
Changes in Doctor–Patient Relationships in China during COVID-19: A Text Mining Analysis


Abstract
1. Introduction
2. Literature Review
3. Materials and Methods
3.1. Data Collection and Preprocessing
3.2. Data Analysis
4. Results
4.1. Sentiment Analysis
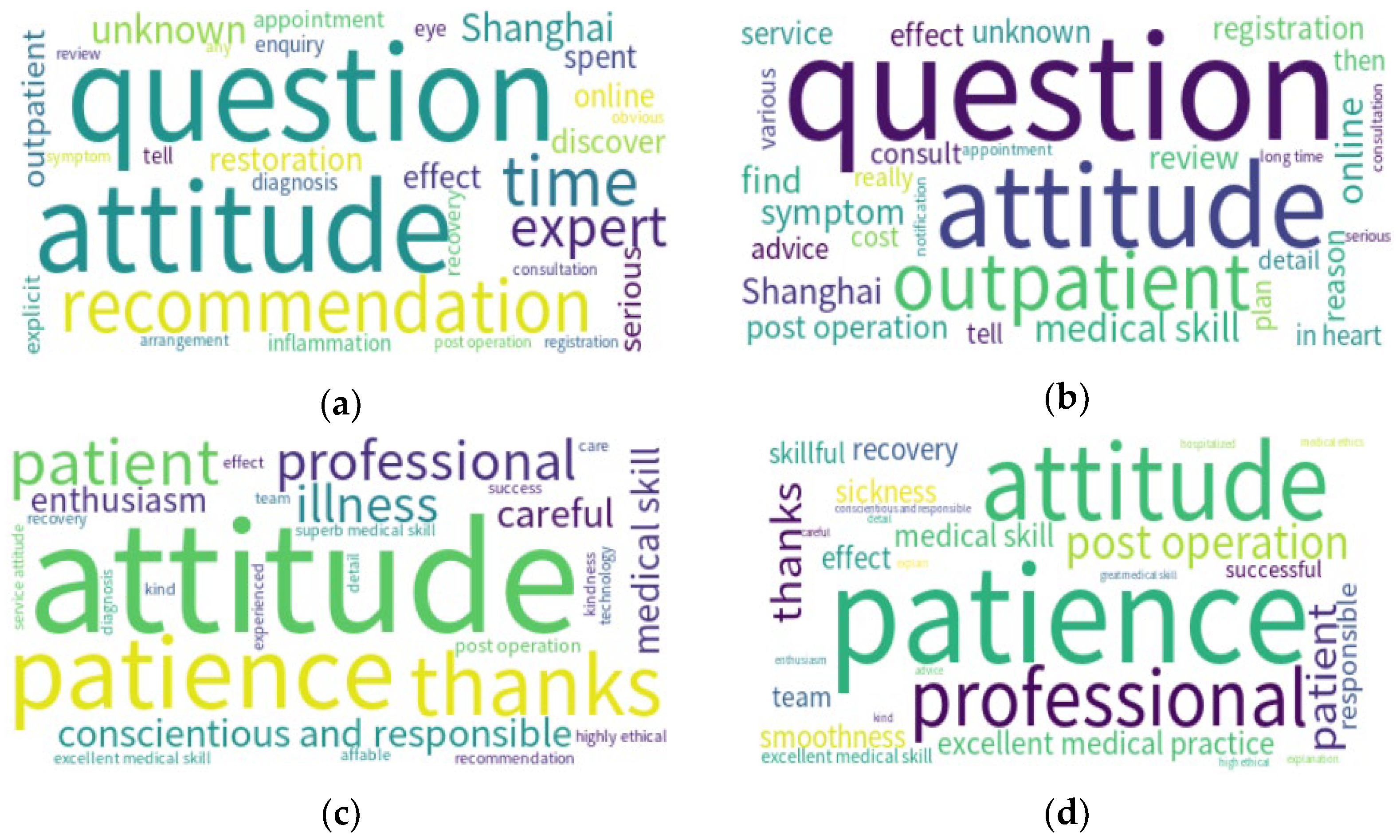
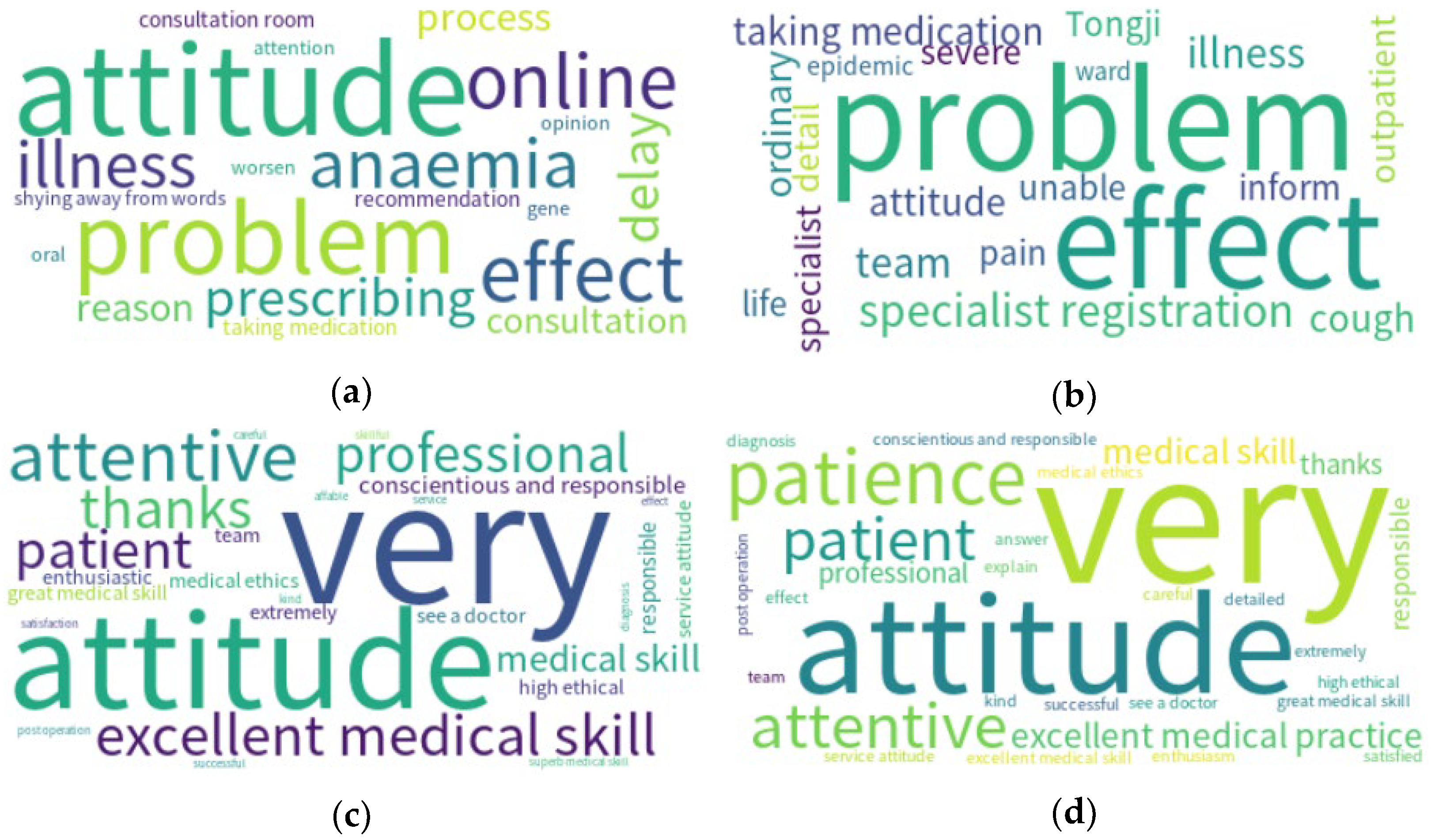
4.2. Word Frequency Analysis
5. Discussion
5.1. Changes in DPRs
5.2. Issues of Hospital Management
5.3. Methodological Contributions
5.4. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 14 August 2022).
- Kumari, A.; Ranjan, P.; Vikram, N.K.; Kaur, D.; Sahu, A.; Dwivedi, S.N.; Baitha, U.; Goel, A. A short questionnaire to assess changes in lifestyle-related behaviour during COVID 19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1697–1701. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Jakhar, D.; Kaur, I. Callous attitude toward doctors during COVID-19. Dermatol. Ther. 2020, 33, e13885. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Yang, Y.; Liu, Z.H.; Zhao, Y.J.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.T. Progression of mental health services during the COVID-19 outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732. [Google Scholar] [CrossRef]
- Yang, T.; Lu, W. The Research Summary on Conflict between Doctor and Patient. Chin. Med. Ethics 2006, 1, 46–48. [Google Scholar]
- Xiang, Y.-T.; Jin, Y.; Wang, Y.; Zhang, Q.; Zhang, L.; Cheung, T. Tribute to health workers in China: A group of respectable population during the outbreak of the COVID-19. Int. J. Biol. Sci. 2020, 16, 1739–1740. [Google Scholar] [CrossRef]
- Chandrasekaran, R.; Mehta, V.; Valkunde, T.; Moustakas, E. Topics, Trends, and Sentiments of Tweets About the COVID-19 Pandemic: Temporal Infoveillance Study. J. Med. Internet Res. 2020, 22, e22624. [Google Scholar] [CrossRef]
- Ji, L.; Pang, P.C.I. Have Patients’ Attitudes towards Doctors Changed with COVID-19? Insights from Online Doctor Reviews in Beijing, China. In Proceedings of the 13th International Conference on E-Business, Management and Economics (ICEME 2022), Beijing, China, 16–18 June 2022. [Google Scholar]
- Manguri, K.H.; Ramadhan, R.N.; Amin, P.R.M. Twitter Sentiment Analysis on Worldwide COVID-19 Outbreaks. Kurd. J. Appl. Res. 2020, 5, 54–65. [Google Scholar] [CrossRef]
- Naseem, U.; Razzak, I.; Khushi, M.; Eklund, P.W.; Kim, J. COVIDSenti: A Large-Scale Benchmark Twitter Data Set for COVID-19 Sentiment Analysis. IEEE Trans. Comput. Soc. Syst. 2021, 8, 1003–1015. [Google Scholar] [CrossRef]
- Hesketh, T.; Wu, D.; Mao, L.; Ma, N. Violence against doctors in China. BMJ 2012, 345, e5730. [Google Scholar] [CrossRef]
- Li, Z.; Xu, J.; Wei, J. Exploring the Determinants of the Evolution of Doctor–Patient Conflict in China: A Group Behaviour Perspective. China Int. J. 2021, 19, 210–234. [Google Scholar] [CrossRef]
- Gao, J.; Ma, X.; Yang, W. Discussing the emergence of contradiction between doctors and patient and development of harmonious relationship. Chin. Health Serv. Manag. 2011, 1, 181–183. [Google Scholar]
- Yang, H.; Du, H.S.; Shang, W. Understanding the influence of professional status and service feedback on patients’ doctor choice in online healthcare markets. Internet Res. 2020, 31, 1236–1261. [Google Scholar] [CrossRef]
- Krot, K.; Rudawska, I. The Role of Trust in Doctor-Patient Relationship: Qualitative Evaluation of Online Feedback from Polish Patients. Econ. Sociol. 2016, 9, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, C.; Richards, S.; Valderas, J.M.; Campbell, J.; Cruz-Díaz, N.P.; Giacomelli, P.; Singh, H. Supervised Machine Learning Algorithms Can Classify Open-Text Feedback of Doctor Performance with Human-Level Accuracy. J. Med. Internet Res. 2017, 19, e65. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, H.; Lei, X.; Shen, J.; Feng, Z. The Influence of Doctors’ Online Reputation on the Sharing of Outpatient Experiences: Empirical Study. J. Med. Internet Res. 2020, 22, e16691. [Google Scholar] [CrossRef]
- Gong, Y.; Wang, H.; Xia, Q.; Zheng, L.; Shi, Y. Factors that determine a Patient’s willingness to physician selection in online healthcare communities: A trust theory perspective. Technol. Soc. 2021, 64, 101510. [Google Scholar] [CrossRef]
- Chen, S.; Guo, X.; Wu, T.; Ju, X. Exploring the Online Doctor-Patient Interaction on Patient Satisfaction Based on Text Mining and Empirical Analysis. Inf. Process. Manag. 2020, 57, 102253. [Google Scholar] [CrossRef]
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 pandemic: A global health crisis. Physiol. Genom. 2020, 52, 549–557. [Google Scholar] [CrossRef]
- Jang, H.; Rempel, E.; Roth, D.; Carenini, G.; Janjua, N.Z. Tracking COVID-19 Discourse on Twitter in North America: Infodemiology Study Using Topic Modeling and Aspect-Based Sentiment Analysis. J. Med. Internet Res. 2021, 23, e25431. [Google Scholar] [CrossRef]
- Valdez, D.; Thij, M.T.; Bathina, K.; Rutter, L.A.; Bollen, J. Social Media Insights into US Mental Health During the COVID-19 Pandemic: Longitudinal Analysis of Twitter Data. J. Med. Internet Res. 2020, 22, e21418. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-X.; Zhang, Y.-Y.; Zhang, X.-W.; Cao, Y.-H.; Zhang, J. Spatial evolution patterns of public panic on Chinese social networks amidst the COVID-19 pandemic. Int. J. Disaster Risk Reduct. 2022, 70, 102762. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, M.M.; Erondu, N.A.; Tomori, O.; Dzau, V.J.; Okiro, E.A.; Maleche, A.; Aniebo, I.C.; Rugege, U.; Holmes, C.B.; Gostin, L.O. Access to lifesaving medical resources for African countries: COVID-19 testing and response, ethics, and politics. Lancet 2020, 395, 1735–1738. [Google Scholar] [CrossRef]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef] [PubMed]
- Gopichandran, V.; Sakthivel, K. Doctor-patient communication and trust in doctors during COVID 19 times—A cross sectional study in Chennai, India. PLoS ONE 2021, 16, e0253497. [Google Scholar] [CrossRef] [PubMed]
- Sanders, A.C.; White, R.C.; Severson, L.S.; Ma, R.; McQueen, R.; Paulo, H.C.A.; Zhang, Y.; Erickson, J.S.; Bennett, K.P. Unmasking the conversation on masks: Natural language processing for topical sentiment analysis of COVID-19 Twitter discourse. AMIA Summits Transl. Sci. Proc. 2021, 2021, 555–564. [Google Scholar]
- Zhou, Y.; Chen, S.; Liao, Y.; Wu, Q.; Ma, Y.; Wang, D.; Wang, X.; Li, M.; Wang, Y.; Wang, Y.; et al. General Perception of Doctor–Patient Relationship from Patients During the COVID-19 Pandemic in China: A Cross-Sectional Study. Front. Public Health 2021, 9, 646486. [Google Scholar] [CrossRef]
- Debortoli, S.; Müller, O.; Junglas, I.; vom Brocke, J. Text Mining for Information Systems Researchers: An Annotated Topic Modeling Tutorial. Commun. Assoc. Inf. Syst. 2016, 39, 110–135. [Google Scholar] [CrossRef]
- Geldsetzer, P. Use of Rapid Online Surveys to Assess People’s Perceptions During Infectious Disease Outbreaks: A Cross-sectional Survey on COVID-19. J. Med. Internet Res. 2020, 22, e18790. [Google Scholar] [CrossRef]
- Garcia, K.; Berton, L. Topic detection and sentiment analysis in Twitter content related to COVID-19 from Brazil and the USA. Appl. Soft Comput. 2020, 101, 107057. [Google Scholar] [CrossRef]
- Pang, P.C.-I.; Liu, L. Why Do Consumers Review Doctors Online? Topic Modeling Analysis of Positive and Negative Reviews on an Online Health Community in China. In Proceedings of the 53rd Hawaii International Conference on System Sciences, Maui, HI, USA, 7–10 January 2020; pp. 705–714. [Google Scholar] [CrossRef]
- Chandra, R.; Krishna, A. COVID-19 sentiment analysis via deep learning during the rise of novel cases. PLoS ONE 2021, 16, e0255615. [Google Scholar] [CrossRef] [PubMed]
- Amblee, N.; Bui, T. Harnessing the Influence of Social Proof in Online Shopping: The Effect of Electronic Word of Mouth on Sales of Digital Microproducts. Int. J. Electron. Commer. 2011, 16, 91–114. [Google Scholar] [CrossRef]
- Lu, N.; Wu, H. Exploring the impact of word-of-mouth about Physicians’ service quality on patient choice based on online health communities. BMC Med. Inform. Decis. Mak. 2016, 16, 151. [Google Scholar] [CrossRef]
- Hao, H.; Zhang, K. The Voice of Chinese Health Consumers: A Text Mining Approach to Web-Based Physician Reviews. J. Med. Internet Res. 2016, 18, e108. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, X.; Sun, J.; Jiang, Y.; Tian, Z. Understanding Patients’ WOM of IT-Enabled Healthcare Service: A Case Study of Online Health Consultation. 2019, pp. 699–708. Available online: https://hdl.handle.net/10125/59510 (accessed on 3 April 2022).
- Liu, L.; Cui, T.; Lederman, R. Does the Emotional Support Doctors Give Patients Influence Doctors’ Online Reputation? In Proceedings of the Pacific Asia Conference on Information Systems (PACIS) 2021, Virtual Event, 12 July 2021; Available online: https://aisel.aisnet.org/pacis2021/9 (accessed on 13 October 2022).
- Alamoodi, A.; Zaidan, B.; Zaidan, A.; Albahri, O.; Mohammed, K.; Malik, R.; Almahdi, E.; Chyad, M.; Tareq, Z.; Hameed, H.; et al. Sentiment analysis and its applications in fighting COVID-19 and infectious diseases: A systematic review. Expert Syst. Appl. 2020, 167, 114155. [Google Scholar] [CrossRef]
- Pang, P.C.-I. Performance Evaluation of Text Embeddings with Online Consumer Reviews in Retail Sectors. In Proceedings of the IEEE/ACIS 22nd International Hybrid Conference on Computer and Information Science (ICIS 2022), Zhuhai, China, 26–28 June 2022. [Google Scholar] [CrossRef]
- Shah, A.M.; Yan, X.; Qayyum, A.; Naqvi, R.A.; Shah, S.J. Mining topic and sentiment dynamics in physician rating websites during the early wave of the COVID-19 pandemic: Machine learning approach. Int. J. Med. Inform. 2021, 149, 104434. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, L.; Li, X.; Gong, Z. Clinical Challenges in an Outbreak of COVID-19 in Wuhan, China: Concerns from Frontiers. Curr. Infect. Dis. Rep. 2020, 22, 30. [Google Scholar] [CrossRef]
- Pang, P.C.-I.; McKay, D.; Chang, S.; Chen, Q.; Zhang, X.; Cui, L. Privacy concerns of the Australian My Health Record: Implications for other large-scale opt-out personal health records. Inf. Process. Manag. 2020, 57, 102364. [Google Scholar] [CrossRef]
- Medhat, W.; Hassan, A.; Korashy, H. Sentiment analysis algorithms and applications: A survey. Ain Shams Eng. J. 2014, 5, 1093–1113. [Google Scholar] [CrossRef]
- Gao, X.; Ding, X.; Wang, W.; Wang, G.; Kang, Y.; Wang, S. Research on Mathematics Teachers’ Professional Growth Factors Based on Keyword Extraction and Sentiment Analysis. In Artificial Intelligence in Education and Teaching Assessment; Wang, W., Wang, G., Ding, X., Zhang, B., Eds.; Springer: Singapore, 2021; pp. 185–195. [Google Scholar] [CrossRef]
- Qiu, Y.; Song, Z.; Chen, Z. Short-term stock trends prediction based on sentiment analysis and machine learning. Soft Comput. 2022, 26, 2209–2224. [Google Scholar] [CrossRef]
- Hartmann, J.; Heitmann, M.; Siebert, C.; Schamp, C. More than a Feeling: Accuracy and Application of Sentiment Analysis. Int. J. Res. Mark. 2022. [Google Scholar] [CrossRef]
- Baron, A.; Rayson, P.; Archer, D. Word frequency and key word statistics in corpus linguistics. Anglistik 2009, 20, 41–67. [Google Scholar]
- Luo, R.; Xu, J.; Zhang, Y.; Ren, X.; Sun, X. PKUSEG: A Toolkit for Multi-Domain Chinese Word Segmentation. arXiv 2019, arXiv:1906.11455. [Google Scholar]
- Řehůřek, R.; Sojka, P. Software Framework for Topic Modelling with Large Corpora. In Proceedings of the LREC 2010 Workshop on New Challenges for NLP Frameworks, ELRA, Valletta, Malta, 22 May 2010; pp. 45–50. [Google Scholar]
- Oraebosi, M.I.; Chia, T.; Oyeniran, O.I. Preparing the next generation of African Healthcare Workers and Scientists: Lessons from Corona Virus Pandemic. Ethic-Med. Public Health 2020, 14, 100535. [Google Scholar] [CrossRef] [PubMed]
- Wuhan Municipal People’s Government. Just Went Online! Wuhan Online Buy Medicine Can Brush Medical Insurance. 2021. Available online: http://www.wuhan.gov.cn/hdjl/rdhy/202106/t20210618_1722628.shtml (accessed on 15 February 2022).
- National Health and Wellness Commission of the People’s Republic of China. Notice of the General Office of the National Health and Wellness Commission on the Issuance of Interim Provisions on Outpatient Quality Management in Medical Institutions. 2022. Available online: http://www.nhc.gov.cn/cms-search/xxgk/getManuscriptXxgk.htm?id=5cad0dde910549019059b7b62a1110e1 (accessed on 22 July 2022).




{kind=link}
{kind=link}
{kind=link}
| Before Pandemic | During Pandemic | Difference | p-Values | |
|---|---|---|---|---|
| Total | 12,000 | 12,000 | --- | --- |
| Number of Positive | 11,652 | 11,741 | +0.8% | 0.999 |
| Number of Negative | 348 | 259 | −25.5% | <0.001 * |
| Average Sentiment Value | 0.9590 | 0.9595 | +0.1% | 0.501 |
| Number of Highly Positive | 11,258 | 11,183 | >0.7% | <0.001 * |
| Number of Highly Negative | 236 | 112 | >52.5% | <0.001 * |
| Before Pandemic | During Pandemic | Difference | p-Values | |
|---|---|---|---|---|
| Total | 12,000 | 12,000 | --- | --- |
| Number of Positive | 11,744 | 11,828 | +0.7% | 0.999 |
| Number of Negative | 256 | 172 | −32.8% | <0.001 * |
| Average Sentiment Value | 0.9741 | 0.9787 | +0.5% | 0.487 |
| Number of Highly Positive | 11,403 | 11,671 | +2.3% | 0.999 |
| Number of Highly Negative | 134 | 46 | −65.7% | <0.001 * |
| Before Pandemic | During Pandemic | Difference | p-Values | |
|---|---|---|---|---|
| Total | 5300 | 5300 | --- | --- |
| Number of Positive | 5221 | 5237 | +0.3% | 0.965 |
| Number of Negative | 79 | 58 | −26.5% | <0.001 * |
| Average Sentiment Value | 0.9726 | 0.9751 | +0.3% | 0.506 |
| Number of Highly Positive | 4996 | 5011 | +0.3% | 0.812 |
| Number of Highly Negative | 37 | 17 | −54.1% | <0.001 * |
| Cases | Mortality | PTPR | DTPR | HTPR | ASV Difference | Severity Ranking | |
|---|---|---|---|---|---|---|---|
| China | 87,071 | 0.7% | 6.22 × 10−5 | 1.93 × 10−2 | 2.51 × 10−1 | --- | (For Reference) |
| Hubei | 68,149 | 2.9% | 1.18 × 10−3 | 4.48 × 10−1 | 1.92 | +0.3% | 1 |
| Shanghai | 1511 | 0.46% | 6.07 × 10−5 | 7.95 × 10−2 | 2.56 × 10−1 | +0.5% | 2 |
| Beijing | 982 | 0.45% | 7.95 × 10−5 | 7.95 × 10−3 | 8.66 × 10−2 | +0.1% | 3 |
| Positive Comments (Beijing) | Negative Comments (Beijing) | ||
|---|---|---|---|
| Before Pandemic | During Pandemic | Before Pandemic | During Pandemic |
| 1. attitude (1589 times) | 1. attitude (1589 times) | 1. attitude (59 times) | 1. hospitalization (29 times) |
| 2. patience (1258 times) | 2. patience (1258 times) | 2. problem (48 times) | 2. see a doctor (28 times) |
| 3. thanks (870 times) | 3. thanks (870 times) | 3. illness (45 times) | 3. registration (28 times) |
| 4. excellent medical skills (741 times) | 4. excellent medical skills (741 times) | 4. serious (27 times) | 4. outpatient (19 times) |
| 5. patient (725 times) | 5. patient (725 times) | 5. symptom (24 times) | 5. serious (19 times) |
| 6. professional (698 times) | 6. professional (698 times) | 6. very (23 times) | 6. recommendation (16 times) |
| 7. conscientious and responsible (652 times) | 7. conscientious and responsible (652 times) | 7. extreme (23 times) | 7. very (16 times) |
| 8. careful (639 times) | 8. careful (639 times) | 8. registration (18 times) | 8. attitude (15 times) |
| 9. post operation (532 times) | 9. post operation (532 times) | 9. patience (17 times) | 9. post operation (15 times) |
| 10. medical skill (512 times) | 10. medical skill (512 times) | 10. recovery (17 times) | 10. review (15 times) |
| Positive Comments (Shanghai) | Negative Comments (Shanghai) | ||
|---|---|---|---|
| Before Pandemic | During Pandemic | Before Pandemic | During Pandemic |
| 1. attitude (1740 times) | 1. patience (1755 times) | 1. question (44 times) | 1. question (33 times) |
| 2. patience (1466 times) | 2. attitude (1590 times) | 2. attitude (38 times) | 2. attitude (18 times) |
| 3. thanks (933 times) | 3. professional (975 times) | 3. recommendation (28 times) | 3. outpatient (16 times) |
| 4. excellent medical skills (800 times) | 4. post-operation (925 times) | 4. time (27 times) | 4. medical skill (14 times) |
| 5. patient (755 times) | 5. patient (834 times) | 5. expert (23 times) | 5. online (13 times) |
| 6. professional (719 times) | 6. thanks (821 times) | 6. Shanghai (22 times) | 6. find (12 times) |
| 7.careful (659 times) | 7. excellent medical practice (820 times) | 7. unknown (22 times) | 7. symptom (12 times) |
| 8. illness (647 times) | 8. medical skill (789 times) | 8. restoration (20 times) | 8. Shanghai (12 times) |
| 9. conscientious and responsible (568 times) | 9.careful (749 times) | 9. outpatient (19 times) | 9. post-operation (12 times) |
| 10. careful (557 times) | 10. recovery (660 times) | 10. discover (19 times) | 10. review (12 times) |
| Positive Comments (Hubei) | Negative Comments (Hubei) | ||
|---|---|---|---|
| Before Pandemic | During Pandemic | Before Pandemic | During Pandemic |
| 1. very (1292 times) | 1. very (1361 times) | 1. attitude (22 times) | 1. problem (9 times) |
| 2. attitude (727 times) | 2. attitude (663 times) | 2. problem (13 times) | 2. effect (8 times) |
| 3. patient (589 times) | 3. patience (655 times) | 3. effect (8 times) | 3. specialist registration (7 times) |
| 4. attentive (463 times) | 4. attentive (476 times) | 4. online (7 times) | 4. illness (6 times) |
| 5. excellent medical skill (395 times) | 5. patient (430 times) | 5. anemia (7 times) | 5. team (6 times) |
| 6. thanks (384 times) | 6. excellent medical practice (363 times) | 6. illness (6 times) | 6. taking medication (5 times) |
| 7. patient (350 times) | 7. medical skill (361 times) | 7. prescribing (6 times) | 7. attitude (5 times) |
| 8. professional (332 times) | 8. professional (359 times) | 8. delay (6 times) | 8. cough (5 times) |
| 9. medical skill (329 times) | 9. thanks (347 times) | 9. process (5 times) | 9. ordinary (5 times) |
| 10. conscientious and responsible (299 times) | 10. responsible (312 times) | 10. reason (5 times) | 10. inform (4 times) |
| Beijing | Shanghai | Hubei | |
|---|---|---|---|
| Total | 12,000 | 12,000 | 5300 |
| Number of Negative (Before Pandemic) | 348 | 256 | 79 |
| Number of Negative (During Pandemic) | 259 | 172 | 58 |
| Number of Negative Difference p-values about Number of Negative | −25.5% <0.001 * | −32.8% <0.001 * | −26.5% <0.001 * |
| Average Sentiment Value (Before Pandemic) | 0.9590 | 0.9741 | 0.9726 |
| Average Sentiment Value (During Pandemic) | 0.9595 | 0.9787 | 0.9751 |
| Average Sentiment Value Difference p-values about Average Sentiment Value Difference | +0.1% 0.501 | +0.5% 0.487 | +0.3% 0.506 |
| Number of Highly Negative (Before Pandemic) | 236 | 134 | 37 |
| Number of Highly Negative (During Pandemic) | 112 | 46 | 17 |
| Number of Highly Negative Difference p-values about Number of Highly Negative | −52.5% <0.001 * | −65.7% <0.001 * | −54.1% <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Pang, P.C.-I.; Xiao, Y.; Wong, D. Changes in Doctor–Patient Relationships in China during COVID-19: A Text Mining Analysis. Int. J. Environ. Res. Public Health 2022, 19, 13446. https://doi.org/10.3390/ijerph192013446
Li J, Pang PC-I, Xiao Y, Wong D. Changes in Doctor–Patient Relationships in China during COVID-19: A Text Mining Analysis. International Journal of Environmental Research and Public Health. 2022; 19(20):13446. https://doi.org/10.3390/ijerph192013446
Chicago/Turabian StyleLi, Jiaxuan, Patrick Cheong-Iao Pang, Yundan Xiao, and Dennis Wong. 2022. "Changes in Doctor–Patient Relationships in China during COVID-19: A Text Mining Analysis" International Journal of Environmental Research and Public Health 19, no. 20: 13446. https://doi.org/10.3390/ijerph192013446
APA StyleLi, J., Pang, P. C.-I., Xiao, Y., & Wong, D. (2022). Changes in Doctor–Patient Relationships in China during COVID-19: A Text Mining Analysis. International Journal of Environmental Research and Public Health, 19(20), 13446. https://doi.org/10.3390/ijerph192013446