
Impact of the COVID-19 Pandemic on the Incidence of Suicidal Behaviors: A Retrospective Analysis of Integrated Electronic Health Records in a Population of 7.5 Million

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Ethical Conduct of the Study
2.3. Variables and Data Sources
2.4. Analysis
3. Results
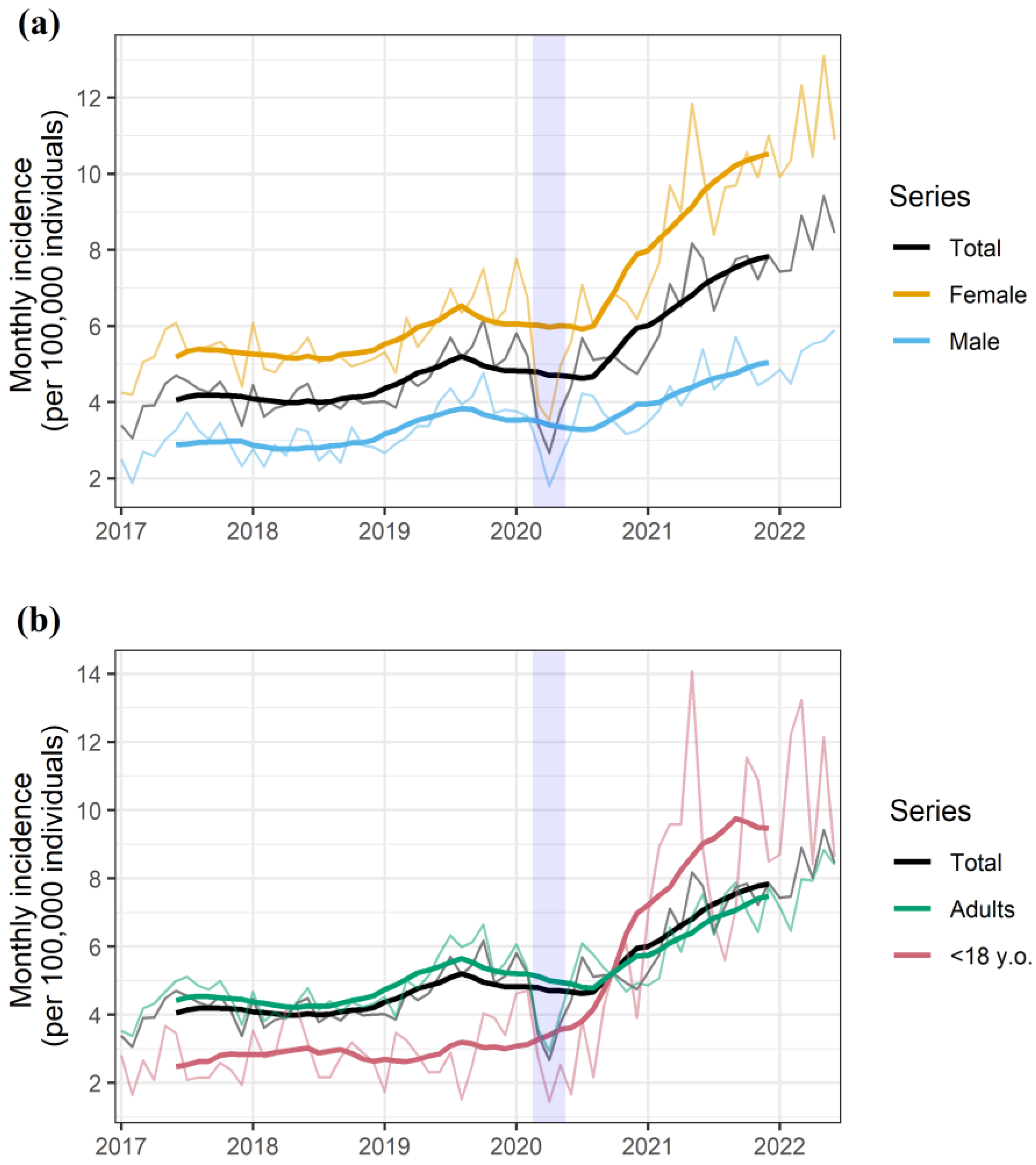
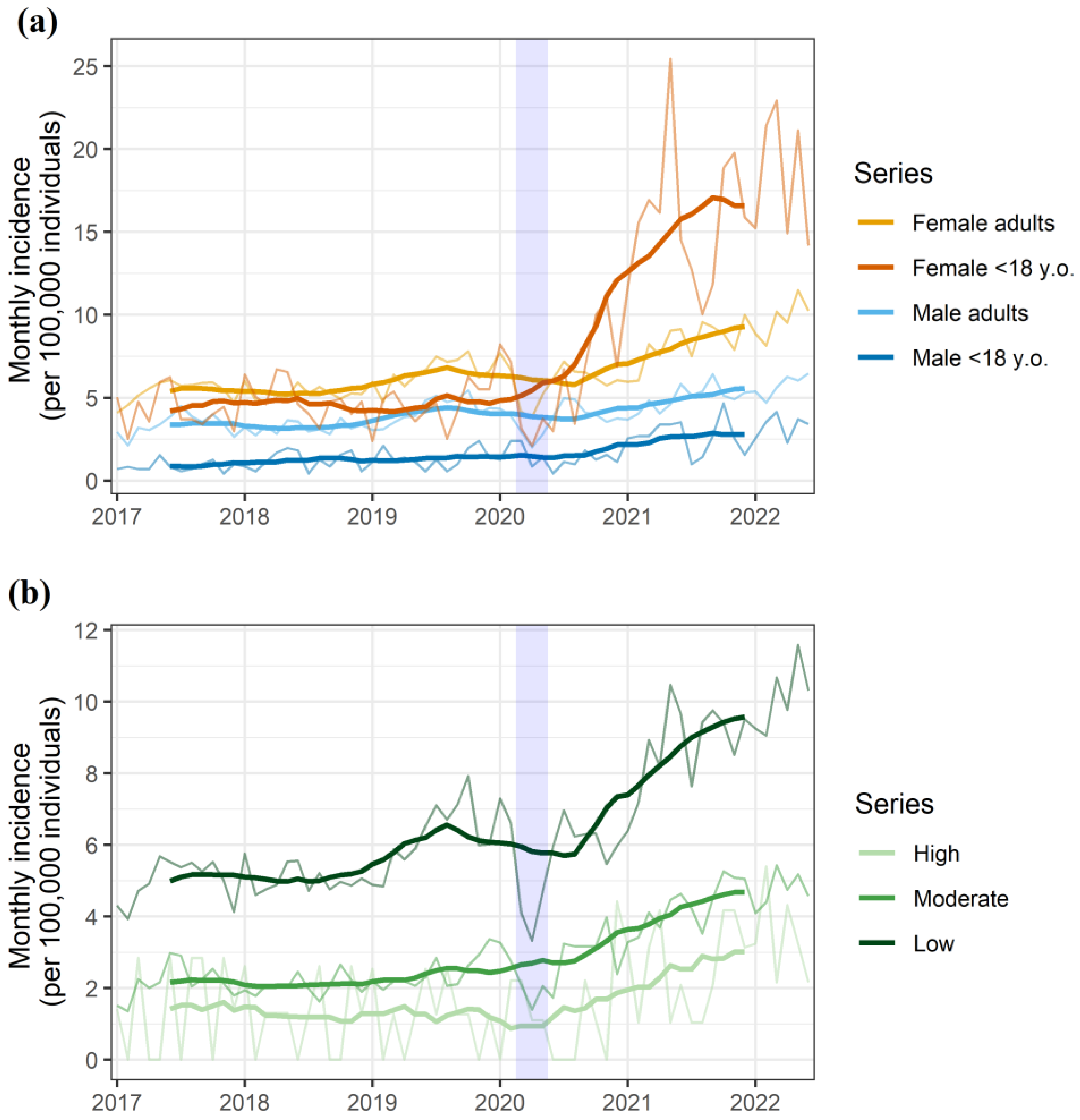
3.1. Incidence of Suicidal Behavior
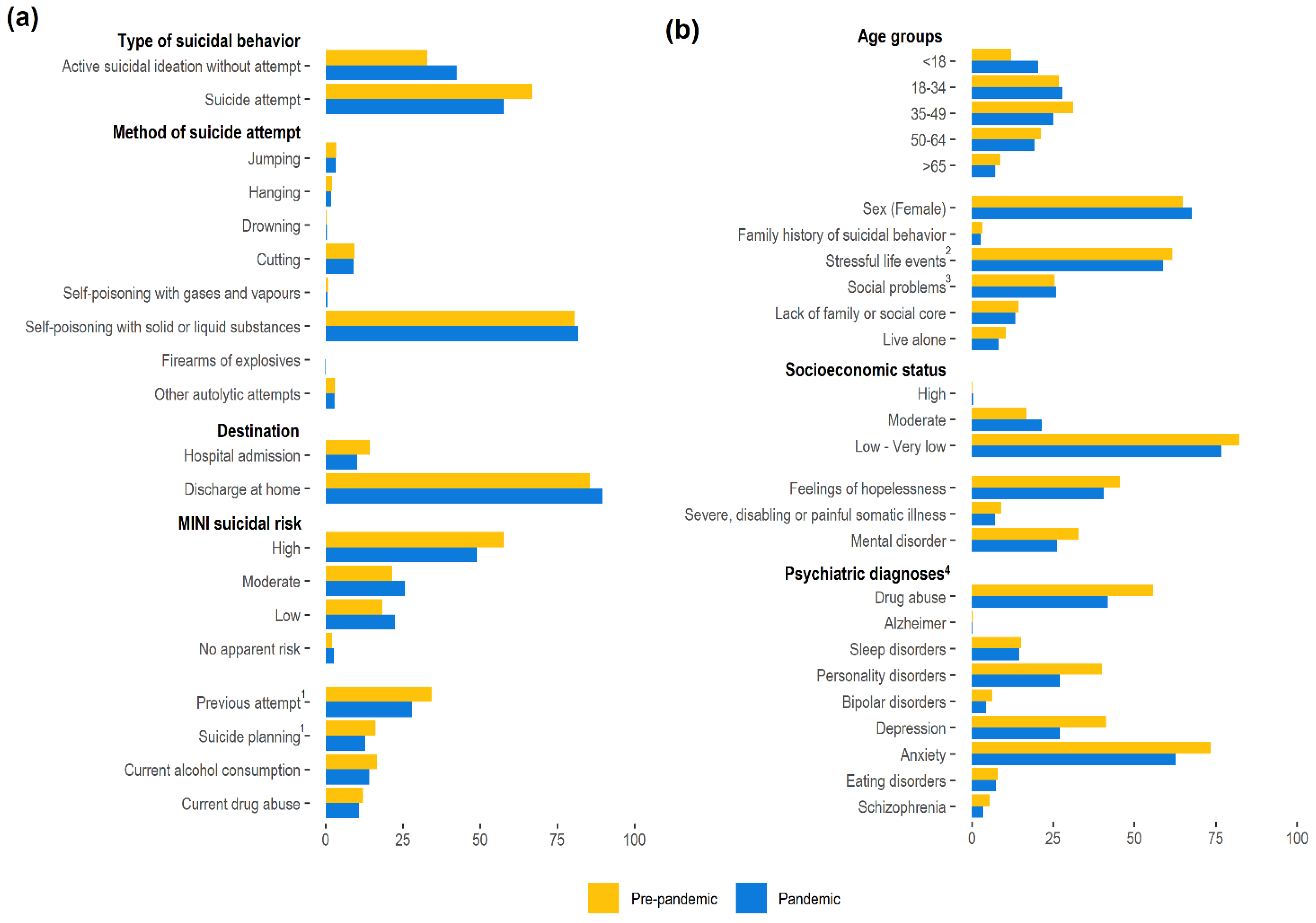
3.2. Risk Factors and Characteristics of Suicidal Behaviors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non–pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Mohamad Marzuki, M.F.; Yaacob, N.A.; Bin Yaacob, N.M.; Abu Hassan, M.R.; Ahmad, S.B. Usable Mobile App for Community education on colorectal cancer: Development process and usability study. JMIR Hum. Factors 2019, 6, e12103. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I. Multidisciplinary research priorities for the COVID–19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Yang, Y.; Li, W.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.T. Mental health services for older adults in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e19. [Google Scholar] [CrossRef]
- The Lancet Psychiatry COVID-19 and mental health. Lancet Psychiatry 2021, 8, 87. [CrossRef]
- Arango, C. Lessons Learned from the Coronavirus Health Crisis in Madrid, Spain: How COVID–19 has changed our lives in the last 2 Weeks. Biol. Psychiatry 2020, 88, e33–e34. [Google Scholar] [CrossRef]
- Fidel Kinori, S.G.; Carot-Sans, G.; Cuartero, A.; Valero-Bover, D.; Piera-Jiménez, J.; Roma Monfa, R.; Garcia, E.; Pérez Sust, P.; Blanch, J.; Ramos-Quiroga, J.A. Web App for emotional management during the COVID-19 pandemic: Platform development and retrospective analysis of Its use throughout two waves of the outbreak in Spain. JMIR Form. Res. 2021, 6, e27402. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 9 July 2022).
- World Health Organization. Suicide Worldwide in 2019. Available online: https://www.who.int/publications/i/item/9789240026643 (accessed on 9 July 2022).
- Ljung, R.; Grunewald, M.; Sundstrom, A.; Sundbom, L.T.; Zethelius, B. Comparison of years of life lost to 1,565 suicides versus 10,650 COVID–19 deaths in 2020 in Sweden: Four times more years of life lost per suicide than per COVID-19 death. Ups. J. Med. Sci. 2022, 127, e8533. [Google Scholar] [CrossRef]
- Merayo-Cano, J.M.; Porras-Segovia, A.; Baca-García, E. COVID-19 impact vs. suicide impact in Spain. Rev. Psiquiatr. Salud Ment. 2022. [Google Scholar] [CrossRef]
- Van der Burgt, M.C.A.; Mérelle, S.; Beekman, A.T.F.; Gilissen, R. The impact of COVID–19 on the Suicide prevention helpline in The Netherlands. Crisis 2022. [Google Scholar] [CrossRef]
- Reif–Leonhard, C.; Lemke, D.; Holz, F.; Ahrens, K.F.; Fehr, C.; Steffens, M.; Grube, M.; Freitag, C.M.; Kölzer, S.C.; Schlitt, S.; et al. Changes in the pattern of suicides and suicide attempt admissions in relation to the COVID-19 pandemic. Eur. Arch. Psychiatry Clin. Neurosci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Demenech, L.M.; Neiva–Silva, L.; Brignol, S.M.S.; Marcon, S.R.; Lemos, S.M.; Tassitano, R.M.; Dumith, S.C. Suicide risk among undergraduate students in Brazil in the periods before and during the COVID-19 pandemic: Results of the SABES-Grad national survey. Psychol. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, E.; Hanley, S.J.B.; Sato, Y.; Saijo, Y. Impact of the COVID–19 pandemic on suicide rates in Japan through December 2021: An interrupted time series analysis. Lancet Reg. Health West. Pacific 2022, 24, 100480. [Google Scholar] [CrossRef] [PubMed]
- Pérez, V.; Elices, M.; Prat, B.; Vieta, E.; Blanch, J.; Alonso, J.; Pifarré, J.; Mortier, P.; Cebrià, A.I.; Campillo, M.T.; et al. The Catalonia Suicide Risk Code: A secondary prevention program for individuals at risk of suicide. J. Affect. Disord. 2020, 268, 201–205. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar]
- Government of Catalonia Statistical Institute of Catalonia (Idescat). Available online: https://www.idescat.cat/indicadors/?id=aec&n=15231&lang=en (accessed on 9 July 2022).
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.r–project.org (accessed on 20 December 2021).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- García-Álvarez, L.; de la Fuente-Tomás, L.; García-Portilla, M.P.; Sáiz, P.A.; Lacasa, C.M.; Dal Santo, F.; González-Blanco, L.; Bobes-Bascarán, M.T.; García, M.V.; Vázquez, C.Á. Early psychological impact of the 2019 coronavirus disease (COVID-19) pandemic and lockdown in a large Spanish sample. J. Glob. Health 2020, 10, 020505. [Google Scholar] [CrossRef]
- Jerónimo, M.Á.; Piñar, S.; Samos, P.; González, A.M.; Bellsolà, M.; Sabaté, A.; León, J.; Aliart, X.; Martín, L.M.; Aceña, R.; et al. Suicidal attempt and suicidal ideation during the COVID-19 pandemic compared to previous years. Rev. Psiquiatr. Salud Ment. 2021. [Google Scholar] [CrossRef]
- Madianos, M.G.; Evi, K. Trauma and natural disaster: The case of earthquakes in Greece. J. Loss Trauma 2010, 15, 138–150. [Google Scholar] [CrossRef]
- Orui, M.; Sato, Y.; Tazaki, K.; Kawamura, I.; Harada, S.; Hayashi, M. Delayed increase in male suicide rates in tsunami disaster– stricken areas following the great east Japan earthquake: A three-year follow-up study in Miyagi prefecture. Tohoku J. Exp. Med. 2015, 235, 215–222. [Google Scholar] [CrossRef][Green Version]
- Gordon, K.H.; Bresin, K.; Dombeck, J.; Routledge, C.; Wonderlich, J.A. The impact of the 2009 Red River Flood on interpersonal risk factors for suicide. Cris. J. Cris. Interv. Suicide Prev. 2011, 32, 52. [Google Scholar] [CrossRef]
- Fradera, M.; Ouchi, D.; Prat, O.; Morros, R.; Martin-Fumadó, C.; Palao, D.; Cardoner, N.; Campillo, M.T.; Pérez-Solà, V.; Pontes, C. Can routine Primary Care Records Help in Detecting Suicide Risk? A Population-Based Case-Control Study in Barcelona. Arch. Suicide Res. 2021, 26, 1395–1409. [Google Scholar] [CrossRef] [PubMed]
- Parra Uribe, I.; Blasco-Fontecilla, H.; García-Parés, G.; Giró Batalla, M.; Llorens Capdevila, M.; Cebrià Meca, A.; De Leon-Martinez, V.; Pérez–Solà, V.; Palao Vidal, D.J. Attempted and completed suicide: Not what we expected? J. Affect. Disord. 2013, 150, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; May, A.M.; Saffer, B.Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef] [PubMed]
- Roso–Llorach, A.; Serra–Picamal, X.; Cos, F.X.; Pallejà-Millán, M.; Mateu, L.; Rosell, A.; Almirante, B.; Ferrer, J.; Gasa, M.; Gudiol, C.; et al. Evolving mortality and clinical outcomes of hospitalized subjects during successive COVID–19 waves in Catalonia, Spain. Glob. Epidemiol. 2022, 4, 100071. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 2017 (N = 3641) | 2018 (N = 3638) | 2019 (N = 4489) | 2020 (N = 4291) | 2021 (N = 6528) | 2022 1 (N = 3871) | |
|---|---|---|---|---|---|---|
| Type of Suicidal Behavior | ||||||
| Active suicidal ideation without attempt | 1034 (28.4%) | 1226 (33.7%) | 1589 (35.4%) | 1640 (38.22%) | 2818 (43.17%) | 1737 (44.87%) |
| Suicide attempt | 2607 (71.6%) | 2412 (66.3%) | 2900 (64.6%) | 2651 (61.78%) | 3710 (56.83%) | 2134 (55.13%) |
| Suicide Attempt Method 2 | ||||||
| Jumping | 79 (3.03%) | 88 (3.65%) | 99 (3.41%) | 111 (4.19%) | 106 (2.86%) | 54 (2.53%) |
| Hanging | 47 (1.8%) | 53 (2.2%) | 70 (2.41%) | 52 (1.96%) | 63 (1.7%) | 41 (1.92%) |
| Drowning | 8 (0.31%) | 8 (0.33%) | 16 (0.55%) | 13 (0.49%) | 12 (0.32%) | 15 (0.7%) |
| Cutting | 232 (8.9%) | 227 (9.41%) | 284 (9.79%) | 249 (9.39%) | 352 (9.49%) | 176 (8.25%) |
| Self-poisoning with gases and vapors | 21 (0.81%) | 15 (0.62%) | 28 (0.97%) | 25 (0.94%) | 22 (0.59%) | 7 (0.33%) |
| Self-poisoning with solid or liquid substances | 2147 (82.36%) | 1937 (80.31%) | 2292 (79.03%) | 2156 (81.33%) | 3047 (82.13%) | 1751 (82.05%) |
| Firearms or explosives | 3 (0.12%) | 4 (0.17%) | 3 (0.1%) | 0 (0%) | 4 (0.11%) | 2 (0.09%) |
| Other autolytic attempts | 70 (2.69%) | 80 (3.32%) | 108 (3.72%) | 45 (1.7%) | 104 (2.8%) | 88 (4.12%) |
| Patient Destination | ||||||
| Hospital admission | 2929 (80.44%) | 3009 (82.71%) | 4117 (91.71%) | 3787 (88.25%) | 5873 (89.97%) | 3499 (90.39%) |
| Discharge at home | 712 (19.56%) | 629 (17.29%) | 372 (8.29%) | 504 (11.75%) | 655 (10.03%) | 372 (9.61%) |
| MINI Suicidal Risk | ||||||
| High | 2223 (61.05%) | 2117 (58.19%) | 2459 (54.78%) | 2232 (52.02%) | 3114 (47.7%) | 1896 (48.98%) |
| Moderate | 711 (19.53%) | 843 (23.17%) | 1006 (22.41%) | 968 (22.56%) | 1783 (27.31%) | 988 (25.52%) |
| Low | 623 (17.11%) | 611 (16.79%) | 919 (20.47%) | 989 (23.05%) | 1442 (22.09%) | 872 (22.53%) |
| No apparent risk | 84 (2.31%) | 67 (1.84%) | 105 (2.34%) | 102 (2.38%) | 189 (2.9%) | 115 (2.97%) |
| Previous attempt 3 | 1298 (35.65%) | 1327 (36.48%) | 1431 (31.88%) | 1332 (31.04%) | 1806 (27.67%) | 1013 (26.17%) |
| Suicide planning 3 | 686 (18.84%) | 553 (15.2%) | 674 (15.01%) | 592 (13.8%) | 810 (12.41%) | 498 (12.86%) |
| Current alcohol consumption | 640 (17.58%) | 587 (16.14%) | 756 (16.84%) | 696 (16.22%) | 879 (13.47%) | 511 (13.2%) |
| Current drug abuse | 442 (12.14%) | 437 (12.01%) | 550 (12.25%) | 523 (12.19%) | 698 (10.69%) | 391 (10.1%) |
| 2017 (N = 3641) | 2018 (N = 3638) | 2019 (N = 4489) | 2020 (N = 4291) | 2021 (N = 6528) | 2022 1 (N = 3871) | |
|---|---|---|---|---|---|---|
| Sociodemographic Characteristics | ||||||
| Age Groups | ||||||
| <18 | 412 (11.32%) | 503 (13.83%) | 473 (10.54%) | 601 (14.01%) | 1492 (22.86%) | 866 (22.37%) |
| 18–34 | 892 (24.5%) | 928 (25.51%) | 1294 (28.83%) | 1227 (28.59%) | 1768 (27.08%) | 1131 (29.22%) |
| 35–49 | 1194 (32.79%) | 1118 (30.73%) | 1387 (30.9%) | 1215 (28.32%) | 1608 (24.63%) | 894 (23.09%) |
| 40–64 | 807 (22.16%) | 772 (21.22%) | 934 (20.81%) | 906 (21.11%) | 1237 (18.95%) | 695 (17.95%) |
| >65 | 336 (9.23%) | 317 (8.71%) | 401 (8.93%) | 342 (7.97%) | 423 (6.48%) | 285 (7.36%) |
| Sex (female) | 2371 (65.12%) | 2394 (65.81%) | 2851 (63.51%) | 2801 (65.28%) | 4483 (68.67%) | 2655 (68.59%) |
| Family history of suicidal behavior | 135 (3.71%) | 119 (3.27%) | 129 (2.87%) | 124 (2.89%) | 174 (2.67%) | 92 (2.38%) |
| Stressful life events 2 | 2271 (62.37%) | 2236 (61.46%) | 2746 (61.17%) | 2642 (61.57%) | 3788 (58.03%) | 2248 (58.07%) |
| Social problems 3 | 883 (24.25%) | 848 (23.31%) | 1239 (27.6%) | 1144 (26.66%) | 1691 (25.9%) | 998 (25.78%) |
| Lack of family or social core | 530 (14.56%) | 530 (14.57%) | 628 (13.99%) | 597 (13.91%) | 894 (13.69%) | 489 (12.63%) |
| Living alone | 408 (11.21%) | 362 (9.95%) | 459 (10.22%) | 367 (8.55%) | 542 (8.3%) | 301 (7.78%) |
| Socioeconomic Level | ||||||
| High | 12 (0.33%) | 11 (0.3%) | 12 (0.27%) | 13 (0.3%) | 29 (0.44%) | 19 (0.49%) |
| Moderate | 634 (17.41%) | 626 (17.21%) | 711 (15.84%) | 881 (20.53%) | 1470 (22.52%) | 790 (20.41%) |
| Low or very low | 2972 (81.63%) | 2982 (81.97%) | 3741 (83.34%) | 3353 (78.14%) | 4970 (76.13%) | 2983 (77.06%) |
| NA | 23 (0.63%) | 19 (0.52%) | 25 (0.56%) | 44 (1.03%) | 59 (0.9%) | 79 (2.04%) |
| Clinical Characteristics | ||||||
| Feelings of hopelessness | 1796 (49.33%) | 1624 (44.64%) | 1958 (43.62%) | 1758 (40.97%) | 2673 (40.95%) | 1544 (39.89%) |
| Severe, disabling or painful somatic illness | 365 (10.02%) | 325 (8.93%) | 405 (9.02%) | 293 (6.83%) | 456 (6.99%) | 286 (7.39%) |
| Mental disorder | 1239 (34.03%) | 1165 (32.02%) | 1462 (32.57%) | 1256 (29.27%) | 1721 (26.36%) | 917 (23.69%) |
| Psychiatric history 4 | ||||||
| Drug abuse | 2023 (55.56%) | 2007 (55.17%) | 2521 (56.16%) | 2368 (55.19%) | 2548 (39.03%) | 1353 (34.95%) |
| Alzheimer | 13 (0.36%) | 11 (0.3%) | 14 (0.31%) | 12 (0.28%) | 9 (0.14%) | 9 (0.23%) |
| Sleep disorders | 478 (13.13%) | 500 (13.74%) | 690 (15.37%) | 662 (15.43%) | 914 (14%) | 522 (13.48%) |
| Personality disorders | 1267 (34.8%) | 1181 (32.46%) | 1464 (32.61%) | 1380 (32.16%) | 1651 (25.29%) | 794 (20.51%) |
| Bipolar disorders | 221 (6.07%) | 219 (6.02%) | 245 (5.46%) | 233 (5.43%) | 258 (3.95%) | 138 (3.56%) |
| Depression | 1365 (37.49%) | 1261 (34.66%) | 1438 (32.03%) | 1336 (31.13%) | 1619 (24.8%) | 819 (21.16%) |
| Anxiety | 2394 (65.75%) | 2421 (66.55%) | 3168 (70.57%) | 2982 (69.49%) | 3932 (60.23%) | 2126 (54.92%) |
| Eating disorders | 272 (7.47%) | 250 (6.87%) | 338 (7.53%) | 328 (7.64%) | 490 (7.51%) | 243 (6.28%) |
| Schizophrenia | 209 (5.74%) | 176 (4.84%) | 215 (4.79%) | 209 (4.87%) | 219 (3.35%) | 90 (2.32%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valero-Bover, D.; Fradera, M.; Carot-Sans, G.; Parra, I.; Piera-Jiménez, J.; Pontes, C.; Palao, D. Impact of the COVID-19 Pandemic on the Incidence of Suicidal Behaviors: A Retrospective Analysis of Integrated Electronic Health Records in a Population of 7.5 Million. Int. J. Environ. Res. Public Health 2022, 19, 14364. https://doi.org/10.3390/ijerph192114364
Valero-Bover D, Fradera M, Carot-Sans G, Parra I, Piera-Jiménez J, Pontes C, Palao D. Impact of the COVID-19 Pandemic on the Incidence of Suicidal Behaviors: A Retrospective Analysis of Integrated Electronic Health Records in a Population of 7.5 Million. International Journal of Environmental Research and Public Health. 2022; 19(21):14364. https://doi.org/10.3390/ijerph192114364
Chicago/Turabian StyleValero-Bover, Damià, Marc Fradera, Gerard Carot-Sans, Isabel Parra, Jordi Piera-Jiménez, Caridad Pontes, and Diego Palao. 2022. "Impact of the COVID-19 Pandemic on the Incidence of Suicidal Behaviors: A Retrospective Analysis of Integrated Electronic Health Records in a Population of 7.5 Million" International Journal of Environmental Research and Public Health 19, no. 21: 14364. https://doi.org/10.3390/ijerph192114364
APA StyleValero-Bover, D., Fradera, M., Carot-Sans, G., Parra, I., Piera-Jiménez, J., Pontes, C., & Palao, D. (2022). Impact of the COVID-19 Pandemic on the Incidence of Suicidal Behaviors: A Retrospective Analysis of Integrated Electronic Health Records in a Population of 7.5 Million. International Journal of Environmental Research and Public Health, 19(21), 14364. https://doi.org/10.3390/ijerph192114364