
The Current Prevalence of Underweight, Overweight, and Obesity Associated with Demographic Factors among Pakistan School-Aged Children and Adolescents—An Empirical Cross-Sectional Study

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Participants
2.2. Measurements
2.3. Weight Status
2.4. Demographic Factors
2.5. Statistical Analysis
3. Results
3.1. Study Participants
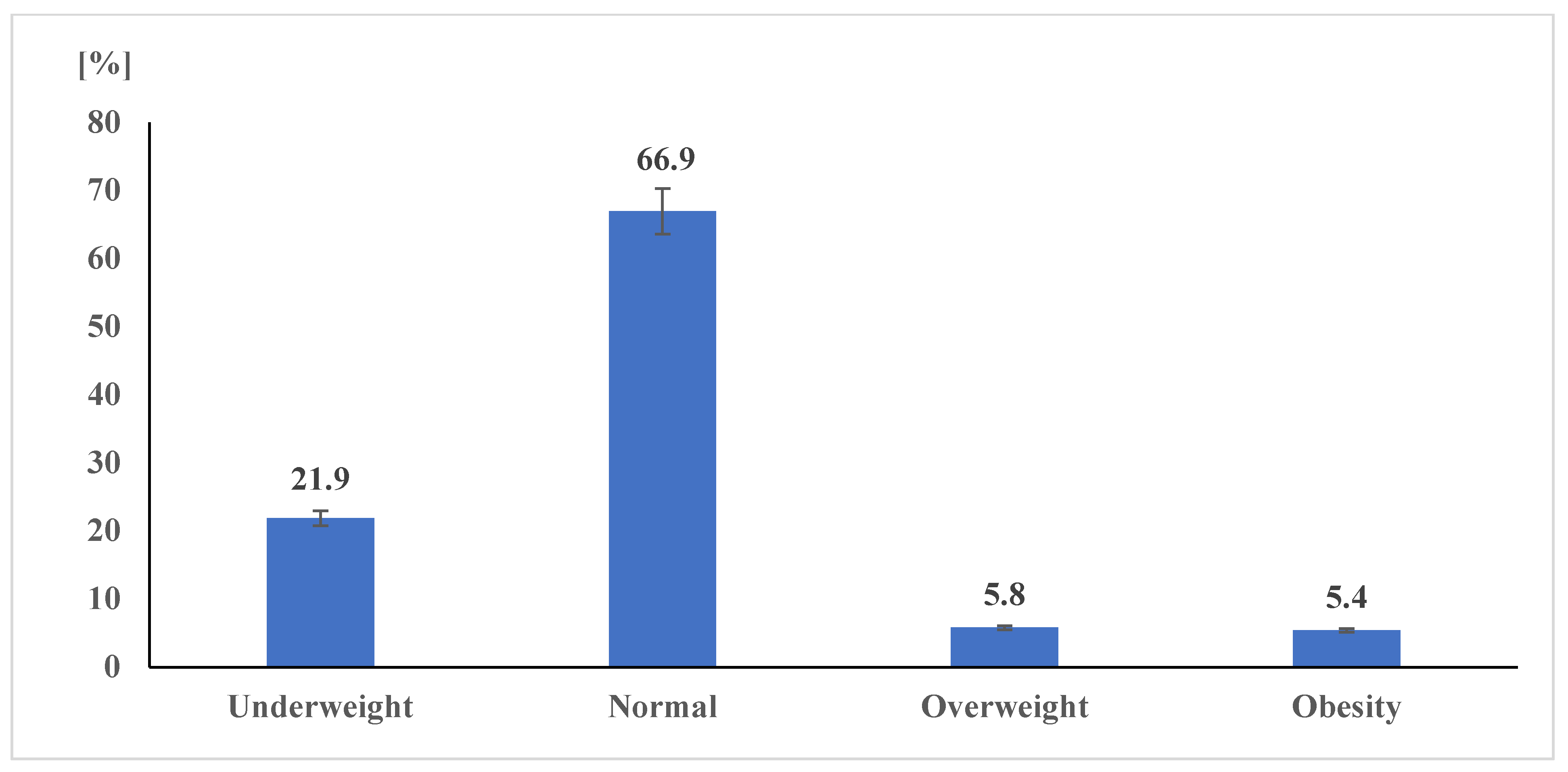
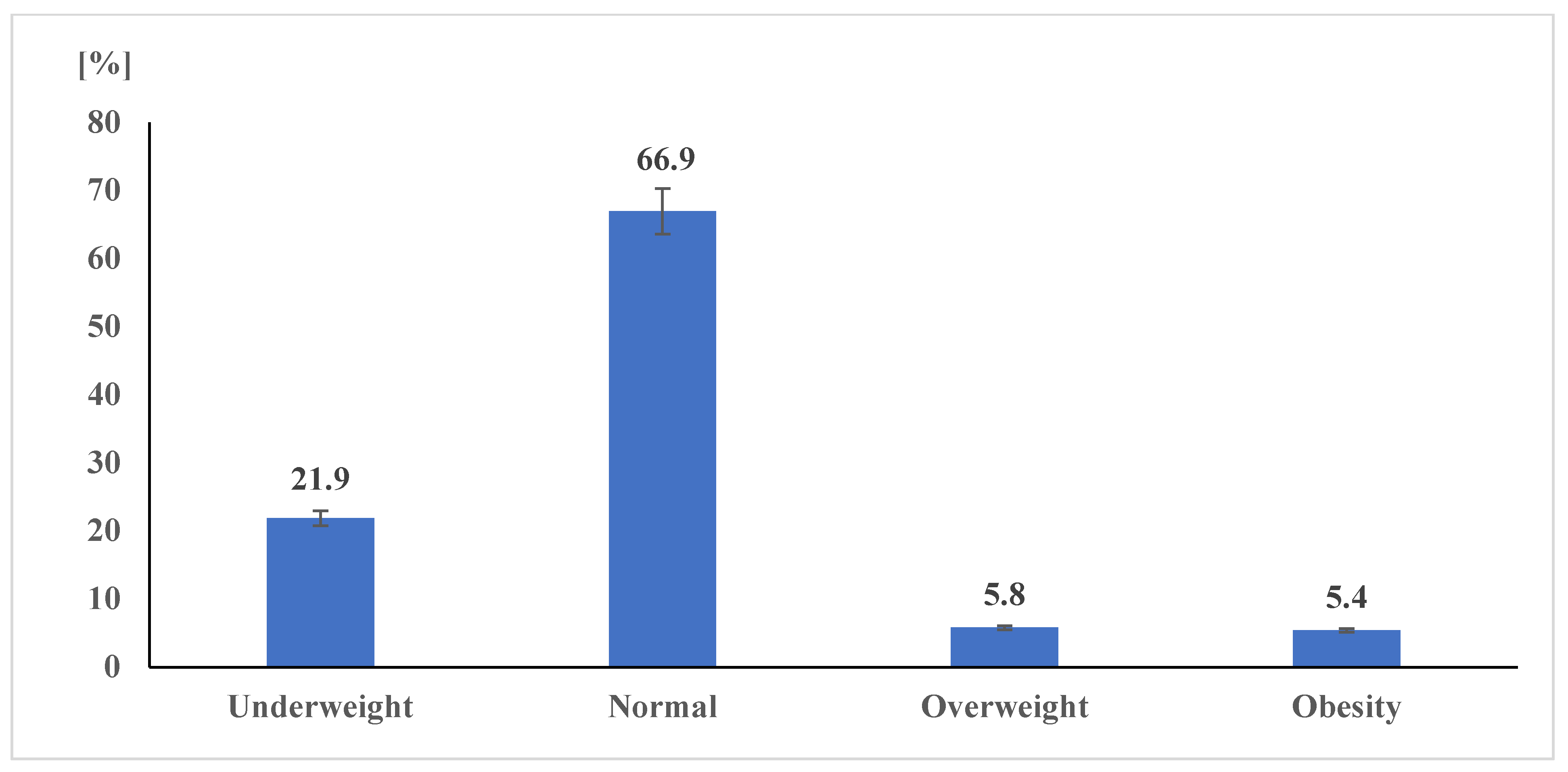
3.2. Prevalence of Body Weight Status
3.3. Correlation of Demographic Parameters with Body Weight Status
3.4. Differences in Body Weight Outcomes Due to Demographic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skjåkødegård, H.F.; Danielsen, Y.S.; Frisk, B.; Hystad, S.W.; Roelants, M.; Pallesen, S.; Conlon, R.P.K.; Wilfley, D.E.; Juliusson, P.B. Beyond sleep duration: Sleep timing as a risk factor for childhood obesity. Pediatric Obes. 2021, 16, e12698. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Zhu, X.; Wu, X. Overweight, obesity, and screen-time viewing among Chinese school-aged children: National prevalence estimates from the 2016 Physical Activity and Fitness in China—The Youth Study. J. Sport Health Sci. 2017, 6, 404–409. [Google Scholar] [CrossRef]
- Zhu, Z.; Yang, Y.; Kong, Z.; Zhang, Y.; Zhuang, J. Prevalence of physical fitness in Chinese school-aged children: Findings from the 2016 Physical Activity and Fitness in China—The Youth Study. J. Sport Health Sci. 2017, 6, 395–403. [Google Scholar] [CrossRef] [PubMed]
- World Obesity Federation. Global Obesity Observatory. Available online: https://data.worldobesity.org/ (accessed on 10 July 2022).
- Haththotuwa, R.N.; Wijeyaratne, C.N.; Senarath, U. Worldwide epidemic of obesity. In Obesity and Obstetrics, 2nd ed.; Mahmood, T.A., Ed.; Elsevier: San Diego, CA, USA, 2020; pp. 3–8. ISBN 9780128179215. [Google Scholar]
- Williams, A.S.; Ge, B.; Petroski, G.; Kruse, R.L.; McElroy, J.A.; Koopman, R.J. Socioeconomic Status and Other Factors Associated with Childhood Obesity. J. Am. Board Fam. Med. 2018, 31, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Gray, J.C.; Schvey, N.A.; Tanofsky-Kraff, M. Demographic, psychological, behavioral, and cognitive correlates of BMI in youth: Findings from the Adolescent Brain Cognitive Development (ABCD) study. Psychol. Med. 2020, 50, 1539–1547. [Google Scholar] [CrossRef]
- Pelusi, C.; Altieri, P.; Gambineri, A.; Repaci, A.; Cavazza, C.; Fanelli, F.; Morselli-Labate, A.M.; Pagotto, U.; Pasquali, R. Behavioral, socio-environmental, educational and demographic correlates of excess body weight in Italian adolescents and young adults. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 279–289. [Google Scholar] [CrossRef]
- Piché, M.-E.; Tchernof, A.; Després, J.-P. Obesity Phenotypes, Diabetes, and Cardiovascular Diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Osadnik, K.; Lejawa, M.; Osadnik, T.; Goławski, M.; Lewandowski, P.; Pawlas, N. “Obesity and Insulin Resistance” Is the Component of the Metabolic Syndrome Most Strongly Associated with Oxidative Stress. Antioxidants 2021, 11, 79. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Cieślar, G.; Stanek, A. Nitrotyrosine, Nitrated Lipoproteins, and Cardiovascular Dysfunction in Patients with Type 2 Diabetes: What Do We Know and What Remains to Be Explained? Antioxidants 2022, 11, 856. [Google Scholar] [CrossRef]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [Green Version]
- Mushtaq, M.U.; Gull, S.; Abdullah, H.M.; Shahid, U.; Shad, M.A.; Akram, J. Prevalence and socioeconomic correlates of overweight and obesity among Pakistani primary school children. BMC Public Health 2011, 11, 724. [Google Scholar] [CrossRef]
- Prentice, A.M. The emerging epidemic of obesity in developing countries. Int. J. Epidemiol. 2006, 35, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Kilic, E.; Özer, Ö.F.; Erek Toprak, A.; Erman, H.; Torun, E.; Kesgin Ayhan, S.; Caglar, H.G.; Selek, S.; Kocyigit, A. Oxidative Stress Status in Childhood Obesity: A Potential Risk Predictor. Med. Sci. Monit. 2016, 22, 3673–3679. [Google Scholar] [CrossRef]
- Danquah, F.I.; Ansu-Mensah, M.; Bawontuo, V.; Yeboah, M.; Udoh, R.H.; Tahiru, M.; Kuupiel, D. Risk factors and morbidities associated with childhood obesity in sub-Saharan Africa: A systematic scoping review. BMC Nutr. 2020, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 July 2022).
- Neuman, M.; Kawachi, I.; Gortmaker, S.; Subramanian, S.V. Urban-rural differences in BMI in low- and middle-income countries: The role of socioeconomic status. Am. J. Clin. Nutr. 2013, 97, 428–436. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration. Rising rural body-mass index is the main driver of the global obesity epidemic in adults. Nature 2019, 569, 260–264. [Google Scholar] [CrossRef]
- Aiyar, A.; Rahman, A.; Pingali, P.L. India’s rural transformation and rising obesity burden. World Dev. 2021, 138, 105258. [Google Scholar] [CrossRef]
- Al-Saeed, W.Y.; Al-Dawood, K.M.; Bukhari, I.A.; Bahnassy, A. Prevalence and socioeconomic risk factors of obesity among urban female students in Al-Khobar city, Eastern Saudi Arabia, 2003. Obes. Rev. 2007, 8, 93–99. [Google Scholar] [CrossRef]
- Ford, N.D.; Patel, S.A.; Narayan, K.V. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health 2017, 38, 145–164. [Google Scholar] [CrossRef]
- Global Hunger Index. Global Hunger Index Scores by 2021 Ghi Rank. Available online: https://www.globalhungerindex.org/ (accessed on 9 July 2022).
- World Obesity Federation. Global Atlas on Childhood Obesity; World Obesity Federation: London, UK, 2019. [Google Scholar]
- Duan, J.; Hu, H.; Wang, G.; Arao, T. Study on Current Levels of Physical Activity and Sedentary Behavior among Middle School Students in Beijing, China. PLoS ONE 2015, 10, e0133544. [Google Scholar] [CrossRef]
- Lazzeri, G.; Azzolini, E.; Pammolli, A.; de Wet, D.R.; Giacchi, M.V. Correlation between physical activity and sedentary behavior with healthy and unhealthy behaviors in Italy and Tuscan region: A cross sectional study. J. Prev. Med. Hyg. 2013, 54, 41–48. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of Overweight and Obesity in the United States, 1999–2004. JAMA 2006, 295, 1549. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.M.; Hill, W.D.; Anderson, E.L.; Sanderson, E.; Deary, I.J.; Davey Smith, G. Multivariable two-sample Mendelian randomization estimates of the effects of intelligence and education on health. Elife 2019, 8, e43990. [Google Scholar] [CrossRef]
- Ickovics, J.R.; Duffany, K.O.; Shebl, F.M.; Peters, S.M.; Read, M.A.; Gilstad-Hayden, K.R.; Schwartz, M.B. Implementing School-Based Policies to Prevent Obesity: Cluster Randomized Trial. Am. J. Prev. Med. 2019, 56, e1–e11. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, F.K.; Moura dos Santos, M.A.; Almeida, M.B.; Nobre, I.G.; Nobre, G.G.; Ferreira e Silva, W.T.; Gomes, T.N.; António Ribeiro Maia, J.; Leandro, C.G. Biological and behavioral correlates of body weight status among rural Northeast Brazilian schoolchildren. Am. J. Hum. Biol 2018, 30, e23096. [Google Scholar] [CrossRef] [PubMed]
- Dutta, K.; Mukherjee, R.; Das, R.; Chowdhury, A.; Sen, D.; Sahu, S. Scheduled optimal sleep duration and screen exposure time promotes cognitive performance and healthy BMI: A study among rural school children of India. Biol. Rhythm Res. 2021, 52, 1501–1513. [Google Scholar] [CrossRef]
- Eid Al Agha, A. Effect of the Family Food Environment and Dietary Behaviors on Obese Children and Adolescents. J. Diabetes Metab. 2016, 7, 661. [Google Scholar] [CrossRef]
- Charilaou, M.; Karekla, M.; Constantinou, M.; Price, S. Relationship between physical activity and type of smoking behavior among adolescents and young adults in Cyprus. Nicotine Tob. Res. 2009, 11, 969–976. [Google Scholar] [CrossRef]
- Czyż, S.; Toriola, A.; Starościak, W.; Lewandowski, M.; Paul, Y.; Oyeyemi, A. Physical Fitness, Physical Activity, Sedentary Behavior, or Diet—What Are the Correlates of Obesity in Polish School Children? Int. J. Environ. Res. Public Health 2017, 14, 664. [Google Scholar] [CrossRef]
- Mansoori, N.; Nisar, N.; Shahid, N.; Mubeen, S.M.; Ahsan, S. Prevalence of obesity and its risk factors among school children in Karachi, Pakistan. Trop. Dr. 2018, 48, 266–269. [Google Scholar] [CrossRef]
- Lu, S.; Cheval, B.; Yu, Q.; Hossain, M.M.; Chen, S.-T.; Taylor, A.; Bao, R.; Doig, S.; Li, J.; Wang, T.; et al. Associations of 24-Hour Movement Behavior with Depressive Symptoms and Anxiety in Children: Cross-Sectional Findings from a Chinese Sample. Healthcare 2021, 9, 1532. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, S.; Duncan, M.J.; Badland, H.; Oliver, M.; Curtis, C. Associations of children’s independent mobility and active travel with physical activity, sedentary behaviour and weight status: A systematic review. J. Sci. Med. Sport 2013, 16, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Keykhaei, F.; Shahraki, M.; Sargolhosseinzadeh, E.; Shahraki, T.; Dashipour, A. Correlation of Body Mass Index and Physical Activity Among 7- to 11-Year Children at Zahedan, Iran. Food Nutr. Bull. 2016, 37, 364–374. [Google Scholar] [CrossRef] [PubMed]
- CDC Global School-Based Student Health Survey. Pakistan GSHS Questionnaire. Available online: https://www.cdc.gov/gshs/ (accessed on 9 July 2022).
- Chen, S.-T.; Liu, Y.; Tremblay, M.S.; Hong, J.-T.; Tang, Y.; Cao, Z.-B.; Zhuang, J.; Zhu, Z.; Wu, X.; Wang, L.; et al. Meeting 24-h movement guidelines: Prevalence, correlates, and the relationships with overweight and obesity among Chinese children and adolescents. J. Sport Health Sci. 2021, 10, 349–359. [Google Scholar] [CrossRef]
- Ahmed, J.; Laghari, A.; Naseer, M.; Mehraj, V. Prevalence of and factors associated with obesity among Pakistani schoolchildren: A school-based, cross-sectional study. East. Mediterr. Health J. 2013, 19, 242–247. [Google Scholar] [CrossRef]
- National Center for Health Statistics. Growth Charts—Clinical Growth Charts. Available online: https://www.cdc.gov/growthcharts/clinical_charts.htm (accessed on 9 July 2022).
- Syahrul, S.; Kimura, R.; Tsuda, A.; Susanto, T.; Saito, R.; Ahmad, F. Prevalence of underweight and overweight among school-aged children and it’s association with children’s sociodemographic and lifestyle in Indonesia. Int. J. Nurs. Sci. 2016, 3, 169–177. [Google Scholar] [CrossRef]
- Tanveer, M.; Roy, N.; Zeba, A.; Haider, S.; Albarha, N.S.; Tanveer, N.; Ali, M.; Tanveer, U. Prevalence of Body Mass Index and Associated with Demographic Factors among Pakistan School-Aged Adolescents. Pak. J. Med. Health Sci. 2022, 16, 212–215. [Google Scholar] [CrossRef]
- Siener, M.; Faber, I.; Hohmann, A. Prognostic Validity of Statistical Prediction Methods Used for Talent Identification in Youth Tennis Players Based on Motor Abilities. Appl. Sci. 2021, 11, 7051. [Google Scholar] [CrossRef]
- Khan, S.; Abbas, A.; Ali, I.; Arshad, R.; Tareen, M.; Shah, M.I. Prevalence of overweight and obesity and lifestyle assessment among school–going children of Multan, Pakistan. Isra Med. J. 2019, 11, 230–233. [Google Scholar]
- Mushtaq, M.U.; Gull, S.; Mushtaq, K.; Abdullah, H.M.; Khurshid, U.; Shahid, U.; Shad, M.A.; Akram, J. Height, weight and BMI percentiles and nutritional status relative to the international growth references among Pakistani school-aged children. BMC Pediatr. 2012, 12, 31. [Google Scholar] [CrossRef]
- Anwar, A.; Anwar, F.; Joiya, H.U.; Ijaz, A.; Rashid, H.; Javaid, A.; Mehmood, M. Prevalence of obesity among the school-going children of Lahore and associated factors. J. Ayub Med. Coll. Abbottabad 2010, 22, 27–32. [Google Scholar]
- Ames, M.E.; Holfeld, B.; Leadbeater, B.J. Sex and age group differences in the associations between sleep duration and BMI from adolescence to young adulthood. Psychol. Health 2016, 31, 976–992. [Google Scholar] [CrossRef]
- Nayak, B.; Vinodbhat, H. Prevalence of Overweight/Obesity among School Children In Karnataka, South India. Int. J. Public Health Res. 2022, 35, 180–184. [Google Scholar]
- Saha, M.; Adhikary, D.K.; Parvin, I.; Sharma, Y.R.; Akhter, F.; Majumder, M. Obesity and Its Risk Factors of among School Children in Sylhet, Bangladesh. J. Nepal Health Res. Counc. 2018, 16, 205–208. [Google Scholar] [CrossRef]
- Adom, T.; de Villiers, A.; Puoane, T.; Kengne, A.P. Prevalence and correlates of overweight and obesity among school children in an urban district in Ghana. BMC Obes. 2019, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Mahtabuddin; Shaik, A.; Afroze, M.K.; Garg, R. A comparison study on the prevalence of obesity and its associated factors among school Children. Int. J. Health Clin. Res. 2021, 4, 21–24. [Google Scholar]
- Ashtekar, S.; Mantri, S.; Wadagale, A. Prevalence and Epidemiology of Overweight and Obesity among Upper Primary School Children in Latur City. MedPulse—Int. Med. J. 2014, 1, 15–19. [Google Scholar]
- Bacardi-Gascón, M.; Jiménez-Cruz, A.; Jones, E.; Velasquez Perez, I.; Loaiza Martinez, J.A. Trends of Overweight and Obesity Among Children in Tijuana, Mexico. Ecol. Food Nutr. 2009, 48, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Narančić, N.; Živičnjak, M.; Škarić-Jurić, T.; Bišof, V.; Barbalic, M.; Rudan, P. Overweight and obesity among children and adolescents in Zagreb Croatia. In Auxology; Savaria University Press: Szombathely, Hungary, 2015; pp. 89–95. ISBN 963-9438-48-0. [Google Scholar]
- Ali, K.; Sadaf, A.; Kousar, S.; Habib, Z. Standard of Physical Education in Pakistan as Compare to U.S.A. Glob. J. Hum.-Soc. Sci. Res. 2014, 7, 8–13. [Google Scholar]

{kind=link}
| Variable | Primary School | Middle School | Secondary School | Higher Secondary School |
|---|---|---|---|---|
| Sample size, n (%) | 797 (22.4) | 1368 (38.5) | 954 (26.9) | 432 (12.2) |
| Age (year; mean ± SD) | 10.90 ± 1.23 | 13.13 ± 1.36 | 15.29 ± 1.11 | 16.81 ± 0.44 |
| Sex, n (%) | ||||
| Boys | 434 (54.5) | 704 (51.5) | 558 (58.5) | 235 (54.5) |
| Girls | 363 (45.5) | 664 (48.5) | 396 (41.5) | 197 (45.6) |
| Age category, n (%) | ||||
| Children 9–11 years | 567 (71.1) | 151 (11.0) | 1 (0.1) | 0 (0) |
| Adolescents 12–17 years | 230 (28.9) | 1217 (89.2) | 953 (99.9) | 432 (100) |
| Religion, n (%) | ||||
| Muslims | 756 (94.9) | 1316 (96.2) | 921 (96.5) | 426 (98.6) |
| Non-Muslims | 41 (5.1) | 52 (3.8) | 33 (3.5) | 6 (1.4) |
| Residence, n (%) | ||||
| Urban | 616 (77.3) | 658 (48.1) | 493 (51.7) | 155 (35.9) |
| Rural | 181 (22.7) | 710 (51.9) | 461 (48.3) | 277 (64.1) |
| School type, n (%) | ||||
| Public | 606 (76.0) | 986 (72.1) | 665 (69.7) | 421 (97.5) |
| Private | 191 (24.0) | 382 (27.9) | 289 (30.3) | 11 (2.5) |
| BMI (mean ± SD) | 15.96 ± 2.52 | 17.88 ± 3.36 | 19.57 ± 3.87 | 20.40 ± 3.53 |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|---|
| 1 | Body weight status | — | ||||||
| 2 | Sex | 0.093 ** | — | |||||
| 3 | Age | 0.066 ** | −0.071 ** | — | ||||
| 4 | Religion | −0.014 | −0.004 | −0.012 | — | |||
| 5 | Residence | −0.004 | −0.046 ** | 0.174 ** | 0.040 * | — | ||
| 6 | School Type | 0.054 ** | −0.008 | −0.129 ** | 0.026 | −0.098 ** | — | |
| 7 | School Level | 0.110 ** | −0.026 | 0.855 ** | −0.051 ** | 0.216 ** | −0.072 ** | — |
| Body Mass Index | ||||||
|---|---|---|---|---|---|---|
| Underweight | Normal Weight | Overweight | Obesity n (%) | |||
| Variables | n (%) | n (%) | n (%) | χ2 | p-Value | |
| Sex | ||||||
| Boys | 490 (25.4) | 1250 (64.7) | 102 (5.3) | 89 (4.6) | 32.71 | 0.001 |
| Girls | 288 (17.8) | 1127 (69.6) | 103 (6.4) | 102 (6.3) | ||
| Age category | ||||||
| Children 9–11 years | 167 (23.2) | 499 (69.4) | 31 (4.3) | 22 (3.1) | 13.88 | 0.003 |
| Adolescent 12–17 years | 611 (21.6) | 1878 (66.3) | 174 (6.1) | 169 (6.0) | ||
| Religion | ||||||
| Muslim | 745 (21.8) | 2291 (67.0) | 203 (5.9) | 180 (5.3) | 7.19 | 0.066 |
| Non-Muslim | 33 (25.0) | 86 (65.2) | 2 (1.5) | 11 (8.3) | ||
| Residence | ||||||
| Urban | 449 (23.4) | 1232 (64.1) | 121 (6.3) | 120 (6.2) | 16.88 | 0.001 |
| Rural | 329 (20.2) | 1145 (70.3) | 84 (5.2) | 71 (4.4) | ||
| School Type | ||||||
| Public | 611 (22.8) | 1793 (67.0) | 132 (4.9) | 142 (5.3) | 17.64 | 0.001 |
| Private | 167 (19.1) | 584 (66.9) | 73 (8.4) | 49 (5.6) | ||
| School Level | ||||||
| Primary | 232 (29.1) | 511 (64.1) | 31 (3.9) | 23 (2.9) | 59.85 | 0.001 |
| Middle | 284 (20.8) | 942 (68.9) | 75 (5.5) | 67 (4.9) | ||
| Secondary | 181 (19.0) | 630 (66.0) | 66 (6.9) | 77 (8.1) | ||
| Higher Secondary | 81 (18.8) | 294 (68.1) | 33 (7.6) | 24 (5.6) | ||
| Total | 778 (21.9) | 2377 (66.9) | 205 (5.8) | 191 (5.4) | ||
| Body Mass Index | ||||||
|---|---|---|---|---|---|---|
| Underweight | Normal Weight | Overweight and Obese | ||||
| Variables | Sex | n (%) | n (%) | n (%) | χ2 | p-Value |
| Age category | ||||||
| Children 9–11 years | Boys | 80 (23.6) | 229 (67.6) | 30 (8.8) | 2.25 | 0.324 |
| Girls | 87 (22.9) | 270 (71.1) | 23 (6.1) | |||
| Adolescent 12–17 years | Boys | 410 (25.8) | 1021 (64.1) | 161 (10.1) | 44.02 | 0.001 |
| Girls | 201 (16.2) | 857 (69.1) | 182 (14.7) | |||
| Religion | ||||||
| Muslim | Boys | 470 (25.3) | 1205 (64.9) | 183 (9.8) | 32.42 | 0.001 |
| Girls | 275 (17.6) | 1086 (69.6) | 200 (12.8) | |||
| Non-Muslim | Boys | 20 (27.4) | 45 (61.6) | 8 (11.0) | 0.88 | 0.641 |
| Girls | 13 (22.0) | 41 (69.5) | 5 (8.5) | |||
| Residence | ||||||
| Urban | Boys | 285 (28.4) | 604 (60.1) | 116 (11.5) | 29.44 | 0.001 |
| Girls | 164 (17.9) | 628 (68.5) | 125 (13.6) | |||
| Rural | Boys | 205 (22.1) | 646 (69.8) | 75 (8.1) | 8.61 | 0.014 |
| Girls | 124 (17.6) | 499 (71.0) | 80 (11.4) | |||
| School Type | ||||||
| Public | Boys | 388 (26.8) | 944 (65.1) | 118 (8.1) | 36.71 | 0.001 |
| Girls | 223 (18.2) | 849 (69.1) | 156 (12.7) | |||
| Private | Boys | 102 (21.2) | 306 (63.6) | 73 (15.2) | 5.24 | 0.073 |
| Girls | 65 (16.6) | 278 (70.9) | 49 (12.5) | |||
| School Level | ||||||
| Primary | Boys | 143 (32.9) | 260 (59.9) | 31 (7.1) | 7.64 | 0.022 |
| Girls | 89 (24.5) | 251 (69.1) | 23 (6.3) | |||
| Middle | Boys | 170 (24.1) | 473 (67.2) | 61 (8.7) | 12.71 | 0.002 |
| Girls | 114 (17.2) | 469 (70.6) | 81 (12.2) | |||
| Secondary | Boys | 131 (23.5) | 350 (62.7) | 77 (13.8) | 17.87 | 0.001 |
| Girls | 50 (12.6) | 280 (70.7) | 66 (16.7) | |||
| Higher Secondary | Boys | 46 (19.6) | 167 (71.1) | 22 (9.4) | 6.60 | 0.037 |
| Girls | 35 (17.8) | 127 (64.5) | 35 (17.8) | |||
| Total | 778 (21.9) | 2377 (66.9) | 396 (11.2) | |||
| Unstandardized Coefficients | Standardized Coefficients | |||||
|---|---|---|---|---|---|---|
| Variables | B | SE | Β | T | Sig. | |
| Constant | 1.634 | 0.130 | 12.542 | 0.001 | ||
| 1 | Sex | 0.120 | 0.023 | 0.085 | 5.103 | 0.001 |
| 2 | Age | −0.014 | 0.010 | −0.046 | −1.434 | 0.152 |
| 3 | Religion | 0.015 | 0.062 | 0.004 | 0.238 | 0.812 |
| 4 | Residence | −0.042 | 0.024 | −0.030 | −1.747 | 0.081 |
| 5 | School Type | 0.087 | 0.027 | 0.054 | 3.197 | 0.001 |
| 6 | School Level | 0.117 | 0.024 | 0.158 | 4.954 | 0.001 |
| Underweight | Overweight | Obesity | ||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Sex a | 1.57 † | 1.33–1.85 | 0.82 | 0.61–1.08 | 0.71 * | 0.53–0.96 |
| Age category b | 0.90 | 0.74–1.10 | 1.45 | 0.98–2.14 | 2.01 ‡ | 1.27–3.16 |
| Religions c | 1.19 | 0.80–1.78 | 0.24 * | 0.06–0.92 | 1.63 | 0.86–3.08 |
| Residence d | 1.20 * | 1.02–1.41 | 1.23 | 0.92–1.64 | 1.46 * | 1.08–1.97 |
| School type e | 0.80 * | 0.66–0.96 | 1.76 | 1.30–2.36 | 1.06 | 0.76–1.48 |
| School level | 0.70 † | 0.60–0.82 | 1.18 | 0.90–1.54 | 1.37 * | 1.05–1.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanveer, M.; Hohmann, A.; Roy, N.; Zeba, A.; Tanveer, U.; Siener, M. The Current Prevalence of Underweight, Overweight, and Obesity Associated with Demographic Factors among Pakistan School-Aged Children and Adolescents—An Empirical Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 11619. https://doi.org/10.3390/ijerph191811619
Tanveer M, Hohmann A, Roy N, Zeba A, Tanveer U, Siener M. The Current Prevalence of Underweight, Overweight, and Obesity Associated with Demographic Factors among Pakistan School-Aged Children and Adolescents—An Empirical Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11619. https://doi.org/10.3390/ijerph191811619
Chicago/Turabian StyleTanveer, Moazzam, Andreas Hohmann, Nadeem Roy, Asifa Zeba, Umar Tanveer, and Maximilian Siener. 2022. "The Current Prevalence of Underweight, Overweight, and Obesity Associated with Demographic Factors among Pakistan School-Aged Children and Adolescents—An Empirical Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 18: 11619. https://doi.org/10.3390/ijerph191811619
APA StyleTanveer, M., Hohmann, A., Roy, N., Zeba, A., Tanveer, U., & Siener, M. (2022). The Current Prevalence of Underweight, Overweight, and Obesity Associated with Demographic Factors among Pakistan School-Aged Children and Adolescents—An Empirical Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(18), 11619. https://doi.org/10.3390/ijerph191811619