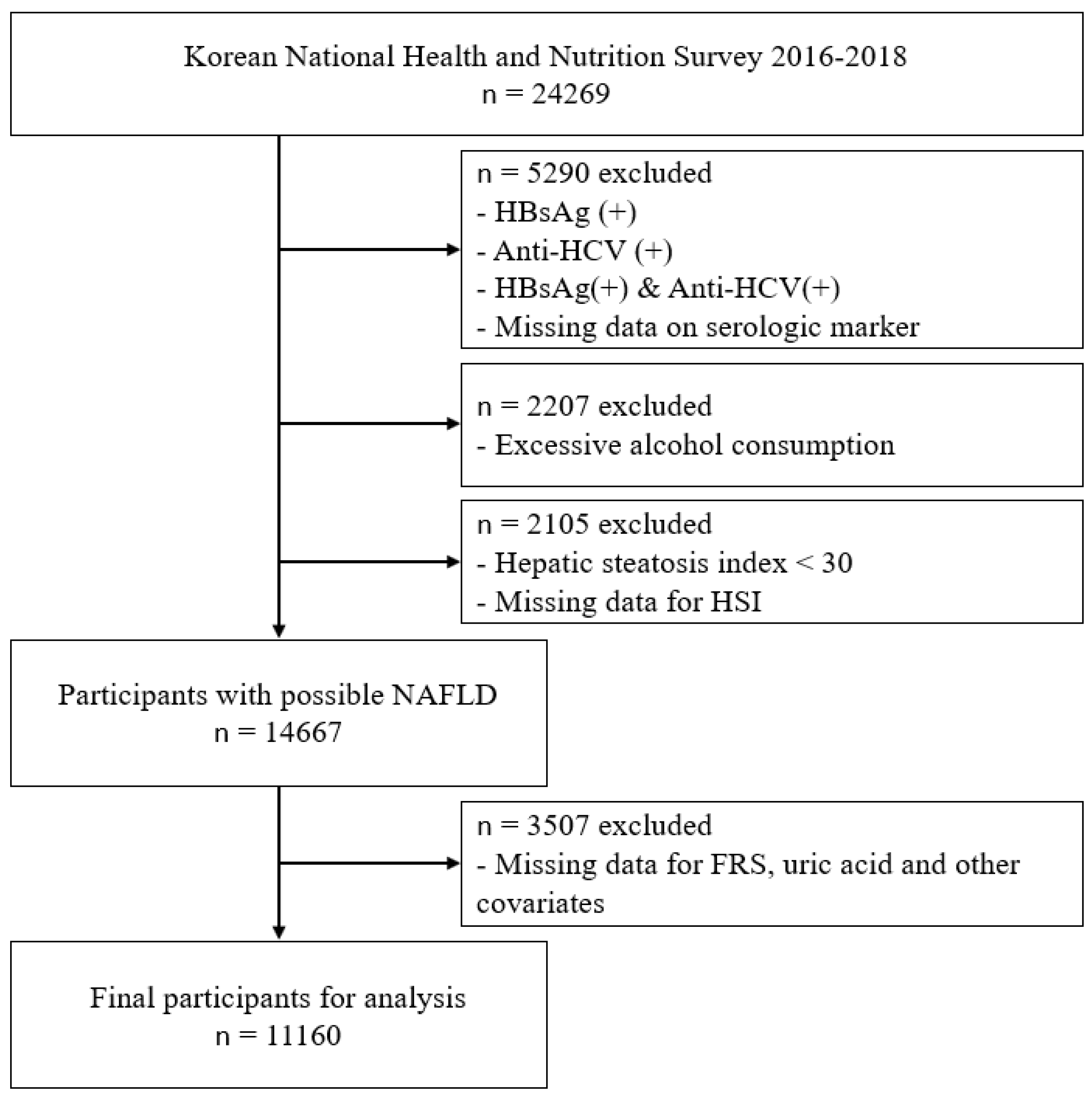
2.1. Study Participants
2.2. Serum Uric Acid
2.3. Framingham Risk Score and the Cardiovascular Disease Risk Groups
2.4. Confounding Variables
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Baseline Characteristics among Serum Uric Acid Quartiles
3.2. Baseline Characteristics of the Participants according to the 10-Year Cardiovascular Disease Risk
3.3. The Association between Serum Uric Acid Level and Having a High CVD Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rinella, M.E. Nonalcoholic fatty liver disease: A systematic review. JAMA 2015, 313, 2263–2273. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sanyal, A.J. The global NAFLD epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.L.; Reeves, H.L.; Burt, A.D.; Tiniakos, D.; McPherson, S.; Leathart, J.B.; Allison, M.E.; Alexander, G.J.; Piguet, A.C.; Anty, R.; et al. TM6SF2 rs58542926 influences hepatic fibrosis progression in patients with non-alcoholic fatty liver disease. Nat. Commun. 2014, 5, 4309. [Google Scholar] [CrossRef] [Green Version]
- Valenti, L.; Al-Serri, A.; Daly, A.K.; Galmozzi, E.; Rametta, R.; Dongiovanni, P.; Nobili, V.; Mozzi, E.; Roviaro, G.; Vanni, E.; et al. Homozygosity for the patatin-like phospholipase-3/adiponutrin I148M polymorphism influences liver fibrosis in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1209–1217. [Google Scholar] [CrossRef] [PubMed]
- Fabbrini, E.; Sullivan, S.; Klein, S. Obesity and nonalcoholic fatty liver disease: Biochemical, metabolic, and clinical implications. Hepatology 2010, 51, 679–689. [Google Scholar] [CrossRef]
- Birkenfeld, A.L.; Shulman, G.I. Nonalcoholic fatty liver disease, hepatic insulin resistance, and type 2 diabetes. Hepatology 2014, 59, 713–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesini, G.; Bugianesi, E.; Forlani, G.; Cerrelli, F.; Lenzi, M.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; Melchionda, N.; et al. Nonalcoholic fatty liver, steatohepatitis, and the metabolic syndrome. Hepatology 2003, 37, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, C.; Yu, C.; Xu, L.; Miao, M. Association of serum uric acid level with non-alcoholic fatty liver disease: A cross-sectional study. J. Hepatol. 2009, 50, 1029–1034. [Google Scholar] [CrossRef]
- Xu, C.; Yu, C.; Xu, L.; Miao, M.; Li, Y. High serum uric acid increases the risk for nonalcoholic Fatty liver disease: A prospective observational study. PLoS ONE 2010, 5, e11578. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Cho, Y.K.; Ryan, M.; Kim, H.; Lee, S.W.; Chang, E.; Joo, K.J.; Kim, J.T.; Kim, B.S.; Sung, K.C. Serum uric Acid as a predictor for the development of nonalcoholic Fatty liver disease in apparently healthy subjects: A 5-year retrospective cohort study. Gut Liver 2010, 4, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD. Cardiovascular Disease and Diabetes: Policies for Better Health and Quality of Care, OECD Health Policy Studies; OECD Publishing: Paris, France, 2015. [Google Scholar] [CrossRef] [Green Version]
- Dahlöf, B. Cardiovascular disease risk factors: Epidemiology and risk assessment. Am. J. Cardiol. 2010, 105, 3a–9a. [Google Scholar] [CrossRef] [PubMed]
- Feig, D.I.; Kang, D.H.; Johnson, R.J. Uric acid and cardiovascular risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Bos, M.J.; Koudstaal, P.J.; Hofman, A.; Witteman, J.C.; Breteler, M.M. Uric acid is a risk factor for myocardial infarction and stroke: The Rotterdam study. Stroke 2006, 37, 1503–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermayr, R.P.; Temml, C.; Gutjahr, G.; Knechtelsdorfer, M.; Oberbauer, R.; Klauser-Braun, R. Elevated uric acid increases the risk for kidney disease. J. Am. Soc. Nephrol. 2008, 19, 2407–2413. [Google Scholar] [CrossRef] [Green Version]
- Culleton, B.F.; Larson, M.G.; Kannel, W.B.; Levy, D. Serum uric acid and risk for cardiovascular disease and death: The Framingham Heart Study. Ann. Intern. Med. 1999, 131, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, A.C.; Miname, M.H.; Santos, R.D. Uric acid: A marker of increased cardiovascular risk. Atherosclerosis 2009, 202, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Chuang, S.Y.; Chen, H.J.; Yeh, W.T.; Pan, W.H. Serum uric acid level as an independent risk factor for all-cause, cardiovascular, and ischemic stroke mortality: A Chinese cohort study. Arthritis Rheumatol. 2009, 61, 225–232. [Google Scholar] [CrossRef]
- Zoppini, G.; Targher, G.; Negri, C.; Stoico, V.; Perrone, F.; Muggeo, M.; Bonora, E. Elevated serum uric acid concentrations independently predict cardiovascular mortality in type 2 diabetic patients. Diabetes Care 2009, 32, 1716–1720. [Google Scholar] [CrossRef] [Green Version]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angulo, P. Nonalcoholic fatty liver disease. N. Engl. J. Med. 2002, 346, 1221–1231. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [Green Version]
- WHO Guidelines Approved by the Guidelines Review Committee. In Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010.
- Jee, S.H.; Sull, J.W.; Park, J.; Lee, S.Y.; Ohrr, H.; Guallar, E.; Samet, J.M. Body-Mass index and mortality in Korean men and women. N. Engl. J. Med. 2006, 355, 779–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef]
- Kwon, S.Y.; Na, Y.A. The assessment of framingham risk score and 10 Year CHD risk according to application of LDL cholesterol or total cholesterol. Korean J. Clin. Lab. Sci. 2016, 48, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Huang, L.; Song, M.; Song, Y. Baseline serum uric acid level as a predictor of cardiovascular disease related mortality and all-cause mortality: A meta-analysis of prospective studies. Atherosclerosis 2013, 231, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Strasak, A.M.; Kelleher, C.C.; Brant, L.J.; Rapp, K.; Ruttmann, E.; Concin, H.; Diem, G.; Pfeiffer, K.P.; Ulmer, H. Serum uric acid is an independent predictor for all major forms of cardiovascular death in 28,613 elderly women: A prospective 21-year follow-up study. Int. J. Cardiol. 2008, 125, 232–239. [Google Scholar] [CrossRef]
- Kleber, M.E.; Delgado, G.; Grammer, T.B.; Silbernagel, G.; Huang, J.; Krämer, B.K.; Ritz, E.; März, W. Uric Acid and Cardiovascular Events: A Mendelian Randomization Study. J. Am. Soc. Nephrol. 2015, 26, 2831–2838. [Google Scholar] [CrossRef] [PubMed]
- Kivity, S.; Kopel, E.; Maor, E.; Abu-Bachar, F.; Segev, S.; Sidi, Y.; Olchovsky, D. Association of serum uric acid and cardiovascular disease in healthy adults. Am. J. Cardiol. 2013, 111, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Panoulas, V.F.; Milionis, H.J.; Douglas, K.M.; Nightingale, P.; Kita, M.D.; Klocke, R.; Elisaf, M.S.; Kitas, G.D. Association of serum uric acid with cardiovascular disease in rheumatoid arthritis. Rheumatology 2007, 46, 1466–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, W.B.; Saag, K.G.; Becker, M.A.; Borer, J.S.; Gorelick, P.B.; Whelton, A.; Hunt, B.; Castillo, M.; Gunawardhana, L. Cardiovascular Safety of Febuxostat or Allopurinol in Patients with Gout. N. Engl. J. Med. 2018, 378, 1200–1210. [Google Scholar] [CrossRef]
- Beardmore, T.D.; Kelley, W.N. Mechanism of allopurinol-mediated inhibition of pyrimidine biosynthesis. J. Lab. Clin. Med. 1971, 78, 696–704. [Google Scholar]
- Takano, Y.; Hase-Aoki, K.; Horiuchi, H.; Zhao, L.; Kasahara, Y.; Kondo, S.; Becker, M.A. Selectivity of febuxostat, a novel non-purine inhibitor of xanthine oxidase/xanthine dehydrogenase. Life Sci. 2005, 76, 1835–1847. [Google Scholar] [CrossRef]
- Pritsos, C.A. Cellular distribution, metabolism and regulation of the xanthine oxidoreductase enzyme system. Chem. Biol. Interact. 2000, 129, 195–208. [Google Scholar] [CrossRef]
- Lanaspa, M.A.; Sanchez-Lozada, L.G.; Choi, Y.J.; Cicerchi, C.; Kanbay, M.; Roncal-Jimenez, C.A.; Ishimoto, T.; Li, N.; Marek, G.; Duranay, M.; et al. Uric acid induces hepatic steatosis by generation of mitochondrial oxidative stress: Potential role in fructose-dependent and -independent fatty liver. J. Biol. Chem. 2012, 287, 40732–40744. [Google Scholar] [CrossRef] [Green Version]
- Kushiyama, A.; Nakatsu, Y.; Matsunaga, Y.; Yamamo.otoya, T.; Mori, K.; Ueda, K.; Inoue, Y.; Sakoda, H.; Fujishiro, M.; Ono, H.; et al. Role of Uric Acid Metabolism-Related Inflammation in the Pathogenesis of Metabolic Syndrome Components Such as Atherosclerosis and Nonalcoholic Steatohepatitis. Mediat. Inflamm. 2016, 2016, 8603164. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R. Insulin resistance, inflammation, and non-alcoholic fatty liver disease. Trends Endocrinol. Metab. 2008, 19, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Marra, F.; Marchesini, G. Increased risk of cardiovascular disease in non-alcoholic fatty liver disease: Causal effect or epiphenomenon? Diabetologia 2008, 51, 1947–1953. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Arcaro, G. Non-Alcoholic fatty liver disease and increased risk of cardiovascular disease. Atherosclerosis 2007, 191, 235–240. [Google Scholar] [CrossRef]
- Edens, M.A.; Kuipers, F.; Stolk, R.P. Non-Alcoholic fatty liver disease is associated with cardiovascular disease risk markers. Obes. Rev. 2009, 10, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Sheth, S.G.; Gordon, F.D.; Chopra, S. Nonalcoholic steatohepatitis. Ann. Intern. Med. 1997, 126, 137–145. [Google Scholar] [CrossRef]
- Froehlich, F.; Lamy, O.; Fried, M.; Gonvers, J.J. Practice and complications of liver biopsy. Results of a nationwide survey in Switzerland. Dig. Dis. Sci. 1993, 38, 1480–1484. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Hernaez, R.; Lazo, M.; Bonekamp, S.; Kamel, I.; Brancati, F.L.; Guallar, E.; Clark, J.M. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: A meta-analysis. Hepatology 2011, 54, 1082–1090. [Google Scholar] [CrossRef] [Green Version]
- Dasarathy, S.; Dasarathy, J.; Khiyami, A.; Joseph, R.; Lopez, R.; McCullough, A.J. Validity of real time ultrasound in the diagnosis of hepatic steatosis: A prospective study. J. Hepatol. 2009, 51, 1061–1067. [Google Scholar] [CrossRef]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B., Sr.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, K.J.; Jang, Y.; Oh, D.J.; Oh, B.H.; Lee, S.H.; Park, S.W.; Seung, K.B.; Kim, H.K.; Yun, Y.D.; Choi, S.H.; et al. The ACC/AHA 2013 pooled cohort equations compared to a Korean Risk Prediction Model for atherosclerotic cardiovascular disease. Atherosclerosis 2015, 242, 367–375. [Google Scholar] [CrossRef]
- Chia, Y.C.; Lim, H.M.; Ching, S.M. Validation of the pooled cohort risk score in an Asian population-a retrospective cohort study. BMC Cardiovasc. Disord. 2014, 14, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selvarajah, S.; Kaur, G.; Haniff, J.; Cheong, K.C.; Hiong, T.G.; van der Graaf, Y.; Bots, M.L. Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population. Int. J. Cardiol. 2014, 176, 211–218. [Google Scholar] [CrossRef] [Green Version]
- Chia, Y.C.; Gray, S.Y.; Ching, S.M.; Lim, H.M.; Chinna, K. Validation of the Framingham general cardiovascular risk score in a multiethnic Asian population: A retrospective cohort study. BMJ Open 2015, 5, e007324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khalidi, B.; Kimball, S.M.; Rotondi, M.A.; Ardern, C.I. Standardized serum 25-hydroxyvitamin D concentrations are inversely associated with cardiometabolic disease in U.S. adults: A cross-sectional analysis of NHANES, 2001–2010. Nutr. J. 2017, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Færch, K.; Bergman, B.; Perreault, L. Does insulin resistance drive the association between hyperglycemia and cardiovascular risk? PLoS ONE 2012, 7, e39260. [Google Scholar] [CrossRef] [Green Version]
- Bellanti, F.; Romano, A.D.; Lo Buglio, A.; Castriotta, V.; Guglielmi, G.; Greco, A.; Serviddio, G.; Vendemiale, G. Oxidative stress is increased in sarcopenia and associated with cardiovascular disease risk in sarcopenic obesity. Maturitas 2018, 109, 6–12. [Google Scholar] [CrossRef]
- Kim, J.H.; Cho, J.J.; Park, Y.S. Relationship between sarcopenic obesity and cardiovascular disease risk as estimated by the Framingham risk score. J. Korean Med. Sci. 2015, 30, 264–271. [Google Scholar] [CrossRef] [Green Version]
- Byeon, C.H.; Kang, K.Y.; Kang, S.H.; Bae, E.J. Sarcopenia is associated with Framingham risk score in the Korean population: Korean National Health and Nutrition Examination Survey (KNHANES) 2010–2011. J. Geriatr. Cardiol. 2015, 12, 366–372. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Quartile 1 (n = 3089) | Quartile 2 (n = 2537) | Quartile 3 (n = 2906) | Quartile 4 (n = 2628) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 52.8 ± 0.2 | 53.1 ± 0.3 | 53.8 ± 0.3 | 51.9 ± 0.3 | <0.001 |
| 30–39 | 496 (18.3) | 420 (19.7) | 440 (18.8) | 511 (25.4) | <0.001 |
| 40–49 | 713 (27.4) | 518 (23.3) | 526 (21.8) | 492 (23.0) | |
| 50–59 | 671 (16.4) | 569 (25.1) | 649 (25.9) | 481 (21.3) | |
| 60–69 | 638 (16.4) | 538 (17.8) | 640 (17.6) | 512 (14.9) | |
| ≥70 | 571 (14.2) | 492 (14.1) | 651 (15.9) | 632 (15.4) | |
| SEX Female | 2745 (88.3) | 2067 (78.6) | 1731 (54.8) | 637 (19.3) | <0.001 |
| Education ≤Elementary school | 767 (20.6) | 569 (17.7) | 627 (16.3) | 480 (12.4) | <0.001 |
| Middle school | 382 (10.6) | 343 (13.2) | 387 (11.4) | 283 (8.8) | |
| High school | 872 (31.0) | 699 (30.2) | 829 (29.9) | 706 (26.8) | |
| ≥College | 1068 (37.8) | 926 (38.9) | 1063 (42.5) | 1159 (52.0) | |
| Household income (quartile) | <0.001 | ||||
| 1/4 | 654 (17.9) | 502 (16.6) | 598 (16.6) | 538 (14.9) | |
| 2/4 | 750 (23.5) | 652 (26.0) | 708 (23.6) | 641 (22.6) | |
| 3/4 | 840 (29.3) | 711 (30.5) | 768 (28.3) | 688 (29.0) | |
| 4/4 | 845 (29.2) | 672 (26.9) | 832 (31.5) | 761 (33.4) | |
| Physical activity Yes | 353 (12.2) | 334 (12.9) | 408 (15.9) | 400 (17.2) | <0.001 |
| Obesity (BMI, kg/m2) | 23.1 ± 0.1 | 23.8 ± 0.1 | 24.5 ± 0.1 | 25.7 ± 0.1 | <0.001 |
| Normal (<25) | 2329 (75.7) | 1727 (68.3) | 1692 (59.5) | 1194 (43.1) | <0.001 |
| Obese (≥25) | 760 (24.3) | 810 (31.7) | 1214 (40.5) | 1434 (56.9) | |
| Dyslipidaemia Yes | 659 (18.9) | 568 (19.8) | 670 (21.5) | 568 (19.2) | 0.105 |
| Chronic kidney disease No | 3086 (99.9) | 2533 (99.9) | 2898 (99.8) | 2612 (99.6) | 0.026 |
| Smoking status | <0.001 | ||||
| Never smoker | 2671 (86.0) | 2014 (76.7) | 1875 (62.0) | 1128 (41.7) | |
| Past smoker | 256 (8.0) | 288 (11.5) | 655 (23.1) | 914 (32.9) | |
| Current smoker | 162 (6.0) | 235 (11.8) | 376 (14.9) | 586 (25.4) | |
| Hypertension | 0.001 | ||||
| Yes | 925 (26.1) | 798 (27.7) | 1083 (33.1) | 1189 (40.4) | |
| Diabetes mellitus | 0.019 | ||||
| Yes | 430 (12.5) | 331 (11.9) | 471 (15.0) | 422 (13.0) | |
| Cardiovascular disease risk | <0.001 | ||||
| ≥20% | 368 (9.9) | 388 (12.8) | 647 (17.4) | 813 (23.3) | |
| <20% | 2721 (90.1) | 2149 (87.2) | 2259 (82.6) | 1815 (76.7) |
| Variables | Low CVD Risk Group (<20%) (n = 8944) | High CVD Risk Group (≥20%) (n = 2216) | p-Value |
|---|---|---|---|
| Age (years) | 49.9 ± 0.1 | 68.7 ± 0.2 | <0.001 |
| 30–39 | 1867 (100) | 0 (0) | <0.001 |
| 40–49 | 2222 (98.4) | 27 (1.6) | |
| 50–59 | 2136 (88.9) | 234 (11.1) | |
| 60–69 | 1729 (73.0) | 599 (27.0) | |
| ≥70 | 930 (44.1) | 1356 (55.9) | |
| Sex Female | 6489 (92.4) | 691 (7.6) | <0.001 |
| Education ≤Elementary school | 1502 (64.0) | 941 (36.0) | <0.001 |
| Middle school | 994 (74.0) | 401 (26.0) | |
| High school | 2580 (86.2) | 526 (13.8) | |
| ≥College | 3868 (93.1) | 348 (6.9) | |
| Household income (quartile) | <0.001 | ||
| 1/4 | 1342 (62.9) | 950 (37.1) | |
| 2/4 | 2183 (83.3) | 568 (16.7) | |
| 3/4 | 2605 (89.3) | 402 (10.7) | |
| 4/4 | 2814 (91.3) | 296 (8.7) | |
| Physical activity Yes | 1314 (90.3) | 181 (9.7) | <0.001 |
| Obesity (BMI, kg/m2) | 24.2 ± 0.0 | 24.9 ± 0.1 | <0.001 |
| Normal (<25) | 5749 (86.5) | 1193 (13.5) | <0.001 |
| Obese (≥25) | 3195 (80.2) | 1023 (19.8) | |
| Dyslipidemia Yes | 1737 (73.5) | 728 (26.5) | <0.001 |
| Chronic kidney disease No | 8925 (84.2) | 2204 (15.8) | <0.001 |
| Smoking status | <0.001 | ||
| Never smoker | 6764 (90.4) | 924 (9.6) | |
| Past smoker | 1341 (73.0) | 772 (27.0) | |
| Current smoker | 839 (69.8) | 520 (30.2) | |
| Hypertension Yes | 2307 (62.0) | 1688 (38.0) | <0.001 |
| Diabetes mellitus Yes | 674 (45.2) | 980 (54.8) | <0.001 |
| Serum uric acid (quartile) | 4.7 (3.9–5.7) | 5.3 (4.4–6.3) | <0.001 |
| 1/4 | 2721 (90.1) | 368 (9.9) | <0.001 |
| 2/4 | 2149 (87.2) | 388 (12.8) | |
| 3/4 | 2259 (82.6) | 647 (17.4) | |
| 4/4 | 1815 (76.7) | 813 (23.3) |
| Crude Model | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Serum uric acid (per 1 mg/dL) | 1.31 (1.26–1.37) | <0.001 | 1.44 (1.38–1.51) | <0.001 | 1.10 (1.02–1.19) | 0.018 |
| Serum Uric Acid (Quartile, mg/dL) | Crude Model | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Q1 (<4.1) | Ref. | Ref. | Ref. | |||
| Q2 (4.1–4.7) | 1.33 (1.11–1.60) | 0.002 | 1.43 (1.18–1.72) | <0.001 | 1.38 (1.03–1.86) | 0.033 |
| Q3 (4.8–5.7) | 1.91 (1.62–2.25) | <0.001 | 2.26 (1.90–2.69) | <0.001 | 1.19 (0.90–1.59) | 0.227 |
| Q4 (≥5.8) | 2.76 (2.34–3.25) | <0.001 | 4.01 (3.37–4.78) | <0.001 | 1.44 (1.07–1.94) | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Kang, K.; Sheol, H.; Shin, J.; Sim, Y.; Yang, T.; Hwang, J.; Lee, J.-M. The Association between Serum Uric Acid Levels and 10-Year Cardiovascular Disease Risk in Non-Alcoholic Fatty Liver Disease Patients. Int. J. Environ. Res. Public Health 2022, 19, 1042. https://doi.org/10.3390/ijerph19031042
Kim K, Kang K, Sheol H, Shin J, Sim Y, Yang T, Hwang J, Lee J-M. The Association between Serum Uric Acid Levels and 10-Year Cardiovascular Disease Risk in Non-Alcoholic Fatty Liver Disease Patients. International Journal of Environmental Research and Public Health. 2022; 19(3):1042. https://doi.org/10.3390/ijerph19031042
Chicago/Turabian StyleKim, Kiduk, Kyoonho Kang, Hyewon Sheol, Jihae Shin, Youngseo Sim, Taehoon Yang, Jeongwon Hwang, and Ju-Mi Lee. 2022. "The Association between Serum Uric Acid Levels and 10-Year Cardiovascular Disease Risk in Non-Alcoholic Fatty Liver Disease Patients" International Journal of Environmental Research and Public Health 19, no. 3: 1042. https://doi.org/10.3390/ijerph19031042
APA StyleKim, K., Kang, K., Sheol, H., Shin, J., Sim, Y., Yang, T., Hwang, J., & Lee, J.-M. (2022). The Association between Serum Uric Acid Levels and 10-Year Cardiovascular Disease Risk in Non-Alcoholic Fatty Liver Disease Patients. International Journal of Environmental Research and Public Health, 19(3), 1042. https://doi.org/10.3390/ijerph19031042