
Chronotype and Social Jetlag Influence Performance and Injury during Reserve Officers’ Training Corps Physical Training

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. ROTC Physical Training and Testing
2.3. Baseline Data Collection
2.4. Saliva Collection and IL-6 ELISA
2.5. Injury Incidence and APFT Score
2.6. Data and Statistical Analysis
3. Results
3.1. Chronotype
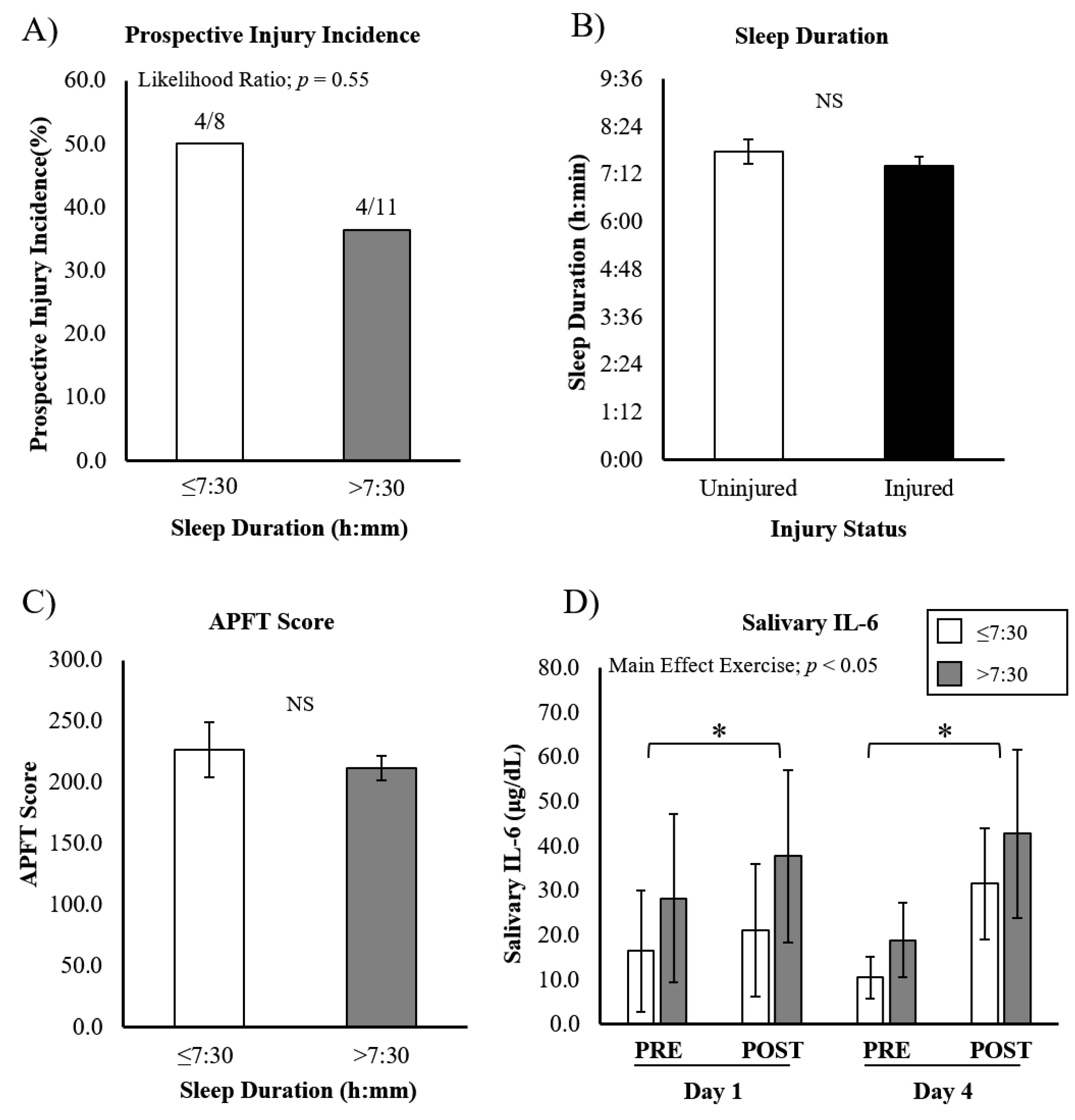
3.2. Sleep Duration
3.3. Social Jetlag
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knaier, R.; Qian, J.; Roth, R.; Infanger, D.; Notter, T.; Wang, W.; Cajochen, C.; Scheer, F. Diurnal Variation in Maximum Endurance and Maximum Strength Performance: A Systematic Review and Meta-analysis. Med. Sci. Sports Exerc. 2022, 54, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between clocks: Daily temporal patterns of human chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Facer-Childs, E.R.; Boiling, S.; Balanos, G.M. The effects of time of day and chronotype on cognitive and physical performance in healthy volunteers. Sports Med. Open. 2018, 4, 47. [Google Scholar] [CrossRef] [PubMed]
- Bonato, M.; La Torre, A.; Saresella, M.; Marventano, I.; Merati, G.; Vitale, J.A. Salivary cortisol concentration after high-intensity interval exercise: Time of day and chronotype effect. Chronobiol. Int. 2017, 34, 698–707. [Google Scholar] [CrossRef]
- Good, C.H.; Brager, A.J.; Capaldi, V.F.; Mysliwiec, V. Sleep in the United States Military. Neuropsychopharmacology 2020, 45, 176–191. [Google Scholar] [CrossRef]
- Mah, C.D.; Kezirian, E.J.; Marcello, B.M.; Dement, W.C. Poor sleep quality and insufficient sleep of a collegiate student-athlete population. Sleep Health 2018, 4, 251–257. [Google Scholar] [CrossRef]
- Simmons, N.; Mandal, S.; Paton, B.; Ahmed, I. Are Circadian Rhythms a New Frontier in Athletic Performance? Curr. Sports Med. Rep. 2022, 21, 5–7. [Google Scholar] [CrossRef]
- Glavin, E.E.; Matthew, J.; Spaeth, A.M. Gender Differences in the Relationship Between Exercise, Sleep, and Mood in Young Adults. Health Educ. Behav. 2021, 49, 128–140. [Google Scholar] [CrossRef]
- Yadav, A.; Rani, S.; Singh, S. Working "out-of-phase" with reference to chronotype compromises sleep quality in police officers. Chronobiol. Int. 2016, 33, 151–160. [Google Scholar] [CrossRef]
- Ruscio, B.A.; Jones, B.H.; Bullock, S.H.; Burnham, B.R.; Canham-Chervak, M.; Rennix, C.P.; Wells, T.S.; Smith, J.W. A process to identify military injury prevention priorities based on injury type and limited duty days. Am. J. Prev. Med. 2010, 38, S19–S33. [Google Scholar] [CrossRef]
- Fullagar, H.H.; Skorski, S.; Duffield, R.; Hammes, D.; Coutts, A.J.; Meyer, T. Sleep and athletic performance: The effects of sleep loss on exercise performance, and physiological and cognitive responses to exercise. Sports Med. 2015, 45, 161–186. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Miller, M.A. Sleep and Cardio-Metabolic Disease. Curr. Cardiol. Rep. 2017, 19, 110. [Google Scholar] [CrossRef]
- Adrian, A.L.; Skeiky, L.; Burke, T.M.; Gutierrez, I.A.; Adler, A.B. Sleep problems and functioning during initial training for a high-risk occupation. Sleep Health 2019, 5, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Ritland, B.M.; Simonelli, G.; Gentili, R.J.; Smith, J.C.; He, X.; Oh, H.; Balkin, T.J.; Hatfield, B.D. Sleep health and its association with performance and motivation in tactical athletes enrolled in the Reserve Officers’ Training Corps. Sleep Health 2019, 5, 309–314. [Google Scholar] [CrossRef]
- Cullen, T.; Thomas, G.; Wadley, A.J. Sleep Deprivation: Cytokine and Neuroendocrine Effects on Perception of Effort. Med. Sci. Sports Exerc. 2020, 52, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Del Gallo, F.; Opp, M.R.; Imeri, L. The reciprocal link between sleep and immune responses. Arch. Ital. Biol. 2014, 152, 93–102. [Google Scholar] [CrossRef]
- Chennaoui, M.; Vanneau, T.; Trignol, A.; Arnal, P.; Gomez-Merino, D.; Baudot, C.; Perez, J.; Pochettino, S.; Eirale, C.; Chalabi, H. How does sleep help recovery from exercise-induced muscle injuries? J. Sci. Med. Sport 2021, 24, 982–987. [Google Scholar] [CrossRef]
- Freitas, L.D.S.N.; da Silva, F.R.; Andrade, H.A.; Guerreiro, R.C.; Paulo, F.V.; de Mello, M.T.; Silva, A. Sleep debt induces skeletal muscle injuries in athletes: A promising hypothesis. Med. Hypotheses 2020, 142, 109836. [Google Scholar] [CrossRef]
- Eliasson, A.H.; Lettieri, C.; Netzer, N. Sleep medicine is coming of age in military medicine: Report from the Military Health System Research Symposium (2017) in Kissimmee, Florida. Sleep Breath 2018, 22, 481–483. [Google Scholar] [CrossRef]
- Milewski, M.D.; Skaggs, D.L.; Bishop, G.A.; Pace, J.L.; Ibrahim, D.A.; Wren, T.A.; Barzdukas, A. Chronic lack of sleep is associated with increased sports injuries in adolescent athletes. J. Pediatr. Orthop. 2014, 34, 129–133. [Google Scholar] [CrossRef]
- Grier, T.; Dinkeloo, E.; Reynolds, M.; Jones, B.H. Sleep duration and musculoskeletal injury incidence in physically active men and women: A study of U.S. Army Special Operation Forces soldiers. Sleep Health 2020, 6, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.H.; Hijmans, J.M.; Minoonejad, H.; Rajabi, R.; Zwerver, J. Factors Associated With Lower Limb Injuries in Recreational Runners: A Cross-Sectional Survey Including Mental Aspects and Sleep Quality. J. Sports Sci. Med. 2021, 20, 204–215. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Y.; Yu, X.; Wang, H.; Zou, B.; Song, W.J.; Gu, W.; Ling, C.Q. Sleep quality and military training injury during basic combat training: A prospective cohort study of Chinese male recruits. Occup. Environ. Med. 2020, 78, 433–437. [Google Scholar] [CrossRef]
- Roenneberg, T.; Pilz, L.K.; Zerbini, G.; Winnebeck, E.C. Chronotype and Social Jetlag: A (Self-) Critical Review. Biology 2019, 8, 54. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Higgins, S.; Stoner, L.; Lubransky, A.; Howe, A.S.; Wong, J.E.; Black, K.; Skidmore, P. Social jetlag is associated with cardiorespiratory fitness in male but not female adolescents. Sleep Med. 2020, 75, 163–170. [Google Scholar] [CrossRef]
- Roenneberg, T.; Allebrandt, K.V.; Merrow, M.; Vetter, C. Social jetlag and obesity. Curr. Biol. 2012, 22, 939–943. [Google Scholar] [CrossRef]
- Tom, J.C.; Schilling, B.K.; Poston, B.; Turner, C.L.; Radzak, K.N. United States university-based officer training and its influence on physical assessment test performance. BMJ Mil Health 2022, 168, 206–211. [Google Scholar] [CrossRef]
- McHugh, M.L. The chi-square test of independence. Biochem. Med. 2013, 23, 143–149. [Google Scholar] [CrossRef]
- Vitale, J.A.; Weydahl, A. Chronotype, Physical Activity, and Sport Performance: A Systematic Review. Sports Med. 2017, 47, 1859–1868. [Google Scholar] [CrossRef]
- Lim, S.T.; Kim, D.Y.; Kwon, H.T.; Lee, E. Sleep quality and athletic performance according to chronotype. BMC Sports Sci. Med. Rehabil. 2021, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Duffy, J.F.; de Castillero, E.R.; Wang, K. Chronotype, Sleep Characteristics, and Musculoskeletal Disorders Among Hospital Nurses. Workplace Health Saf. 2018, 66, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Biggins, M.; Purtill, H.; Fowler, P.; Bender, A.; Sullivan, K.O.; Samuels, C.; Cahalan, R. Sleep in elite multi-sport athletes: Implications for athlete health and wellbeing. Phys. Ther. Sport 2019, 39, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Dennis, J.; Dawson, B.; Heasman, J.; Rogalski, B.; Robey, E. Sleep patterns and injury occurrence in elite Australian footballers. J. Sci. Med. Sport 2016, 19, 113–116. [Google Scholar] [CrossRef]
- Reilly, T.; Piercy, M. The effect of partial sleep deprivation on weight-lifting performance. Ergonomics 1994, 37, 107–115. [Google Scholar] [CrossRef]
- Abedelmalek, S.; Souissi, N.; Chtourou, H.; Denguezli, M.; Aouichaoui, C.; Ajina, M.; Aloui, A.; Dogui, M.; Haddouk, S.; Tabka, Z. Effects of partial sleep deprivation on proinflammatory cytokines, growth hormone, and steroid hormone concentrations during repeated brief sprint interval exercise. Chronobiol. Int. 2013, 30, 502–509. [Google Scholar] [CrossRef]
- Kang, H.; Lee, M.; Jang, S.J. The Impact of Social Jetlag on Sleep Quality among Nurses: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 18, 47. [Google Scholar] [CrossRef]
- McMahon, D.M.; Burch, J.B.; Youngstedt, S.D.; Wirth, M.D.; Hardin, J.W.; Hurley, T.G.; Blair, S.N.; Hand, G.A.; Shook, R.P.; Drenowatz, C.; et al. Relationships between chronotype, social jetlag, sleep, obesity and blood pressure in healthy young adults. Chronobiol. Int. 2019, 36, 493–509. [Google Scholar] [CrossRef]
- Umemura, G.S.; Pinho, J.P.; Goncalves, B.D.S.B.; Furtado, F.; Forner-Cordero, A. Social jetlag impairs balance control. Sci. Rep. 2018, 8, 9406. [Google Scholar] [CrossRef]
- Peake, J.M.; Markworth, J.F.; Nosaka, K.; Raastad, T.; Wadley, G.D.; Coffey, V.G. Modulating exercise-induced hormesis: Does less equal more? J. Appl. Physiol. 2015, 119, 172–189. [Google Scholar] [CrossRef]
- Slavish, D.C.; Graham-Engeland, J.E.; Smyth, J.M.; Engeland, C.G. Salivary markers of inflammation in response to acute stress. Brain Behav. Immun. 2015, 44, 253–269. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| M/F | 21/6 |
| Height (cm) | 171.7 ± 10.5 |
| Weight (kg) | 75.7 ± 15.6 |
| Age (years) | 21.3 ± 3.7 |
| BMI | 25.5 ± 3.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGinnis, G.R.; Thompson, S.T.; Aguilar, C.D.; Dial, M.B.; Tandy, R.D.; Radzak, K.N. Chronotype and Social Jetlag Influence Performance and Injury during Reserve Officers’ Training Corps Physical Training. Int. J. Environ. Res. Public Health 2022, 19, 13644. https://doi.org/10.3390/ijerph192013644
McGinnis GR, Thompson ST, Aguilar CD, Dial MB, Tandy RD, Radzak KN. Chronotype and Social Jetlag Influence Performance and Injury during Reserve Officers’ Training Corps Physical Training. International Journal of Environmental Research and Public Health. 2022; 19(20):13644. https://doi.org/10.3390/ijerph192013644
Chicago/Turabian StyleMcGinnis, Graham R., Shani T. Thompson, Charli D. Aguilar, Michael B. Dial, Richard D. Tandy, and Kara N. Radzak. 2022. "Chronotype and Social Jetlag Influence Performance and Injury during Reserve Officers’ Training Corps Physical Training" International Journal of Environmental Research and Public Health 19, no. 20: 13644. https://doi.org/10.3390/ijerph192013644
APA StyleMcGinnis, G. R., Thompson, S. T., Aguilar, C. D., Dial, M. B., Tandy, R. D., & Radzak, K. N. (2022). Chronotype and Social Jetlag Influence Performance and Injury during Reserve Officers’ Training Corps Physical Training. International Journal of Environmental Research and Public Health, 19(20), 13644. https://doi.org/10.3390/ijerph192013644