
Perceived Disaster Preparedness and Willingness to Respond among Emergency Nurses in South Korea: A Cross-Sectional Study

Abstract
1. Introduction Background
2. Methods
2.1. Design
2.2. Study Participants and Collection
2.3. Instrument
2.3.1. General and Disaster-Related Characteristics
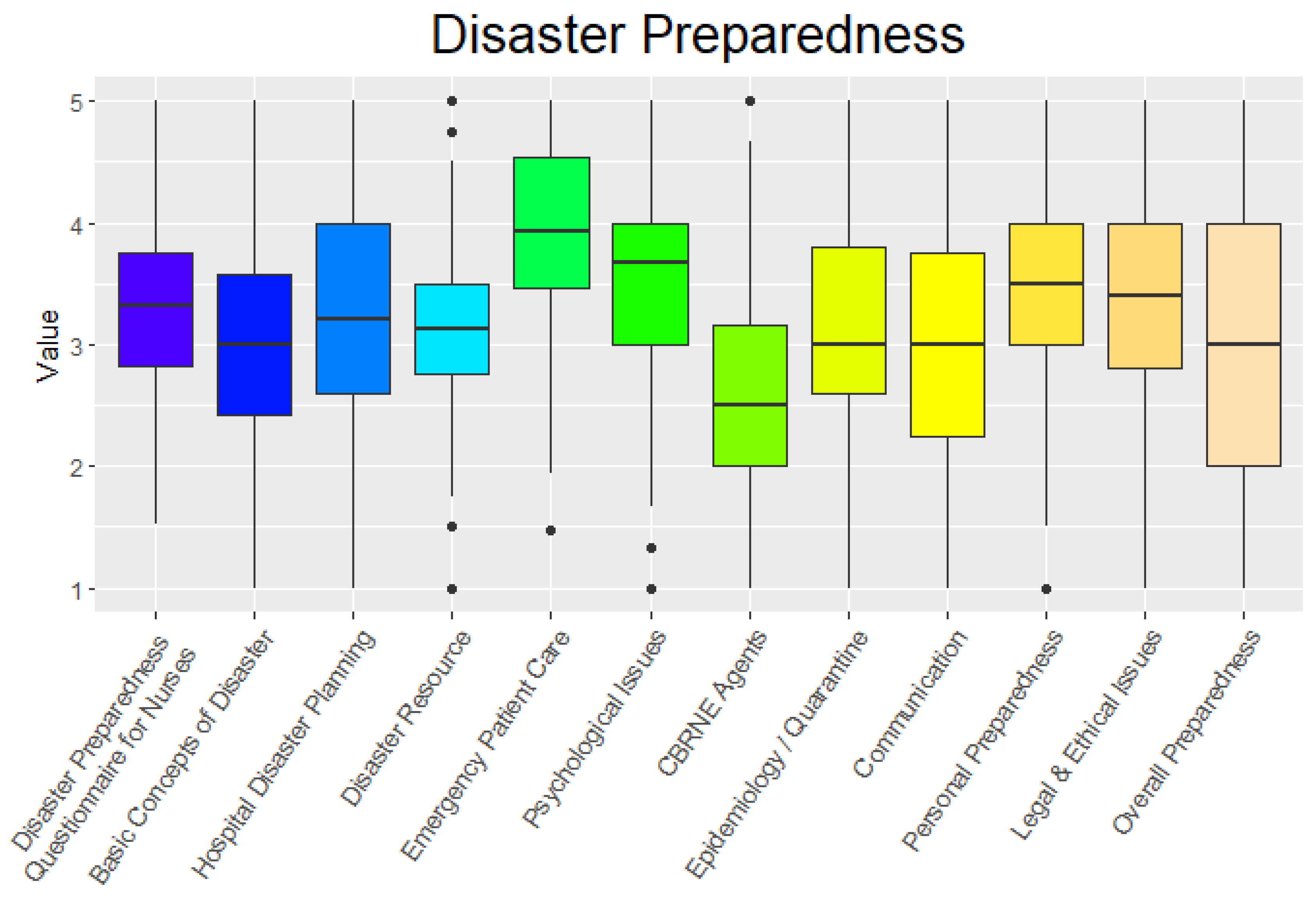
2.3.2. Disaster Preparedness
2.3.3. Willingness to Respond (WTR)
2.4. Data Analysis
3. Results
3.1. Differences in Disaster Preparedness and WTR by Demographic Characteristics
3.2. Differences in Disaster Preparedness and WTR by Disaster-Related Characteristics
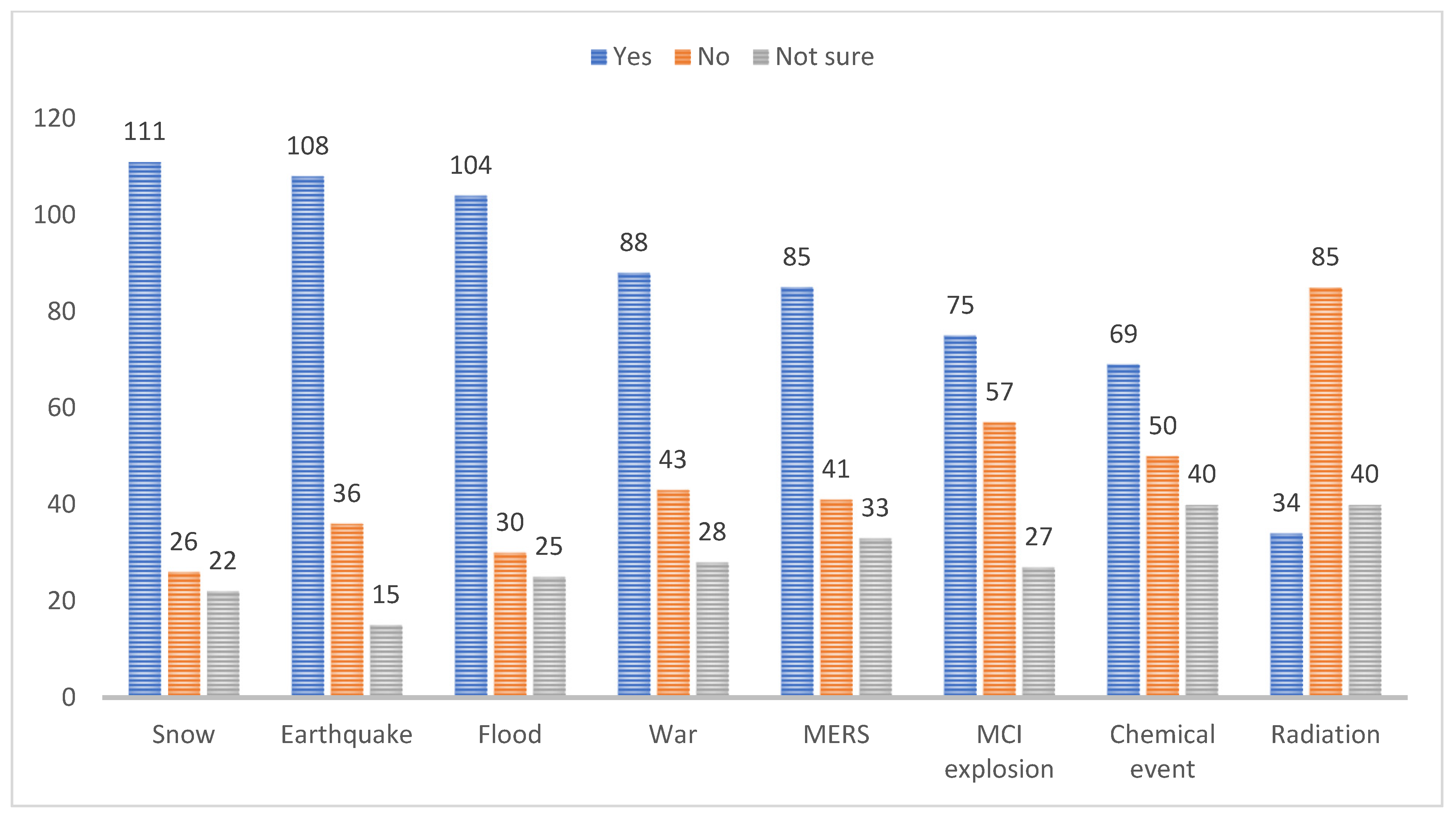
3.3. WTR by Disaster Event
4. Discussion
5. Implications for Emergency Clinical Care
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CRED. C for R on the E of Disasters. Annual Disaster Statistical Review 2017. 2017. Available online: https://www.cred.be/annual-disaster-statistical-review-2017 (accessed on 2 May 2022).
- Ann, E.G.; Keum, K.L.; Choi, S.Y. A Study on the Disaster Preparedness of Nurses in Some Korean Regional Emergency Medical Centers. Korean J. Mil. Nurs. Res. 2011, 29, 94–109. [Google Scholar]
- Said, N.B.; Chiang, V.C.L. The knowledge, skill competencies, and psychological preparedness of nurses for disasters: A systematic review. Int. Emerg. Nurs. 2020, 48, 100806. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.J.; Miller, E.L.; Skaggs, M.K.D. Nursing Self-perceptions of Emergency Preparedness at a Rural Hospital. J. Emerg. Nurs. 2017, 43, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Setyawati, A.D.; Lu, Y.Y.; Liu, C.Y.; Liang, S.Y. Disaster Knowledge, Skills, and Preparedness Among Nurses in Bengkulu, Indonesia: A Descriptive Correlational Survey Study. J. Emerg. Nurs. 2020, 46, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Knezek, E.B.; Vu, T.; Lee, J. Emergency responder willingness to respond during disasters: A literature review. J. Conting. Crisis Manag. 2021, 30, 71–81. [Google Scholar] [CrossRef]
- Kim, J.; Chung, H.S. Disaster medical response system in Korea. J. Korean Med. Assoc. 2019, 62, 252–257. [Google Scholar] [CrossRef]
- Lee, J.Y.; Lee, J.Y.; Lee, S.H.; Kim, J.; Park, H.Y.; Kim, Y.; Kwon, K.T. The experiences of health care workers during the COVID-19 pandemic in Korea: A qualitative study. J. Korean Med. Sci. 2021, 36, e170. [Google Scholar] [CrossRef]
- Shanafelt, T.; Ripp, J.; Trockel, M. Understanding and Addressing Sources of Anxiety Among Health Care Professionals During the COVID-19 Pandemic. J. Am. Med. Assoc. 2020, 323, 2133–2134. [Google Scholar] [CrossRef]
- Sarah, C.; Sharon, K.; Anne-Maree, K. Is COVID-19 the straw that broke the back of the emergency nursing workforce? Emerg. Med. Australas. 2021, 33, 1095–1099. [Google Scholar]
- Kim, E.; Unionized Health Workers to Go on Strike Sept. 2 Amid Prolonged Pandemic. Available online: https://en.yna.co.kr/view/AEN20210827006800320 (accessed on 27 August 2021).
- Welfare SKM of H and Emergency Medical Emergency Response Manual. 2016. Available online: http://www.mohw.go.kr/upload/viewer/skin/doc.html?fn=1452774726313_20160114213207.pdf&rs=/upload/viewer/result/202205/ (accessed on 1 August 2022).
- Baack, S.; Alfred, D. Nurses’ Preparedness and Perceived Competence in Managing Disasters: Nurses’ Perceived Competence in Disasters. J. Nurs. Sch. 2013, 45, 281–287. [Google Scholar] [CrossRef]
- Fung, O.W.M.; Loke, A.Y.; Lai, C.K.Y. Disaster preparedness among Hong Kong nurses. J. Adv. Nurs. 2008, 62, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Ghavami, V.; Saghi, F.K.; Asghari, A.; Shabanikiya, H. Predictors of nurses’ reporting for work at the time of epidemics and natural disasters; solutions for hospital surge capacity. J. Nurs. Sch. 2021, 54, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Arbon, P.; Ranse, J.; Cusack, L.; Considine, J.; Shaban, R.Z.; Woodman, R.J.; Bahnisch, L.; Kako, M.; Hammad, K.; Mitchell, B. Australasian emergency nurses’ willingness to attend work in a disaster: A survey. Australas. Emerg. Nurs. J. 2013, 16, 52–57. [Google Scholar] [CrossRef]
- Ogedegbe, C.; Nyirenda, T.; DelMoro, G.; Yamin, E.; Feldman, J. Health care workers and disaster preparedness: Barriers to and facilitators of willingness to respond. Int. J. Emerg. Med. 2012, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Almukhlifi, Y.; Crowfoot, G.; Wilson, A.; Hutton, A. Emergency healthcare workers’ preparedness for disaster management: An integrative review. J. Clin. Nurs. 2021, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Balicer, R.D.; Catlett, C.L.; Barnett, D.J.; Thompson, C.B.; Hsu, E.B.; Morton, M.J.; Semon, N.L.; Watson, C.M.; Gwon, H.S.; Links, J.M. Characterizing Hospital Workers’ Willingness to Respond to a Radiological Event. PLoS ONE 2011, 6, e25327. [Google Scholar] [CrossRef]
- Rajesh, G.; Pai, M.B.H.; Shenoy, R.; Priya, H. Willingness to Participate in Disaster Management Among Indian Dental Graduates. Prehospital Disaster Med. 2012, 27, 439–444. [Google Scholar] [CrossRef]
- Burke, R.V.; Goodhue, C.J.; Chokshi, N.K.; Upperman, J.S. Factors Associated with Willingness to Respond to a Disaster: A Study of Healthcare Workers in a Tertiary Setting. Prehospital Disaster Med. 2011, 26, 244–250. [Google Scholar] [CrossRef]
- Qureshi, K.; Gershon, R.R.M.; Sherman, M.F.; Straub, M.T.; Gebbie, E.; Mccollum, M.; Erwin, M.M.J.; Morse, S.S. Health Care Workers’ Ability and Willingness to Report to Duty During Catastrophic Disasters. J. Urban Health 2005, 82, 378–388. [Google Scholar] [CrossRef]
- Lee, Y.R.; Lee, M.H. A Study on Disaster Preparedness Competency in Public Health Center Workers. J. Korean Acad. Soc. Nurs. Educ. 2016, 22, 96–109. [Google Scholar] [CrossRef]
- Jung, E.Y.; Kim, H.; Joe, S.Y. Current State of Disaster Education in Undergraduate Nursing Programs in South Korea. Korean J. Mil. Nurs. Res. 2018, 36, 106–119. [Google Scholar] [CrossRef]
- Nafar, H.; Aghdam, E.T.; Derakhshani, N.; Sani’Ee, N.; Sharifian, S.; Goharinezhad, S. A systematic mapping review of factors associated with willingness to work under emergency condition. Hum. Resour. Health 2021, 19, 76. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.S.; Lee, J.E. Hospital Nurses’ Willingness to Respond in a Disaster. J. Nurs. Adm. 2021, 51, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J.; Yboa, B.C.; McEnroe-Petitte, D.M.; Lobrino, L.R.; Brennan, M.G.B. Disaster Preparedness in Philippine Nurses. J. Nurs. Sch. 2016, 48, 98–105. [Google Scholar] [CrossRef]
- Baker, O.G. Preparedness assessment for managing disasters among nurses in an international setting: Implications for nurses. Int. Emerg. Nurs. 2021, 56, 100993. [Google Scholar] [CrossRef]
- Goodhue, C.J.; Burke, R.V.; Ferrer, R.R.; Chokshi, N.K.; Dorey, F.; Upperman, J.S. Willingness to Respond in a Disaster: A Pediatric Nurse Practitioner National Survey. J. Pediatr. Health Care 2012, 26, e7–e20. [Google Scholar] [CrossRef]
- Turner, J.A.; Rebmann, T.; Loux, T.M.; Charney, R.L. Willingness to Respond to Radiological Disasters Among First Responders in St. Louis, Missouri. Health Secur. 2020, 18, 318–328. [Google Scholar] [CrossRef]
- Lee, J.Y.; Hong, J.H.; Park, E.Y. Beyond the fear: Nurses’ experiences caring for patients with Middle East respiratory syndrome: A phenomenological study. J. Clin. Nurs. 2020, 29, 3349–3362. [Google Scholar] [CrossRef]
- Kim, Y. Nurses’ experiences of care for patients with Middle East respiratory syndrome-coronavirus in South Korea. Am. J. Infect. Control 2018, 46, 781–787. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Categories | n | % | DPQ-N | t/F(p) | WTR | t/F(p) | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||||
| Gender | Female | 130 | 82.3 | 3.30 | 0.69 | 1.32(0.19) | 4.28 | 2.64 | 0.11(0.911) |
| Male | 28 | 17.7 | 3.49 | 0.81 | 4.21 | 3.02 | |||
| Age | 29.27 (5.37) † | 3.33 | 0.71 | 4.27 | 2.70 | ||||
| Educational status | 3-year College graduate | 25 | 15.8 | 3.64 | 0.58 | 4.09(0.018) | 4.4 | 3.27 | 0.20(0.817) |
| Bachelor’s | 111 | 70.3 | 3.23 | 0.72 | 4.18 | 2.59 | |||
| Master’s or higher | 22 | 13.9 | 3.49 | 0.75 | 4.55 | 2.61 | |||
| Religion | Yes | 56 | 35.4 | 3.41 | 0.75 | 1.01(0.315) | 4.57 | 2.78 | 1.06(.293) |
| No | 102 | 64.6 | 3.29 | 0.70 | 4.10 | 2.65 | |||
| Marital status | Married | 43 | 27.2 | 3.55 | 0.67 | 2.42(0.017) | 3.91 | 2.92 | −1.02(0.308) |
| Single | 115 | 72.8 | 3.25 | 0.71 | 4.4 | 2.61 | |||
| Children | Yes | 25 | 15.8 | 3.67 | 0.61 | 2.64(0.009) | 3.84 | 3.00 | −0.86(0.391) |
| No | 133 | 84.2 | 3.27 | 0.72 | 4.35 | 2.64 | |||
| Dependents | Yes | 61 | 38.6 | 3.46 | 0.79 | 1.79(0.076) | 4.62 | 2.68 | 1.32(0.188) |
| (Excluding children) | No | 97 | 61.4 | 3.25 | 0.66 | 4.04 | 2.70 | ||
| Pets | Yes | 35 | 22.2 | 3.14 | 0.58 | −1.76(0.079) | 4.46 | 2.65 | 0.47(0.636) |
| No | 123 | 77.8 | 3.28 | 0.74 | 4.21 | 2.72 | |||
| Support system | Yes | 83 | 52.5 | 3.34 | 0.68 | 0.18(0.858) | 4.45 | 2.53 | 0.88(0.379) |
| No | 75 | 47.5 | 3.32 | 0.75 | 4.07 | 2.87 | |||
| Perceived health problems | Yes | 7 | 4.4 | 3.62 | 0.97 | 0.18(0.858) | 5.29 | 2.29 | 1.02(0.308) |
| No | 151 | 95.6 | 3.32 | 0.70 | 4.22 | 2.71 | |||
| Clinical experience (year) | Short (<5) | 80 | 50.6 | 3.20 | 0.69 | −2.43(0.016) | 4.36 | 2.63 | 0.45(0.650) |
| Long (>5) | 78 | 49.4 | 3.47 | 0.71 | 4.17 | 2.78 | |||
| Emergency Department (years) | Short (<5) | 85 | 53.8 | 3.24 | 0.70 | −1.83(0.069) | 4.32 | 2.63 | 0.26(0.795) |
| Long (>5) | 73 | 46.2 | 3.44 | 0.72 | 4.21 | 2.79 | |||
| Current position | Staff nurse | 122 | 77.2 | 3.28 | 0.73 | −1.61(0.109) | 4.26 | 2.65 | −0.03(0.976) |
| Charge/Head nurse | 36 | 22.8 | 3.50 | 0.65 | 4.28 | 2.89 | |||
| Characteristics | Categories | n | % | DPQ-N | t/F(p) | WTR | t/F(p) | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||||
| Personal disaster experience (victim or witness) | Yes | 40 | 25.3 | 3.68 | 0.75 | 3.65(<0.001) | 4.58 | 2.56 | 0.84(0.403) |
| No | 118 | 74.7 | 3.22 | 0.67 | 4.16 | 2.75 | |||
| Disaster experience in a disaster scene as a professional | Yes | 21 | 13.3 | 3.83 | 0.68 | 3.58(<0.001) | 5.57 | 2.48 | 2.42(0.017) |
| No | 137 | 86.7 | 3.25 | 0.69 | 4.07 | 2.68 | |||
| KDMAT | Yes | 49 | 31.0 | 3.81 | 0.63 | 6.26(<0.001) | 5.02 | 2.54 | 2.39(0.018) |
| No | 109 | 69.0 | 3.12 | 0.65 | 3.93 | 2.71 | |||
| Disaster training within a year | Yes | 91 | 57.6 | 3.59 | 0.62 | 5.84(<0.001) | 4.76 | 2.71 | 2.73(0.007) |
| No | 67 | 42.4 | 2.98 | 0.69 | 3.60 | 2.55 | |||
| Safety concerns during a disaster | Self | 49 | 31.0 | 3.22 | 0.80 | 0.53(0.586) | 4.31 | 2.67 | 0.64(0.531) |
| Family | 135 | 85.4 | 3.34 | 0.69 | 4.26 | 2.73 | |||
| No concern | 9 | 5.7 | 3.38 | 0.61 | 3.22 | 3.19 | |||
| Available resources during disaster | Yes | 33 | 20.9 | 3.55 | 0.67 | 2.10(0.126) | 4.12 | 2.61 | 0.67(0.513) |
| No | 83 | 52.5 | 3.26 | 0.75 | 4.49 | 2.76 | |||
| Not sure | 42 | 26.6 | 3.30 | 0.65 | 3.93 | 2.67 | |||
| Compensation for disaster participation | Yes | 31 | 19.6 | 3.51 | 0.71 | 2.13(0.122) | 4.19 | 2.89 | 0.26(0.772) |
| No | 80 | 50.6 | 3.22 | 0.70 | 4.41 | 2.64 | |||
| Not sure | 47 | 29.7 | 3.40 | 0.72 | 4.06 | 2.71 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, W.-S.; Hyun, S.Y.; Oh, H. Perceived Disaster Preparedness and Willingness to Respond among Emergency Nurses in South Korea: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 11812. https://doi.org/10.3390/ijerph191811812
Choi W-S, Hyun SY, Oh H. Perceived Disaster Preparedness and Willingness to Respond among Emergency Nurses in South Korea: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11812. https://doi.org/10.3390/ijerph191811812
Chicago/Turabian StyleChoi, Won-Seok, Sung Youl Hyun, and Hyunjin Oh. 2022. "Perceived Disaster Preparedness and Willingness to Respond among Emergency Nurses in South Korea: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 18: 11812. https://doi.org/10.3390/ijerph191811812
APA StyleChoi, W.-S., Hyun, S. Y., & Oh, H. (2022). Perceived Disaster Preparedness and Willingness to Respond among Emergency Nurses in South Korea: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(18), 11812. https://doi.org/10.3390/ijerph191811812