
Shift Work and Early Arterial Stiffness: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility
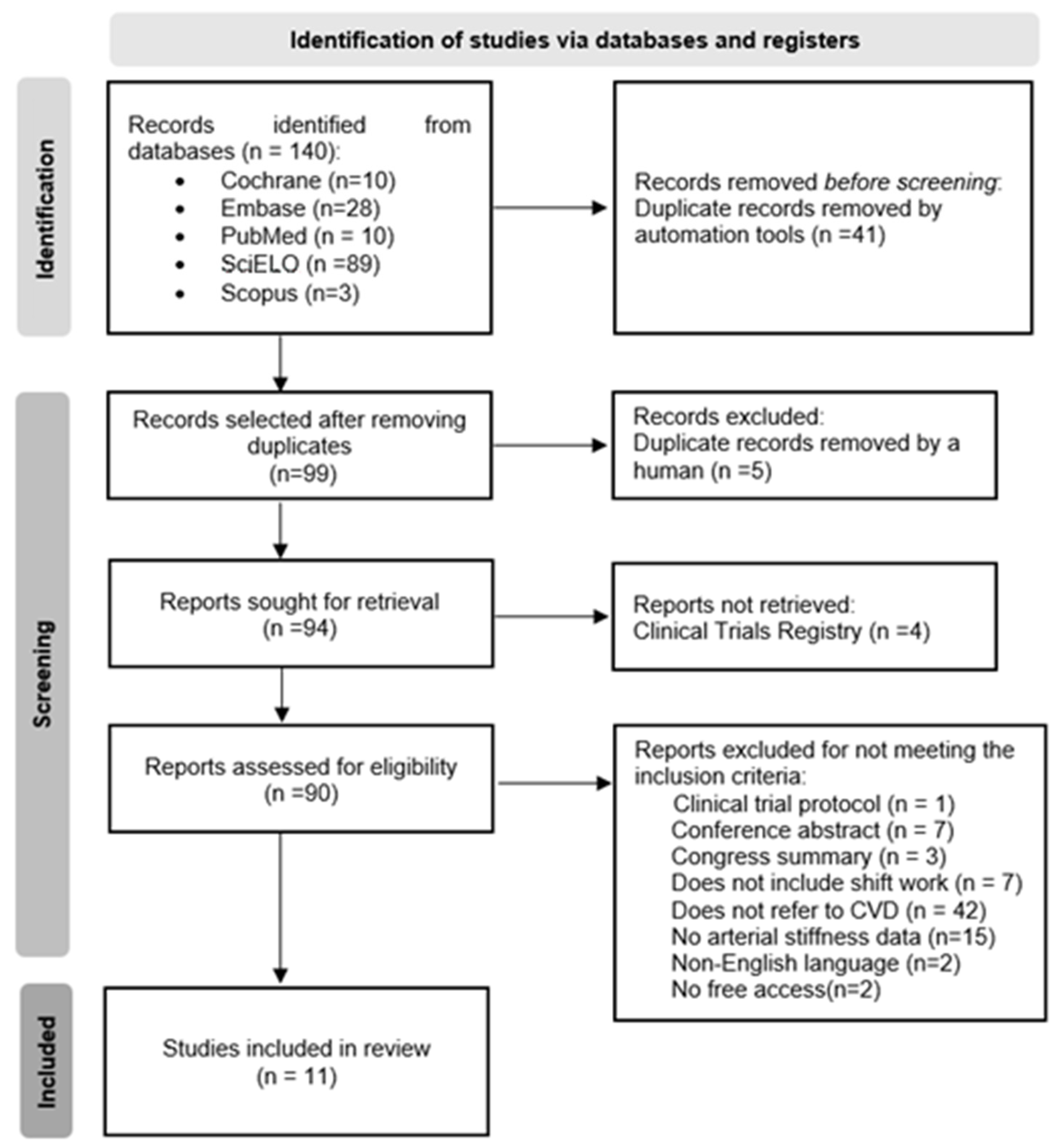
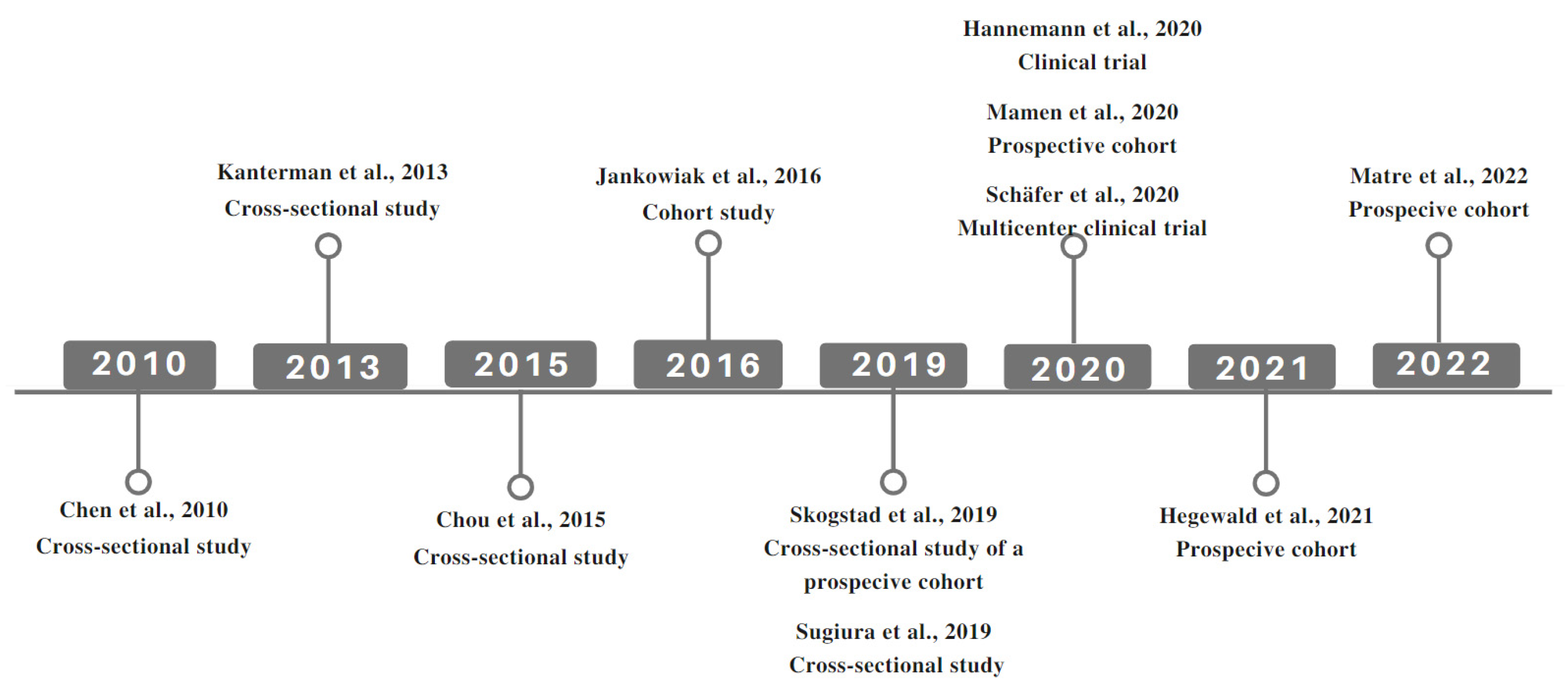
3. Results

{kind=link}
{kind=link}
| Author and Year | Country | Study Design | N | Gender and Age | Type of Worker | Exposure | Study Duration/Follow-Up |
|---|---|---|---|---|---|---|---|
| Chen et al. (2010) [23] | Taiwan | Cross-sectional | 184 | 100% males, mean age 42.2 years | Bus drivers | Night work on different days | 3 months |
| Kantermann et al. (2013) [21] | Belgium | Cross-sectional | 77 | 100% males, mean age 42 ± 7.6 years | Steel workers | Shift work, included night work | 2009 to 2011 |
| Chou et al. (2015) [28] | Taiwan | Cross-sectional | 576 | 85.2% females, mean age 40.5 years | Health professionals | Shift work and night work | Not reported |
| Jankowiak et al. (2016) [25] | Germany | Cohort | 10.475 | 74.2% males, age 35–64 years | Variety of professions | Current and previous night work | 2007 to 2012 |
| Skogstad et al. (2019) [26] | Norway | Cross-sectional prospective cohort | 94 | 86.17% males, 49.7 years DW/40.3 years SW | Industrial employees | 8 or 12 h night shift depending on the week | 2018 to 2021 |
| Sugiura et al. (2019) [29] | Japan | Cross-sectional | 10.073 | 100% males, 46.6 ± 8.1 years | Industrial employees | Nighttime hours with or without an irregular schedule | 2008 to 2009 |
| Hannemann et al. (2020) [32] | Germany | Interventional | 24 | 58% females/34.2 ± 8.6 years (IG), 75% females/37.3 ± 13.7 years (CG) | Not reported | At least 3 nightshifts/1 month for a period of at least 6 months. | 24 weeks |
| Mamen et al. (2020) [27] | Norway | Interventional prospective cohort | 94 | 86% males, 38.4 ± 11.5 CG/ 43.1 ± 10.5 IG years | Industrial employees | 8 or 12 h night shift depending on the week | 8 weeks |
| Schäfer et al. (2020) [30] | Austria and Germany | Interventional | 64 | 79.9% female gender, 36.7 ± 12.2 years | Various professions | Shift work, included night work | 24 weeks |
| Hegewald et al. (2021) [31] | Germany | Prospective cohort | 2.426 | 51.1% male gender, 46.5 ± 7.3 years | Not reported | Shift work, included night work | 2007 to 2012 |
| Matre et al. (2022) [24] | Norway | Prospective cohort | 19 | 89.47% male gender, 40.9 ± 11.5 years | Industrial employees | 8 or 12 h night shift depending on the week | 2018 to 2021, follow-up 5 weeks |
| Author and Year | Objective | Collected Data/Methods | Assessment of Arterial Stiffness | Groups |
|---|---|---|---|---|
| Chen et al. (2010) [23] | To examine the links between shift work and arteriosclerosis | Interview, measurement of BaPWV, BP, anthropometric data and laboratory assay | BaPWV (VP-2000—Colin Co., Ltd., Komaki, Japan) | EG = shift workers and CG = regular hours workers |
| Kantermann et al. (2013) [21] | To identify atherosclerotic risk in work shifts and to observe its relationship with social jetlag and shift schedule | Questionnaires, BMI, BP, AS measurements | PWV (Vicorder-Skidmore Medical, Bristol, UK) | Workers on fast CW and slow CC shifts |
| Chou et al. (2015) [28] | To explore the relationship between multiple work-related risk and arteriosclerosis | Eletronic questionnaire, Measurements of: arteriosclerosis, job stress, mental health and CVR (smoking status, BMI, FBG, CHOL and AH). | BaPWV/CAVI (VaSera VS-1000, Fukuda Denshi, Japan) | Analyzed according to: gender, job-related factors and presence of CVR |
| Jankowiak et al. (2016) [25] | Check for associations and dose-response relationships between current exposure and cumulative exposure to night work and atherosclerosis | Interviews (including job data), blood sampling (fibrinogen and CRP) and clinical examinations (AS, BP and AH). | PWV (Digital photoplethysmography—Pulse Trace PCA 2™, Micro Medical Ltd., currently CareFusion) | EG = Night shift worker and CG = day worker |
| Skogstad et al. (2019) [26] | To present the initial results of a cohort of workers in industrial shifts. | Questionnaires, BP, HR, VO2max Test, blood analyses (lipids, HbA1c, CRP), exposure to toxins, AS (CBP, AP, AIx, PWV) and USCA | PWV (SphygmoCor XCEL®—AtCor Medical Pty Ltd., Sydney, Australia) | EG = shift worker, including night work and CG = day worker |
| Sugiura et al. (2019) [29] | To analyze how shift work and lifestyle habits interfere with the accumulation of visceral fat and the presence of atherosclerosis | Anthropometric data, BP, blood samples (lipids, creatinine, FBG, HbA1c), AS (CAVI e IMT) e VFA (CT). | CAVI (Vasera VS-1000 automatic system—Fukuda Denshi, Tokyo, Japan) | EG = Shift workers and CG= fixed daytime workers |
| Hannemann et al. (2020) [32] | To assess whether timed physical exercise interferes with glucose metabolism, circadian rhythms, and 24 h blood pressure in shift workers. | Questionaries, anthropometric data, job data, actigraphy, effects of timed physical, exercise performance, glucose tolerance, diurnal rhythms of melatonin and cortisol, and 24 h BP, AS, HOMA-IR and QUICKI | 24 h-PWV (BPLab®—OOO Petr Telegin, Nizhny Novgorod, Russia) | IG = night workers with exercise and CG = night workers without exercise |
| Mamen et al. (2020) [27] | To examine whether high-intensity PA would modify the risk of CVD in the studied group. | Questionnaire, AP, BP, HR, CBP, AIx, PP, PWV, HbA1c, HDL, LDL, CHOL, CRP, VO2max, PAI | PWV (SphygmoCor XCEL®—AtCor | IG = ≥10 training sessions and CG = 0 ou < 10 training sessions |
| Schäfer et al. (2020) [30] | To assess whether timed aerobic exercise before night work reduces CVR and AS | 35 min of HIIT/12 weeks, anthropometric data, glucose metabolism, lipid profile, exercise capacity and PWV. | PWV (Mobil-o-Graph®—NG (IEM, Stolberg, Germany) | IG = 35min HIIT before each NW and CG = no training |
| Hegewald et al. (2021) [31] | To examine whether WLC can impact AH incidence and cardiovascular health | Questionnaire (including COPSOQ), WLC, AH, Stiffness Index. | Stiffness Index (Pulse Trace PCA2 device—Micro Medical imited/Carefusion) | 2 subsamples: (1) included AH and AS, and (2) excluded CVD (MI, stroke, AF, PAD, CAD, and CHF). |
| Matre et al. (2022) [24] | To investigate associations between sleep duration, number of awakenings, BP and AS in shift workers. | BP, HR, PWV, actigraphy | PWV (SphygmoCor XCEL®—Atcor Medical, New South Wales, Australia) | Analyzed sleep duration and number of awakenings according to: diary and actigraphy |
| Author and Year | Main Results | Considered Confounder Factors | Limitations |
|---|---|---|---|
| Chen et al. (2010) [23] | BaPWV increased by 3.6 cm/s for per 1-year increment in years of shift driving | Age, education level, smoking, alcohol, tea and coffee consumption, PA, sleep time, WC, BP, BMI, CHOL, HDL, LDL, plasma glucose and insulin. | Working hours starting at different times. Noise and motor exhaust are possible CVD. Selecting healthy workers can have biased results Small sample limited statistical ability to detect risk. |
| Kantermann et al. (2013) [21] | There was no significant difference in PWV between shift-rotations (CW, CC and DW) | Analyzes involving PWV were adjusted for age, BP, HR, BMI, WHR and smoking as covariates. | The small sample may have influenced the lack of statistical difference in PWV between the two shift groups |
| Chou et al. (2015) [28] | The sleep duration < 6 h and weekly work hours > 60 h were significantly associated with increased risk of arteriosclerosis | Adjustments for age, gender, education, medical profession and CVR (smoking, BMI, HR, BP, FBG and CHOL) were included in the analysis model. | Lack of validation of the use of the BaPWV formula for the Taiwanese population. Included only medical staff. The sample size was modest, and the study design weakens the causal relationship. |
| Jankowiak et al. (2016) [25] | Night SW with >660 NS within the last 10 years increased AS (0.33 m/s), with 4% flow velocity increase compared to non-night workers. | Covariates included in the different regression models: basic confounders (age and gender), current occupational exposures, lifestyle factors (smoking, alcohol, WHR), Socioeconomic status and dispositional factors (menopause status, family history of MI or stroke). | The analyzes were of a transversal cut. There was no precise data on types of turns and direction of rotation. The number of valid measurements of vascular function was limited. Physical activity cannot be considered an adjustment. |
| Skogstad et al. (2019) [26] | Longer time (years) of SW was associated with increased IMT and high CRP. | Adjustments for age, gender and smoking were used in the analysis model. | Cross-sectional design, possible selection bias (workers) and CVD-related covariates (unhealthy eating habits and alcohol intake) were not considered. |
| Sugiura et al. (2019) [29] | VFA, CAVI, and IMT values were significantly greater in fixed daytime workers than in shift workers | Analyzes were performed with different models adjusted for: age, systolic BP, HDL, LDL, TGL, creatinine, VFA, CAVI, CCA and IMT in different ways. | The study design was cross-sectional. The background of the participants was heterogeneous. The categorizations considered only two groups |
| Hannemann et al. (2020) [32] | Timed exercise sessions before the NS have no significant effect on glucose tolerance, 24 h BP, and circadian rhythms of melatonin and cortisol. | Not reported | Small number of participants. Adoption of low-intensity exercise (weaker zeitgeber). Light PA and food intake were not controlled. Baseline fitness level was better in IG workers. |
| Mamen et al. (2020) [27] | Short training sessions with 4 min of high-intensity PA, 3 times/week/8 weeks among rotating SW reduced some CVD risk (BP, HbA1c). | Not reported | Misclassification of exercise level. Self-reported activities can be biased, especially low-intensity training activity. |
| Schäfer et al. (2020) [30] | 12 weeks of HIIT within 2 h before NS work improves physical exercise capacity and AS (reduction of −0.1 ± 1.1m/s) | Not reported | Not reported |
| Hegewald et al. (2021) [31] | There was no association between WLC and incident hypertension or increased AS, but results stratified by gender resulted in a hazard ratio of 1.47 (95% CI 0.54–3.98) for incident CVD among women. | Depending on the model: sex, age, socioeconomic level, WLC (management position, NS and working hours/week), factors of private life, smoking, alcohol abuse and WHR. | Few incidents CVD were observed in the first five years among women. Selection bias may have occurred (healthy worker). They could not estimate the effect of private life roles interfering with work on cardiovascular health. |
| Matre et al. (2022) [24] | Shorter sleep duration was associated with higher BP and partly with higher PWV, indicating an increased risk of CVD with reduced sleep | Analyzes involving PWV were adjusted for gender and age | Sample size. Data not representative of the population. Sleep duration calculated by an actigraphy not validated against polysomnography. Wide divergence between actigraphy and diary data. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IARC Monographs Vol 124 Group. Carcinogenicity of night shift work. Lancet Oncol. 2019, 20, 1058–1059. [Google Scholar] [CrossRef]
- Costa, G. Shift work and health: Current problems and preventive actions. Saf. Health Work 2010, 1, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Organisation Internationale du Travail. Recommendation R178—Night Work Recommendation, 1990 (No. 178) (ilo.org). Available online: https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_INSTRUMENT_ID:312516 (accessed on 15 September 2022).
- Anttila, T.; Oinas, T. 24/7 society: The new timing of work? In Family, Work and Well-Being; Lawrence Erlbaum: Mahwah, NJ, USA, 2018. [Google Scholar]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.R.C.; Marqueze, E.C.; Sargent, C.; Wright, K.P., Jr.; Ferguson, S.A.; Tucker, P. Working Time Society consensus statements: Evidence-based effects of shift work on physical and mental health. Ind. Health 2019, 57, 139–157. [Google Scholar] [CrossRef]
- Schnall, P.L.; Dobson, M.; Landsbergis, P. Globalization, Work, and Cardiovascular Disease. Int. J. Health Serv. 2016, 46, 656–692. [Google Scholar] [CrossRef]
- Rosa, D.; Terzoni, S.; Dellafiore, F.; Destrebecq, A. Systematic review of shift work and nurses’ health. Occup. Med. 2019, 69, 237–243. [Google Scholar] [CrossRef]
- Vyas, M.V.; Garg, A.X.; Iansavichus, A.V.; Costella, J.; Donner, A.; Laugsand, L.E.; Janszky, I.; Mrkobrada, M.; Parraga, G.; Hackam, D.G. Shift work and vascular events: Systematic review and meta-analysis. BMJ 2012, 345, e4800. [Google Scholar] [CrossRef]
- Lunde, L.-K.; Skare, Ø.; Mamen, A.; Sirnes, P.A.; Aass, H.C.D.; Øvstebø, R.; Goffeng, E.; Matre, D.; Nielsen, P.; Heglum, H.S.A.; et al. Cardiovascular Health Effects of Shift Work with Long Working Hours and Night Shifts: Study Protocol for a Three-Year Prospective Follow-Up Study on Industrial Workers. Int. J. Environ. Res. Public Health 2020, 17, 589. [Google Scholar] [CrossRef]
- Ferguson, J.M.; Costello, S.; Neophytou, A.M.; Balmes, J.R.; Bradshaw, P.T.; Cullen, M.R.; Eisen, E.A. Night and rotational work exposure within the last 12 months and risk of incident hypertension. Scand. J. Work Environ. Health 2019, 45, 256–266. [Google Scholar] [CrossRef]
- van Sloten, T.T.; Protogerou, A.D.; Henry, R.M.; Schram, M.T.; Launer, L.J.; Stehouwer, C.D. Association between arterial stiffness, cerebral small vessel disease and cognitive impairment: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2015, 53, 121–130. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Segers, P.; Hughes, T.; Townsend, R. Large-Artery Stiffness in Health and Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 74, 1237–1263. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.P.; Kim, H.-L. Incremental value of the measures of arterial stiffness in cardiovascular risk assessment. Rev. Cardiovasc. Med. 2022, 23, 6. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial stiffness and cardiovascular events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kim, S.S.; Kim, I.J.; Kim, J.H.; Kim, B.H.; Kim, M.K.; Lee, S.H.; Lee, C.W.; Kim, M.C.; Ahn, J.H.; et al. Arterial stiffness is an independent predictor for risk of mortality in patients with type 2 diabetes mellitus: The REBOUND study. Cardiovasc. Diabetol. 2020, 19, 143. [Google Scholar] [CrossRef]
- Wassertheurer, S.; Kropf, J.; Weber, T.; van der Giet, M.; Baulmann, J.; Ammer, M.; Hametner, B.; Mayer, C.C.; Eber, B.; Magometschnigg, D. A new oscillometric method for pulse wave analysis: Comparison with a common tonometric method. J. Hum. Hypertens. 2010, 24, 498–504. [Google Scholar] [CrossRef]
- Weber, T.; Chirinos, J.A. Pulsatile arterial haemodynamics in heart failure. Eur. Heart. J. 2018, 39, 3847–3854. [Google Scholar] [CrossRef]
- Puttonen, S.; Kivimäki, M.; Elovainio, M.; Pulkki-Råback, L.; Hintsanen, M.; Vahtera, J.; Telama, R.; Juonala, M.; Viikari, J.S.; Raitakari, O.T.; et al. Shift work in young adults and carotid artery intima-media thickness: The Cardiovascular Risk in Young Finns study. Atherosclerosis 2009, 205, 608–613. [Google Scholar] [CrossRef]
- Charles, L.E.; Fekedulegn, D.; Burchfiel, C.M.; Fujishiro, K.; Landsbergis, P.; Diez Roux, A.V.; Macdonald, L.; Foy, C.G.; Andrew, M.E.; Stukovsky, K.H.; et al. Associations of work hours with carotid intima-media thickness and ankle-brachial index: The Multi-Ethnic Study of Atherosclerosis (MESA). Occup. Environ. Med. 2012, 69, 713–720. [Google Scholar] [CrossRef]
- Kantermann, T.; Duboutay, F.; Haubruge, D.; Kerkhofs, M.; Schmidt-Trucksäss, A.; Skene, D.J. Atherosclerotic risk and social jetlag in rotating shift-workers: First evidence from a pilot study. Work 2013, 46, 273–282. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Chen, C.-C.; Shiu, L.-J.; Li, Y.-L.; Tung, K.-Y.; Chan, K.-Y.; Yeh, C.-J.; Chen, S.-C.; Wong, R.-H. Shift work and arteriosclerosis risk in professional bus drivers. Ann. Epidemiol. 2010, 20, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Matre, D.; Sirnes, P.A.; Goffeng, E.; Skare, Ø.; Skogstad, M. Sleep Duration, Number of Awakenings and Arterial Stiffness in Industrial Shift Workers: A Five-Week Follow-Up Study. Int. J. Environ. Res. Public Health 2022, 19, 1964. [Google Scholar] [CrossRef] [PubMed]
- Jankowiak, S.; Backé, E.; Liebers, F.; Schulz, A.; Hegewald, J.; Garthus-Niegel, S.; Nübling, M.; Blankenberg, S.; Pfeiffer, N.; Lackner, K.J.; et al. Current and cumulative night shift work and subclinical atherosclerosis: Results of the Gutenberg Health Study. Int. Arch. Occup. Environ. Health 2016, 89, 1169–1182. [Google Scholar] [CrossRef] [PubMed]
- Skogstad, M.; Mamen, A.; Lunde, L.-K.; Ulvestad, B.; Matre, D.; Aass, H.C.D.; Øvstebø, R.; Nielsen, P.; Samuelsen, K.N.; Skare, Ø.; et al. Shift Work Including Night Work and Long Working Hours in Industrial Plants Increases the Risk of Atherosclerosis. Int. J. Environ. Res. Public Health 2019, 16, 521. [Google Scholar] [CrossRef] [PubMed]
- Mamen, A.; Øvstebø, R.; Sirnes, P.A.; Nielsen, P.; Skogstad, M. High-Intensity Training Reduces CVD Risk Factors among Rotating Shift Workers: An Eight-Week Intervention in Industry. Int. J. Environ. Res. Public Health 2020, 17, 3943. [Google Scholar] [CrossRef]
- Chou, L.-P.; Li, C.-Y.; Hu, S.C. Work-Related Psychosocial Hazards and Arteriosclerosis. Int. Heart J. 2015, 56, 644–650. [Google Scholar] [CrossRef]
- Sugiura, T.; Dohi, Y.; Takagi, Y.; Yoshikane, N.; Ito, M.; Suzuki, K.; Nagami, T.; Iwase, M.; Seo, Y.; Ohte, N. Impacts of lifestyle behavior and shift work on visceral fat accumulation and the presence of atherosclerosis in middle-aged male workers. Hypertens. Res. 2020, 43, 235–245. [Google Scholar] [CrossRef]
- Schäfer, C.; Mayr, B.; Müller, E.E.; Augner, C.; Hannemann, J.; Böger, R.H.; Schönfelder, M.; Niebauer, J. Exercise training prior to night shift work improves physical work capacity and arterial stiffness. Eur. J. Prev. Cardiol. 2020, 27, 891–893. [Google Scholar] [CrossRef]
- Hegewald, J.; Starke, K.R.; Garthus-Niegel, S.; Schulz, A.; Nübling, M.; Latza, U.; Jankowiak, S.; Liebers, F.; Rossnagel, K.; Riechmann-Wolf, M.; et al. Correction: Work-life conflict and cardiovascular health: 5-year follow-up of the Gutenberg Health Study. PLoS ONE 2021, 16, e0258075. [Google Scholar] [CrossRef]
- Hannemann, J.; Laing, A.; Glismann, K.; Skene, D.J.; Middleton, B.; Staels, B.; Marx, N.; Grant, P.J.; Federici, M.; Niebauer, J.; et al. Timed physical exercise does not influence circadian rhythms and glucose tolerance in rotating night shift workers: The EuRhythDia study. Diabetes Vasc. Dis. Res. 2020, 17, 1479164120950616. [Google Scholar] [CrossRef]
- Hermansson, J.; Gillander Gådin, K.; Karlsson, B.; Lindahl, B.; Stegmayr, B.; Knutsson, A. Ischemic stroke and shift work. Scand. J. Work Environ. Health 2007, 33, 435–439. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Haupt, C.M.; Alte, D.; Dörr, M.; Robinson, D.M.; Felix, S.B.; John, U.; Völzke, H. The relation of exposure to shift work with atherosclerosis and myocardial infarction in a general population. Atherosclerosis 2008, 201, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, B.H.; Knutsson, A.K.; Lindahl, B.O.; Alfredsson, L.S. Metabolic disturbances in male workers with rotating three-shift work. Results of the WOLF study. Int. Arch. Occup. Environ. Health 2003, 76, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, B.; Knutsson, A.; Lindahl, B. Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27,485 people. Occup. Environ. Med. 2001, 58, 747–752. [Google Scholar] [CrossRef]
- Sookoian, S.; Gemma, C.; Fernández Gianotti, T.; Burgueño, A.; Alvarez, A.; González, C.D.; Pirola, C.J. Effects of rotating shift work on biomarkers of metabolic syndrome and inflammation. J. Intern. Med. 2007, 261, 285–292. [Google Scholar] [CrossRef]
- Fujino, Y.; Iso, H.; Tamakoshi, A.; Inaba, Y.; Koizumi, A.; Kubo, T.; Yoshimura, T.; Japanese Collaborative Cohort Study Group. A prospective cohort study of shift work and risk of ischemic heart disease in Japanese male workers. Am. J. Epidemiol. 2006, 164, 128–135. [Google Scholar] [CrossRef]
- Knutsson, A.; Akerstedt, T.; Jonsson, B.G.; Orth-Gomer, K. Increased risk of ischaemic heart disease in shift workers. Lancet 1986, 2, 89–92. [Google Scholar] [CrossRef]
- Knutsson, A.; Hallquist, J.; Reuterwall, C.; Theorell, T.; Akerstedt, T. Shiftwork and myocardial infarction: A case-control study. Occup. Environ. Med. 1999, 56, 46–50. [Google Scholar] [CrossRef]
- Brown, D.L.; Feskanich, D.; Sánchez, B.N.; Rexrode, K.M.; Schernhammer, E.S.; Lisabeth, L.D. Rotating night shift work and the risk of ischemic stroke. Am. J. Epidemiol. 2009, 169, 1370–1377. [Google Scholar] [CrossRef]
- Gangwisch, J.E. Response to “Sleep duration and hypertension with special emphasis on gender and obesity”. Am. J. Hypertens. 2013, 26, 1363–1364. [Google Scholar] [CrossRef][Green Version]
- Mason, I.C.; Grimaldi, D.; Reid, K.J.; Warlick, C.D.; Malkani, R.G.; Abbott, S.M.; Zee, P.C. Light exposure during sleep impairs cardiometabolic function. Proc. Natl. Acad. Sci. USA 2022, 119, e2113290119. [Google Scholar] [CrossRef] [PubMed]
- Heiser, P.; Dickhaus, B.; Opper, C.; Schreiber, W.; Clement, H.W.; Hasse, C.; Hennig, J.; Krieg, J.C.; Wesemann, W. Platelet serotonin and interleukin-1 beta after sleep deprivation and recovery sleep in humans. J. Neural. Transm. 1997, 104, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Irokawa, M.; Nishinaga, M.; Funayama, H.; Ikeda, U.; Shimada, K. Effect of a Change in the Sleep/Wake Cycle on the Diurnal Variation of Fibrinolytic Parameters. J. Thromb. Thrombolysis 1998, 5, 165–168. [Google Scholar] [CrossRef]
- Krueger, J.M.; Majde, J.A. Humoral links between sleep and the immune system: Research issues. Ann. N. Y. Acad. Sci. 2003, 992, 9–20. [Google Scholar] [CrossRef]
- Boyko, E.J.; Seelig, A.D.; Jacobson, I.G.; Hooper, T.I.; Smith, B.; Smith, T.C.; Crum-Cianflone, N.F.; Millennium Cohort Study Team. Sleep characteristics, mental health, and diabetes risk: A prospective study of U.S. military service members in the Millennium Cohort Study. Diabetes Care 2013, 36, 3154–3161. [Google Scholar] [CrossRef] [PubMed]
- Mosendane, T.; Mosendane, T.; Raal, F.J. Shift work and its effects on the cardiovascular system. Cardiovasc. J. Afr. 2008, 19, 210–215. [Google Scholar]
- Crnko, S.; Du Pré, B.C.; Sluijter, J.P.G.; Van Laake, L.W. Circadian rhythms and the molecular clock in cardiovascular biology and disease. Nat. Rev. Cardiol. 2019, 16, 437–447. [Google Scholar] [CrossRef]
- Crnko, S.; Cour, M.; Van Laake, L.W.; Lecour, S. Vasculature on the clock: Circadian rhythm and vascular dysfunction. Vasc. Pharmacol. 2018, 108, 1–7. [Google Scholar] [CrossRef]
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose-response relationship. Scand. J. Work Environ. Health 2018, 44, 229–238. [Google Scholar] [CrossRef]
- Virtanen, M.; Heikkilä, K.; Jokela, M.; Ferrie, J.E.; Batty, G.D.; Vahtera, J.; Kivimäki, M. Long working hours and coronary heart disease: A systematic review and meta-analysis. Am. J. Epidemiol. 2012, 176, 586–596. [Google Scholar] [CrossRef]
- Lewis, P.; Korf, H.W.; Kuffer, L.; Groß, J.V.; Erren, T.C. Exercise time cues (zeitgebers) for human circadian systems can foster health and improve performance: A systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000443. [Google Scholar] [CrossRef] [PubMed]
- López-Soto, P.J.; Fabbian, F.; Cappadona, R.; Zucchi, B.; Manfredini, F.; García-Arcos, A.; Carmona-Torres, J.M.; Manfredini, R.; Rodríguez-Borrego, M.A. Chronotype, nursing activity, and gender: A systematic review. J. Adv. Nurs. 2019, 75, 734–748. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, A. Health disorders of shift workers. Occup. Med. 2003, 53, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, B.; Alfredsson, L.; Knutsson, A.; Andersson, E.; Torén, K. Total mortality and cause-specific mortality of Swedish shift- and dayworkers in the pulp and paper industry in 1952–2001. Scand. J. Work Environ. Health 2005, 31, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Ellingsen, T.; Bener, A.; Gehani, A.A. Study of shift work and risk of coronary events. J. R. Soc. Promot. Health 2007, 127, 265–267. [Google Scholar] [CrossRef]
- Zieman, S.J.; Melenovsky, V.; Kass, D.A. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef]
- Anujuo, K.; Stronks, K.; Snijder, M.B.; Jean-Louis, G.; van den Born, B.-J.; Peters, R.J.; Agyemang, C. Relationship between sleep duration and arterial stiffness in a multi-ethnic population: The HELIUS study. Chronobiol. Int. 2016, 33, 543–552. [Google Scholar] [CrossRef]
- Wickwire, E.M.; Geiger-Brown, J.; Scharf, S.M.; Drake, C.L. Shift Work and Shift Work Sleep Disorder: Clinical and Organizational Perspectives. Chest 2017, 151, 1156–1172. [Google Scholar] [CrossRef]
- Strohmaier, S.; Devore, E.E.; Zhang, Y.; Schernhammer, E.S. A Review of Data of Findings on Night Shift Work and the Development of DM and CVD Events: A Synthesis of the Proposed Molecular Mechanisms. Curr. Diabetes Rep. 2018, 18, 132. [Google Scholar] [CrossRef]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef]


| Item | Definition |
|---|---|
| Population | Adults, aged > 18 years |
| Intervention/Exposure | Night shift work |
| Control | Non-shift workers and day workers |
| Outcomes | Early arterial stiffness as a possible trigger of cardiovascular risk |
| Databases Searched | Key Words (MeSH Terms) to Create Search Strings |
|---|---|
| Cochrane | Shift work; shift worker; schedule shift work. |
| Embase | Night work; night shift work. |
| PubMed | Arteriosclerosis; atherosclerotic risk. |
| Scielo | Stiffness, vascular; vascular stiffnesses; arterial stiffness; arterial stiffnesses; stiffness, aortic. |
| Scopus | Pulse wave velocity; pulse wave velocities. |
| No filters were used | Strings were created according to each database using the Boolean operators OR and AND. |
| Selection Criteria for Inclusion Based on Title, Abstract and Eligibility Stage | |
| Inclusion: | Exclusion: |
| Quantitative studies related to shift work, including night shifts and arterial stiffness. | Experimental studies. |
| Original and research articles, longitudinal studies, cohort studies, and case–control studies. | Review articles not including quantitative data. |
| Available online with free access and as full text. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gusmão, W.D.P.; Pureza, I.R.O.M.; Moreno, C.R.C. Shift Work and Early Arterial Stiffness: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 14569. https://doi.org/10.3390/ijerph192114569
Gusmão WDP, Pureza IROM, Moreno CRC. Shift Work and Early Arterial Stiffness: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(21):14569. https://doi.org/10.3390/ijerph192114569
Chicago/Turabian StyleGusmão, Waléria D. P., Isabele R. O. M. Pureza, and Claudia R. C. Moreno. 2022. "Shift Work and Early Arterial Stiffness: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 21: 14569. https://doi.org/10.3390/ijerph192114569
APA StyleGusmão, W. D. P., Pureza, I. R. O. M., & Moreno, C. R. C. (2022). Shift Work and Early Arterial Stiffness: A Systematic Review. International Journal of Environmental Research and Public Health, 19(21), 14569. https://doi.org/10.3390/ijerph192114569