
A Qualitative Evaluation of the Barriers and Enablers for Implementation of an Asymptomatic SARS-CoV-2 Testing Service at the University of Nottingham: A Multi-Site Higher Education Setting in England

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
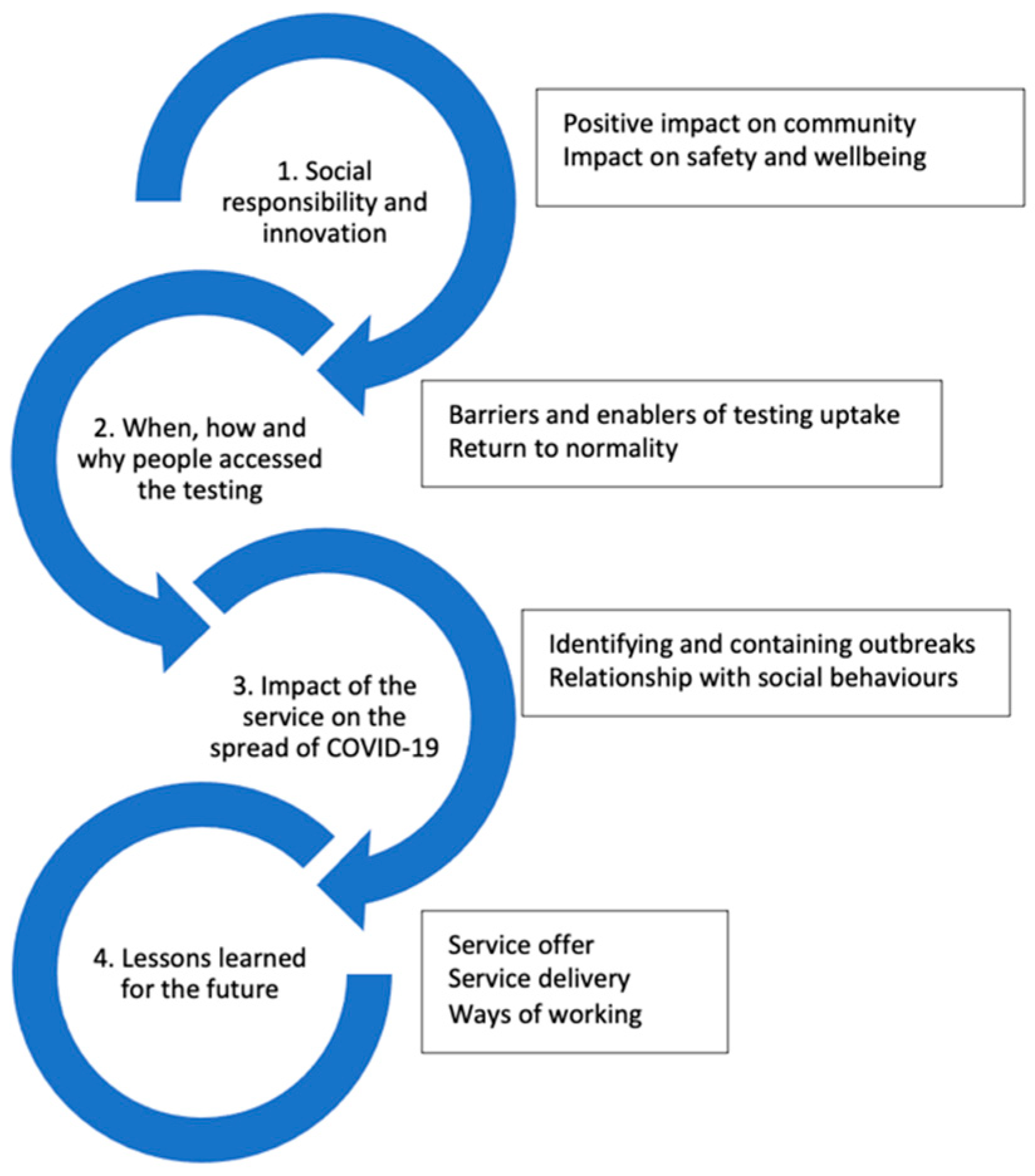
3.1. Theme 1: Social Responsibility and Innovation
3.1.1. Sub-Theme 1: Positive Impact on Community
“…whenever we started the testing site momentum, that had a very strong and positive impact on the community …by us taking the testing out to the community area and being visible it showed how serious we took the pandemic itself …just being more visible was pretty big.”(Respondent 5)
3.1.2. Sub-Theme 2: Impact on Safety and Wellbeing
“…having these sorts of testing things would mean that if they were in, they knew that most of the people there were being tested and were therefore safe…I think it was incredibly reassuring.”(Respondent 12)
“They were incredibly grateful for it because a number of members of staff had ‘at risk’ partners for health reasons to covid so to know that they could test regularly and know that they were not going to put their partner or family member at risk was a huge benefit for them.”(Respondent 15)
“…they’ve been getting tested to make sure that they, they keep their, their partner safe and therefore they, the, the wider population safe as well.”(Respondent 8)
“…Staff would have been more worried because the isolating for 10 days would have meant losing 10 days of work, or potentially bringing COVID to their family, kids etc and I think, if anything it was the value of the service was appreciated more by staff in my opinion for these reasons.”(Respondent 3)
3.2. Theme 2: When, How and Why People Accessed the Testing
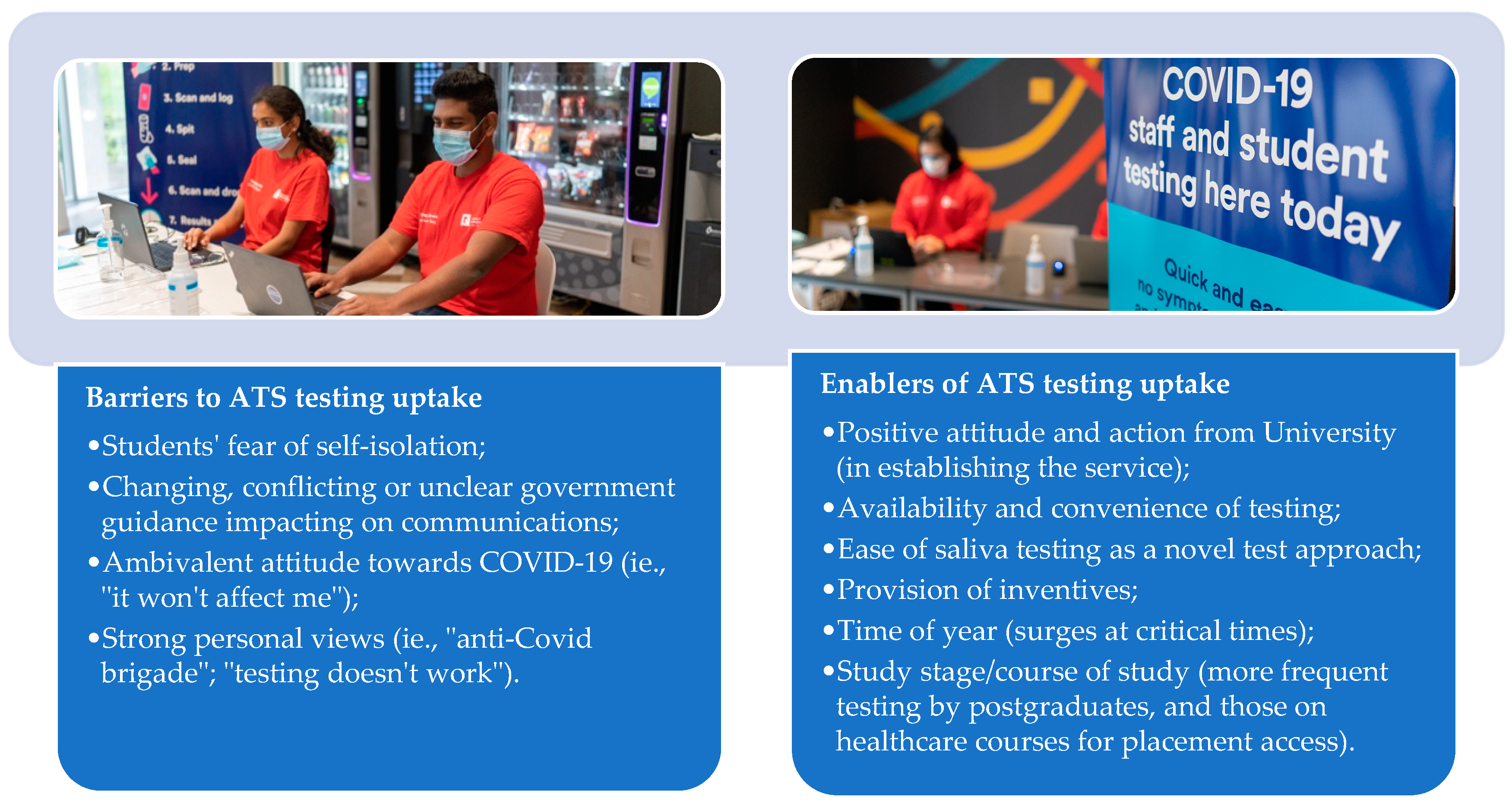
3.2.1. Sub-Theme: Barriers and Enablers of Testing Uptake
“…the sheer demand of the test at peak times like end of terms or before holidays, like Christmas, they were very popular times for the test, people heavily relied on the test to feel safe, to go home to their family …”(Respondent 3)
“we always saw an uptake in the number of students who were testing when, when it was incentivised.”(Respondent 24)
“… it’s a great window into human psyche that offering a relatively small treat as it were, gave people a positive reason to, uh, to, to want to donate a, a saliva sample rather than just being told that they had to…”(Respondent 8)
“…they just simply didn’t like the swab testing…the ability to just basically dribble into a tube and then pop that in a bag and leave it somewhere for somebody to collect and then report back whether you’re positive or not positive…seemed very beneficial.”(Respondent 8)
“…the students were so worried that they would test positive, and then the whole floor [of the residence] would need to isolate…human nature was different to what we predicted.”(Respondent 13)
“… we extended our provision to cover primary school age children of staff to help them when the schools were requiring regular test …I do believe that the staff really value the service that we provide.”(Respondent 16)
“…the easing of … the rules to a way that negatively impacts on the people’s desire to test.”(Respondent 7)
“…when the national regulations were eased off and pretty much scrapped it meant we got less people testing… our sample numbers fell through the floor…government guidelines definitely hindered the sort of, the input and output of the service.”(Respondent 10)
3.2.2. Return to Normality
“…that thing with the NHS, which was the alternative…you could order lateral flows, or you could ask for PCR [polymerase chain reaction], but the PCR you were supposed to have symptoms to get it but with our PCR test, they could be testing daily, even without having the symptoms so they could catch the infection extremely early on.”(Respondent 2)
3.3. Impact of the Service on the Spread of COVID-19
3.3.1. Identifying and Containing Outbreaks
“I think we ended up just chasing outbreaks rather than preventing them, which was fine because we just identified lots of problems, but we didn’t know what to do with the outbreaks once they were there other than to say isolate but because the government guidance changed so much, you know Halls are not a household, household isn’t a massive building so how you know, it’s almost like we needed some clearer guidance on what to tell students once they were positive.”(Respondent 1)
“…if testing was mandated, it would be a more effective service, and a large amount of time and thought was given to how we engage with students, where it’s an optional process.”(Respondent 24)
“I don’t think it was helpful in stopping spread, because of, the inability of the university to make it a requirement…I was met with, well, they can’t mandate testing…”(Respondent 21)
3.3.2. Relationship with Social Behaviours
“I think the people who were going to follow the rules and social distance and wash their hands …they would have done so even if the Testing Service wasn’t in place, but it might have been a good reminder.”(Respondent 21)
“…people went to the either extreme…you would have people who were like ‘I am negative, so give me a hug, so it’s fine, we will share a drink’ or whatever and then you had other people who were the opposite who said ‘I’m negative, I don’t’ want to get it, so don’t go near me.’ But it forced people into two very extreme views and behaviours, I think. I don’t think anyone was really in the middle by the end.”(Respondent 1)
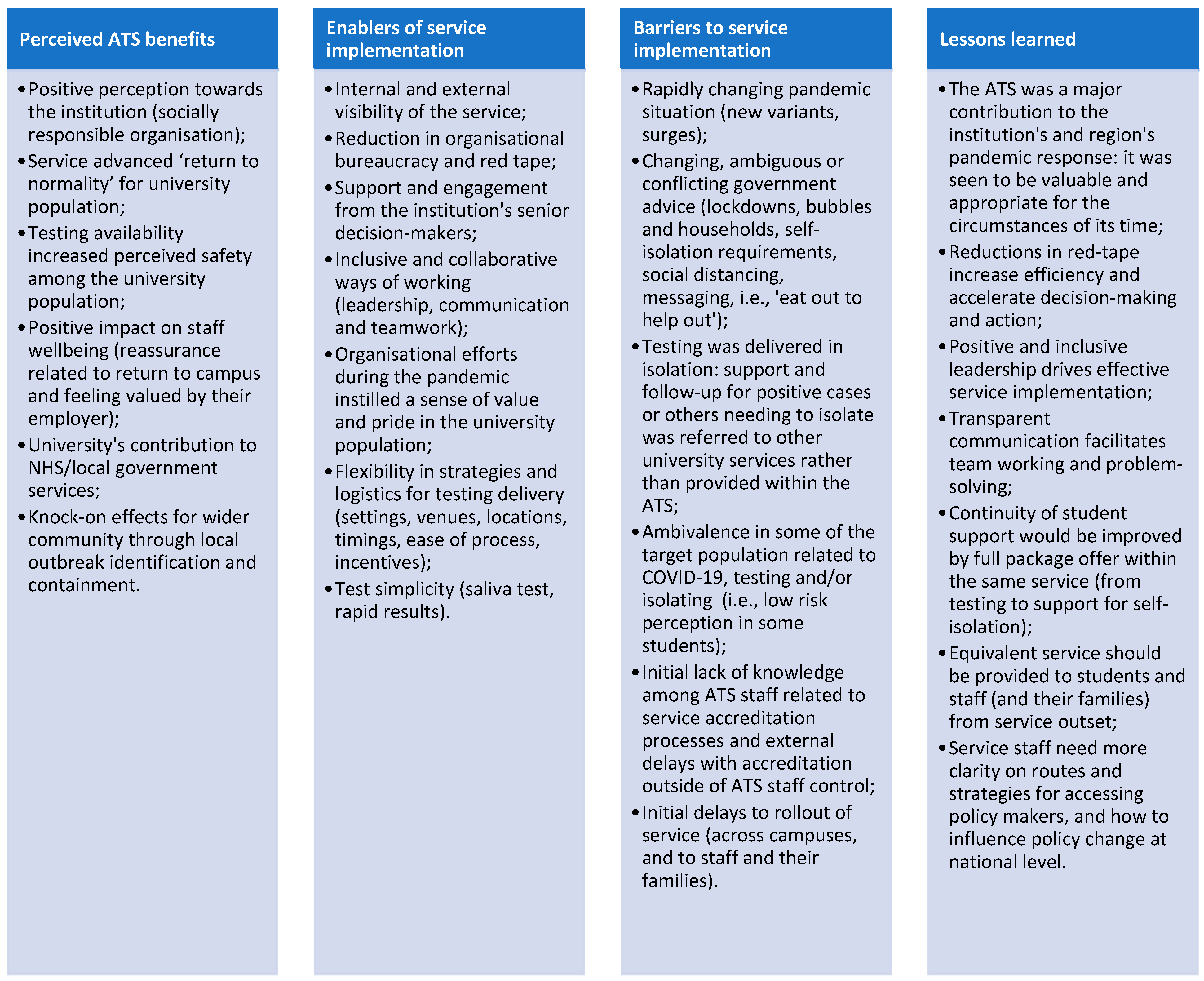
3.4. Lessons Learned for the Future
3.4.1. Service Offer
“…but I guess that what the service is a testing service, you know if it wanted to also, it could have extended to isolation service and wellbeing, but we gave that back to the Uni to do really. It was like at the end of our remit, erm, which you know, was hard because we were the ones telling people, and ‘cause it was a telephone call, it wasn’t just an email, that you didn’t know these people, you got to hear their voices, got to hear how they reacted, it was quite hard, because you want to do more…”(Respondent 1)
“…I was pushing in those early days that we had opened up the testing service much more quickly to, to staff members … better integration of, of the students and the staff early on, and then expanding it out more rapidly to the, the family members.”(Respondent 8)
3.4.2. Service Delivery
“…a bit of a regret there that we weren’t able to get better engagement with the government departments to roll out what arguably is a simpler and an easier test.”(Respondent 8)
3.4.3. Ways of Working
“…throw money and give us roots to get problems solved without a huge amount of red tape…we can just operate to get something done...having a hotline to the people that can actually make decisions that the university will follow was particularly welcome.”(Respondent 12)
4. Discussion
4.1. Theme 1: Social Responsibility and Innovation
4.2. Themes 2 and 3: Testing Uptake and Service Impact on the Spread of COVID-19
4.3. Theme 4: Lessons Learned for the Future
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gebru, A.A.; Birhanu, T.; Wendimu, E.; Ayalew, A.F.; Mulat, S.; Abasimel, H.Z.; Kazemi, A.; Tadesse, B.A.; Gebru, B.A.; Deriba, B.S. Global burden of COVID-19: Situational analyis and review. Hum. Antibodies 2021, 29, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Knight, H.; Carlisle, S.; O’Connor, M.; Briggs, L.; Fothergill, L.; Al-Oraibi, A.; Yildirim, M.; Morling, J.R.; Corner, J.; Ball, J. Impacts of the COVID-19 pandemic and Self-Isolation on students and staff in higher education: A qualitative study. Int. J. Environ. Res. Public Health 2021, 18, 10675. [Google Scholar] [CrossRef]
- Blake, H.; Knight, H.; Jia, R.; Corner, J.; Morling, J.R.; Denning, C.; Ball, J.K.; Bolton, K.; Figueredo, G.; Morris, D.E. Students’ views towards SARS-CoV-2 mass asymptomatic testing, social distancing and self-isolation in a university setting during the COVID-19 pandemic: A qualitative study. Int. J. Environ. Res. Public Health 2021, 18, 4182. [Google Scholar] [CrossRef] [PubMed]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Leal Filho, W.; Wall, T.; Rayman-Bacchus, L.; Mifsud, M.; Pritchard, D.J.; Lovren, V.O.; Farinha, C.; Petrovic, D.S.; Balogun, A.-L. Impacts of COVID-19 and social isolation on academic staff and students at universities: A cross-sectional study. BMC Public Health 2021, 21, 1213. [Google Scholar] [CrossRef]
- Blake, H.; Mahmood, I.; Dushi, G.; Yildirim, M.; Gay, E. Psychological impacts of COVID-19 on healthcare trainees and perceptions towards a digital wellbeing support package. Int. J. Environ. Res. Public Health 2021, 18, 10647. [Google Scholar] [CrossRef] [PubMed]
- Segaloff, H.E.; Cole, D.; Rosenblum, H.G.; Lee, C.C.; Morgan, C.N.; Remington, P.; Pitts, C.; Kelly, P.; Baggott, J.; Bateman, A.; et al. Risk Factors for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection and Presence of Anti–SARS-CoV-2 Antibodies among University Student Dormitory Residents, September–November 2020; Open Forum Infectious Diseases; Oxford University Press: New York, NY, USA, 2021; p. ofab405. [Google Scholar]
- Amen, A.M.; Barry, K.W.; Boyle, J.M.; Brook, C.E.; Choo, S.; Cornmesser, L.T.; Dilworth, D.J.; Doudna, J.A.; Ehrenberg, A.J.; Fedrigo, I.; et al. Blueprint for a pop-up SARS-CoV-2 testing lab. Nat. Biotechnol. 2020, 38, 791–797. [Google Scholar] [CrossRef]
- Faherty, L.J.; Master, B.K.; Steiner, E.D.; Kaufman, J.H.; Predmore, Z.; Stelitano, L.; Leschitz, J.T.; Phillips, B.; Schwartz, H.L.; Wolfe, R.L. COVID-19 Testing in K-12 Schools: Insights from Early Adopters; RAND Corporation: Santa Monica, CA, USA, 2021. [Google Scholar] [CrossRef]
- Maya, S.; McCorvie, R.; Jacobson, K.; Shete, P.B.; Bardach, N.; Kahn, J.G. COVID-19 Testing Strategies for K-12 Schools in California: A Cost-Effectiveness Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9371. [Google Scholar] [CrossRef]
- Perkins, T.A.; Stephens, M.; Alvarez Barrios, W.; Cavany, S.; Rulli, L.; Pfrender, M.E. Performance of Three Tests for SARS-CoV-2 on a University Campus Estimated Jointly with Bayesian Latent Class Modeling. Microbiol. Spectr. 2022, 10, e01220-21. [Google Scholar] [CrossRef] [PubMed]
- Towers, S.A.; Gemechu, N.B.; Nagaraj, N.C.; Landry, M.M.; Beane, P.; Sardon, G.A., Jr.; Weiss, E.C.; Liu, C.M.; Park, D.E.; Aziz, M.; et al. SARS-CoV-2 surveillance and outbreak response on an urban American college campus. J. Am. Coll. Health 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ranoa, D.R.E.; Holland, R.L.; Alnaji, F.G.; Green, K.J.; Wang, L.; Fredrickson, R.L.; Wang, T.; Wong, G.N.; Uelmen, J.; Maslov, S. Mitigation of SARS-CoV-2 transmission at a large public university. Nat. Commun. 2022, 13, 3207. [Google Scholar] [CrossRef] [PubMed]
- Kuhfeldt, K.; Turcinovic, J.; Sullivan, M.; Landaverde, L.; Doucette-Stamm, L.; Hamer, D.H.; Platt, J.T.; Klapperich, C.; Landsberg, H.E.; Connor, J.H. Examination of SARS-CoV-2 In-Class Transmission at a Large Urban University with Public Health Mandates Using Epidemiological and Genomic Methodology. JAMA Netw. Open 2022, 5, e2225430. [Google Scholar] [CrossRef] [PubMed]
- Goss, M.D.; Checovich, M.M.; Bell, C.; Barlow, S.; Temte, J.L. Surveillance of SARS-CoV-2 in Asymptomatic Faculty and Staff at the University of Wisconsin-Madison. WMJ 2022, 121, 121–126. [Google Scholar]
- Landaverde, L.; McIntyre, D.; Robson, J.; Fu, D.; Ortiz, L.; Chen, R.; Oliveira, S.M.; Fan, A.; Barrett, A.; Burgay, S.P. Buildout and integration of an automated high-throughput CLIA laboratory for SARS-CoV-2 testing on a large urban campus. SLAS Technol. 2022, 27, 302–311. [Google Scholar] [CrossRef]
- Weil, A.A.; Sohlberg, S.L.; O’Hanlon, J.A.; Casto, A.M.; Emanuels, A.W.; Lo, N.K.; Greismer, E.P.; Magedson, A.M.; Wilcox, N.C.; Kim, A.E.; et al. SARS-CoV-2 Epidemiology on a Public University Campus in Washington State. Open Forum Infect Dis. 2021, 8, ofab464. [Google Scholar] [CrossRef]
- Ehrenberg, A.J.; Moehle, E.A.; Brook, C.E.; Doudna Cate, A.H.; Witkowsky, L.B.; Sachdeva, R.; Hirsh, A.; Barry, K.; Hamilton, J.R.; Lin-Shiao, E. Launching a saliva-based SARS-CoV-2 surveillance testing program on a university campus. PLoS ONE 2021, 16, e0251296. [Google Scholar] [CrossRef]
- Hockstein, N.G.; Moultrie, L.; Fisher, M.; Mason, R.C.; Scott, D.C.; Coker, J.F.; Tuxward, A.; Terheyden, J.; Canter, N.; Coons, M. Assessment of a multifaceted approach, including frequent PCR testing, to mitigation of COVID-19 transmission at a residential historically Black university. JAMA Netw. Open 2021, 4, e2137189. [Google Scholar] [CrossRef]
- Chang, J.T.; Crawford, F.W.; Kaplan, E.H. Repeat SARS-CoV-2 testing models for residential college populations. Health Care Manag. Sci. 2021, 24, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.M.; Atkins, B.D.; Keeling, M.J.; Tildesley, M.J.; Dyson, L. Modelling SARS-CoV-2 transmission in a UK university setting. Epidemics 2021, 36, 100476. [Google Scholar] [CrossRef] [PubMed]
- Lopman, B.; Liu, C.Y.; Le Guillou, A.; Handel, A.; Lash, T.L.; Isakov, A.P.; Jenness, S.M. A modeling study to inform screening and testing interventions for the control of SARS-CoV-2 on university campuses. Sci. Rep. 2021, 11, 5900. [Google Scholar] [CrossRef] [PubMed]
- Packel, L.; Reingold, A.; Hunter, L.; Facente, S.; Li, Y.; Harte, A.; Nicolette, G.; Urnov, F.D.; Lu, M.; Petersen, M. Piloting an integrated SARS-CoV-2 testing and data system for outbreak containment among college students: A prospective cohort study. PLoS ONE 2021, 16, e0245765. [Google Scholar] [CrossRef] [PubMed]
- Nerhood, K.J.; James, E.R.; Hardin, A.; Bray, J.E.; Hines, T.S.; Young, A.E.; Bhavnani, D. Screening Programs for SARS-CoV-2 Infections on a University Campus—Austin, Texas, 30 September–30 November 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 1201. [Google Scholar] [CrossRef] [PubMed]
- Denny, T.N.; Andrews, L.; Bonsignori, M.; Cavanaugh, K.; Datto, M.B.; Deckard, A.; DeMarco, C.T.; DeNaeyer, N.; Epling, C.A.; Gurley, T. Implementation of a pooled surveillance testing program for asymptomatic SARS-CoV-2 infections on a college campus—Duke University, Durham, North Carolina, 2 August–11 October 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1743. [Google Scholar] [CrossRef] [PubMed]
- Vander Schaaf, N.A.; Fund, A.J.; Munnich, B.V.; Zastrow, A.L.; Fund, E.E.; Senti, T.L.; Lynn, A.F.; Kane, J.J.; Love, J.L.; Long, G.J. Routine, Cost-Effective SARS-CoV-2 Surveillance Testing Using Pooled Saliva Limits Viral Spread on a Residential College Campus. Microbiol. Spectr. 2021, 9, e01089-21. [Google Scholar] [CrossRef]
- Gillam, T.B.; Cole, J.; Gharbi, K.; Angiolini, E.; Barker, T.; Bickerton, P.; Brabbs, T.; Chin, J.; Coen, E.; Cossey, S. Norwich COVID-19 testing initiative pilot: Evaluating the feasibility of asymptomatic testing on a university campus. J. Public Health 2021, 43, 82–88. [Google Scholar] [CrossRef]
- Blake, H.; Corner, J.; Cirelli, C.; Hassard, J.; Briggs, L.; Daly, J.M.; Bennett, M.; Chappell, J.G.; Fairclough, L.; McClure, C.P. Perceptions and experiences of the University of Nottingham pilot SARS-CoV-2 asymptomatic testing service: A mixed-methods study. Int. J. Environ. Res. Public Health 2021, 18, 188. [Google Scholar] [CrossRef]
- Barry, G.; McCarney, C.; Farrelly, M.; Breathnach, R.; Mooney, C.; More, S.J. Rapid antigen testing for SARS-CoV-2 infection in a university setting in Ireland: Learning from a 6-week pilot study. Public Health Pract. 2022, 3, 100255. [Google Scholar] [CrossRef]
- Blake, H.; Carlisle, S.; Fothergill, L.; Hassard, J.; Favier, A.; Corner, J.; Ball, J.K.; Denning, C. Mixed-methods process evaluation of a residence-based SARS-CoV-2 testing participation pilot on a UK university campus during the COVID-19 pandemic. BMC Public Health 2022, 22, 1470. [Google Scholar] [CrossRef]
- Adams, W.C. Conducting semi-structured interviews. In Handbook of Practical Program Evaluation, 4th ed.; Newcomer, K.E., Harry, H.P., Wholey, J.S., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; pp. 492–505. [Google Scholar] [CrossRef]
- Bourgeault, I.; Dingwall, R.; De Vries, R. The SAGE Handbook of Qualitative Methods in Health Research; SAGE Publications Ltd.: Southend Oaks, CA, USA, 2010. [Google Scholar]
- UK Health Security Agency. COVID-19 Variants Identified in the UK–Latest Updates. Available online: https://www.gov.uk/government/news/covid-19-variants-identified-in-the-uk-latest-updates (accessed on 23 September 2022).
- Jenkins, H.H.; Lopez, A.A.T.; Tarantini, F.S.; Tomlin, H.; Scales, D.; Lee, I.-N.; Wu, S.; Hyde, R.; Lis-Slimak, K.; Byaruhanga, T. Performance evaluation of a non-invasive one-step multiplex RT-qPCR assay for detection of SARS-CoV-2 direct from saliva. Sci. Rep. 2022, 12, 11553. [Google Scholar] [CrossRef]
- Pijuan-Galito, S.; Tarantini, F.S.; Tomlin, H.; Jenkins, H.; Thompson, J.L.; Scales, D.; Stroud, A.; Tellechea Lopez, A.; Hassall, J.; McTernan, P.G. Saliva for COVID-19 testing: Simple but useless or an undervalued resource? Front. Virol. 2021, 29, 778790. [Google Scholar] [CrossRef]
- Tarantini, F.S.; Wu, S.; Jenkins, H.; Tellechea Lopez, A.; Tomlin, H.; Hyde, R.; Lis-Slimak, K.; Thompson, J.L.; Pijuan-Galitó, S.; Scales, D. Direct RT-qPCR Assay for the Detection of SARS-CoV-2 in Saliva Samples. Methods Protoc. 2022, 5, 25. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.L.; Velasco, A.D.R.; Cardall, A.; Tarbox, R.; Richardson, J.; Clarke, G.; Lister, M.; Howson-Wells, H.C.; Fleming, V.M.; Khakh, M. Comparative effects of viral-transport-medium heat inactivation upon downstream SARS-CoV-2 detection in patient samples. J. Med. Microbiol. 2021, 70, 001301. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The use of triangulation in qualitative research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef]
- Matheson, N.J.; Warne, B.; Weekes, M.P.; Maxwell, P.H. Mass testing of university students for COVID-19. BMJ 2021, 375, n2388. [Google Scholar] [CrossRef] [PubMed]
- Schultes, O.; Clarke, V.; Paltiel, A.D.; Cartter, M.; Sosa, L.; Crawford, F.W. COVID-19 Testing and Case Rates and Social Contact Among Residential College Students in Connecticut during the 2020–2021 Academic Year. JAMA Netw. Open 2021, 4, e2140602. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: Mass testing at UK universities is haphazard and unscientific, finds BMJ investigation. BMJ 2021, 372, n848. [Google Scholar] [CrossRef]
- He, H.; Harris, L. The impact of COVID-19 pandemic on corporate social responsibility and marketing philosophy. J. Bus. Res. 2020, 116, 176–182. [Google Scholar] [CrossRef]
- Navickas, V.; Kontautiene, R.; Stravinskienė, J.; Bilan, Y. Paradigm shift in the concept of corporate social responsibility: COVID-19. Green Financ. 2021, 3, 138–152. [Google Scholar] [CrossRef]
- Lourenço, M.L.; Silva, M.R.R.; Oliveira, R.S.G. University social responsibility and empathy in organizations during COVID-19 pandemic in Brazil. Soc. Responsib. J. 2021, 18, 806–824. [Google Scholar] [CrossRef]
- Hu, W.; Zhang, S.; Liu, S. Red Tape and Community Workers’ Proactive Behavior During COVID-19: Applying the Job Demands–Resources Model. Front. Psychol. 2022, 13, 871025. [Google Scholar] [CrossRef] [PubMed]
- Suseno, Y.; Standing, C.; Gengatharen, D.; Nguyen, D. Innovative work behaviour in the public sector: The roles of task characteristics, social support, and proactivity. Aust. J. Pub. Admin. 2020, 79, 41–59. [Google Scholar] [CrossRef]
- Crant, J.M. Proactive behavior in organizations. J. Manag. 2000, 26, 435–462. [Google Scholar] [CrossRef]
- Blake, H.; Somerset, S.; Mahmood, I.; Mahmood, N.; Corner, J.; Ball, J.K.; Denning, C. Workforce experiences of a rapidly established SARS-CoV-2 asymtpomatic testing service in a higher education set-ting: A qualitative study. Int. J. Environ. Res. Public Health 2022, 19, 12464. [Google Scholar] [CrossRef]
- Choi, B.C.; Pang, T.; Lin, V.; Puska, P.; Sherman, G.; Goddard, M.; Ackland, M.J.; Sainsbury, P.; Stachenko, S.; Morrison, H.; et al. Can scientists and policy makers work together? J. Epidemiol. Community Health 2005, 59, 632–637. [Google Scholar] [CrossRef]
- Miskry, A.; Abdullah, A.S.; Hamid, A.A.; Darweesh, A.H.M. The impact of COVID-19 pandemic on university faculty, staff, and students and coping strategies used during the lockdown in the United Arab Emirates. Front. Psychol. 2021, 12, 682757. [Google Scholar] [CrossRef]
- Cairney, P. The UK government’s COVID-19 policy: Assessing evidence-informed policy analysis in real time. Br. Politics 2021, 16, 90–116. [Google Scholar] [CrossRef]
- Brook, C.E.; Northrup, G.R.; Ehrenberg, A.J.; Doudna, J.A.; Boots, M.; Consortium, I.S.-C.-T. Optimizing COVID-19 control with asymptomatic surveillance testing in a university environment. Epidemics 2021, 37, 100527. [Google Scholar] [CrossRef]
- Fleming, C.; Drennan, V.M.; Kerry-Barnard, S.; Reid, F.; Adams, E.J.; Sadiq, S.T.; Phillips, R.; Majewska, W.; Harding-Esch, E.M.; Cousins, E.C. Understanding the acceptability, barriers and facilitators for chlamydia and gonorrhoea screening in technical colleges: Qualitative process evaluation of the “Test n Treat” trial. BMC Public Health 2020, 20, 1212. [Google Scholar]
- Watson, D.; Baralle, N.L.; Alagil, J.; Anil, K.; Ciccognani, S.; Dewar-Haggart, R.; Fearn, S.; Groot, J.; Knowles, K.; Meagher, C. How do we engage people in testing for COVID-19? A rapid qualitative evaluation of a testing programme in schools, GP surgeries and a university. BMC Public Health 2022, 22, 305. [Google Scholar] [CrossRef]
- Alston, M.; Allan, J.; Bell, K.; Brown, A.; Dowling, J.; Hamilton, P.; McKinnon, J.; McKinnon, N.; Mitchell, R.; Whittenbury, K. ‘SERPS Up’: Support, engagement and retention of postgraduate students: A model of postgraduate support. Aust. J. Adult Learn. 2005, 45, 172–190. [Google Scholar]
- Serpas, D.G.; Ignacio, D.A. COVID-19 fear mediates the relationship between perceived risk and preventive behaviors: The moderating role of perceived effectiveness. Psychol. Health 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Schneider, I.K.; Dorrough, A.R.; Frank, C. Ambivalence and self-reported adherence to recommendations to reduce the spread of COVID-19. Soc. Psychol. 2021, 52, 362. [Google Scholar] [CrossRef]
- Mangrum, D.; Niekamp, P. JUE Insight: College student travel contributed to local COVID-19 spread. J. Urban Econ. 2020, 127, 103311. [Google Scholar] [CrossRef]
- Al-Oraibi, A.; Fothergill, L.; Yildirim, M.; Knight, H.; Carlisle, S.; O’Connor, M.; Briggs, L.; Morling, J.R.; Corner, J.; Ball, J.K. Exploring the Psychological Impacts of COVID-19 Social Restrictions on International University Students: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 7631. [Google Scholar] [CrossRef]
- Jones, L.F.; Batteux, E.; Bonfield, S.; Bhogal, J.K.; Taylor, J.; Caiado, C.; Ramagge, J.; Weston, D. Durham University students’ experiences of asymptomatic COVID-19 testing: A qualitative study. BMJ Open 2021, 11, e055644. [Google Scholar] [CrossRef]
- DHSC. New Campaign Urges Public to Get Tested Twice a Week. Available online: https://www.gov.uk/government/news/new-campaign-urges-public-to-get-tested-twice-a-week (accessed on 26 August 2022).
- Dennis, A.; Robin, C.; Carter, H. The social media response to twice-weekly mass asymptomatic testing in England. BMC Public Health 2022, 22, 182. [Google Scholar] [CrossRef] [PubMed]
- Wanat, M.; Logan, M.; Hirst, J.A.; Vicary, C.; Lee, J.J.; Perera, R.; Tracey, I.; Duff, G.; Tufano, P.; Fanshawe, T. Perceptions on undertaking regular asymptomatic self-testing for COVID-19 using lateral flow tests: A qualitative study of university students and staff. BMJ Open 2021, 11, e053850. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blake, H.; Somerset, S.; Mahmood, I.; Mahmood, N.; Corner, J.; Ball, J.K.; Denning, C. A Qualitative Evaluation of the Barriers and Enablers for Implementation of an Asymptomatic SARS-CoV-2 Testing Service at the University of Nottingham: A Multi-Site Higher Education Setting in England. Int. J. Environ. Res. Public Health 2022, 19, 13140. https://doi.org/10.3390/ijerph192013140
Blake H, Somerset S, Mahmood I, Mahmood N, Corner J, Ball JK, Denning C. A Qualitative Evaluation of the Barriers and Enablers for Implementation of an Asymptomatic SARS-CoV-2 Testing Service at the University of Nottingham: A Multi-Site Higher Education Setting in England. International Journal of Environmental Research and Public Health. 2022; 19(20):13140. https://doi.org/10.3390/ijerph192013140
Chicago/Turabian StyleBlake, Holly, Sarah Somerset, Ikra Mahmood, Neelam Mahmood, Jessica Corner, Jonathan K. Ball, and Chris Denning. 2022. "A Qualitative Evaluation of the Barriers and Enablers for Implementation of an Asymptomatic SARS-CoV-2 Testing Service at the University of Nottingham: A Multi-Site Higher Education Setting in England" International Journal of Environmental Research and Public Health 19, no. 20: 13140. https://doi.org/10.3390/ijerph192013140
APA StyleBlake, H., Somerset, S., Mahmood, I., Mahmood, N., Corner, J., Ball, J. K., & Denning, C. (2022). A Qualitative Evaluation of the Barriers and Enablers for Implementation of an Asymptomatic SARS-CoV-2 Testing Service at the University of Nottingham: A Multi-Site Higher Education Setting in England. International Journal of Environmental Research and Public Health, 19(20), 13140. https://doi.org/10.3390/ijerph192013140