1. Introduction
The coronavirus disease 2019 (COVID-19), which spread all around the world after the first case in Wuhan in November 2019, induced isolation, stressful conditions related to the fear of dying and the many bereavements and socio-economic consequences. Since the beginning of the COVID-19 pandemic, many research studies have highlighted its great impact on mental health in the general population, with increased rates of depression, anxiety and PTSD in comparison with the prevalence of these psychiatric disorders before the COVID-19 pandemic [
1]. Several studies have highlighted the negative impacts of COVID-19 pandemic on the access to and quality of maternity health services, in particular in the early phase of the pandemic due to restrictions on partner and visitor attendance [
2,
3] or due to adaptive practices in maternal care with the use of telemedicine [
4]. Women also could potentially be anxious towards a risk of contamination for themselves or their fetus, but also towards vaccination against SARS-CoV-2 and its potential side effects. Data on the impact of COVID-19 pandemic on mental health issues for women who delivered during this period need to be explored further.
While between 20% and 48% of women report a traumatic experience associated with the delivery [
5,
6], the taboo that surrounds it maintains the idea that this phenomenon remains exceptional and that it is limited to situations of obstetrical complications. However, childbirth with no medical complications, whether obstetric or neonatal, can nevertheless also be experienced as traumatic and can lead to complications in the mental well-being of the mother, the father and the child. The authors of a recent meta-analysis suggested the use of the terminology of birth-related post-traumatic stress disorder (PTSD) to describe a PTSD resulting in a traumatic childbirth and concluded that 4.7% of mothers developed birth-related PTSD and 12.3% of mothers developed birth-related post-traumatic stress symptoms (PTSS) [
7]. Actually, a traumatic childbirth does not necessarily give rise to the development of birth-related PTSD, which is the most serious clinical evolution and can be limited to birth-related PTSS, which can include post-traumatic stress symptoms that are not sufficient to validate the criteria for a PTSD diagnosis.
Birth-related PTSD and birth-related PTSS are associated with deleterious effects on breastfeeding, which is more prematurely stopped [
8], as well as impacting child health and development, mother–child attachment and the quality of attachment [
9], with deleterious effects on the couple’s relationship [
10]. They are highly co-morbid with post-partum depression (PPD) [
11]. Despite these long-term consequences of birth-related PTSD, there is currently no routine prevention of PTSD implemented in most maternity services, unlike prevention strategies for PPD, which are most commonly developed. However, many predictors have been identified and confirmed by numerous robust studies [
9,
12,
13,
14]. According to a diathesis stress model of the aetiology of childbirth PTSD, risk factors are divided into three categories: pre-birth, peripartum and post-partum [
9,
12,
13,
14]. First, pre-birth vulnerability factors are involved, such as antenatal depression, fear of childbirth, poor health or complications in pregnancy, PTSD related to a previous traumatic event and counselling for pregnancy or birth, suggesting help being needed during pregnancy or birth [
8,
10,
11,
12]. Concerning birth, negative subjective birth experiences, having an operative birth (assisted vaginal or caesarean), a lack of support and dissociation appeared as the most important risk factors [
9,
12,
13,
14]. In high-risk samples of women that had pre-eclampsia or emergency caesarean sections (and not in other women), marital status, poor health or complications in pregnancy and negative emotions in birth influence the risk of birth-related PTSD [
9]. Concerning the post-partum period, PPD, other comorbid symptoms, stress and poor coping are identified risk factors related to childbirth PTSD [
15]. A recent meta-analysis highlighted controversial findings for risk factors underlying traumatic birth and birth-related PTSD, showing that the factors involved in traumatic childbirth are different from those involved in birth-related PTSD [
16].
A traumatic childbirth must validate the definition of a traumatic event according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) to diagnose birth-related PTSD [
17]. Although the majority of previous studies focusing on traumatic childbirth and birth-related PTSD have used the DSM-IV criteria, the DSM-IV/DSM-5 comparison study conducted by Kilpatrick and colleagues [
18] concluded that 60% of PTSD cases that met the DSM-IV criteria but not the proposed DSM-5 PTSD criteria were excluded from DSM-5.
Indeed, some significant conceptual changes concerning traumatic events and PTSD need to be mentioned. With DSM-5, some important differences concerning PTSD diagnoses in comparison with the last version, DSM-IV, have been highlighted [
19]. According to the definition of the 5th version of the DSM criteria (DSM-5) [
17], a traumatic event is no longer characterized by a subjective component as it was with DSM-IV. The definition of a traumatic event according to DSM-5 is the first and mandatory criterion to diagnose a PTSD and consists of being exposed to death, serious injury or sexual violence, whether actual or potential. Consequently, this definition excludes stressful events that do not involve an immediate threat to life or physical injury, such as psychosocial stressors, although a subjective definition was used in DSM-IV, namely a “threat to physical integrity”, which was the origin of many critiques and the idea that the definition of a traumatic event in DSM-IV was too inclusive [
19].
According to the DSM-5 criteria, a birth-related PTSD diagnosis needs to validate the definition of a traumatic event (criterion A1) and the individual needs to re-experience the traumatic event related to childbirth (criterion B1), present avoidance symptoms (criterion C1), develop alterations in cognition and mood (criterion D1), experience alterations in arousal and hyperactivity (criterion E1) and experience these symptoms for more than one month (criterion F1). The symptoms must also create distress or a functional impairment (criterion G1) and must validate an exclusion criterion regarding medication, substance use or other illnesses that could explain the symptoms (criterion H1) [
17].
Although the prevalence of birth-related PTSD and its predictors have been studied in many Western countries before COVID-19 pandemic, there are limited data reported in Switzerland [
15] so far to be used as comparative data. We initiated a cross-sectional study to estimate the prevalence of traumatic childbirth, birth-related PTSD, post-partum depression and breastfeeding before the pandemic COVID-19 had occurred, but we started the collection of data during the COVID-19 pandemic. Taking account of this unexpected context for our research, we decided to provide an assessment of stress factors directly related to the COVID-19 pandemic and to analyze their associations with traumatic childbirth and birth-related PTSD, in addition to the known risk factors for birth-related PTSD.
We wanted to assess whether the COVID-19 pandemic (1) increases the risks of traumatic childbirth, childbirth-related PTSD and post-partum depression; and (2) alters the influence of known factors of childbirth-related PTSD. We hypothesized that stress factors related to the COVID-19 pandemic increase the prevalence rates of traumatic childbirth-related PTSD and post-partum depression and that the influence of known factors involved in these clinical context have been modified during the COVID-19 pandemic. The study’s main objective was to assess the prevalence rates of traumatic childbirth and birth-related PTSD in women who delivered during the COVID-19 pandemic. The main secondary objective was first to analyze the already known factors related to COVID-19 associated with traumatic childbirth and birth-related PTSD, while the final secondary objectives were to evaluate whether the presence of birth-related PTSD may be associated with a greater risk of developing comorbid post-partum depression at one month post-partum and to assess the association of breastfeeding practices with birth-related PTSD.
2. Materials and Methods
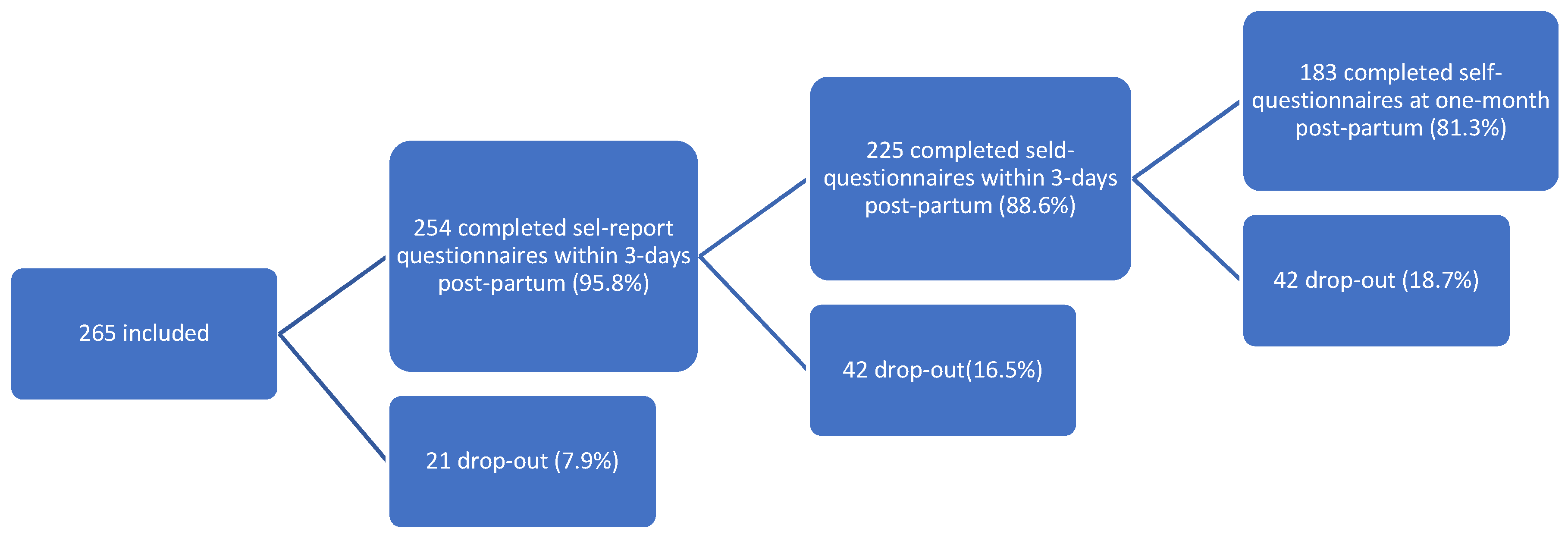
This was a prospective cohort study of all women who delivered at the University Hospitals of Geneva between 25 January 2021 and 10 March 2022 with two follow-up time-points: an early assessment within 3 days of delivery and a visit at one month post-partum. This hospital manages pregnancies and deliveries at high risk of complications and complex psychosocial situations. The eligibility criteria were any woman older than 18 years who delivered at the Geneva University Hospitals’ maternity wards after 29 weeks of amenorrhea (w.a.) and who consented to participate. We conducted a physical interview in their room during maternity to inform them of and to check the inclusion criteria. Women who did not read or speak fluent French were excluded. The recruitment started after childbirth and within 3 days of the maternity stay.
Once eligible, the participating mothers received an e-mail on their smartphone and completed an online self-report questionnaire within 3 days of their maternity stay and at one month post-partum. During the first assessment, they completed self-report questionnaires for the following variables: (1) age, nationality and current profession; (2) data about delivery routes, whereby maternal or neonatal complications were collected on medical files, support and information provided by healthcare workers during delivery; (3) antenatal depression; (4) peritraumatic reactions around childbirth; (5) psychiatric history and previous psychiatric treatments; (6) questions related to COVID-19 regarding pregnancy and the maternity stay. During the second assessment, at one month post-partum, the mothers completed self-report questionnaires for the following variables: (1) birth-related PTSD; (2) previous traumatic events according to the DSM-5 criteria; (3) questions related to COVID-19 during the post-partum period; (4) breastfeeding; (5) perceived support by the patient’s entourage. They also received a teleconsultation to look for diagnoses of birth-related PTSD and post-partum depression according to DSM-5 criteria. In case of no answer, three automatic reminders were provided by e-mail.
Depending on the results of the assessment of birth-related PTSD or post-partum depression, a referral to a mental health specialist was proposed, independently of the study.
We describe our outcomes in detail and the tools we used above for each step of the study.
2.1. Primary and Secondary Outcomes
At one month post-partum, the participating women were invited to a clinical interview through a teleconsultation conducted by an experimented psychologist or psychiatrist of research team that had each more than 5 years of clinical experience. To validate the criteria for the presence of traumatic childbirth (primary outcome), the clinician checked if criterion A according to DSM-5 for traumatic events corresponded to the last childbirth; then, the other diagnostic criteria for birth-related PTSD according to the DSM-5 criteria were searched (secondary outcome) [
17]. The clinician also searched for the presence of PPD according to the criteria for DSM-5 (secondary outcome) [
17]. Information regarding stopping or not breastfeeding at one month was collected during this clinical interview (secondary outcome) [
8]. The self-report questionnaire included items for the French validation of the PTSD Checklist for DSM-5, assessing the 20 DSM-5 symptoms of PTSD, which we used to evaluate the intensity of birth-related PTSD [
20,
21].
2.2. Known Risk Factors of Birth-Related PTSD
We searched known risk factors of birth-related PTSD during maternity stays, such as antenatal depression [
11,
14] using the French translation of the Edinburgh Post-Partum Depression Scale (EPDS), a set of 10 screening questions used to identify women who may have post-partum depression, with each answer being scored from 0 to 3 [
22,
23] and with a total score higher than 11 being interpreted as antenatal depression. The modalities of childbirth (delivery route, instrumented delivery, maternal and neonatal complications) [
7,
11] and the level of satisfaction with the quality of care, support and medical information provided by healthcare workers (HCW) were evaluated on a 5-point Likert scale [
7,
11]. The presence of a peritraumatic reaction linked the delivery was assessed using the French version of The Peritraumatic Distress Inventory, a 13-item self-report questionnaire that measures the level of distress experienced by an individual during and shortly after a traumatic event [
24,
25], and the Peritraumatic Dissociative Experiences Questionnaire, a self-report inventory used to assess dissociation occurring at the time of the trauma [
26,
27] which is known as a predictive factor of related to childbirth PTSD [
28]. For both tools, the assessment was considered as positive if the total score was higher than 15 [
24,
26]. The participating women were also interviewed about the use of a previous psychotropic treatment, the presence of previous traumatic events (including traumatic childbirth according to DSM-5 and specific types of previous traumatic events, e.g., physical, sexual aggression, severe disease) [
7,
11]. We tested the perceived social support using the 5-point Likert scale during the post-partum period [
29].
2.3. Other Variables and Confounding Factors
We tested potential risk factors of birth-related PTSD that are related to the COVID-19 pandemic and that are not known. We provided questions using the 5-point Likert scale concerning access to care for their pregnancy and the newborn after delivery and access to care for physical or mental health, during pregnancy and the post-partum period, concerning the effects of isolation from their relatives, the economic consequences, the use of teleworking, the fear of being infected by SARS-CoV-2, the perception of the restrictions of visits during maternity stay, the presence of infected persons in close contact with delivering women during COVID-19, the impact of the COVID-19 context on the experience of pregnancy and delivery and the received social support. We also assessed for contamination by SARS-CoV-2 during pregnancy.
2.4. Data Use and Recording
All medical and socio-demographic data were recorded using the REDCap electronic data capture tools hosted at the University Hospitals of Geneva, Switzerland [
30]. If the participant did not attend the one month consultation, she was considered as a drop-out. In cases of premature exit from the study, before the first month post-partum, the coded data collected were recorded using REDCap and then used for the analysis of the results.
2.5. Statistical Analysis
We anticipated that 200 participants would be needed to be able to estimate the prevalence of birth-related PTSD at 4% with a precision of ±2.7% using a 95% confidence interval (95% CI).
The continuous variables were described using the mean ± standard deviation (SD), median and interquartile range; the categorical variables by frequencies and relative proportions. We reported the prevalence of PTSD due to traumatic childbirth or breastfeeding at one month with the 95% CI using the exact binomial method. We assessed the associations between different factors (socio-demographic, clinical and related to COVID-19) with the four outcomes (traumatic childbirth, birth-related PTSD, post-partum depression and breastfeeding) separately by applying four different logistic regression models. For each outcome, we provided univariate analyses then we constructed multivariable models if we had a minimal number of events per variable. We used a stepwise approach by choosing all variables associated with the outcome at p < 0.25 in the univariate analyses, then we kept in the final multivariable models all variables that were significantly associated with the outcome (parsimonious) and also variables that showed a confounding effect by changing the coefficient of regression by more than 25% after being stepped out of the model. We verified the adequacy of each model using the Hosmer–Lemeshow test. We provided the pseudo-R2 value to assess the predictive value of the model. We reported the associations between the factors and outcomes using their odds ratios (ORs) and 95% confidence intervals (95% CI). All p-values below 0.05 were considered statistically significant.
5. Conclusions
To the best of our knowledge, this is the first study to have explored traumatic childbirth and birth-related PTSD according to DSM-5 in Switzerland during the COVID-19 pandemic and the related risk and protective factors. The prevalence rates of traumatic childbirth and birth-related PTSD were not as high as expected. The results regarding known risk factors such as antenatal depression, a previous traumatic event of any type, neonatal complications, peritraumatic distress and peritraumatic dissociation were consistent with the literature for birth-related PTSD, but we found no influence of a psychiatric history or of the delivery route. Women who suffered from limited access to pre-natal care due to the COVID-19 pandemic during their pregnancy were more at risk of developing a birth-related PTSD, but we were not able to draw a conclusion regarding the influence of the other factors related to the COVID-19 pandemic, such as fear of contamination, isolation or socio-economic change due to COVID-19, on birth-related PTSD or traumatic childbirth. During the maternity stay, the approach for the prevention of birth-related PTSD should focus on antenatal depression screening, which appears as the main antenatal risk factor, and on peritraumatic dissociation, which appears as the main peripartum factor, so as to detect women at risk of being exposed to traumatic childbirth and to developing birth-related PTSD. Attention should be placed on the education of the medical staff and midwives regarding the post-natal PTSD risks so as to better clinically identify and manage peritraumatic dissociation around childbirth.



 and
and 
{kind=link}
