
Effects of Nutrition Counselling and Unconditional Cash Transfer on Child Growth and Family Food Security in Internally Displaced Person Camps in Somalia—A Quasi-Experimental Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Sample Size
2.4. Interventions
2.5. Data Collection
2.6. Primary and Secondary Outcomes Measures
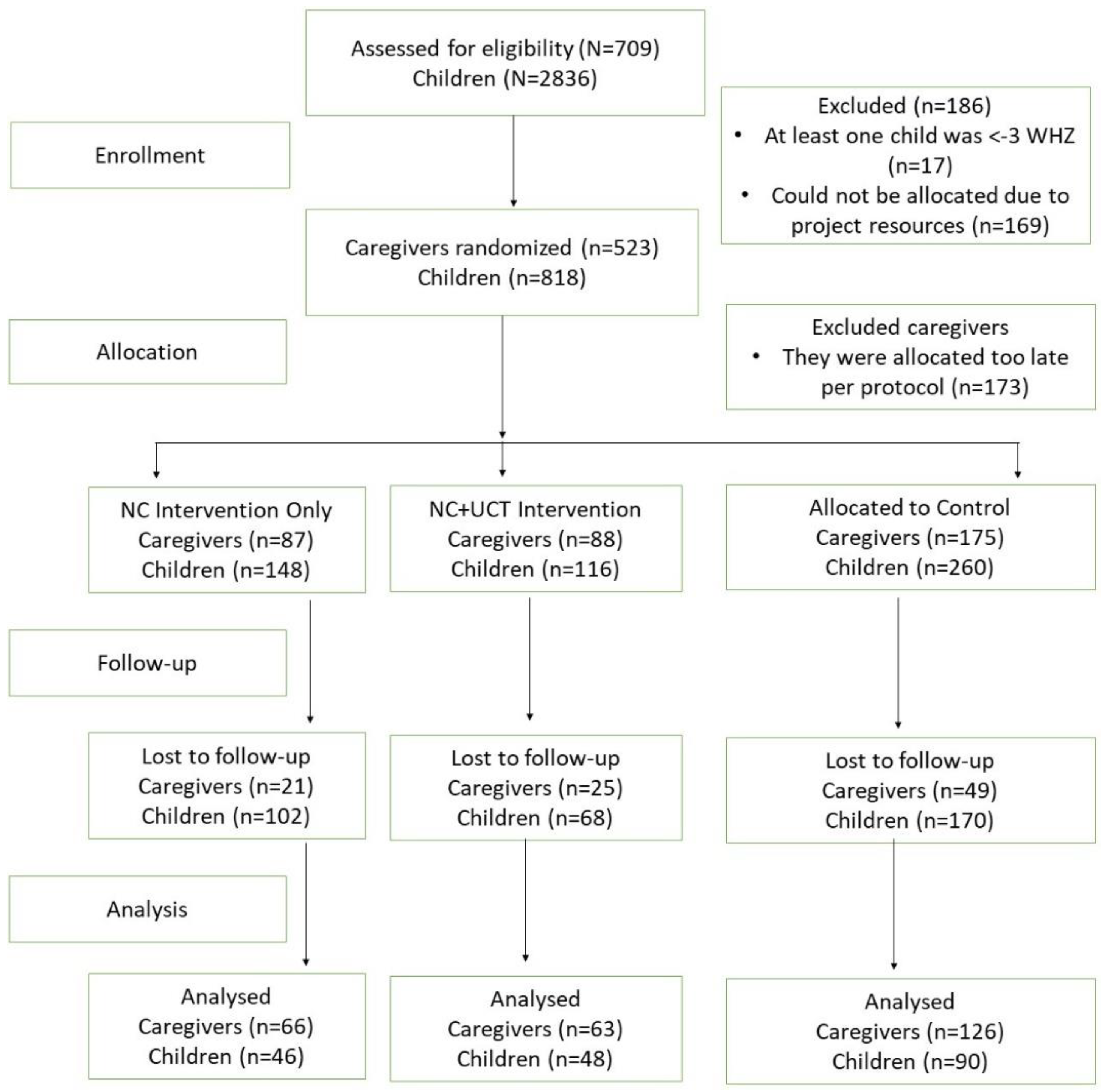
2.7. Randomization
2.8. Statistical Analysis
3. Results
3.1. Growth Outcomes in Children
3.2. Food Security and Household Expenses
4. Discussion
Strength and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Aguayo, V.M.; Badgaiyan, N.; Dzed, L. Determinants of child wasting in Bhutan. Insights from nationally representative data. PHN 2017, 20, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, D.; Amarnani, E.; Sen, A.; Ebadi, N.; Cortbaoui, P.; Melgar-Quiñonez, H. Determinants of child anthropometric indicators in Ethiopia. BMC Public Health 2018, 18, 626. [Google Scholar] [CrossRef] [PubMed]
- United Nations Childrens Fund. Improving Child Nutrition: The Achievable Imperative for Global Progress; UNICEF: New York, NY, USA, 2013; pp. 1–14. [Google Scholar]
- Sandstrom, S.; Juhola, S. Continue to blame it on the rain? Conceptualization of drought and failure of food systems in the Greater Horn of Africa. Environ. Hazards 2017, 16, 71–91. [Google Scholar] [CrossRef]
- Dilley, M.; Boudreau, T.E. Coming to terms with vulnerability: A critique of the food security definition. Food Policy 2001, 26, 229–247. [Google Scholar] [CrossRef]
- Akhade, K.S.; Sankhe, L.R.; Akarte, S.V. Magnitude of malnutrition among underfive children in urban slums of commercial capital of India and its multifactorial causation: A community-based study. Fam. Med. Prim. Care Rev. 2019, 8, 3865. [Google Scholar] [CrossRef]
- Kalid, M.; Osman, F.; Sulaiman, M.; Dykes, F.; Erlandsson, K. Infant and young child nutritional status and their caregivers’ feeding knowledge and hygiene practices in internally displaced person camps, Somalia. BMC Nutr. 2019, 5, 1–11. [Google Scholar] [CrossRef]
- Sircar, N.R.; Friedman, E.A. Financial security and public health: How basic income & cash transfers can promote health. Glob. Public Health 2018, 13, 1878–1888. [Google Scholar]
- Harris-Fry, H.; Saville, N.M.; Paudel, P.; Manandhar, D.S.; Cortina-Borja, M.; Skordis, J. Relative power: Explaining the effects of food and cash transfers on allocative behaviour in rural Nepalese households. J. Dev. Econ. 2022, 154, 102784. [Google Scholar] [CrossRef]
- Fernald, L.C.; Gertler, P.J.; Hidrobo, M. Conditional cash transfer programs: Effects on growth, health, and development in young children. In The Oxford Handbook of Poverty and Child Development; Oxford University Press: Oxford, UK, 2012; pp. 569–600. [Google Scholar]
- Manley, J.; Slavchevska, V. Are cash transfers the answer for child nutrition in sub-Saharan Africa? A literature review. Dev. Policy Rev. 2019, 37, 204–224. [Google Scholar] [CrossRef]
- Owusu-Addo, E.; Renzaho, A.M.; Smith, B.J. The impact of cash transfers on social determinants of health and health inequalities in sub-Saharan Africa: A systematic review. Health Policy Plan. 2018, 33, 675–696. [Google Scholar] [CrossRef] [PubMed]
- Pega, F.; Pabayo, R.; Benny, C.; Lee, E.-Y.; Lhachimi, S.K.; Liu, S.Y. Unconditional cash transfers for reducing poverty and vulnerabilities: Effect on use of health services and health outcomes in low-and middle-income countries. Cochrane Database Syst. Rev. 2017, 2017, CD011135. [Google Scholar] [CrossRef] [PubMed]
- Manley, J.; Balarajan, Y.; Malm, S.; Harman, L.; Owens, J.; Murthy, S.; Stewart, D.; Winder-Rossi, N.E.; Khurshid, A. Cash transfers and child nutritional outcomes: A systematic review and meta-analysis. BMJ Glob. Health 2020, 5, e003621. [Google Scholar] [CrossRef]
- Leroy, J.L.; Ruel, M.; Verhofstadt, E. The impact of conditional cash transfer programmes on child nutrition: A review of evidence using a programme theory framework. J. Dev. Eff. 2009, 1, 103–129. [Google Scholar] [CrossRef]
- De Onis, M.; Onyango, A.W. WHO child growth standards. Lancet 2008, 371, 204. [Google Scholar] [CrossRef]
- Parmar, P.K.; Benjamin-Chung, J.; Smith, L.S.; Htoo, S.N.; Laeng, S.; Lwin, A.; Mahn, M.; Maung, C.; Reh, D.; Shwe Oo, E.K. Health and human rights in eastern Myanmar prior to political transition: A population-based assessment using multistaged household cluster sampling. MC Int. Health Hum. Rights 2014, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mullany, L.C.; Lee, C.I.; Yone, L.; Paw, P.; Oo, E.K.S.; Maung, C.; Lee, T.J.; Beyrer, C. Access to essential maternal health interventions and human rights violations among vulnerable communities in eastern Burma. PLoS Med. 2008, 5, e242. [Google Scholar] [CrossRef] [PubMed]
- Mullany, L.C.; Richards, A.K.; Lee, C.I.; Suwanvanichkij, V.; Maung, C.; Mahn, M.; Beyrer, C.; Lee, T.J. Population-based survey methods to quantify associations between human rights violations and health outcomes among internally displaced persons in eastern Burma. JECH 2007, 61, 908–914. [Google Scholar] [CrossRef]
- World Health Organization &UNICEF. Infant Young Child Feeding Counselling: An Integrated Course 2006; WHO: Geneva, Switzerland, 2014; Volume 11, Available online: http://apps.who.int/iris/bitstream/handle/10665/43567/9789241594745_eng.pdf;jsessionid=70A044F3E278D497DBBCFC9C97C7B6E6?sequence=1 (accessed on 15 February 2021).
- WHO. WHO child growth standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar]
- Radimer, K.L.; Olson, C.M.; Campbell, C.C. Development of indicators to assess hunger. J. Nutr. 1990, 120, 1544–1548. [Google Scholar] [CrossRef]
- Swindale, A.; Bilinsky, P. Household Dietary Diversity Score (HDDS) for Measurement of Household Food Access: Indicator Guide. In FANTA Project; Food and Nutrition Technical Assistance Project, Academy for Educational Development: Washington, DC, USA, 2006. [Google Scholar]
- Filmer, D.; Pritchett, L.H. Estimating wealth effects without expenditure data—Or tears: An application to educational enrollments in states of India. Demography 2001, 38, 115–132. [Google Scholar]
- Nandy, S.; Svedberg, P. The Composite Index of Anthropometric Failure (CIAF): An alternative indicator for malnutrition in young children. In Handbook of Anthropometry; Springer: Berlin/Heidelberg, Germany, 2012; pp. 127–137. [Google Scholar]
- Swindale, A.; Bilinsky, P. Development of a universally applicable household food insecurity measurement tool: Process, current status, and outstanding issues. J. Nutr. 2006, 136, 1449S–1452S. [Google Scholar] [CrossRef]
- Nikièma, L.; Huybregts, L.; Martin-Prevel, Y.; Donnen, P.; Lanou, H.; Grosemans, J.; Offoh, P.; Dramaix-Wilmet, M.; Sondo, B.; Roberfroid, D.; et al. Effectiveness of facility-based personalized maternal nutrition counseling in improving child growth and morbidity up to 18 months: A cluster-randomized controlled trial in rural Burkina Faso. PLoS ONE 2017, 12, e0177839. [Google Scholar] [CrossRef]
- Elisaria, E.; Mrema, J.; Bogale, T.; Segafredo, G.; Festo, C. Effectiveness of integrated nutrition interventions on childhood stunting: A quasi-experimental evaluation design. BMC Nutr. 2021, 7, 17. [Google Scholar] [CrossRef]
- Ahmed, A.; Hoddinott, J.; Roy, S. Food Transfers, Cash Transfers, Behavior Change Communication and Child Nutrition: Evidence from Bangladesh; International Food Policy Research Institute: Washington, DC, USA, 2019; Volume 1868. [Google Scholar]
- de Groot, R.; Yablonski, J.; Valli, E. The impact of cash and health insurance on child nutrition during the first 1000 days: Evidence from Ghana. Food Policy 2022, 107, 102217. [Google Scholar] [CrossRef]
- van Daalen, K.R.; Dada, S.; James, R.; Ashworth, H.C.; Khorsand, P.; Lim, J.; Mooney, C.; Khankan, Y.; Essar, M.Y.; Kuhn, I.; et al. Impact of conditional and unconditional cash transfers on health outcomes and use of health services in humanitarian settings: A mixed-methods systematic review. BMJ Glob. Health 2022, 7, e007902. [Google Scholar] [CrossRef]
- Seal, A.; Dolan, C.; Trenouth, L. REFANI Synthesis Report. Research on Food Assistance for Nutritional Impact; Consortium London: London, UK, 2017. [Google Scholar]
- Seidenfeld, D.; Handa, S.; Tembo, G.; Michelo, S.; Harland Scott, C.; Prencipe, L. The Impact of an Unconditional Cash Transfer on Food Security and Nutrition: The Zambia Child Grant Programme; Institute of Development Studies: Falmer, UK, 2014; pp. 36–42. [Google Scholar]
- Davis, B.; Handa, S. How Much Do Programmes Pay? Transfer Size in Selected National Cash Transfer Programmes in Sub-Saharan Africa; UNICEF. Office of Research-Innocenti: New York, NY, USA, 2015. [Google Scholar]
- Grijalva-Eternod, C.S.; Jelle, M.; Haghparast-Bidgoli, H.; Colbourn, T.; Golden, K.; King, S.; Cox, C.L.; Morrison, J.; Skordis-Worrall, J.; Fottrell, E. A cash-based intervention and the risk of acute malnutrition in children aged 6–59 months living in internally displaced persons camps in Mogadishu, Somalia: A non-randomised cluster trial. PLoS Med. 2018, 15, e1002684. [Google Scholar] [CrossRef]
- Bastagli, F.; Hagen-Zanker, J.; Harman, L.; Barca, V.; Sturge, G.; Schmidt, T.; Pellerano, L. Cash Transfers: What Does the Evidence Say. A Rigorous Review of Programme Impact and the Role of Design and Implementation Features; ODI: London, UK, 2016; Volume 1. [Google Scholar]
- Yoong, J.; Rabinovich, L.; Diepeveen, S. The Impact of Economic Resource Transfers to Women Versus Men: A Systematic Review; Institute of Education technical report; University of London (London, EPPI-Centre): London, UK, 2012. [Google Scholar]
- Tommasi, D. Control of resources, bargaining power and the demand of food: Evidence from PROGRESA. J. Econ. Behav. Organ. 2019, 161, 265–286. [Google Scholar] [CrossRef]
- Giugliani, E.R.; Horta, B.L.; Loret de Mola, C.; Lisboa, B.O.; Victora, C.G. Effect of breastfeeding promotion interventions on child growth: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 20–29. [Google Scholar] [CrossRef]
- Renzaho, A.M.N.; Chen, W.; Rijal, S.; Dahal, P.; Chikazaza, I.R.; Dhakal, T.; Chitekwe, S. The impact of unconditional child cash grant on child malnutrition and its immediate and underlying causes in five districts of the Karnali Zone, Nepal–A trend analysis. Arch Public Health 2019, 77, 24. [Google Scholar] [CrossRef]
- Dewey, K.G. Reducing stunting by improving maternal, infant and young child nutrition in regions such as South Asia: Evidence, challenges and opportunities. Matern. Child. Nutr. 2016, 12, 27–38. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.M.; Olofin, I.; Flaxman, S.; Fawzi, W.W.; Spiegelman, D.; Caulfield, L.E.; Black, R.E.; Ezzati, M.; Danaei, G.; Study, N.I.M. The effect of multiple anthropometric deficits on child mortality: Meta-analysis of individual data in 10 prospective studies from developing countries. AJCN 2013, 97, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, L.E.; de Onis, M.; Blössner, M.; Black, R.E. Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumonia, malaria, and measles. AJCN 2004, 80, 193–198. [Google Scholar] [CrossRef]
- Christian, P.; Lee, S.E.; Donahue Angel, M.; Adair, L.S.; Arifeen, S.E.; Ashorn, P.; Barros, F.C.; Fall, C.H.; Fawzi, W.W.; Hao, W. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low-and middle-income countries. Int. J. Epidemiol. 2013, 42, 1340–1355. [Google Scholar] [CrossRef]
- Danaei, G.; Andrews, K.G.; Sudfeld, C.R.; Fink, G.; McCoy, D.C.; Peet, E.; Sania, A.; Smith Fawzi, M.C.; Ezzati, M.; Fawzi, W.W. Risk factors for childhood stunting in 137 developing countries: A comparative risk assessment analysis at global, regional, and country levels. PLoS Med. 2016, 13, e1002164. [Google Scholar] [CrossRef]
- Hillbruner, C.; Moloney, G. When early warning is not enough—Lessons learned from the 2011 Somalia Famine. Glob. Food Sec. 2012, 1, 20–28. [Google Scholar] [CrossRef]
- Bhandari, N.; Mazumder, S.; Bahl, R.; Martines, J.; Black, R.; Bhan, M. Other members of the Infant Feeding Study Group: An educational intervention to promote appropriate complementary feeding practices and physical growth in infants and young children in rural Haryana, India. J. Nutr. 2004, 134, 2342–2348. [Google Scholar] [PubMed]


{kind=link}
| Topics Covered |
|---|
|
| Caregiver Variables | Baseline | |||
|---|---|---|---|---|
| NC (n = 87) | NC + UCT (n = 88) | Control (n = 175) | ||
| Districts | Dayniile, n (%) | 22 (25.3) | 22 (25) | 44 (25.1) |
| Dharkanley, n (%) | 65 (74.7) | 66 (75.0) | 131 (74.9) | |
| Caregiver age, n (%) | 15–19 | 3 (3.5) | 6 (6.8) | 16 (9.1) |
| 20–29 | 37 (42.5) | 64 (72.7) | 89 (50.9) | |
| 30–39 | 41 (47.1) | 16 (18.2) | 60 (34.3) | |
| 40≥ | 6 (6.9) | 2 (2.3) | 10 (5.7) | |
| Married caregivers, n (%) | 84 (97.0) | 86 (97.7) | 155 (88.6) | |
| Age at first marriage, (mean ± sd) | 16.0 ± 1.8 | 16 ± 2.4 | 16.0 ± 2.2 | |
| Age at first childbirth, (mean ± sd) | 17.0 ± 1.8 | 18.0 ± 2.4 | 17.0 ± 2.1 | |
| Socioeconomic status of household, n (%) | Low | 28 (32) | 26 (30) | 42 (24) |
| Middle | 25 (28.7) | 22 (25) | 45 (25.7) | |
| Upper | 34 (39.1) | 40 (45.5) | 88 (50.3) | |
| Average number of children, (mean ± sd) | 7 ± 3.5 | 5 ± 3.1 | 5 ± 3.1 | |
| Caregivers attended ANC during the last pregnancy a, n (%) | 27 (79.4) | 32 (94.1) | 56 (93.3) | |
| Month visited at ANC during the first pregnancy a, (mean ± sd) | 5 ± 1.6 | 4 ± 1.5 | 4 ± 1.5 | |
| Child Variables | NC (n = 148) | NC + UCT (n = 116) | Control (n = 260) | |
| Sex of child is female, n (%) | 24 (52.2) | 25 (52.1) | 50 (55.6) | |
| Age of the child in months, (mean ± sd) | 34.7 ± 15.9 | 27 ± 15.3 | 29.7 ± 14.9 | |
| Variables of Interest | NC | NC + UCT | Control | Effect of NC vs. Control | p | Effects of NC + UCT vs. Control | p | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | Baseline | Follow-Up | Adjusted OR (95% CI) a | Adjusted OR (95% CI) a | |||
| n = 148 | n = 46 | n = 116 | n = 48 | n = 260 | n = 90 | |||||
| Wasting, n (%) | 18 (12.2) | 7 (15.2) | 18 (15.5) | 9 (18.7) | 31 (11.9) | 16 (17.8) | 0.81 (0.26–2.56) | 0.722 | 0.79 (0.26–2.36) | 0.67 |
| Underweight, n (%) | 44 (29.7) | 21 (45.7) | 42 (36.2) | 22 (45.8) | 91 (35.00) | 43 (47.8) | 1.29 (0.40–3.48) | 0.603 | 0.88 (0.33–2.35) | 0.81 |
| Stunting, n (%) | 25 (16.9) | 10 (21.7) | 20 (17.2) | 16 (33.3) | 44 (16.9) | 22 (24.4) | 0.84 (0.29–2.46) | 0.764 | 1.51 (0.55–4.20) | 0.43 |
| Composite index of anthropometric failure b, n (%) | 62 (41.9) | 28 (60.8) | 58 (50.0) | 32 (66.7) | 124 (47.7) | 57 (63.3) | 1.21 (0.45–3.25) | 0.701 | 1.06 (0.39–2.87) | 0.91 |
| Children’s minimum dietary diversity (≥4 food groups), n (%) | 18 (12.2) | 28 (60.9) | 9 (7.8) | 22 (45.8) | 31 (11.9) | 52 (57.8) | 1.16 (0.39–3.48) | 0.779 | 1.01 (0.31–3.27) | 0.99 |
| Child dietary diversity score (mean ± sd) | 3.3 ± 1.2 | 4.8 ± 1.6 | 2.9 ± 1.3 | 4.6 ± 2.0 | 3.2 ± 1.4 | 4.8 ± 1.9 | −0.18 (−0.90) | 0.612 | 0.03 (−0.78–0.84) | 0.95 |
| Indicator of Interest | NC | NC + UCT | Control | Effect of NC vs. Control | p | Effect of NC + UCT vs. Control | p | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline n = 87 | Follow-Up n = 66 | Baseline n = 88 | Follow-Up n = 63 | Baseline n = 175 | Follow-Up n = 126 | Adjusted Coefficient (95% CI) | Adjusted Coefficient (95% CI) | |||
| Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | Mean (95% CI) | |||||
| Household dietary diversity score (12 food groups) | 6.9 (6.6–7.3) | 7.2 (6.7–7.7) | 6.8 (6.5–7.2) | 7.4 (7.1–7.8) | 6.8 (6.7–7.0) | 7.4 (7.1–7.8) | −0.3 (−1.2–0.4) | 0.31 | −0.1 (−0.8–0.7) | 0.90 |
| Household hunger scale score | 3.3 (3.1–3.6) | 2.1 (1.7–2.5) | 3.3 (3.1–3.6) | 2.6 (2.2–3.0) | 3.5 (3.3–3.7) | 2.5 (2.2–2.8) | −0.2 (−0.9–0.4) | 0.37 | 0.2 (−0.3–0.8) | 0.55 |
| Household food consumption score | 10.5 (9.7–11.4) | 10.9 (9.8–12.0) | 10.0 (9.4–10.7) | 11.8 (10.9–12.7) | 10.8 (10.3–11.3) | 11.8 (11.3–15.5) | −0.7 (−2.2–0.8) | 0.35 | 0.7 (−0.7–2.0) | 0.31 |
| Household Expenses a | ||||||||||
| Food | 46 (40.5–51.0) | 46 (40.3–52.6) | 41 (35.8–46.5) | 43 (39.2–46.9) | 43 (39.4–47.3) | 39 (36.7–41.9) | 4.7 (−3.7–13.1) | 0.27 | 5.9 (−1.9–13.7) | 0.14 |
| Water | 9 (6.8–10.3) | 6 (4.8–6.6) | 8 (6.2–9.2) | 6 (4.5–7.2) | 8 (7.2–9.6) | 5 (4.3–5.8) | 0.4 (−1.7–2.6) | 0.69 | 1.4 (−0.7–3.6) | 0.18 |
| Fuel for cooking | 9 (7.4–10.8) | 9 (7.0–10.3) | 7 (5.8–8.4) | 7 (6.4–8.4) | 8 (6.9–8.8) | 7 (6.5–7.9) | 0.21 (−2.3–2.8) | 0.86 | 0.94 (−0.9–2.8) | 0.34 |
| Education | 4 (2.2–5.2) | 5 (3.1–6.9) | 2 (0.5–2.8) | 2 (0.7–2.9) | 3 (1.5–3.9) | 4 (2.7–5.3) | −0.1 (−3.2–3.1) | 0.96 | −1.2 (−3.7–1.3) | 0.34 |
| Health expenses for children under 18 | 4 (2.5–5.7) | 4 (1.7–7.3) | 3 (1.4–3.6) | 1 (0.4–2.2) | 2 (1.4–3.0) | 2 (0.8–2.3) | 0.3 (−3.9–4.4) | 0.90 | −0.7 (−2.6–1.1) | 0.41 |
| Health expenses for all members over 18 | 4 (2.3–5.6) | 2 (0.9–3.6) | 3 (1.8–4.5) | 1 (0.03–1.3) | 3 (1.7–4.7) | 2 (0.7–2.2) | −0.0 (−2.6–2.5) | 0.98 | −0.8 (−3.0–1.4) | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, M.K.; Flacking, R.; Sulaiman, M.; Osman, F. Effects of Nutrition Counselling and Unconditional Cash Transfer on Child Growth and Family Food Security in Internally Displaced Person Camps in Somalia—A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2022, 19, 13441. https://doi.org/10.3390/ijerph192013441
Ali MK, Flacking R, Sulaiman M, Osman F. Effects of Nutrition Counselling and Unconditional Cash Transfer on Child Growth and Family Food Security in Internally Displaced Person Camps in Somalia—A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2022; 19(20):13441. https://doi.org/10.3390/ijerph192013441
Chicago/Turabian StyleAli, Mohamed Kalid, Renée Flacking, Munshi Sulaiman, and Fatumo Osman. 2022. "Effects of Nutrition Counselling and Unconditional Cash Transfer on Child Growth and Family Food Security in Internally Displaced Person Camps in Somalia—A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 19, no. 20: 13441. https://doi.org/10.3390/ijerph192013441
APA StyleAli, M. K., Flacking, R., Sulaiman, M., & Osman, F. (2022). Effects of Nutrition Counselling and Unconditional Cash Transfer on Child Growth and Family Food Security in Internally Displaced Person Camps in Somalia—A Quasi-Experimental Study. International Journal of Environmental Research and Public Health, 19(20), 13441. https://doi.org/10.3390/ijerph192013441