
Biomass Smoke Exposure and Atopy among Young Children in the Western Highlands of Guatemala: A Prospective Cohort Study

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Biomass Smoke Exposure
2.3. Skin Prick Tests
2.4. Allergic Outcome Questionnaires
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of Variance |
| CI | Confidence Interval |
| CO | Carbon Monoxide |
| CRECER | The Chronic Respiratory Effects of Early Childhood Exposure to Respirable PM cohort study |
| HAP | Household Air Pollution |
| ISAAC | International Study of Asthma and Allergies in Childhood |
| OR | Odds Ratio |
| PM | Particulate Matter |
| QRQ | Quarterly Respiratory Questionnaire |
| RCT | Randomized Controlled Trial |
| RESPIRE | the Randomized Exposure Study of Pollution Indoors and Respiratory Effects |
| SD | Standard Deviation |
| SES | Socioeconomic Status |
| SPT | Skin Prick Test |
| Th | T Helper cells |
Appendix A

{kind=link}
{kind=link}
| Time | Values | Main Analysis | Alternative 1 | Alternative 2 | Alternative 3 |
|---|---|---|---|---|---|
| Birth | X1 | X1 | X1 | (X1 + X2 + X3)/3 | |
| - | X1 | X1 | X1 | (X1 + X2 + X3)/3 | |
| RESPIRE CO tube 1 | X1 | X1 | X1 | X1 | (X1 + X2 + X3)/3 |
| - | X2 | X2 | X2 | (X1 + X2 + X3)/3 | |
| RESPIRE CO tube 2 | X2 | X2 | X2 | X2 | (X1 + X2 + X3)/3 |
| - | X3 | X3 | X3 | (X1 + X2 + X3)/3 | |
| Last RESPIRE CO tube | X3 | X3 | X3 | X3 | (X1 + X2 + X3)/3 |
| - | X3 | (X3 + X4)/2 | X4 | (X1 + X2 + X3)/3 | |
| ~18 months old (600 days) | X3 | (X3 + X4)/2 | X4 | (X4 + X5 + X6 + X7)/3 | |
| - | X4 | (X3 + X4)/2 | X4 | (X4 + X5 + X6 + X7)/3 | |
| - | X4 | (X3 + X4)/2 | X4 | (X4 + X5 + X6 + X7)/3 | |
| - | X4 | (X3 + X4)/2 | X4 | (X4 + X5 + X6 + X7)/3 | |
| CRECER CO tube 1 | X4 | X4 | X4 | X4 | (X4 + X5 + X6 + X7)/3 |
| - | X5 | X5 | X5 | (X4 + X5 + X6 + X7)/3 | |
| CRECER CO tube 2 | X5 | X5 | X5 | X5 | (X4 + X5 + X6 + X7)/3 |
| - | X6 | X6 | X6 | (X4 + X5 + X6 + X7)/3 | |
| Last CRECER CO tube before first QRQ | X6 | X6 | X6 | X6 | (X4 + X5 + X6 + X7)/3 |
| - | X6 | X6 | X6 | (X4 + X5 + X6 + X7)/3 | |
| First QRQ | X6 | X6 | X6 | (X4 + X5 + X6 + X7)/3 | |
| - | 0 | 0 | 0 | 0 | |
| CRECER CO tube after first QRQ | X7 | 0 | 0 | 0 | 0 |
| Study | Country | Exposure | Outcome | Measure of Association (95% CIs) |
|---|---|---|---|---|
| This study | Guatemala (rural) | Open fire vs. chimney stove | Asthma symptoms | OR = 2.42 (1.11–5.48) |
| This study | Guatemala (rural) | Open fire vs. chimney stove | Rhinitis symptoms | OR = 2.01 (1.13–3.58) |
| This study | Guatemala (rural) | Open fire vs. chimney stove | Eczema | OR = 1.02 (0.92–1.12) |
| This study | Guatemala (rural) | Biomass-related cumulative CO (ppm-year) | Rhinitis symptoms | OR = 1.09 (1.02–1.18) |
| This study | Guatemala (rural) | Open fire vs. chimney stove | Sensitization to aeroallergen | OR ranges from 0.72 to 1.67, p > 0.05 |
| Honicky et al. [35] | USA | Wood stove vs. gas stove | Respiratory illness symptoms | p < 0.001 |
| Morris et al. [36] | USA | Wood stove | Lower respiratory tract infection | OR = 4.85 (1.69–12.91) |
| Von Mutius et al. * [20] | Germany (rural) | Coal/wood heating | Sensitization to aeroallergen | OR = 0.67 (0.49–0.93) |
| Von Mutius et al. * [20] | Germany (rural) | Coal/wood heating | Hay fever | OR = 0.57 (0.34–0.98) |
| Kilpelainen, M. et al. [21] | Germany | Wood stove heating | Allergic rhinitis | OR = 0.96 (0.77–1.20) |
| Vicedo-Cabrera, A.M. et al. [22] | Spain | Biomass cooking | Eczema | OR = 1.51 (0.60–3.81) |
| Vicedo-Cabrera, A.M. et al. [22] | Spain | Biomass heating | Eczema | OR = 1.02 (0.82–3.25) |
| Schei et al. [23] | Guatemala | Open fire cooking | Any asthma symptoms | OR = 3.4 (1.3–8.5) |
| Schei et al. [23] | Guatemala | Open fire cooking | Asthma diagnosis | OR =1.8 (0.76–4.19) |
| Oluwole et al. [15] | Nigeria (rural) | Biomass cooking | Asthma symptoms | OR =1.33 (1.05–1.69) |
| Thacher et al. [16] | Nigeria | Biomass cooking | Asthma symptoms | OR = 2.36, (0.66–8.44) |
References
- World Health Organization (WHO). Household Air Pollution and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/household-air-pollution-and-health (accessed on 28 July 2022).
- Lee, K.K.; Bing, R.; Kiang, J.; Bashir, S.; Spath, N.; Stelzle, D.; Mortimer, K.; Bularga, A.; Doudesis, D.; Joshi, S.S.; et al. Adverse health effects associated with household air pollution: A systematic review, meta-analysis, and burden estimation study. Lancet Glob. Health 2020, 8, e1427–e1434. [Google Scholar] [CrossRef]
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.B.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J.; et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef]
- Heinzerling, A.P.; Guarnieri, M.J.; Mann, J.K.; Diaz, J.V.; Thompson, L.M.; Diaz, A.; Bruce, N.G.; Smith, K.R.; Balmes, J.R. Lung function in woodsmoke-exposed Guatemalan children following a chimney stove intervention. Thorax 2016, 71, 421–428. [Google Scholar] [CrossRef]
- Po, J.Y.; FitzGerald, J.M.; Carlsten, C. Respiratory disease associated with solid biomass fuel exposure in rural women and children: Systematic review and meta-analysis. Thorax 2011, 66, 232–239. [Google Scholar] [CrossRef]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S.C. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: A systematic review and a meta-analysis of birth cohort studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef]
- Morgenstern, V.; Zutavern, A.; Cyrys, J.; Brockow, I.; Koletzko, S.; Kramer, U.; Behrendt, H.; Herbarth, O.; von Berg, A.; Bauer, C.P.; et al. Atopic diseases, allergic sensitization, and exposure to traffic-related air pollution in children. Am. J. Respir. Crit. Care Med. 2008, 177, 1331–1337. [Google Scholar] [CrossRef]
- Brandt, E.B.; Myers, J.M.; Ryan, P.H.; Hershey, G.K. Air pollution and allergic diseases. Curr. Opin. Pediatr. 2015, 27, 724–735. [Google Scholar] [CrossRef]
- Ahn, K. The role of air pollutants in atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 993–1000. [Google Scholar] [CrossRef]
- Brandt, E.B.; Biagini Myers, J.M.; Acciani, T.H.; Ryan, P.H.; Sivaprasad, U.; Ruff, B.; LeMasters, G.K.; Bernstein, D.I.; Lockey, J.E.; LeCras, T.D.; et al. Exposure to allergen and diesel exhaust particles potentiates secondary allergen-specific memory responses, promoting asthma susceptibility. J. Allergy Clin. Immunol. 2015, 136, 295–303.e7. [Google Scholar] [CrossRef]
- Codispoti, C.D.; LeMasters, G.K.; Levin, L.; Reponen, T.; Ryan, P.H.; Biagini Myers, J.M.; Villareal, M.; Burkle, J.; Evans, S.; Lockey, J.E.; et al. Traffic pollution is associated with early childhood aeroallergen sensitization. Ann. Allergy Asthma Immunol. 2015, 114, 126–133. [Google Scholar] [CrossRef]
- Thacher, J.D.; Gruzieva, O.; Pershagen, G.; Neuman, A.; van Hage, M.; Wickman, M.; Kull, I.; Melen, E.; Bergstrom, A. Parental smoking and development of allergic sensitization from birth to adolescence. Allergy 2016, 71, 239–248. [Google Scholar] [CrossRef]
- Gallant, M.J.; Ellis, A.K. Prenatal and early-life exposure to indoor air-polluting factors and allergic sensitization at 2 years of age. Ann. Allergy Asthma Immunol. 2020, 124, 283–287. [Google Scholar] [CrossRef]
- Balmes, J.R. Household air pollution from domestic combustion of solid fuels and health. J. Allergy Clin. Immunol. 2019, 143, 1979–1987. [Google Scholar] [CrossRef]
- Oluwole, O.; Arinola, G.O.; Huo, D.; Olopade, C.O. Biomass fuel exposure and asthma symptoms among rural school children in Nigeria. J. Asthma 2017, 54, 347–356. [Google Scholar] [CrossRef]
- Thacher, J.D.; Emmelin, A.; Madaki, A.J.; Thacher, T.D. Biomass fuel use and the risk of asthma in Nigerian children. Respir. Med. 2013, 107, 1845–1851. [Google Scholar] [CrossRef]
- Kumar, R.; Nagar, J.K.; Goel, N.; Kumar, P.; Kushwah, A.S.; Gaur, S.N. Indoor air pollution and asthma in children at Delhi, India. Pneumonol. Alergol. Pol. 2015, 83, 275–282. [Google Scholar] [CrossRef]
- Kumar, R.; Nagar, J.K.; Raj, N.; Kumar, P.; Kushwah, A.S.; Meena, M.; Gaur, S.N. Impact of domestic air pollution from cooking fuel on respiratory allergies in children in India. Asian Pac. J. Allergy Immunol. 2008, 26, 213–222. [Google Scholar]
- Norbäck, D.; Lu, C.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Sun, Y.; Wang, J.; et al. Sources of indoor particulate matter (PM) and outdoor air pollution in China in relation to asthma, wheeze, rhinitis and eczema among pre-school children: Synergistic effects between antibiotics use and PM10 and second hand smoke. Environ. Int. 2019, 125, 252–260. [Google Scholar] [CrossRef]
- von Mutius, E.; Illi, S.; Nicolai, T.; Martinez, F.D. Relation of indoor heating with asthma, allergic sensitisation, and bronchial responsiveness: Survey of children in south Bavaria. BMJ (Clin. Res. Ed.) 1996, 312, 1448–1450. [Google Scholar] [CrossRef]
- Kilpelainen, M.; Koskenvuo, M.; Helenius, H.; Terho, E. Wood stove heating, asthma and allergies. Respir. Med. 2001, 95, 911–916. [Google Scholar] [CrossRef]
- Vicedo-Cabrera, A.M.; Garcia-Marcos, L.; Llopis-Gonzalez, A.; Lopez-Silvarrey-Varela, A.; Miner-Canflanca, I.; Batlles-Garrido, J.; Blanco-Quiros, A.; Busquets-Monge, R.M.; Diaz-Vazquez, C.; Gonzalez-Diaz, C.; et al. Atopic dermatitis and indoor use of energy sources in cooking and heating appliances. BMC Public Health 2012, 12, 890. [Google Scholar] [CrossRef]
- Schei, M.A.; Hessen, J.O.; Smith, K.R.; Bruce, N.; McCracken, J.; Lopez, V. Childhood asthma and indoor woodsmoke from cooking in Guatemala. J. Expo. Anal. Environ. Epidemiol. 2004, 14 (Suppl. S1), S110–S117. [Google Scholar] [CrossRef]
- Smith, K.R.; McCracken, J.P.; Weber, M.W.; Hubbard, A.; Jenny, A.; Thompson, L.M.; Balmes, J.; Diaz, A.; Arana, B.; Bruce, N. Effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE): A randomised controlled trial. Lancet 2011, 378, 1717–1726. [Google Scholar] [CrossRef]
- Smith-Sivertsen, T.; Diaz, E.; Pope, D.; Lie, R.T.; Diaz, A.; McCracken, J.; Bakke, P.; Arana, B.; Smith, K.R.; Bruce, N. Effect of reducing indoor air pollution on women’s respiratory symptoms and lung function: The RESPIRE Randomized Trial, Guatemala. Am. J. Epidemiol. 2009, 170, 211–220. [Google Scholar] [CrossRef]
- Northcross, A.; Chowdhury, Z.; McCracken, J.; Canuz, E.; Smith, K.R. Estimating personal PM2.5 exposures using CO measurements in Guatemalan households cooking with wood fuel. J. Environ. Monit. 2010, 12, 873–878. [Google Scholar] [CrossRef]
- McCracken, J.P.; Schwartz, J.; Diaz, A.; Bruce, N.; Smith, K.R. Longitudinal relationship between personal CO and personal PM2.5 among women cooking with woodfired cookstoves in Guatemala. PLoS ONE 2013, 8, e55670. [Google Scholar] [CrossRef]
- Naeher, L.P.; Smith, K.R.; Leaderer, B.P.; Neufeld, L.; Mage, D.T. Carbon Monoxide as a Tracer for Assessing Exposures to Particulate Matter in Wood and Gas Cookstove Households of Highland Guatemala. Environ. Sci. Technol. 2001, 35, 575–581. [Google Scholar] [CrossRef]
- Smith, K.R.; McCracken, J.P.; Thompson, L.; Edwards, R.; Shields, K.N.; Canuz, E.; Bruce, N. Personal child and mother carbon monoxide exposures and kitchen levels: Methods and results from a randomized trial of woodfired chimney cookstoves in Guatemala (RESPIRE). J. Expo. Sci. Environ. Epidemiol. 2010, 20, 406–416. [Google Scholar] [CrossRef]
- McCracken, J.P.; Schwartz, J.; Bruce, N.; Mittleman, M.; Ryan, L.M.; Smith, K.R. Combining individual- and group-level exposure information: Child carbon monoxide in the Guatemala woodstove randomized control trial. Epidemiology 2009, 20, 127–136. [Google Scholar] [CrossRef]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.W.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- Thompson, L.; Diaz, J.; Jenny, A.; Diaz, A.; Bruce, N.; Balmes, J. Nxwisen, ntzarrin or ntzo’lin? Mapping children’s respiratory symptoms among indigenous populations in Guatemala. Soc. Sci. Med. 2007, 65, 1337–1350. [Google Scholar] [CrossRef]
- Matsui, E.C.; Wood, R.A.; Rand, C.; Kanchanaraksa, S.; Swartz, L.; Curtin-Brosnan, J.; Eggleston, P.A. Cockroach allergen exposure and sensitization in suburban middle-class children with asthma. J. Allergy Clin. Immunol. 2003, 112, 87–92. [Google Scholar] [CrossRef]
- Kossove, D. Smoke-filled rooms and lower respiratory disease in infants. S. Afr. Med. J. 1982, 61, 622–624. [Google Scholar]
- Honicky, R.E.; Osborne, J.S., III; Akpom, C.A. Symptoms of respiratory illness in young children and the use of wood-burning stoves for indoor heating. Pediatrics 1985, 75, 587–593. [Google Scholar] [CrossRef]
- Morris, K.; Morgenlander, M.; Coulehan, J.L.; Gahagen, S.; Arena, V.C. Wood-burning stoves and lower respiratory tract infection in American Indian children. Am. J. Dis. Child. 1990, 144, 105–108. [Google Scholar] [CrossRef]
- Miller, R.L.; Chew, G.L.; Bell, C.A.; Biedermann, S.A.; Aggarwal, M.; Kinney, P.L.; Tsai, W.Y.; Whyatt, R.M.; Perera, F.P.; Ford, J.G. Prenatal exposure, maternal sensitization, and sensitization in utero to indoor allergens in an inner-city cohort. Am. J. Respir. Crit. Care Med. 2001, 164, 995–1001. [Google Scholar] [CrossRef]
- Ege, M.J.; Herzum, I.; Büchele, G.; Krauss-Etschmann, S.; Lauener, R.P.; Roponen, M.; Hyvärinen, A.; Vuitton, D.A.; Riedler, J.; Brunekreef, B.; et al. Prenatal exposure to a farm environment modifies atopic sensitization at birth. J. Allergy Clin. Immunol. 2008, 122, 407–412.e404. [Google Scholar] [CrossRef]
- Kerkhof, M.; Wijga, A.; Smit, H.A.; De Jongste, J.C.; Aalberse, R.C.; Brunekreef, B.; Gerritsen, J.; Postma, D.S.; PIAMA Study Group. The effect of prenatal exposure on total IgE at birth and sensitization at twelve months and four years of age: The PIAMA study. Pediatr. Allergy Immunol. 2005, 16, 10–18. [Google Scholar] [CrossRef]
- Al-Tamprouri, C.; Malin, B.; Bill, H.; Lennart, B.; Anna, S. Cat and dog ownership during/after the first year of life and risk for sensitization and reported allergy symptoms at age 13. Immun. Inflamm. Dis. 2019, 7, 250–257. [Google Scholar] [CrossRef]
- Gern, J.E.; Reardon, C.L.; Hoffjan, S.; Nicolae, D.; Li, Z.; Roberg, K.A.; Neaville, W.A.; Carlson-Dakes, K.; Adler, K.; Hamilton, R.; et al. Effects of dog ownership and genotype on immune development and atopy in infancy. J. Allergy Clin. Immunol. 2004, 113, 307–314. [Google Scholar] [CrossRef]
- Wills-Karp, M.; Santeliz, J.; Karp, C.L. The germless theory of allergic disease: Revisiting the hygiene hypothesis. Nat. Rev. Immunol. 2001, 1, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Guarner, F.; Bourdet-Sicard, R.; Brandtzaeg, P.; Gill, H.S.; McGuirk, P.; van Eden, W.; Versalovic, J.; Weinstock, J.V.; Rook, G.A. Mechanisms of disease: The hygiene hypothesis revisited. Nat. Clin. Pract. Gastroenterol. Hepatol. 2006, 3, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Garn, H.; Renz, H. Epidemiological and immunological evidence for the hygiene hypothesis. Immunobiology 2007, 212, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, S.F.; Stanwell-Smith, R.; Crevel, R.W.R.; Pickup, J. Too clean, or not too clean: The Hygiene Hypothesis and home hygiene. Clin. Exp. Allergy 2006, 36, 402–425. [Google Scholar] [CrossRef]
- Cooper, P.J. Intestinal worms and human allergy. Parasite Immunol. 2004, 26, 455–467. [Google Scholar] [CrossRef]
- Bisgaard, H.; Li, N.; Bonnelykke, K.; Chawes, B.L.K.; Skov, T.; Paludan-Müller, G.; Stokholm, J.; Smith, B.; Krogfelt, K.A. Reduced diversity of the intestinal microbiota during infancy is associated with increased risk of allergic disease at school age. J. Allergy Clin. Immunol. 2011, 128, 646–652.e645. [Google Scholar] [CrossRef]
- Li, R.; Kou, X.; Xie, L.; Cheng, F.; Geng, H. Effects of ambient PM2.5 on pathological injury, inflammation, oxidative stress, metabolic enzyme activity, and expression of c-fos and c-jun in lungs of rats. Environ. Sci. Pollut. Res. Int. 2015, 22, 20167–20176. [Google Scholar] [CrossRef]
- Liu, K.; Hua, S.; Song, L. PM2.5 Exposure and Asthma Development: The Key Role of Oxidative Stress. Oxidative Med. Cell. Longev. 2022, 2022, 3618806. [Google Scholar] [CrossRef]
- Bekki, K.; Ito, T.; Yoshida, Y.; He, C.; Arashidani, K.; He, M.; Sun, G.; Zeng, Y.; Sone, H.; Kunugita, N.; et al. PM2.5 collected in China causes inflammatory and oxidative stress responses in macrophages through the multiple pathways. Environ. Toxicol. Pharmacol. 2016, 45, 362–369. [Google Scholar] [CrossRef]
- Zhao, C.; Wang, Y.; Su, Z.; Pu, W.; Niu, M.; Song, S.; Wei, L.; Ding, Y.; Xu, L.; Tian, M.; et al. Respiratory exposure to PM2.5 soluble extract disrupts mucosal barrier function and promotes the development of experimental asthma. Sci. Total Environ. 2020, 730, 139145. [Google Scholar] [CrossRef]
- Schelegle, E.S.; Miller, L.A.; Gershwin, L.J.; Fanucchi, M.V.; Van Winkle, L.S.; Gerriets, J.E.; Walby, W.F.; Mitchell, V.; Tarkington, B.K.; Wong, V.J.; et al. Repeated episodes of ozone inhalation amplifies the effects of allergen sensitization and inhalation on airway immune and structural development in Rhesus monkeys. Toxicol. Appl. Pharmacol. 2003, 191, 74–85. [Google Scholar] [CrossRef]
- Avdalovic, M.V.; Tyler, N.K.; Putney, L.; Nishio, S.J.; Quesenberry, S.; Singh, P.J.; Miller, L.A.; Schelegle, E.S.; Plopper, C.G.; Vu, T.; et al. Ozone Exposure During thE Early Postnatal Period Alters the Timing and Pattern of Alveolar Growth and Development in Nonhuman Primates. Anat. Rec. 2012, 295, 1707–1716. [Google Scholar] [CrossRef]
- Swiston, J.R.; Davidson, W.; Attridge, S.; Li, G.T.; Brauer, M.; van Eeden, S.F. Wood smoke exposure induces a pulmonary and systemic inflammatory response in firefighters. Eur. Respir. J. 2008, 32, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Kunzli, N.; Avol, E.; Wu, J.; Gauderman, W.J.; Rappaport, E.; Millstein, J.; Bennion, J.; McConnell, R.; Gilliland, F.D.; Berhane, K.; et al. Health effects of the 2003 Southern California wildfires on children. Am. J. Respir. Crit. Care Med. 2006, 174, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Adewole, O.O.; Desalu, O.O.; Nwogu, K.C.; Adewole, T.O.; Erhabor, G.E. Respiratory symptoms and lung function patterns in workers exposed to wood smoke and cooking oil fumes (mai suya) in Nigeria. Ann. Med. Health Sci. Res. 2013, 3, 38–42. [Google Scholar] [CrossRef] [PubMed]


| Group 1 | Group 2 | Group 3 | |
|---|---|---|---|
| Plancha installation age | (<6 months) | (~18 months) | (~57 months) |
| Number of children | n = 188 | n = 192 | n = 157 |
| Sex | |||
| Female | 99 (52.7%) | 101 (52.6%) | 82 (52.2%) |
| Age at first allergy questionnaire | |||
| Mean (SD) | 3.57 (0.487) | 3.55 (0.561) | 3.57 (0.756) |
| Maternal race | |||
| Indigenous (Mam) | 185 (98.4%) | 190 (99.0%) | 156 (99.4%) |
| Paternal race | |||
| Indigenous (Mam) | 177 (94.1%) | 186 (96.9%) | 156 (99.4%) |
| Number of children in household | |||
| Mean (SD) | 5.01 (2.37) | 4.98 (2.41) | 4.69 (2.42) |
| Second-hand smoke | |||
| Smoker in household | 14 (7.4%) | 22 (11.5%) | 16 (10.2%) |
| Kitchen type | |||
| Single structure, open kitchen | 31 (16.5%) | 31 (16.1%) | 17 (10.8%) |
| Single structure, partitioned kitchen | 12 (6.4%) | 8 (4.2%) | 7 (4.5%) |
| Separate structure, open kitchen | 19 (10.1%) | 18 (9.4%) | 30 (19.1%) |
| Separate structure, partitioned kitchen | 126 (67.0%) | 135 (70.3%) | 103 (65.6%) |
| Temazcal (native steam bath) use | |||
| Temascal at home | 147 (78.2%) | 147 (76.6%) | 117 (74.5%) |
| Average weekly temascal use time of the child (minutes): mean (SD) | 26.3 (17.3) | 26.8 (19.9) | 27.6 (17.0) |
| Pets and farm animals at home | |||
| Cattle: mean (SD) | 0.62 (0.91) | 0.55 (0.78) | 0.59 (0.85) |
| Sheep: mean (SD) | 1.62 (3.69) | 1.25 (2.20) | 1.58 (3.21) |
| Horses, mules, donkeys: mean (SD) | 0.27 (0.53) | 0.34 (0.58) | 0.31 (0.60) |
| Pigs: mean (SD) | 1.82 (1.86) | 1.54 (1.50) | 1.52 (1.61) |
| Poultry: (y/n) | 180 (95.7%) | 179 (93.2%) | 152 (96.8%) |
| Dogs: (y/n) | 170 (90.4%) | 177 (92.2%) | 127 (80.9%) |
| Cats: (y/n) | 89 (47.3%) | 81 (42.2%) | 61 (38.9%) |
| Pigeons: (y/n) | 15 (8.0%) | 13 (6.8%) | 16 (10.2%) |
| Other animals: (y/n) | 21 (11.2%) | 15 (7.8%) | 18 (11.5%) |
| Family history of allergic outcomes | |||
| Maternal asthma | 30 (16.0%) | 33 (17.2%) | 52 (33.1%) |
| Maternal rhinitis | 20 (10.6%) | 26 (13.5%) | 42 (26.8%) |
| Maternal eczema | 24 (12.8%) | 28 (14.6%) | 34 (21.7%) |
| Maternal education | |||
| None | 64 (34.0%) | 73 (38.0%) | 46 (29.3%) |
| Primary school | 117 (62.2%) | 116 (60.4%) | 109 (69.4%) |
| Middle school or higher | 7 (3.7%) | 3 (1.6%) | 2 (1.3%) |
| Paternal education | |||
| None | 22 (11.7%) | 26 (13.5%) | 19 (12.1%) |
| Primary school | 133 (70.7%) | 130 (67.7%) | 110 (70.1%) |
| Middle school or higher | 24 (12.8%) | 28 (14.6%) | 27 (17.2%) |
| Unknown | 9 (4.8%) | 8 (4.2%) | 1 (0.6%) |
| Socioeconomics (SES) | |||
| Land-owning | 169 (89.9%) | 172 (89.6%) | 125 (79.6%) |
| Home-owning | 158 (84.0%) | 167 (87.0%) | 120 (76.4%) |
| Number of major assets *: mean (SD) | 1.68 (1.01) | 1.71 (1.13) | 1.59 (1.08) |
| Group 1 | Group 2 | Group 3 | ||
|---|---|---|---|---|
| Plancha installation age | (<6 months) | (~18 months) | (~57 months) | One-way ANOVA p-value |
| mean (SD) | mean (SD) | mean (SD) | ||
| median [Min, Max] | median [Min, Max] | median [Min, Max] | ||
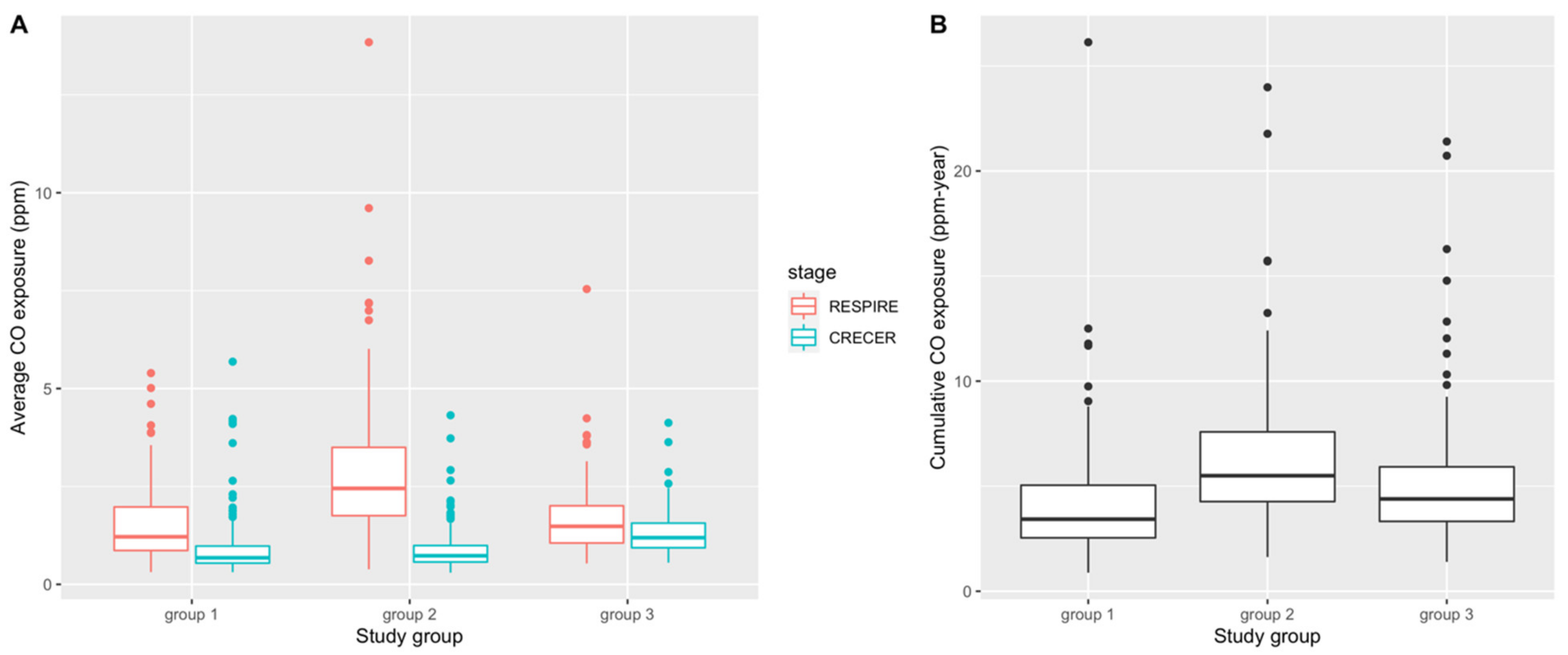
| CO exposure during RESPIRE (ppm) | 1.47 * (0.92) | 2.87 (1.71) | 1.67 # (0.87) | <0.001 |
| 1.21 * [0.31, 5.69] | 2.47 [0.39, 13.8] | 1.48 # [0.53, 7.54] | ||
| CO exposure during CRECER (ppm) | 0.89 * (0.72) | 0.89 * (0.53) | 1.30 (0.55) | <0.001 |
| 0.67 * [0.31, 5.69] | 0.75 * [0.30, 4.32] | 1.18 [0.55, 4.13] | ||
| Cumulative CO before allergy questionnaire ^ (ppm-year) | 4.16 (2.69) | 6.21 (3.19) | 5.12 (3.07) | <0.001 |
| 3.43 [0.88, 26.1] | 5.50 [1.63, 24.0] | 4.39 [1.40, 21.4] |
| Group 1 (Baseline) | Group 2 | Group 3 | p Value for Equal Proportions | |
|---|---|---|---|---|
| Plancha Installation Age | (<6 Months) | (~18 Months) | (~57 Months) | |
| Number of Cases (%) | Number of Cases (%) | Number of Cases (%) | ||
| Positive SPT result | n = 184 | n = 187 | n = 155 | |
| D. farinae | 29 (15.8%) | 25 (13.4%) | 17 (11.0%) | 0.44 |
| D. pteronyssinus | 9 (4.9%) | 11 (5.9%) | 9 (5.8%) | 0.90 |
| Cockroach | 70 (38.0%) | 69 (36.9%) | 56 (36.1%) | 0.93 |
| Dog | 1 (0.5%) | 6 (3.2%) | 2 (1.3%) | 0.13 |
| Cat | 5 (2.7%) | 4 (2.1%) | 3 (1.9%) | 0.88 |
| Ragweed | 1 (0.5%) | 1 (0.5%) | 0 (0%) | 0.66 |
| Maternal-reported allergic symptoms | n = 188 | n = 192 | n = 157 | |
| Asthma symptoms | ||||
| Any wheezing episode | 13 (6.9%) | 12 (6.2%) | 29 (18.5%) | <0.001 |
| Exercise-induced wheezing | 8 (4.3%) | 6 (3.1%) | 9 (5.7%) | 0.49 |
| Cough | 54 (28.7%) | 40 (20.8%) | 60 (38.2%) | <0.01 |
| Rhinitis symptoms | ||||
| Sneezing, congestion, or rhinorrhea | 33 (17.6%) | 47 (24.5%) | 54 (34.4%) | <0.01 |
| Allergic conjunctivitis symptoms | ||||
| Itchy or watery eyes | 33 (17.6%) | 26 (13.5%) | 27 (17.2%) | 0.21 |
| Eczema symptoms | 24 (12.8%) | 25 (13.0%) | 22 (14.0%) | 0.94 |
| Group 2 | Group 3 | |||||
|---|---|---|---|---|---|---|
| Plancha Installation Age | (~18 Months) | (~57 Months) | ||||
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| Positive SPT result | ||||||
| D. farina | 0.82 (0.46, 1.47) | 0.77 (0.41, 1.42) | 0.81 (0.43, 1.53) | 0.66 (0.34, 1.24) | 0.72 (0.36, 1.44) | 0.72 (0.35, 1.46) |
| D. pteronyssinus | 1.22 (0.49, 3.08) | 1.31 (0.50, 3.57) | 1.24 (0.45, 3.51) | 1.20 (0.46, 3.15) | 1.78 (0.61, 5.26) | 1.67 (0.54, 5.21) |
| Cockroach | 0.95 (0.63, 1.45) | 0.93 (0.60, 1.45) | 0.93 (0.60, 1.46) | 0.92 (0.59. 1.43) | 0.91 (0.56, 1.46) | 0.87 (0.53, 1.41) |
| Dog | 6.07 (1.02, 115.17) | 8.11 (1.07, 178.7) | 11.25 (1.19, 437.76) | 2.39 (0.23, 51.77) | 2.96 (0.18, 82.70) | 2.54 (0.10, 133.51) |
| Cat | 0.78 (0.19, 3.00) | 0.49 (0.09, 2.30) | 0.47 (0.08, 2.25) | 0.71 (0.14, 2.93) | 0.45 (0.07, 2.29) | 0.40 (0.06, 2.11) |
| Asthma symptoms | ||||||
| Any wheezing episode | 0.90 (0.39, 2.03) | 0.74 (0.30, 1.81) | 0.74 (0.30, 1.82) | 3.05 (1.56, 6.28) | 2.44 (1.14, 5.47) | 2.42 (1.11, 5.48) |
| Exercise-induced wheezing | 0.73 (0.23, 2.13) | 0.59 (0.16, 2.03) | 0.54 (0.15, 1.91) | 1.37 (0.51, 3.73) | 0.83 (0.25, 2.73) | 0.72 (0.21, 2.42) |
| Cough | 0.65 (0.41, 1.04) | 0.65 (0.39, 1.08) | 0.67 (0.40, 1.11) | 1.53 (0.98, 2.41) | 1.42 (0.86, 2.34) | 1.60 (0.96, 2.67) |
| Rhinitis symptoms | ||||||
| Sneezing, congestion, or rhinorrhea | 1.52 (0.93, 2.52) | 1.47 (0.86, 2.57) | 1.47 (0.85, 2.67) | 2.46 (1.50, 4.09) | 2.06 (0.18, 3.63) | 2.01 (1.13, 3.58) |
| Allergic conjunctivitis symptoms | ||||||
| Itchy or watery eyes | 1.32 (0.71, 2.47) | 1.04 (0.52, 2.08) | 1.01 (0.50, 2.03) | 1.74 (0.94, 3.28) | 1.41 (0.71, 2.85) | 1.30 (0.64, 2.66) |
| Eczema symptoms | 1.02 (0.56, 1.87) | 1.04 (0.54, 2.02) | 1.05 (0.54, 2.03) | 1.11 (0.59, 2.08) | 0.86 (0.42, 1.72) | 0.82 (0.40, 1.67) |
| Model 1 | Model 2 | Model 3 | |
|---|---|---|---|
| Positive SPT result | |||
| D. farina | 0.98 (0.90, 1.06) | 0.96 (0.87, 1.05) | 0.96 (0.86, 1.05) |
| D. pteronyssinus | 0.95 (0.81, 1.08) | 0.98 (0.83, 1.12) | 0.99 (0.83, 1.12) |
| Cockroach | 0.96 (0.90, 1.02) | 0.97 (0.91, 1.04) | 0.97 (0.91, 1.04) |
| Dog | 1.01 (0.78, 1.19) | 1.02 (0.76, 1.25) | 1.04 (0.77, 1.30) |
| Cat | 1.00 (0.80, 1.16) | 1.00 (0.77, 1.22) | 1.00 (0.76, 1.22) |
| Asthma symptoms | |||
| Any wheezing episode | 0.94 (0.84, 1.04) | 0.98 (087, 1.10) | 0.99 (0.87, 1.10) |
| Exercise-induced wheezing | 0.99 (0.85, 1.12) | 1.07 (0.90, 1.23) | 1.06 (0.89, 1.22) |
| Cough | 0.96 (0.90, 1.02) | 0.99 (0.92, 1.06) | 0.99 (0.92, 1.07) |
| Rhinitis symptoms | |||
| Sneezing, congestion, or rhinorrhea | 1.05 (0.99, 1.11) | 1.10 (1.02, 1.18) | 1.09 (1.02, 1.18) |
| Allergic conjunctivitis symptoms | |||
| Itchy or watery eyes | 1.07 (0.99, 1.14) | 1.12 (1.03, 1.22) | 1.11 (1.02, 1.21) |
| Eczema symptoms | 0.98 (0.89, 1.06) | 1.02 (0.92, 1.11) | 1.02 (0.92, 1.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, W.; Wang, L.A.; Mann, J.; Jenny, A.; Romero, C.; Kuster, A.; Canuz, E.; Pillarisetti, A.; Smith, K.R.; Balmes, J.; et al. Biomass Smoke Exposure and Atopy among Young Children in the Western Highlands of Guatemala: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 14064. https://doi.org/10.3390/ijerph192114064
Lu W, Wang LA, Mann J, Jenny A, Romero C, Kuster A, Canuz E, Pillarisetti A, Smith KR, Balmes J, et al. Biomass Smoke Exposure and Atopy among Young Children in the Western Highlands of Guatemala: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(21):14064. https://doi.org/10.3390/ijerph192114064
Chicago/Turabian StyleLu, Wenxin, Laura Ann Wang, Jennifer Mann, Alisa Jenny, Carolina Romero, Andrea Kuster, Eduardo Canuz, Ajay Pillarisetti, Kirk R. Smith, John Balmes, and et al. 2022. "Biomass Smoke Exposure and Atopy among Young Children in the Western Highlands of Guatemala: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 19, no. 21: 14064. https://doi.org/10.3390/ijerph192114064
APA StyleLu, W., Wang, L. A., Mann, J., Jenny, A., Romero, C., Kuster, A., Canuz, E., Pillarisetti, A., Smith, K. R., Balmes, J., & Thompson, L. (2022). Biomass Smoke Exposure and Atopy among Young Children in the Western Highlands of Guatemala: A Prospective Cohort Study. International Journal of Environmental Research and Public Health, 19(21), 14064. https://doi.org/10.3390/ijerph192114064