

The Effect of Breaking Up Sedentary Time with Calisthenics on Neuromuscular Function: A Preliminary Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.3. Accelerometry
2.4. Measures of Neuromuscular Function
2.5. Calisthenics Intervention
2.6. Data Analysis
2.7. Statistics
3. Results
3.1. Participant Physical and Sedentary Behaviour Characteristics
3.2. Sedentary Behaviour
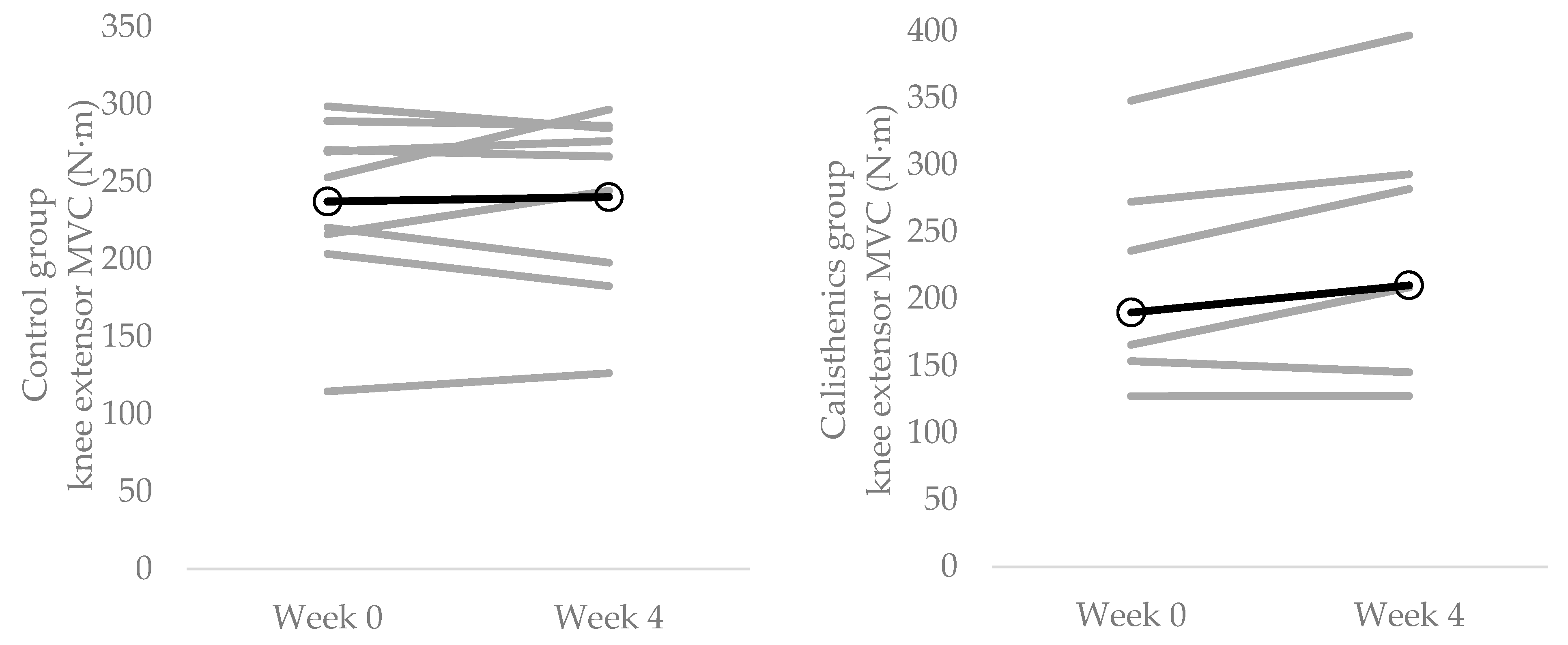
3.3. Muscle Strength
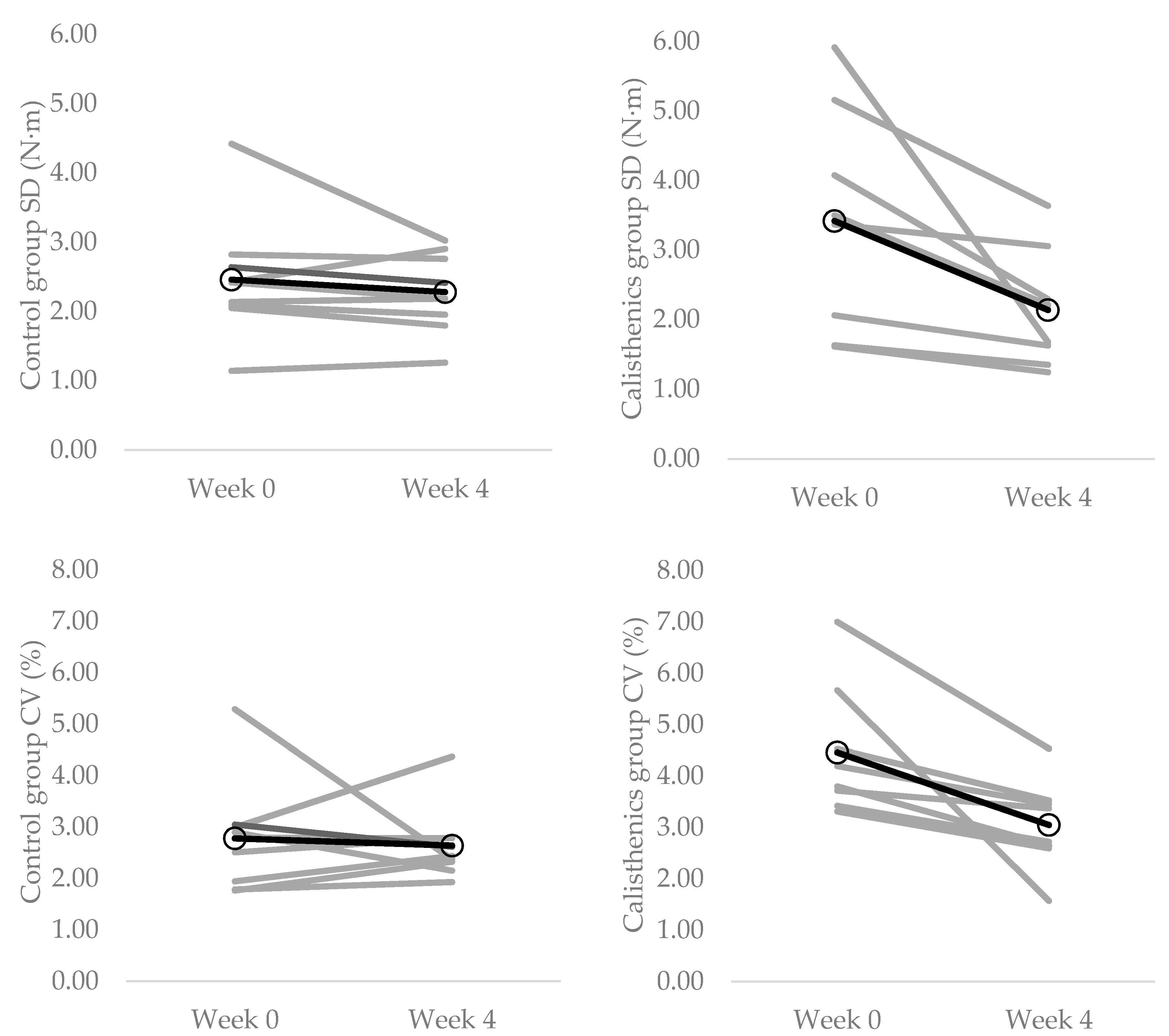
3.4. Muscle Force Control Strength
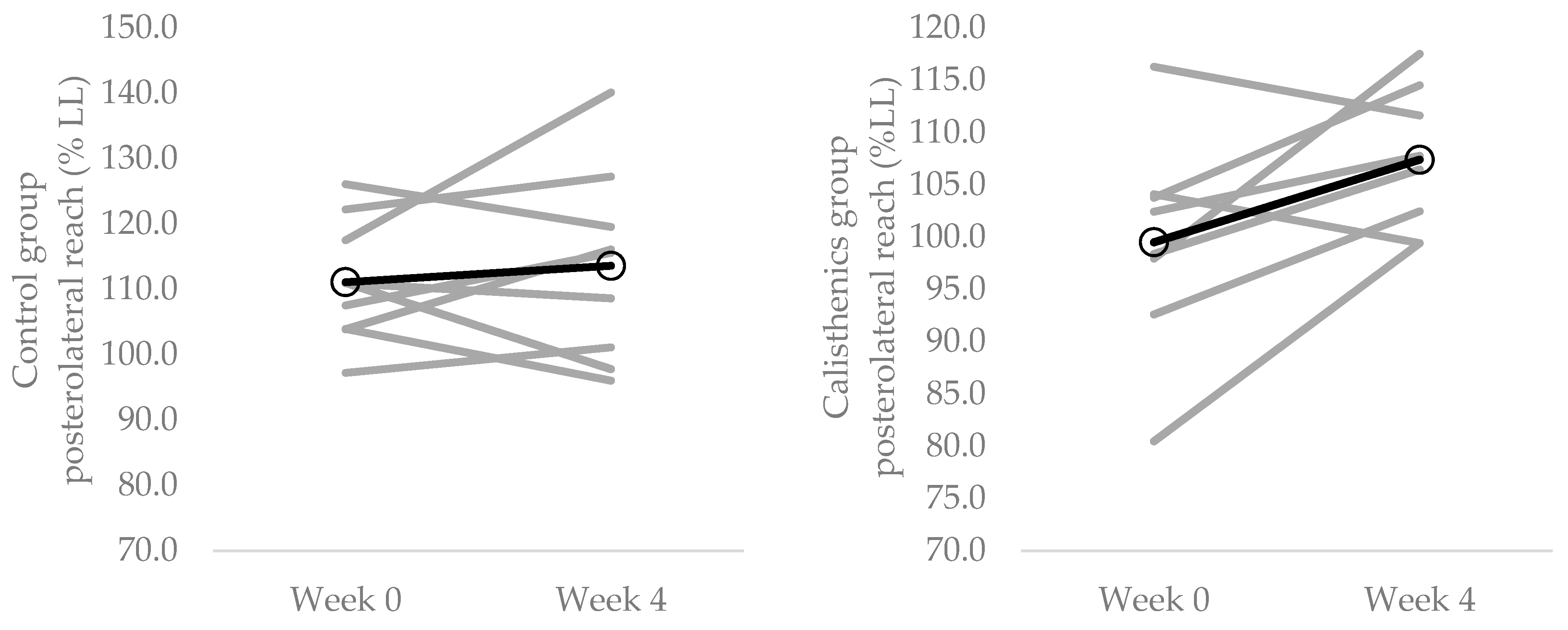
3.5. Dynamic Balance
4. Discussion
4.1. Effect of Calisthenics on Neuromuscular Function
4.2. Limitations and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volpi, E.; Nazemi, R.; Fujita, S. Muscle tissue changes with aging. Curr. Opin. Clin. Nutr. Metab. Care 2004, 7, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Hunter, K.; Pereira, H.M.; Keenan, K.G. The aging neuromuscular system and motor performance. J. Appl. Physiol. 2016, 121, 982–995. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Howard, B.; Healy, G.N.; Owen, N. Too much sitting—A health hazard. Diabetes Res. Clin. Pract. 2012, 97, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary behavior research network (SBRN)—Terminology consensus and project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in sedentary time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef]
- Parry, S.; Straker, L.; Gilson, N.D.; Smith, A.J. Participatory workplace interventions can reduce sedentary time for office workers—A randomised controlled trial. PLoS ONE 2013, 8, e78957. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendelton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical activity change during COVID-19 confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Rodriguez-Almagro, J.; Onieva-Zafram, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.D.C.; Hernández-Martinez, A. Physical activity and sedentary lifestyle in university students: Changes during confinement due to the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef]
- Hamilton, M.T. The role of skeletal muscle contractile duration throughout the whole day: Reducing sedentary time and promoting universal physical activity in all people. J. Physiol. 2018, 596, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Comp. Physiol. 2012, 2, 1132–1211. [Google Scholar]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Koster, A.; Caserotti, P.; Patel, K.V.; Matthews, C.E.; Berrigan, D.; Van Domelen, D.R.; Brychta, R.J.; Chen, K.Y.; Harris, T.B. Association of sedentary time with mortality independent of moderate to vigorous physical activity. PLoS ONE 2012, 7, e37696. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Baumann, A.; Lee, I.M.; Series, L.P.A.; Lancet Sedentary Behaviour Working Group. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Adams, G.R.; Hather, B.M.; Dudley, G.A. Effect of short-term unweighting on human skeletal muscle strength and size. Aviat. Space Environ. Med. 1994, 65, 1116–1121. [Google Scholar]
- Clark, B.C.; Manini, T.M.; Bolanowski, S.J.; Ploutz-Snyder, L.L. Adaptations in human neuromuscular function following prolonged unweighting: II. Neurological properties and motor imagery efficacy. J. Appl. Physiol. 2006, 101, 264–272. [Google Scholar] [CrossRef]
- Duchateau, J.; Hainaut, K. Effects of immobilization on contractile properties, recruitment and firing rates of human motor units. J. Physiol. 1990, 422, 55–65. [Google Scholar] [CrossRef]
- Seki, K.; Taniguchi, Y.; Narusawa, M. Effects of joint immobilization on firing rate modulation of human motor units. J. Physiol. 1990, 530, 507–519. [Google Scholar] [CrossRef]
- Volkers, K.M.; de Kieviet, J.F.; Wittingen, H.P.; Scherder, E.J.A. Lower limb muscle strength (LLMS): Why sedentary life should never start? A review. Arch. Geront. Geriatr. 2012, 54, 399–414. [Google Scholar] [CrossRef]
- Hamer, M.; Stamatakis, E. Screen-based sedentary behavior, physical activity, and muscle strength in the English longitudinal study of ageing. PLoS ONE 2013, 8, e66222. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Pierce, J.R.; Manini, T.M.; Ploutz-Snyder, L.L. Effect of prolonged unweighting of human skeletal muscle on neuromotor force control. Eur. J. Appl. Physiol. 2007, 100, 53–62. [Google Scholar] [PubMed]
- Pijnappels, M.; van der Burg, J.C.E.; Reeves, N.D.; van Dieën, J. Identification of elderly fallers by muscle strength measures. Eur. J. Appl. Physiol. 2008, 102, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Allet, L.; Kim, H.; Ashton-Miller, J.; De Mott, T.; Richardson, J.K. Frontal plane hip and ankle sensorimotor function, not age, predicts unipedal stance time. Muscle Nerve 2012, 45, 578–585. [Google Scholar] [PubMed]
- Davis, L.A.; Allen, S.P.; Hamilton, L.D.; Grabowski, A.M.; Enoka, R.M. Differences in postural sway among healthy adults are associated with the ability to perform steady contractions with leg muscles. Exp. Brain Res. 2020, 238, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Mear, E.; Gladwell, V.; Pethick, J. Knee extensor force control as a predictor of dynamic balance. SportRχiv 2022. [Google Scholar] [CrossRef]
- Enoka, R.M.; Farina, D. Force steadiness: From motor units to voluntary actions. Physiology 2021, 36, 114–130. [Google Scholar]
- Davis, M.G.; Fox, K.R.; Stathi, A.; Travers, T.; Thompson, J.L.; Cooper, A.R. Objectively measured sedentary time and its association with physical function in older adults. J. Aging Phys. Act. 2013, 22, 474–481. [Google Scholar] [CrossRef]
- Willoughby, T.; Copeland, J.L. Sedentary time is not independently related to postural stability or leg strength in women 50–67 years old. Appl. Physiol. Nutr. Metab. 2015, 40, 1123–1128. [Google Scholar]
- Caplan, N.; Forbes, A.; Radha, S.; Stewart, S.; Ewen, A.; Gibson, A.S.C.; Kader, D. Effects of 1 week of unilateral ankle immobilization on plantar-flexor strength, balance, and walking speed: A pilot study in asymptomatic volunteers. J. Sport Rehabil. 2015, 24, 156–162. [Google Scholar]
- Carter, S.E.; Jones, M.; Gladwell, V.F. Energy expenditure and heart rate responses to breaking up sedentary time with three different physical activity interventions. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Thosar, S.S.; Bielko, S.L.; Mather, K.J.; Johnston, J.D.; Wallace, J.P. Effect of prolonged sitting and breaks in sitting time on endothelial function. Med. Sci. Sports Exerc. 2015, 47, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.N.; Kingwell, B.A.; Sethi, P.; Cerin, E.; Owen, N.; Dunstan, D.W. Breaking up prolonged sitting reduces resting blood pressure in overweight/obese adults. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Bergouignan, A.; Latouche, C.; Heywood, S.; Grace, M.S.; Reddy-Luthmoodoo, M.; Natoli, A.K.; Owen, N.; Dunstan, D.W.; Kingwell, B.A. Frequent interruptions of sedentary time modulates contraction-and insulin-stimulated glucose uptake pathways in muscle: Ancillary analysis from randomized clinical trials. Sci. Rep. 2016, 6, 32004. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Kingwell, B.A.; Owen, N.; Dunstan, D.W. Breaking up workplace sitting time with intermittent standing bouts improves fatigue and musculoskeletal discomfort in overweight/obese office workers. Occup. Environ. Med. 2014, 71, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T. Standing and mortality in a prospective cohort of Canadian adults. Med. Sci. Sports Exerc. 2014, 46, 940–946. [Google Scholar] [CrossRef]
- Bull, F.C.; Biddle, S.; Buchner, D.; Ferguson, R.; Foster, C.; Fox, K.; Haskell, B.; Mutrie, N. Physical Activity Guidelines in the UK: Review and Recommendations; School of Sport, Exercise and Health Sciences, Loughborough University: Loughborough, UK, 2010; pp. 1–72. [Google Scholar]
- Brown, W.J.; Bauman, A.E.; Bull, F.C.; Burton, N.W. Development of Evidence-Based Physical Activity Recommendations for Adults (18–64 Years); Australian Government Department of Health: Canberra, Australia, 2012. [Google Scholar]
- World Health Organization. Physical Activity. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 20 September 2022).
- Latouche, C.; Jowett, J.B.; Carey, A.L.; Bertovic, D.A.; Owen, N.; Dunstan, D.W.; Kingwell, B.A. Effects of breaking up prolonged sitting on skeletal muscle gene expression. J. Appl. Physiol. 2013, 114, 453–460. [Google Scholar] [CrossRef]
- Carr, L.J.; Walaska, K.A.; Marcus, B.H. Feasibility of a portable pedal exercise machine for reducing sedentary time in the workplace. Br. J. Sports Med. 2012, 46, 430–435. [Google Scholar] [CrossRef]
- Carter, S.E.; Gladwell, V.F. Effect of breaking up sedentary time with callisthenics on endothelial function. J. Sports Sci. 2017, 35, 1508–1514. [Google Scholar] [CrossRef]
- Harrington, D.M.; Welk, G.J.; Donnelly, A.E. Validation of MET estimates and step measurement using the ActivPAL physical activity logger. J. Sports Sci. 2011, 29, 627–633. [Google Scholar] [CrossRef]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Ringhof, S.; Stein, T. Biomechanical assessment of dynamic balance: Specificity of different balance tests. Hum. Mov. Sci. 2018, 58, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The reliability of an instrumented device for measuring components of the Star Excursion Balance Test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar] [PubMed]
- Hertel, J.; Miller, S.; Denegar, C. Intratester and intertester reliability during the Star Excursion Balance Test. J. Sport Rehabil. 2000, 9, 104–116. [Google Scholar] [CrossRef]
- Coughlan, G.T.; Fullam, K.; Delahunt, E.; Gissane, C.; Caulfield, B.M. A comparison between performance on selected direction of the Star Excursion Balance Test and the Y Balance Test. J. Athl. Train. 2012, 47, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Kern, D.S.; Semmler, J.G.; Enoka, R.M. Long-term activity in the upper and lower-limb muscles of humans. J. Appl. Physiol. 2001, 91, 2224–2232. [Google Scholar] [CrossRef]
- Pethick, J.; Winter, S.L.; Burnley, M. Fatigue-induced changes in knee-extensor torque complexity and muscle metabolic rate are dependent on joint angle. Eur. J. Appl. Physiol. 2021, 121, 3117–3131. [Google Scholar] [CrossRef]
- Hoffman, J. Physiological Aspects of Sport Training and Performance; Human Kinetics: Champaign, IL, USA, 2002. [Google Scholar]
- Gribble, P.A.; Hertel, J. Considerations for normalizing measures of the Star Excursion Balance Test. Meas. Phys. Ed. Exerc. Sci. 2003, 7, 89–100. [Google Scholar] [CrossRef]
- Pethick, J.; Winter, S.L.; Burnley, M. Did you know? Using entropy and fractal geometry to quantify fluctuations in physiological outputs. Acta Physiol. Scand. 2021, 233, e13670. [Google Scholar] [CrossRef]
- Pethick, J.; Winter, S.L.; Burnley, M. Physiological complexity: Influence of ageing, disease and neuromuscular fatigue on muscle force and torque fluctuations. Exp. Physiol. 2021, 106, 2046–2059. [Google Scholar] [CrossRef]
- Enoka, R.M.; Christou, E.A.; Hunter, S.K.; Kornatz, K.W.; Semmler, J.G.; Taylor, A.M.; Tracy, B.L. Mechanisms that contribute to differences in motor performance between young and old adults. J. Electromyogr. Kinesiol. 2003, 13, 1–12. [Google Scholar] [CrossRef]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.K.; Buldyrev, S.V.; Havlin, S.; Simons, M.; Stanley, H.E.; Goldberger, A.L. Mosaic organization of DNA nucleotides. Phys. Rev. E 1991, 49, 1685–1689. [Google Scholar] [CrossRef] [PubMed]
- Pethick, J.; Winter, S.L.; Burnley, M. Fatigue reduces the complexity of knee extensor torque fluctuations during maximal and submaximal intermittent isometric contractions in man. J. Physiol. 2015, 593, 2085–2096. [Google Scholar] [CrossRef] [PubMed]
- Benatti, F.B.; Ried-Larsen, M. The effects of breaking up prolonged sitting time: A review of experimental studies. Med. Sci. Sports Exerc. 2015, 47, 2053–2061. [Google Scholar] [CrossRef]
- del Pozo-Cruz, J.; García-Hermoso, A.; Alfonso-Rosa, R.M.; Alvarez-Barbosa, F.; Owen, N.; Chastin, S.; del Pozo-Cruz, B. Replacing sedentary time: Meta-analysis of objective-assessment studies. Am. J. Prev. Med. 2018, 55, 395–402. [Google Scholar] [CrossRef]
- Sardinha, L.B.; Ekelund, U.; dos Santos, L.; Cyrino, E.S.; Silva, A.M.; Santos, D. Breaking-up sedentary time is associated with impairment in activities of daily living. Exp. Gerontol. 2015, 72, 57–62. [Google Scholar] [CrossRef]
- Jönhagen, S.; Halvorsen, K.; Benoit, D.L. Muscle activation and length changes during two lunge exercises: Implications for rehabilitation. Scand. J. Med. Sci. Sports 2009, 19, 561–568. [Google Scholar] [CrossRef]
- Slater, L.V.; Hart, J.M. Muscle activation patterns during different squat techniques. J. Strength Cond. Res. 2017, 31, 667–676. [Google Scholar] [CrossRef]
- Kotarsky, C.J.; Christensen, B.K.; Miller, J.S.; Hackney, K.J. Effect of progressive calisthenic push-up training on muscle strength and thickness. J. Strength Cond. Res. 2018, 32, 651–659. [Google Scholar] [CrossRef]
- Del Vecchio, A.; Casolo, A.; Negro, F.; Scorcellati, M.; Bazzuchi, I.; Enoka, R.; Felici, F.; Farina, D. The increase in muscle force after 4 weeks of strength training is mediated by adaptations in motor unit recruitment and rate coding. J. Physiol. 2019, 597, 1873–1887. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Xia, J.; Gathirua-Mwangi, W.M.; Guo, J.; Li, Y.; McKenzie, S.; Song, Y. Associations of muscle mass and strength with all-cause mortality among US older adults. Med. Sci. Sports Exerc. 2018, 50, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D. Lower extremity muscular strength, sedentary behavior, and mortality. Age 2016, 38, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.D.; Dingwell, J. Separating the effects of age and walking speed on gait variability. Gait Posture 2008, 27, 572–577. [Google Scholar] [CrossRef]
- Keogh, J.W.; Morrison, S.; Barrett, R. Strength training improves tri-digit finger pinch force control of older adults. Arch. Phys. Med. Rehabil. 2007, 88, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Isear, J.A., Jr.; Erickson, J.C.; Worrell, T.W. EMG analysis of lower extremity muscle recruitment patterns during an unloaded squat. Med. Sci Sports Exerc. 1997, 29, 532–539. [Google Scholar] [CrossRef]
- Lockie, R.G.; Schultz, A.B.; Callaghan, S.J.; Jeffriess, M.D. The effects of isokinetic knee extensor and flexor strength on dynamic stability as measured by functional reaching. Isokinet. Exerc. Sci. 2013, 21, 301–309. [Google Scholar] [CrossRef]
- Benis, R.; Bonato, M.; La Torre, A. Elite female basketball players’ body-weight neuromuscular training and performance on the Y-balance test. J. Athl. Train. 2016, 51, 688–695. [Google Scholar] [CrossRef]
- Xiong, J.; Li, S.; Cao, A.; Qian, L.; Peng, B.; Xiao, D. Effects of integrative neuromuscular training intervention on physical performance in elite female table tennis players: A randomized controlled trial. PLoS ONE 2022, 17, e0262775. [Google Scholar] [CrossRef]
- Parry, S.; Straker, L. The contribution of office work to sedentary behaviour associated risk. BMC Public Health 2013, 13, 296. [Google Scholar] [CrossRef]
- Piasecki, M.; Ireland, A.; Jones, D.A.; McPhee, J.S. Age-dependent motor unit remodelling in human limb muscles. Biogerontology 2016, 17, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Pethick, J.; Taylor, M.J.D.; Harridge, S.D.R. Aging and skeletal muscle force control: Current perspectives and future directions. Scand. J. Med. Sci. Sports 2022, 32, 1430–1433. [Google Scholar] [CrossRef] [PubMed]
- Leightley, D.; Yap, M.H.; Coulson, J.; Piasecki, M.; Cameron, J.; Barnouin, Y.; Tobias, J.; McPhee, J.S. Postural stability during standing balance and sit-to-stand in master athlete runners compared with nonathletic old and young adults. J. Aging Phys. Act. 2017, 25, 345–350. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control (n = 9) | Intervention (n = 8) | |
|---|---|---|
| Age (years) | 29.9 ± 9.7 | 37.4 ± 15.8 |
| Height (m) | 1.74 ± 0.07 | 1.71 ± 0.12 |
| Body mass (kg) | 81.7 ± 22.7 | 71.6 ± 22.6 |
| Daily sitting time (hours) week 0 | 10.7 ± 1.7 | 9.1 ± 2.7 |
| Daily sitting time (hours) week 4 | 9.3 ± 1.4 | 10.3 ± 1.1 |
| Daily steps week 0 | 8354 ± 4919 | 7948 ± 3591 |
| Daily steps week 4 | 7759 ± 4068 | 8456 ± 3720 |
| Control | Intervention | |||
|---|---|---|---|---|
| Week 0 | Week 4 | Week 0 | Week 4 | |
| MVC (N·m) | 237.4 ± 53.7 | 240.3 ± 58.5 | 189.8 ± 87.6 | 210.2 ± 104.6 |
| SD | ||||
| 10% MVC (N·m) | 0.87 ± 0.20 | 0.86 ± 0.13 | 0.83 ± 0.33 | 0.79 ± 0.24 |
| 20% MVC (N·m) | 1.24 ± 0.19 | 1.16 ± 0.23 | 1.37 ± 0.47 | 1.27 ± 0.85 |
| 40% MVC (N·m) | 2.46 ± 0.88 | 2.28 ± 0.57 | 3.41 ± 1.60 | 2.14 ± 0.85 |
| CV | ||||
| 10% MVC (%) | 3.81 ± 0.69 | 3.71 ± 1.03 | 4.29 ± 0.99 | 4.17 ± 0.81 |
| 20% MVC (%) | 2.97 ± 0.97 | 2.78 ± 0.64 | 3.74 ± 1.00 | 3.49 ± 1.09 |
| 40% MVC (%) | 2.78 ± 107 | 2.64 ± 0.71 | 4.46 ± 1.27 | 3.05 ± 0.87 |
| ApEn | ||||
| 10% MVC | 0.83 ± 0.12 | 0.78 ± 0.03 | 0.85 ± 0.10 | 0.80 ± 0.08 |
| 20% MVC | 0.73 ± 0.13 | 0.71 ± 0.05 | 0.76 ± 0.14 | 0.70 ± 0.10 |
| 40% MVC | 0.59 ± 0.09 | 0.60 ± 0.05 | 0.52 ± 0.17 | 0.58 ± 0.09 |
| DFA α | ||||
| 10% MVC | 1.04 ± 0.07 | 0.99 ± 0.06 | 1.00 ± 0.10 | 1.03 ± 0.21 |
| 20% MVC | 1.16 ± 0.07 | 1.10 ± 0.05 | 1.14 ± 0.11 | 1.13 ± 0.14 |
| 40% MVC | 1.30 ± 0.05 | 1.25 ± 0.05 | 1.29 ± 0.09 | 1.23 ± 0.08 |
| Y balance test (left stance) | ||||
| Anterior reach (% LL) | 65.4 ± 10.0 | 64.8 ± 8.0 | 62.1 ± 6.3 | 63.3 ± 6.1 |
| Posteromedial reach (% LL) | 111.5 ± 14.3 | 115.4 ± 16.3 | 102.9 ± 10.3 | 106.9 ± 6.9 |
| Posterolateral reach (% LL) | 111.1 ± 8.9 | 113.6 ± 14.5 | 99.5 ± 10.3 | 107.4 ± 6.8 |
| Composite reach (% LL) | 104.2 ± 11.3 | 106.4 ± 14.3 | 97.7 ± 11.6 | 102.4 ± 6.5 |
| Y balance test (right stance) | ||||
| Anterior reach (% LL) | 64.5 ± 6.5 | 64.5 ± 6.3 | 60.9 ± 5.6 | 64.2 ± 4.8 |
| Posteromedial reach (% LL) | 113.7 ± 14.1 | 112.8 ± 14.6 | 106.4 ± 7.7 | 107.8 ± 6.3 |
| Posterolateral reach (% LL) | 112.0 ± 12.6 | 111.4 ± 14.9 | 104.0 ± 5.9 | 106.0 ± 9.2 |
| Composite reach (% LL) | 105.2 ± 12.9 | 104.7 ± 12.9 | 100.4 ± 8.5 | 102.8 ± 7.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mear, E.; Gladwell, V.F.; Pethick, J. The Effect of Breaking Up Sedentary Time with Calisthenics on Neuromuscular Function: A Preliminary Study. Int. J. Environ. Res. Public Health 2022, 19, 14597. https://doi.org/10.3390/ijerph192114597
Mear E, Gladwell VF, Pethick J. The Effect of Breaking Up Sedentary Time with Calisthenics on Neuromuscular Function: A Preliminary Study. International Journal of Environmental Research and Public Health. 2022; 19(21):14597. https://doi.org/10.3390/ijerph192114597
Chicago/Turabian StyleMear, Emily, Valerie Frances Gladwell, and Jamie Pethick. 2022. "The Effect of Breaking Up Sedentary Time with Calisthenics on Neuromuscular Function: A Preliminary Study" International Journal of Environmental Research and Public Health 19, no. 21: 14597. https://doi.org/10.3390/ijerph192114597
APA StyleMear, E., Gladwell, V. F., & Pethick, J. (2022). The Effect of Breaking Up Sedentary Time with Calisthenics on Neuromuscular Function: A Preliminary Study. International Journal of Environmental Research and Public Health, 19(21), 14597. https://doi.org/10.3390/ijerph192114597