
Prevalence of Anxiety and Depression Symptoms and Their Relationship with Nutritional Status and Mortality in Patients with Colorectal Cancer

 , , , ,
, , , ,
Abstract
1. Introduction
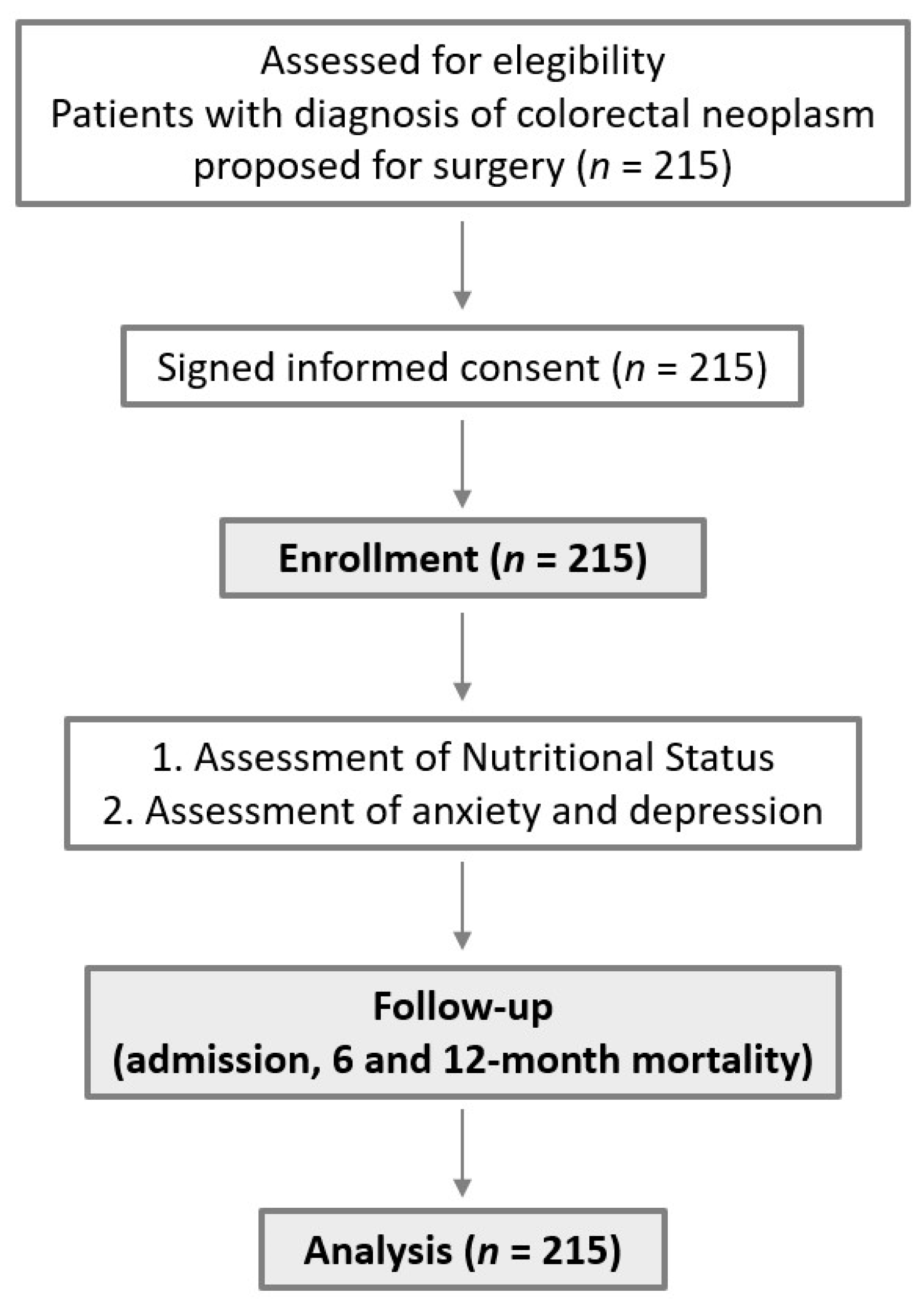
2. Materials and Methods
2.1. Assessment of Nutritional Status
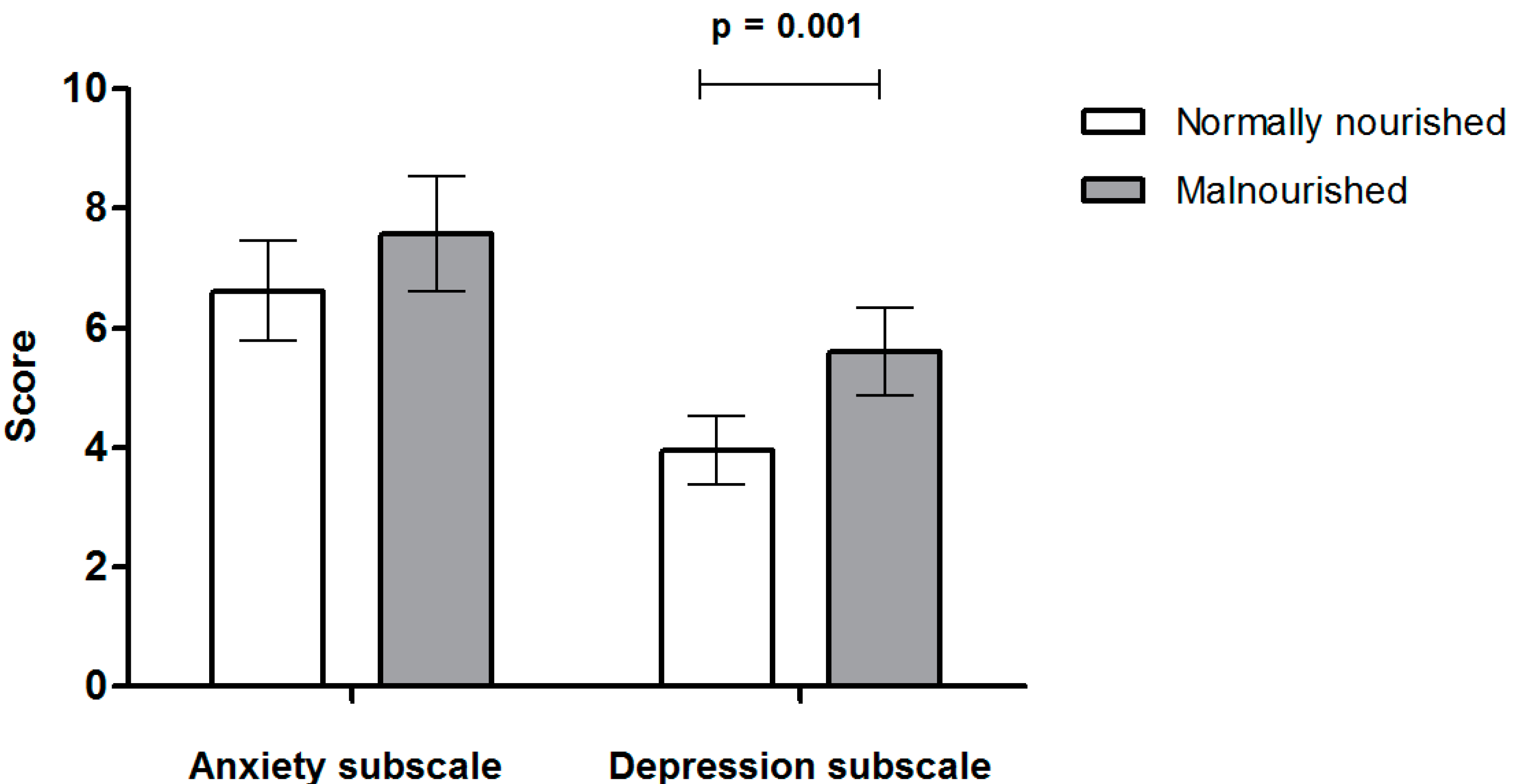
2.2. Assessment of Symptoms of Anxiety and Depression
2.3. Clinical Outcomes
2.4. Data Analysis
2.5. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gillis, C.; Richer, L.; Fenton, T.R.; Gramlich, L.; Keller, H.; Culos-Reed, S.N.; Sajobi, T.T.; Awasthi, R.; Carli, F. Colorectal cancer patients with malnutrition suffer poor physical and mental health before surgery. Surgery 2021, 170, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Gastroenterol. Rev. Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef]
- Peng, Y.-N.; Huang, M.-L.; Kao, C.-H. Prevalence of Depression and Anxiety in Colorectal Cancer Patients: A Literature Review. Int. J. Env. Res. Public Health 2019, 16, 411. [Google Scholar] [CrossRef]
- Mosher, C.E.; Winger, J.; Given, B.A.; Helft, P.R.; O’Neil, B.H. Mental health outcomes during colorectal cancer survivorship: A review of the literature. Psychooncology 2016, 25, 1261–1270. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN practical guideline: Clinical nutrition in surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Ruan, X.; Wang, X.; Zhang, Q.; Nakyeyune, R.; Shao, Y.; Shen, Y.; Niu, C.; Zhu, L.; Zang, Z.; Wei, T.; et al. The performance of three nutritional tools varied in colorectal cancer patients: A retrospective analysis. J. Clin. Epidemiol. 2022, 149, 12–22. [Google Scholar] [CrossRef]
- Pitman, A.; Suleman, S.; Hyde, N.; Hodgkiss, A. Depression and anxiety in patients with cancer. BMJ 2018, 361, k1415. [Google Scholar] [CrossRef]
- Caruso, R.; Nanni, M.G.; Riba, M.; Sabato, S.; Mitchell, A.J.; Croce, E.; Grassi, L. Depressive spectrum disorders in cancer: Prevalence, risk factors and screening for depression: A critical review. Acta Oncol. 2017, 56, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.; Hansen, C.H.; Martin, P.; Symeonides, S.; Ramessur, R.; Murray, G.; Sharpe, M. Prevalence, associations, and adequacy of treatment of major depression in patients with cancer: A cross-sectional analysis of routinely collected clinical data. Lancet Psychiatry 2014, 1, 343–350. [Google Scholar] [CrossRef]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Ehrsson, Y.; Fransson, P.; Einarsson, S. Mapping Health-Related Quality of Life, Anxiety, and Depression in Patients with Head and Neck Cancer Diagnosed with Malnutrition Defined by GLIM. Nutrients 2021, 13, 1167. [Google Scholar] [CrossRef]
- Chabowski, M.; Polański, J.; Jankowska-Polańska, B.; Janczak, D.; Rosińczuk, J. Is nutritional status associated with the level of anxiety, depression and pain in patients with lung cancer? J. Thorac. Dis. 2018, 10, 2303–2310. [Google Scholar] [CrossRef]
- Sánchez-Torralvo, F.J.; Contreras-Bolívar, V.; Ruiz-Vico, M.; Abuín-Fernández, J.; González-Almendros, I.; Barrios, M.; Olveira, G. Relationship between malnutrition and the presence of symptoms of anxiety and depression in hospitalized cancer patients. Support Care Cancer 2022, 30, 1607–1613. [Google Scholar] [CrossRef]
- Aminisani, N.; Nikbakht, H.; Jafarabadi, M.A.; Shamshirgaran, S.M. Depression, anxiety, and health related quality of life among colorectal cancer survivors. J. Gastrointest. Oncol. 2017, 8, 81–88. [Google Scholar] [CrossRef]
- Martínez-Escribano, C.; Moreno, F.A.; Pérez-López, M.; Cunha-Pérez, C.; Belenguer-Varea, A.; Peredo, D.C.; González, F.J.B.; Tarazona-Santabalbina, F.J. Malnutrition and Increased Risk of Adverse Outcomes in Elderly Patients Undergoing Elective Colorectal Cancer Surgery: A Case-Control Study Nested in a Cohort. Nutrients 2022, 14, 207. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, E.; Hilsden, R.; Hawel, J.D.; Elnahas, A.I.; Schlachta, C.M.; Alkhamesi, N.A. Preoperative malnutrition in patients with colorectal cancer. Can. J. Surg. 2021, 64, E621–E629. [Google Scholar] [CrossRef]
- Lopes, J.P.; de Castro Cardoso Pereira, P.M.; dos Reis Baltazar Vicente, A.F.; Bernardo, A.; De Mesquita, M.F. Nutritional status assessment in colorectal cancer patients. Nutr. Hosp. 2013, 28, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Torralvo, F.J.; González-Poveda, I.; García-Olivares, M.; Porras, N.; Gonzalo-Marín, M.; Tapia, M.J.; Mera-Velasco, S.; Toval-Mata, J.A.; Ruiz-López, M.; Carrasco-Campos, J.; et al. Poor Physical Performance Is Associated with Postoperative Complications and Mortality in Preoperative Patients with Colorectal Cancer. Nutrients 2022, 14, 1484. [Google Scholar] [CrossRef]
- Gascón-Ruiz, M.; Casas-Deza, D.; Torres-Ramón, I.; Zapata-García, M.; Alonso, N.; Sesma, A.; Lambea, J.; Álvarez-Alejandro, M.; Quílez, E.; Isla, D.; et al. GLIM vs ESPEN criteria for the diagnosis of early malnutrition in oncological outpatients. Clin. Nutr. 2021, 40, 3741–3747. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Wang, B.; Gao, Y.; Ma, X. Prevalence and relationship of malnutrition and distress in patients with Cancer using questionnaires 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Cancer 2018, 18, 1272. [Google Scholar] [CrossRef]
- Lambert, J.E.; Hayes, L.D.; Keegan, T.J.; Subar, D.A.; Gaffney, C.J. The Impact of Prehabilitation on Patient Outcomes in Hepatobiliary, Colorectal, and Upper Gastrointestinal Cancer Surgery: A PRISMA-Accordant Meta-analysis. Ann. Surg. 2021, 274, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Bousquet-Dion, G.; Awasthi, R.; Elsherbini, N.; Liberman, S.; Boutros, M.; Stein, B.; Charlebois, P.; Ghitulescu, G.; Morin, N.; et al. Effect of Multimodal Prehabilitation vs Postoperative Rehabilitation on 30-Day Postoperative Complications for Frail Patients Undergoing Resection of Colorectal Cancer: A Randomized Clinical Trial. JAMA Surg. 2020, 155, 233. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Lu, Z.; Zhu, M.; Lu, X. Trimodal prehabilitation for older surgical patients: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2022, 34, 485–494. [Google Scholar] [CrossRef]
- López, L.M.; Llovera, A.P.; Serra-Aracil, X.; Pla, S.S.; Guerrero, V.L.; Rebasa, P.; Domínguez, C.T.; Caballé, G.P.; Castela, R.M.; Giménez, L.S.; et al. Estudio observacional prospectivo unicéntrico sobre el efecto de la prehabilitación trimodal en cirugía colorrectal. Cirugía Española 2020, 98, 605–611. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Li, J.-Q.; Shi, J.-F.; Que, J.-Y.; Liu, J.-J.; Lappin, J.; Leung, J.; Ravindran, A.V.; Chen, W.-Q.; Qiao, Y.-L.; et al. Depression and anxiety in relation to cancer incidence and mortality: A systematic review and meta-analysis of cohort studies. Mol. Psychiatry 2020, 25, 1487–1499. [Google Scholar] [CrossRef]
- Walker, J.; Mulick, A.; Magill, N.; Symeonides, S.; Gourley, C.; Burke, K.; Belot, A.; Quartagno, M.; van Niekerk, M.; Toynbee, M.; et al. Major Depression and Survival in People With Cancer. Psychosom. Med. 2021, 83, 410–416. [Google Scholar] [CrossRef]
- Smith, H.R. Depression in cancer patients: Pathogenesis, implications and treatment. Oncol. Lett. 2015, 9, 1509. [Google Scholar] [CrossRef] [PubMed]
- Saini, S.M.; Koon, S.T.M.; Bujang, M.A.; Chye, G.L.C.; Sharip, S.; Wahab, S.; Jaafar, N.R.N.; Fong, C.L.; Baharudin, A. Effect of Anxiety and Depression on Survival of Cancer Patients, a 13 Year Follow-up. Asian Pac. J. Cancer Care 2021, 6, 9–13. [Google Scholar] [CrossRef]
- Matsushita, T.; Matsushima, E.; Maruyama, M. Anxiety and depression of patients with digestive cancer. Psychiatry Clin. Neurosci. 2005, 59, 576–583. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n = 215 | ||
|---|---|---|
| Age (years) | mean ± SD (min–max) | 68.4 ± 10.3 (40–89) |
| Sex | n (%) | |
| Men | 123 (57.2) | |
| Women | 92 (42.8) | |
| Type of cancer | n (%) | |
| Colon | 124 (57.7) | |
| Rectum | 91 (42.3) | |
| Stage | n (%) | |
| I | 28 (13) | |
| II | 67 (31.2) | |
| III | 95 (44.2) | |
| IV | 25 (11.6) | |
| BMI (kg/m2) | mean ± SD (min–max) | 26.9 ± 5.2 (15.8–47.6) |
| Surgical complications | n (%) | 90 (41.9) |
| Malnutrition according to GLIM criteria | n (%) | 116 (53.9) |
| HADSA score | mean ± SD | 7.38 ± 4.59 |
| HADSD score | mean ± SD | 5 ± 3.59 |
| Possible presence of anxiety (HADSA ≥ 8) | n (%) | 90 (41.9) |
| Possible presence of depression (HADSD ≥ 8) | n (%) | 47 (21.9) |
| Probable presence of anxiety (HADSA ≥ 11) | n (%) | 55 (25.6) |
| Probable presence of depression (HADSD ≥ 11) | n (%) | 17 (7.9) |
| In-hospital mortality | n (%) | 4 (1.9) |
| 1-month mortality | n (%) | 5 (2.3) |
| 6-month mortality | n (%) | 9 (4.2) |
| 12-month mortality | n (%) | 12 (5.6) |
| Crude | Adjusted | |||||||
|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value | |||
| Lower | Upper | Lower | Upper | |||||
| Possible presence of anxiety (HADSA ≥ 8) | 1.15 | 0.64 | 2.06 | 0.644 | 1.25 | 0.66 | 2.36 | 0.495 |
| Possible presence of depression (HADSD ≥ 8) | 4.45 | 1.92 | 10.29 | <0.001 | 3.68 | 1.53 | 8.86 | 0.004 |
| Probable presence of anxiety (HADSA ≥ 11) | 1.85 | 0.93 | 3.68 | 0.078 | 2.19 | 1.04 | 4.63 | 0.04 |
| Probable presence of depression (HADSD ≥ 11) | 11.34 | 1.44 | 89.08 | 0.004 | 10.19 | 1.13 | 92.24 | 0.039 |
| Crude | Adjusted | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% CI | p Value | Odds Ratio | 95% CI | p Value | ||||
| Lower | Upper | Lower | Upper | ||||||
| Possible presence of anxiety (HADSA ≥ 8) | Surgical complications | 1.05 | 0.61 | 1.82 | 0.86 | 0.94 | 0.52 | 1.69 | 0.83 |
| Mortality during admission | 1.40 | 0.19 | 10.11 | 1 | 1.52 | 0.21 | 11.07 | 0.68 | |
| Mortality within 6 m | 1.12 | 0.29 | 4.28 | 1 | 1.21 | 0.31 | 4.70 | 0.78 | |
| Mortality within 12 m | 0.68 | 0.20 | 2.33 | 0.77 | 0.74 | 0.21 | 2.55 | 0.63 | |
| Possible presence of depression (HADSD ≥ 8) | Surgical complications | 1.50 | 0.78 | 2.90 | 0.23 | 1.43 | 0.69 | 2.99 | 0.34 |
| Mortality during admission | 11.32 | 1.15 | 111.48 | 0.01 | 11.38 | 1.02 | 126.56 | 0.048 | |
| Mortality within 6 m | 4.85 | 1.25 | 18.86 | 0.013 | 4.25 | 1.02 | 17.69 | 0.046 | |
| Mortality within 12 m | 3.93 | 1.20 | 12.81 | 0.016 | 3.52 | 1.02 | 12.22 | 0.047 | |
| Probable presence of anxiety (HADSA ≥ 11) | Surgical complications | 0.93 | 0.50 | 1.75 | 0.83 | 0.79 | 0.39 | 1.59 | 0.52 |
| Mortality during admission | 2.98 | 0.41 | 21.69 | 0.27 | 2.91 | 0.39 | 21.69 | 0.29 | |
| Mortality within 6 m | 1.48 | 0.37 | 6.36 | 0.69 | 1.41 | 0.33 | 5.95 | 0.64 | |
| Mortality within 12 m | 0.97 | 0.25 | 3.71 | 1 | 0.92 | 0.24 | 3.61 | 0.91 | |
| Probable presence of depression (HADSD ≥ 11) | Surgical complications | 1.60 | 0.59 | 4.33 | 0.35 | 1.68 | 0.53 | 5.34 | 0.38 |
| Mortality during admission | 13 | 1.71 | 98.89 | 0.007 | 14.67 | 1.54 | 140.21 | 0.02 | |
| Mortality within 6 m | 6.82 | 1.54 | 30.22 | 0.004 | 6.62 | 1.34 | 32.61 | 0.02 | |
| Mortality within 12 m | 4.48 | 1.08 | 18.43 | 0.025 | 4.35 | 0.96 | 19.66 | 0.056 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soria-Utrilla, V.; Sánchez-Torralvo, F.J.; González-Poveda, I.; Mera-Velasco, S.; Porras, N.; Toval-Mata, J.A.; García-Olivares, M.; Ruiz-López, M.; Gonzalo-Marín, M.; Carrasco-Campos, J.; et al. Prevalence of Anxiety and Depression Symptoms and Their Relationship with Nutritional Status and Mortality in Patients with Colorectal Cancer. Int. J. Environ. Res. Public Health 2022, 19, 13548. https://doi.org/10.3390/ijerph192013548
Soria-Utrilla V, Sánchez-Torralvo FJ, González-Poveda I, Mera-Velasco S, Porras N, Toval-Mata JA, García-Olivares M, Ruiz-López M, Gonzalo-Marín M, Carrasco-Campos J, et al. Prevalence of Anxiety and Depression Symptoms and Their Relationship with Nutritional Status and Mortality in Patients with Colorectal Cancer. International Journal of Environmental Research and Public Health. 2022; 19(20):13548. https://doi.org/10.3390/ijerph192013548
Chicago/Turabian StyleSoria-Utrilla, Virginia, Francisco José Sánchez-Torralvo, Iván González-Poveda, Santiago Mera-Velasco, Nuria Porras, José Antonio Toval-Mata, María García-Olivares, Manuel Ruiz-López, Montserrat Gonzalo-Marín, Joaquín Carrasco-Campos, and et al. 2022. "Prevalence of Anxiety and Depression Symptoms and Their Relationship with Nutritional Status and Mortality in Patients with Colorectal Cancer" International Journal of Environmental Research and Public Health 19, no. 20: 13548. https://doi.org/10.3390/ijerph192013548
APA StyleSoria-Utrilla, V., Sánchez-Torralvo, F. J., González-Poveda, I., Mera-Velasco, S., Porras, N., Toval-Mata, J. A., García-Olivares, M., Ruiz-López, M., Gonzalo-Marín, M., Carrasco-Campos, J., Tapia, M. J., Santoyo-Santoyo, J., & Olveira, G. (2022). Prevalence of Anxiety and Depression Symptoms and Their Relationship with Nutritional Status and Mortality in Patients with Colorectal Cancer. International Journal of Environmental Research and Public Health, 19(20), 13548. https://doi.org/10.3390/ijerph192013548