
Risk, Obligation, and Public Noncompliance with Mobility Directives in China during the COVID-19 Pandemic


Abstract
:1. Introduction
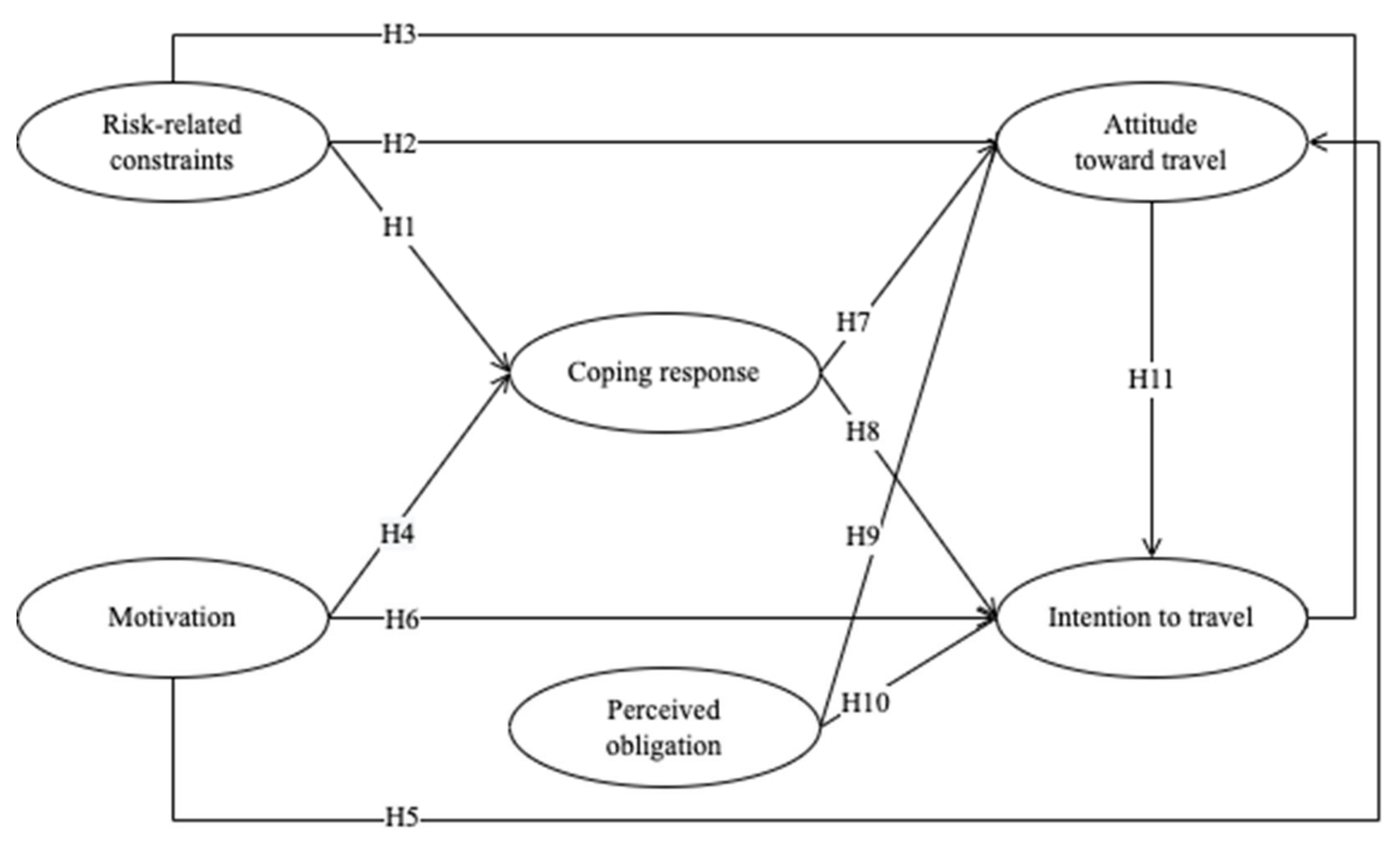
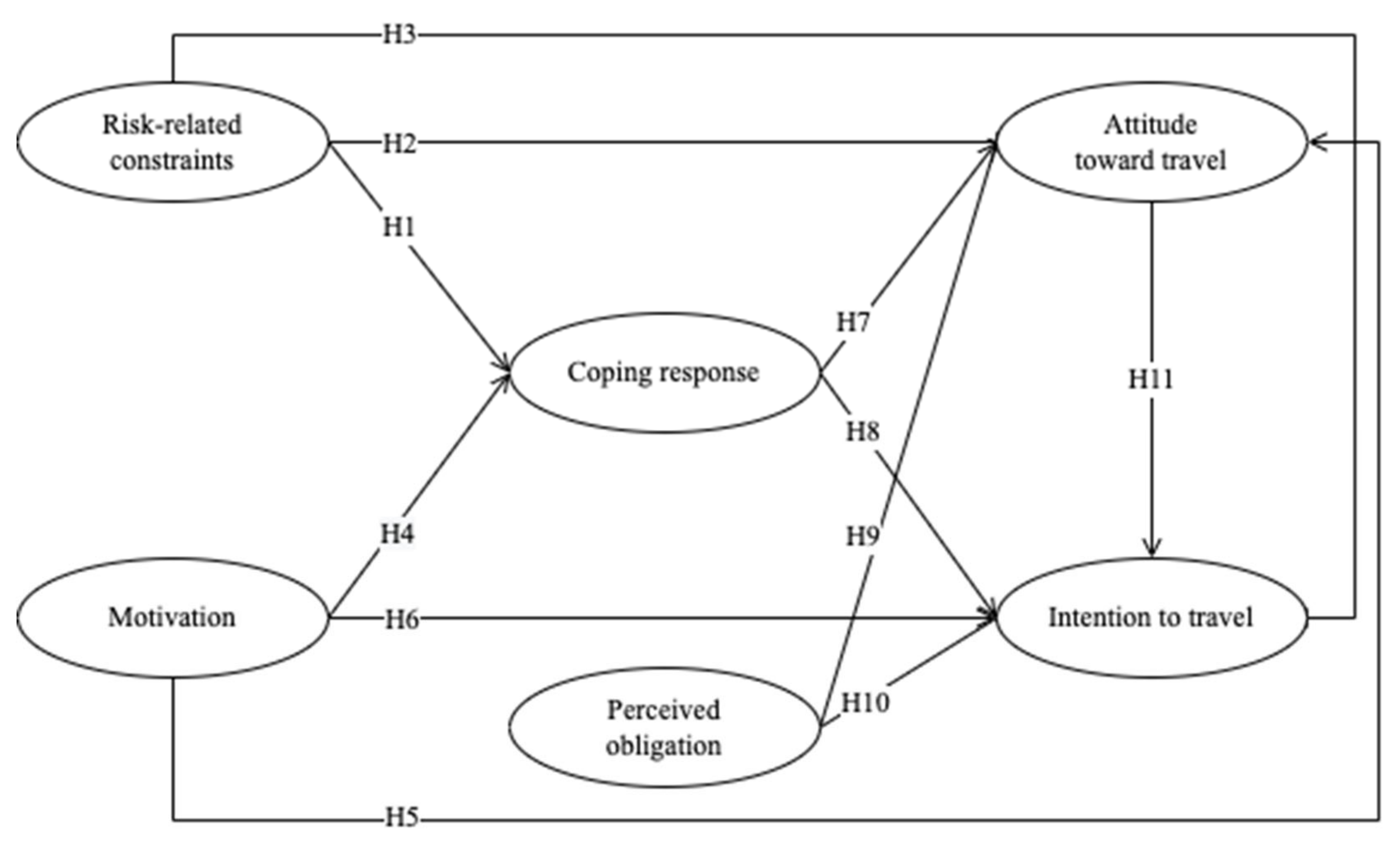
2. Theoretical Background and Hypothesis Development
2.1. Epidemics and Public Compliance Behavior
2.2. Interaction between Travel Motivations and Risk-Related Constraints
2.3. Coping: Adaptive and Maladaptive Responses
2.4. Perceived Obligation and Attitude/Intention
3. Methods
3.1. Measurement Scale
3.2. Setting and Sampling
3.3. Data Analysis Methods
4. Results
4.1. Travel Motivations and Risk-Related Constraints
4.2. Coping, Obligation, Attitude, and Intention to Travel
4.3. Comparison of Those Who Traveled and Those Who Did Not
4.4. Dynamic Travel Decision-Making during the Pandemic
4.4.1. Measurement Models
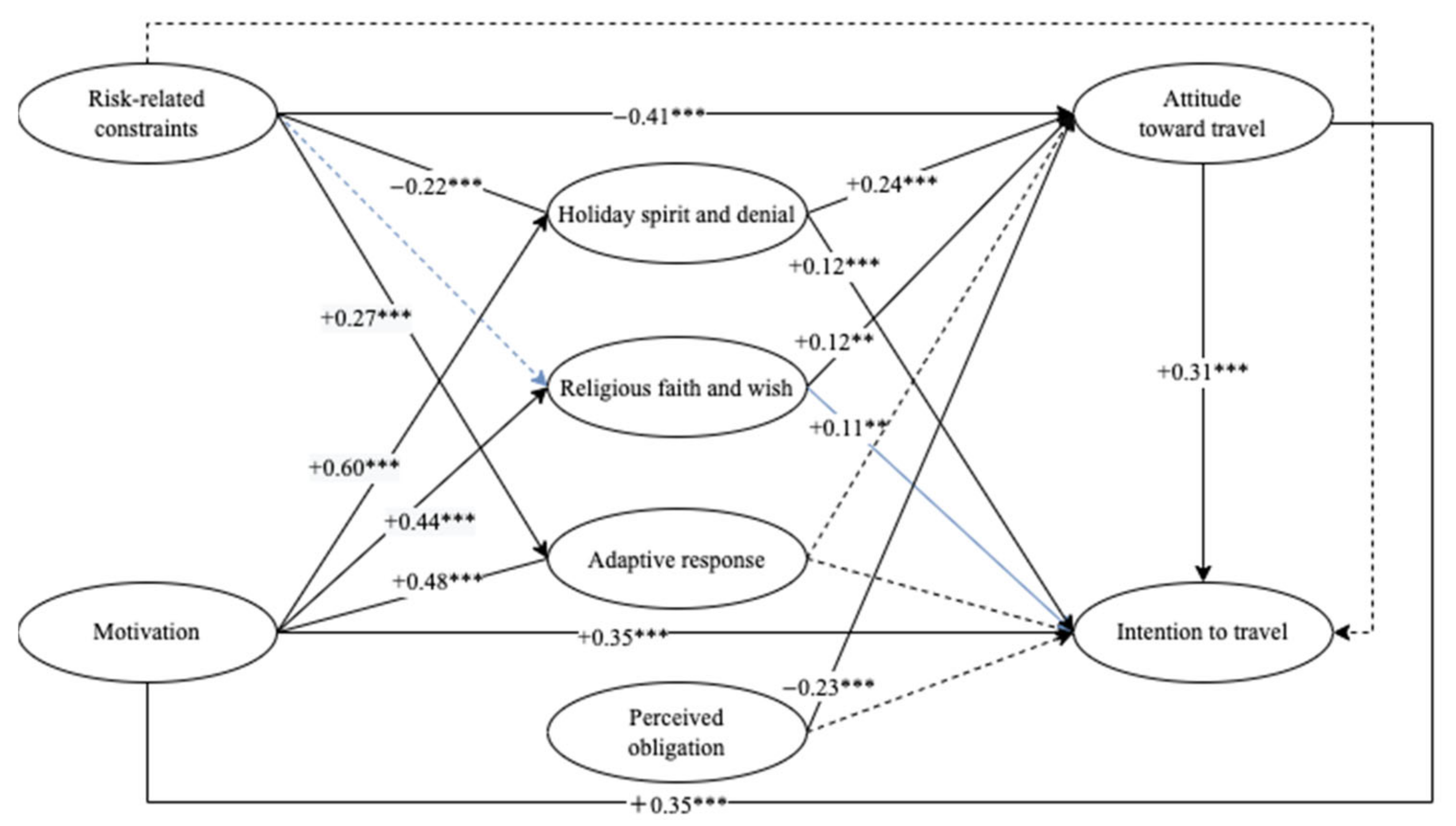
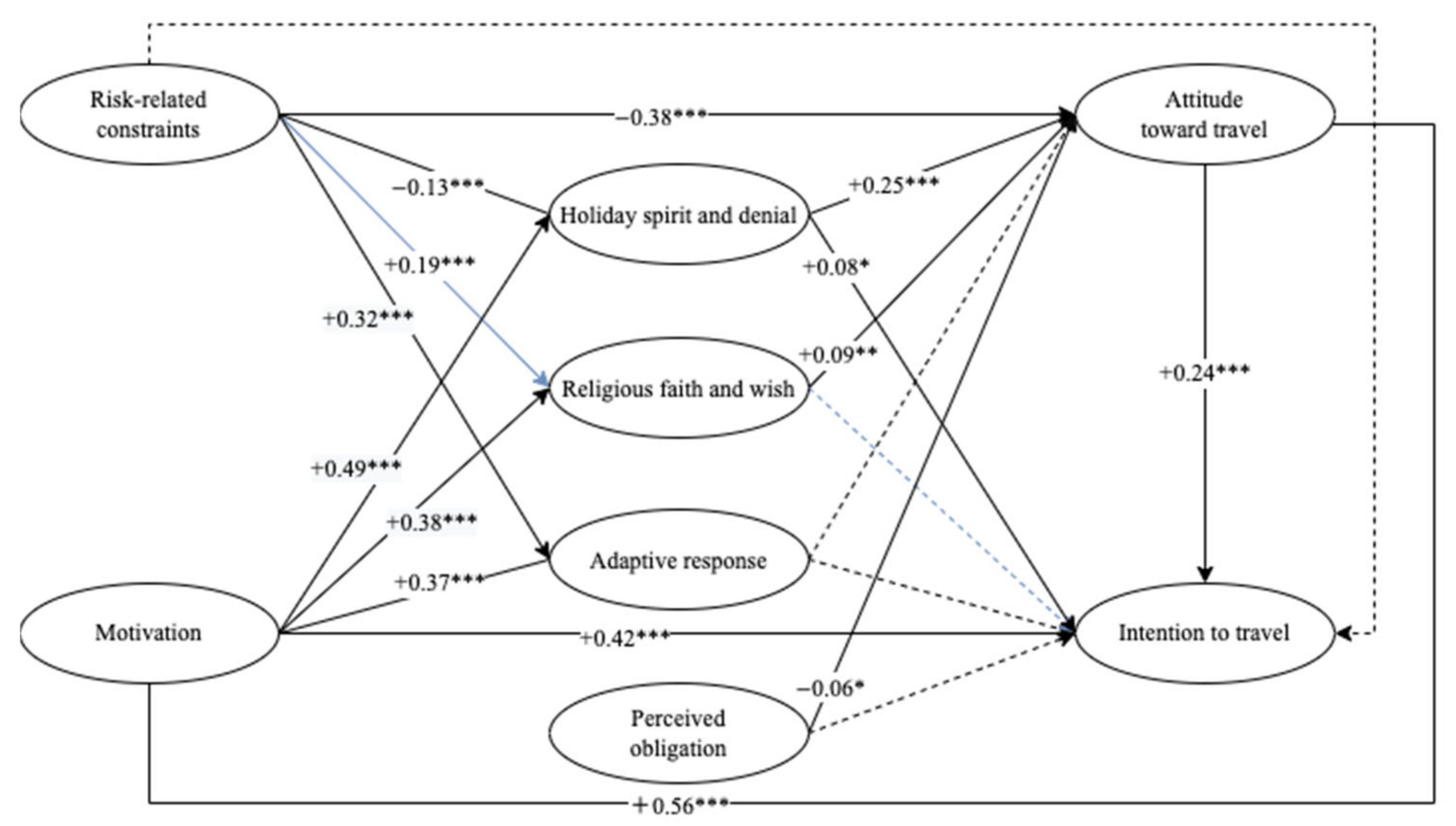
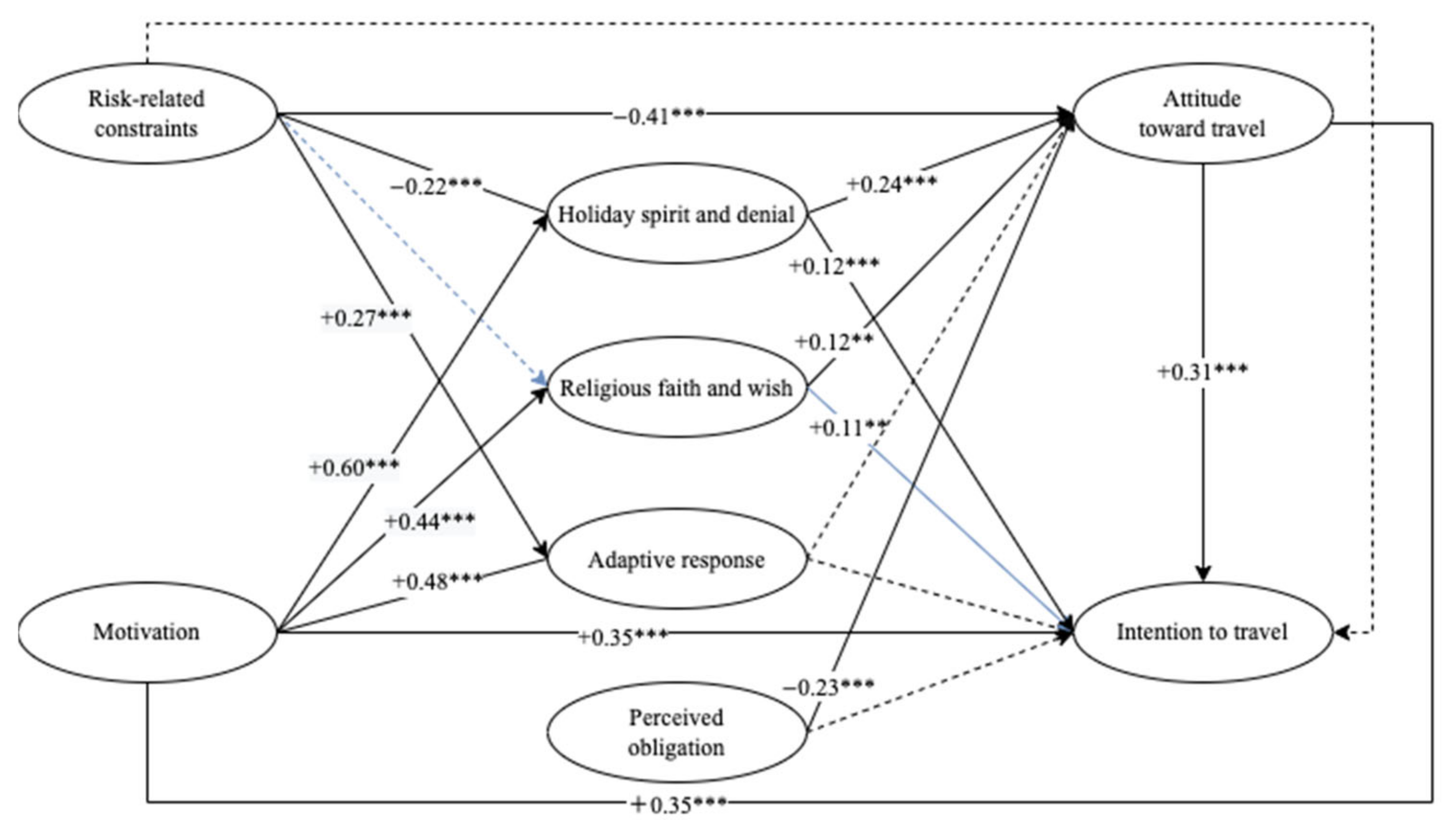
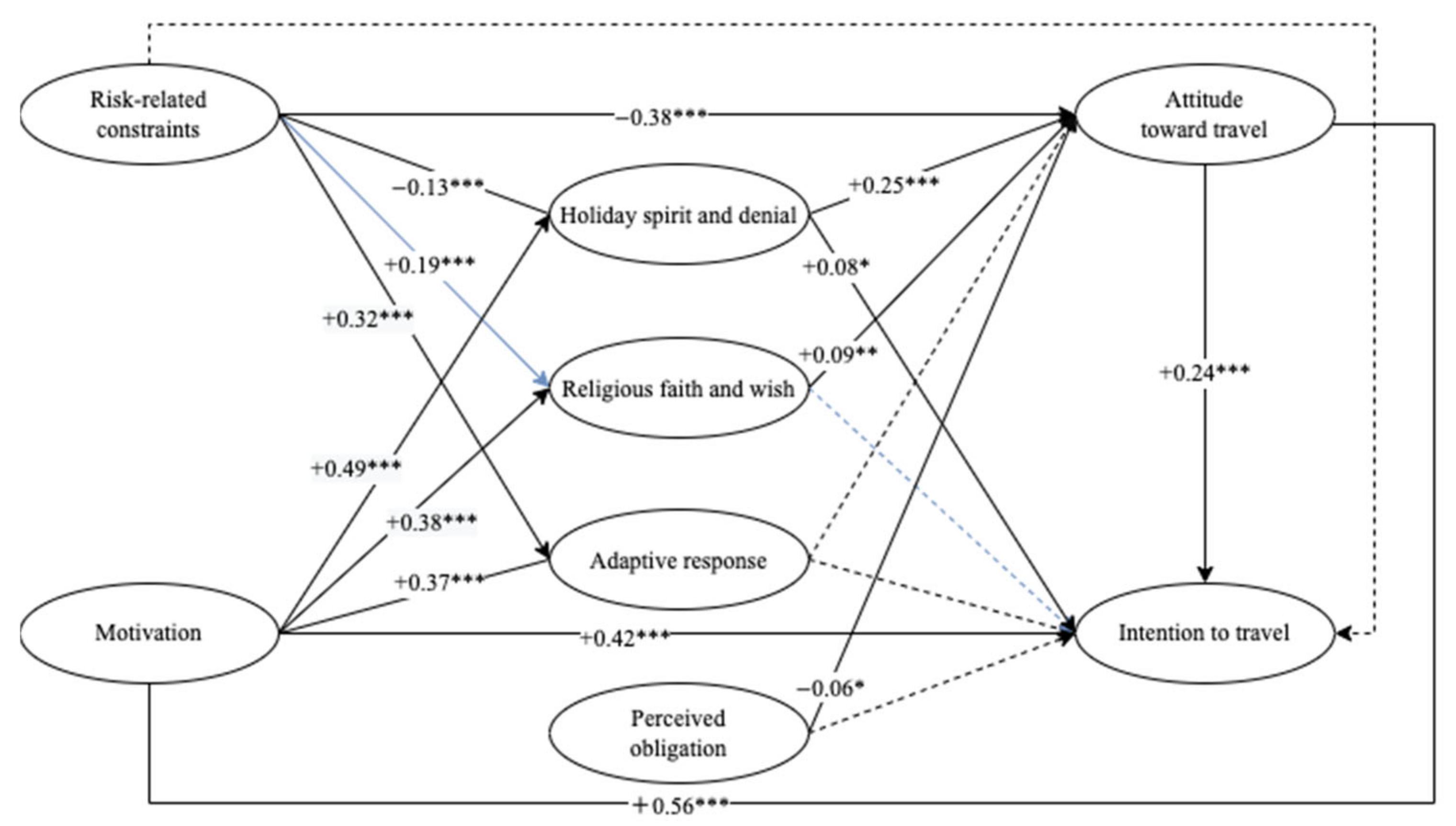
4.4.2. Hypothesis Testing
4.4.3. Mediating Effects
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Factor | Item | Reference |
|---|---|---|
| Relaxation and proximity to nature | relax in a beautiful location | Zhang et al., 2021 [60] |
| visit scenic spots to exercise my muscles and bones | ||
| enjoy the beautiful natural scenery | ||
| visit sunny places and relieve my anxiety regarding the epidemic | ||
| Pull motives | The online booking for ticket reduces risks. | |
| The scenic spot is equipped with hardware and software for epidemic prevention and control, which dispels my worries. | ||
| The scenic spot uses big data to fully understand the health status of tourists. | ||
| The scenic spot implements time-based and decentralized tours, which are relatively safe. | ||
| Ordinary motives | seek novelty | |
| increase knowledge through travel | ||
| experience a different culture and life | ||
| spend a happy time with family/friends | ||
| Peak shifting motives | enjoy the beautiful scenery alone | |
| easier to find an angle to avoid the crowd when taking pictures | ||
| take advantage of the recent free time to travel | ||
| Intrapersonal constraints | I worry about contracting COVID-19 while travelling in scenic spots. | Cahyanto et al., 2016 [40] Chen et al., 2013 [31] Hung and Petrick, 2012 [35] Nyaupane and Andereck, 2008 [59] |
| I am worried about contracting COVID-19 while using transportation facilities. | ||
| I am afraid of COVID-19 and worried about becoming infected. | ||
| I don’t like taking risks; I cherish life. | ||
| Interpersonal constraints | hard to find a companion | |
| My family and friends disagree with my intention to travel now. | ||
| I am worried about being criticized by others for travelling now. | ||
| Structural constraints | Hotels, restaurants, etc. are risky. | |
| The external environment is too complicated. | ||
| encounter many difficulties and inconveniences | ||
| I can travel anytime, and I don’t have to do it now. | ||
| Perceived obligation | I feel obligated to stay at home to support epidemic prevention and control. | Hartanto et al., 2020 [61] |
| I feel obligated to ensure adherence to the restrictions of home isolation so as to respect others. | ||
| I feel obligated to main vigilance in the critical period of epidemic prevention. | ||
| Holiday spirit and denial | I am always in good health and have a strong immune system; so, I will be fine when traveling. | Wang et al., 2019 [9] |
| I wear a mask and wash my hands in time; so, I don’t have to worry about infection. | ||
| I try not to think too much about the health risks every time I travel. | ||
| Religious faith and wish | I believe that any health issues I might encounter during travelling will be miraculously cured in the future. | |
| God will protect me from the virus. | ||
| If it’s your destiny to get infected during your trip, there is little you can do. | ||
| Adaptive response | Wait in line at least 1.5 m apart from another person and try to avoid crowded areas. | |
| Seek information on the progress of epidemic prevention and control. | ||
| Attitude | Travelling now is suitable. | Hung and Hsu, 2009 [57] |
| Travelling now is pleasant. | ||
| Travelling now is safe. | ||
| Intention | I plan to go to an urban park. | Hung and Hsu, 2009 [57] |
| I plan to taste nearby cuisine. | ||
| I desire to visit short-distance tourist attractions. | ||
| I desire to travel to low-risk destinations. | ||
| I intend to visit natural scenic spots. |
References
- Li, J.; Nguyen, T.H.H.; Coca-Stefaniak, J.A. Coronavirus impacts on post-pandemic planned travel behaviours. Ann. Tour. Res. 2020, 102964. [Google Scholar] [CrossRef]
- Williams, A.M.; Baláž, V. Tourism risk and uncertainty: Theoretical reflections. J. Travel Res. 2014, 54, 271–287. [Google Scholar] [CrossRef]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Piontti, A.P.Y.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef]
- Germani, A.; Buratta, L.; Delvecchio, E.; Mazzeschi, C. Emerging adults and COVID-19: The role of individualism-collectivism on perceived risks and psychological maladjustment. Int. J. Environ. Res. Public. Health 2020, 17, 3497. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.; Lam, E.P.; Chan, C.; Chan, S.; Chiu, M.; Chong, W.; Chu, K.; Hon, M.; Kwan, L.; Tsang, K.; et al. Practice and technique of using face mask amongst adults in the community: A cross-sectional descriptive study. BMC Public Health 2020, 20, 948. [Google Scholar] [CrossRef] [PubMed]
- Hailu, W.; Derseh, L.; Hunegnaw, M.T.; Tesfaye, T.; Abebaw, D. Compliance, barriers, and facilitators to social distancing measures for prevention of coronavirus disease 2019 in Northwest Ethiopia, 2020. Curr. Ther. Res. 2021, 94, 100632. [Google Scholar] [CrossRef]
- Wang, D.; Marmo-Roman, S.; Krase, K.; Phanord, L. Compliance with preventative measures during the COVID-19 pandemic in the USA and Canada: Results from an online survey. Soc. Work Health Care 2021, 60, 240–255. [Google Scholar] [CrossRef]
- Yue, R.P.H.; Lau, B.H.P.; Chan, C.L.W.; Ng, S.-M. Risk perception as a double-edged sword in policy compliance in COVID-19 pandemic? A two-phase evaluation from Hong Kong. J. Risk Res. 2021, 1936612. [Google Scholar] [CrossRef]
- Wang, J.; Liu-Lastres, B.; Ritchie, B.W.; Mills, D.J. Travellers’ self-protections against health risks: An application of the full protection motivation theory. Ann. Tour. Res. 2019, 78, 102743. [Google Scholar] [CrossRef]
- Kaim, A.; Siman-Tov, M.; Jaffe, E.; Adini, B. Factors that enhance or impede compliance of the public with governmental regulation of lockdown during COVID-19 in Israel. Int. J. Disaster Risk Reduct. 2021, 66, 102596. [Google Scholar] [CrossRef]
- Offurum, C.J.; Leibetseder, M.; Jenull, B. Understanding Compliant Behavior During a Pandemic: Contribution From the Perspective of Schema-Based Psychotherapy. Front. Psychol. 2022, 13, 805987. [Google Scholar] [CrossRef]
- Asnakew, Z.; Asrese, K.; Andualem, M. Community Risk Perception and Compliance with Preventive Measures for COVID-19 Pandemic in Ethiopia. Risk Manag. Healthc. Policy 2020, 13, 2887–2897. [Google Scholar] [CrossRef]
- Copping, L.T. Anxiety and COVID-19 compliance behaviors in the UK: The moderating role of conspiratorial thinking. Personal. Individ. Differ. 2022, 192, 111604. [Google Scholar] [CrossRef]
- Siegrist, M.; Luchsinger, L.; Bearth, A. The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID-19 Cases. Risk Anal. 2021, 41, 787–800. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van Der Bles, A.M.; Spiegelhalter, D.; Van Der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Wong, C.M.L.; Jensen, O. The paradox of trust: Perceived risk and public compliance during the COVID-19 pandemic in Singapore. J. Risk Res. 2020, 23, 1021–1030. [Google Scholar] [CrossRef]
- Franzen, A.; Wöhner, F. Fatigue during the COVID-19 pandemic: Evidence of social distancing adherence from a panel study of young adults in Switzerland. PLoS ONE 2021, 16, 0261276. [Google Scholar]
- Erisen, C. Psychological foundations and behavioral consequences of COVID-19 conspiracy theory beliefs: The Turkish case. Int. Polit. Sci. Rev. 2022. [Google Scholar] [CrossRef]
- Leblanc-Sirois, Y.; Gagnon, M.È.; Blanchette, I. Affective States During the First Wave of the COVID-19 Pandemic: Progression of Intensity and Relation With Public Health Compliance Behavior. Front. Psychol. 2022, 13, 883995. [Google Scholar] [CrossRef]
- Cohen, A.S.; Lutzke, L.; Otten, C.D.; Arvai, J. I Think, Therefore I Act: The Influence of Critical Reasoning Ability on Trust and Behavior During the COVID-19 Pandemic. Risk Anal. 2022, 42, 1073–1085. [Google Scholar] [CrossRef]
- Choma, B.L.; Hodson, G.; Sumantry, D.; Hanoch, Y.; Gummerum, M. Ideological and Psychological Predictors of COVID-19-Related Collective Action, Opinions, and Health Compliance Across Three Nations. J. Soc. Polit. Psychol. 2021, 9, 123–143. [Google Scholar] [CrossRef]
- Wang, C.; Tang, N.; Zhen, D.; Wang, X.R.; Zhang, J.; Cheong, Y.; Zhu, Q. Need for cognitive closure and trust towards government predicting pandemic behavior and mental health: Comparing United States and China. Curr. Psychol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.; Morakabati, Y. Tourism activity, terrorism and political instability within the Commonwealth: The cases of Fiji and Kenya. Int. J. Tour. Res. 2008, 10, 537–556. [Google Scholar] [CrossRef]
- Fu, C.; Liao, L.; Huang, W. Behavioral Implementation and Compliance of Anti-Epidemic Policy in the COVID-19 Crisis. Int. J. Environ. Res. Public. Health 2021, 18, 3776. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.; Nicolau, J.L.; Kang, J.; Sharma, A.; Lee, H. Travel decision determinants during and after COVID-19: The role of tourist trust, travel constraints, and attitudinal factors. Tour. Manag. 2022, 88, 104428. [Google Scholar] [CrossRef] [PubMed]
- Backman, S.J.; Crompton, J.L. Discriminating between continuers and discontinuers of two public leisure services. J. Park Recreat. Adm. 1989, 7, 56–71. [Google Scholar]
- Crawford, D.W.; Jackson, E.L.; Godbey, G. A hierarchical model of leisure constraints. Leis. Sci. 1991, 13, 309–320. [Google Scholar] [CrossRef]
- Jackson, E.L.; Crawford, D.W.; Godbey, G. Negotiation of leisure constraints. Leis. Sci. 1993, 15, 1–11. [Google Scholar] [CrossRef]
- Crawford, D.W.; Godbey, G. Reconceptualizing barriers to family leisure. Leis. Sci. 1987, 9, 119–127. [Google Scholar] [CrossRef]
- Gilbert, D.; Hudson, S. Tourism demand constraints. Ann. Tour. Res. 2000, 27, 906–925. [Google Scholar] [CrossRef]
- Chen, H.J.; Chen, P.J.; Okumus, F. The relationship between travel constraints and destination image: A case study of Brunei. Tour. Manag. 2013, 35, 198–208. [Google Scholar] [CrossRef]
- Aliperti, G.; Cruz, A.M. Investigating tourists’ risk information processing. Ann. Tour. Res. 2019, 79, 102803. [Google Scholar] [CrossRef]
- Guo, Y.; Hou, X. The effects of job crafting on tour leaders’ work engagement: The mediating role of person-job fit and meaningfulness of work. Int. J. Contemp. Hosp. Manag. 2022, 34, 1649–1667. [Google Scholar] [CrossRef]
- Hubbard, J.; Mannell, R.C. Testing competing models of the leisure constraint negotiation process in a corporate employee recreation setting. Leis. Sci. 2001, 23, 145–163. [Google Scholar] [CrossRef]
- Hung, K.; Petrick, J.F. Testing the effects of congruity, travel constraints, and self-efficacy on travel intentions: An alternative decision-making model. Tour. Manag. 2012, 33, 855–867. [Google Scholar] [CrossRef]
- Zheng, C.; Zhang, J.; Guo, Y.; Zhang, Y.; Qian, L. Disruption and reestablishment of place attachment after large-scale disasters: The role of perceived risk, negative emotions, and coping. Int. J. Disaster Risk Reduct. 2019, 40, 101273. [Google Scholar] [CrossRef]
- Hastall, M.R.; Scherenberg, V. Widerstände gegen Präventionsmaßnahmen während der COVID-19-Pandemie: Ursachen und Strategien für ihre Minimierung. Prävent. Gesundh. 2022. [Google Scholar] [CrossRef]
- Fox, K.M.; McDermott, L. Where is leisure when death is present? Leis. Sci. 2021, 43, 267–272. [Google Scholar] [CrossRef]
- Rittichainuwat, B.N.; Chakraborty, G. Perceived travel risks regarding terrorism and disease: The case of Thailand. Tour. Manag. 2009, 30, 410–418. [Google Scholar] [CrossRef]
- Cahyanto, I.; Wiblishauser, M.; Pennington-Gray, L.; Schroeder, A. The dynamics of travel avoidance: The case of Ebola in the US. Tour. Manag. Perspect. 2016, 20, 195–203. [Google Scholar] [CrossRef]
- Rippetoe, P.A.; Rogers, R.W. Effects of components of protection-motivation theory on adaptive and maladaptive coping with a health threat. J. Pers. Soc. Psychol. 1987, 52, 596–604. [Google Scholar] [CrossRef]
- Tanner, J.F.; Hunt, J.B.; Eppright, D.R. The protection motivation model: A normative model of fear appeals. J. Mark. 1991, 55, 36–45. [Google Scholar] [CrossRef]
- Wismans, A.; Letina, S.; Wennberg, K.; Thurik, R.; Baptista, R.; Burke, A.; Dejardin, M.; Janssen, F.; Santarelli, E.; Torrès, O.; et al. The role of impulsivity and delay discounting in student compliance with COVID-19 protective measures. Personal. Individ. Differ. 2021, 179, 110925. [Google Scholar] [CrossRef]
- Morakabati, Y. Tourism, travel risk and travel risk perceptions: A study of travel risk perceptions and the effects of incidents on tourism. PhD Thesis, University of Bournemouth, Bournemouth, UK, 2007. [Google Scholar]
- Saha, S.; Yap, G. The Moderation Effects of Political Instability and Terrorism on Tourism Development: A Cross-Country Panel Analysis. J. Travel Res. 2014, 53, 509–521. [Google Scholar] [CrossRef]
- Styhre, A. Rethinking knowledge: A Bergsonian critique of the notion of tacit knowledge. Br. J. Manag. 2004, 15, 177–188. [Google Scholar] [CrossRef]
- Floyd, M.F.; Pennington-Gray, L. Profiling risk perceptions of tourists. Ann. Tour. Res. 2004, 31, 1051–1054. [Google Scholar] [CrossRef]
- Fuchs, G.; Uriely, N.; Reichel, A.; Maoz, D. Vacationing in a terror-stricken destination: Tourists’ risk perceptions and rationalizations. J. Travel Res. 2013, 52, 182–191. [Google Scholar] [CrossRef]
- Jonas, A.; Mansfeld, Y.; Paz, S.; Potasman, I. Determinants of health risk perception among low-risk-taking tourists traveling to developing countries. J. Travel Res. 2011, 49, 87–99. [Google Scholar] [CrossRef]
- Cho, H.; Guo, Y.; Torelli, C. Collectivism fosters preventive behaviors to contain the spread of COVID-19: Implications for social marketing in public health. Psychol. Mark. 2022, 39, 694–700. [Google Scholar] [CrossRef]
- Kim, H.S.; Sherman, D.K.; Updegraff, J.A. Fear of Ebola. Psychol. Sci. 2016, 27, 935–944. [Google Scholar] [CrossRef]
- Zhang, X.; Liang, X.; Sun, H. Individualism–Collectivism, Private Benefits of Control, and Earnings Management: A Cross-Culture Comparison. J. Bus. Ethics 2013, 114, 655–664. [Google Scholar] [CrossRef]
- Zheng, D.; Luo, Q.; Ritchie, B.W. Afraid to travel after COVID-19? Self-protection, coping and resilience against pandemic ‘travel fear’. Tour. Manag. 2021, 83, 104261. [Google Scholar] [CrossRef]
- Oishi, S.; Komiya, A. Natural disaster risk and collectivism. J. Cross-Cult. Psychol. 2017, 48, 1263–1270. [Google Scholar] [CrossRef]
- Cashdan, E.; Steele, M. Pathogen Prevalence, Group Bias, and Collectivism in the Standard Cross-Cultural Sample. Hum. Nat. 2013, 24, 59–75. [Google Scholar] [CrossRef]
- Lee, J.; Kim, Y. When thinking of my death leads to thinking of others’ deaths: The effect of collectivism, psychological closeness, and mortality salience on prosocial behavioral intentions in the Sewol ferry disaster. J. Risk Res. 2021, 24, 756–770. [Google Scholar] [CrossRef]
- Huang, S.; Hsu, C.H. Effects of travel motivation, past experience, perceived constraint, and attitude on revisit intention. J. Travel Res. 2009, 48, 29–44. [Google Scholar] [CrossRef]
- Churchill, G.A. A paradigm for developing better measures of marketing constructs. J. Mark. Res. 1979, 16, 64–73. [Google Scholar] [CrossRef]
- Nyaupane, G.P.; Andereck, K.L. Understanding Travel Constraints: Application and Extension of a Leisure Constraints Model. J. Travel Res. 2008, 46, 433–439. [Google Scholar] [CrossRef]
- Zhang, H.; Zhuang, M.; Cao, Y.; Pan, J.; Zhang, X.; Zhang, J.; Zhang, H. Social Distancing in Tourism Destination Management during the COVID-19 Pandemic in China: A Moderated Mediation Model. Int. J. Environ. Res. Public. Health 2021, 18, 11223. [Google Scholar] [CrossRef]
- Hartanto, A.; Lau, I.Y.M.; Yong, J.C. Culture moderates the link between perceived obligation and biological health risk: Evidence of culturally distinct pathways for positive health outcomes. Soc. Sci. Med. 2020, 244, 112644. [Google Scholar] [CrossRef]
- Nunnally, J.C. Psychometric Theory. Am. Educ. Res. J. 1978, 5, 83. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS; Sage Publications: Beverly Hills, CA, USA, 2009. [Google Scholar]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics. J. Mark. Res. 1981, 18, 382–388. [Google Scholar] [CrossRef]
- Hair, J.F. Multivariate Data Analysis: A Global Perspective; Prentice Hall: Upper Saddle River, NJ, USA, 2009; ISBN 0-13-515309-3. [Google Scholar]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing moderated mediation hypotheses: Theory, methods, and prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2013; ISBN 1-4625-3465-1. [Google Scholar]
- Shrout, P.E.; Bolger, N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef]
- Rana, I.A.; Bhatti, S.S.; Aslam, A.B.; Jamshed, A.; Ahmad, J.; Shah, A.A. COVID-19 risk perception and coping mechanisms: Does gender make a difference? Int. J. Disaster Risk Reduct. 2021, 55, 102096. [Google Scholar] [CrossRef]
- Shanka, M.S.; Kotecho, M.G. Combining rationality with morality—Integrating theory of planned behavior with norm activation theory to explain compliance with COVID-19 prevention guidelines. Psychol. Health Med. 2021. [Google Scholar] [CrossRef]
- Holba, A.M. Groundwork for an Ethics of death: Leisure, faith, resilience. J. Commun. Relig. 2016, 39, 5–20. [Google Scholar]
- Mheidly, N.; Fares, J. Leveraging media and health communication strategies to overcome the COVID-19 infodemic. J. Public Health Policy 2020, 41, 410–420. [Google Scholar] [CrossRef]
- González-Padilla, D.A.; Tortolero-Blanco, L. Social media influence in the COVID-19 Pandemic. Int. Braz. J. Urol. 2020, 46, 120–124. [Google Scholar] [CrossRef]
- Bendau, A.; Petzold, M.B.; Pyrkosch, L.; Mascarell Maricic, L.; Betzler, F.; Rogoll, J.; Große, J.; Ströhle, A.; Plag, J. Associations between COVID-19 related media consumption and symptoms of anxiety, depression and COVID-19 related fear in the general population in Germany. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 283–291. [Google Scholar] [CrossRef]
- Zhu, H.; Deng, F. How to Influence Rural Tourism Intention by Risk Knowledge during COVID-19 Containment in China: Mediating Role of Risk Perception and Attitude. Int. J. Environ. Res. Public. Health 2020, 17, 3514. [Google Scholar] [CrossRef]
- Wang, J.; Choe, Y.; Song, H. Korean Domestic Tourists’ Decision-Making Process under Threat of COVID-19. Int. J. Environ. Res. Public. Health 2021, 18, 10835. [Google Scholar] [CrossRef]
- Zhong, L.; Sun, S.; Law, R.; Li, X.; Yang, L. Perception, Reaction, and Future Development of the Influence of COVID-19 on the Hospitality and Tourism Industry in China. Int. J. Environ. Res. Public. Health 2022, 19, 991. [Google Scholar] [CrossRef]
- Lu, J.; Xiao, X.; Xu, Z.; Wang, C.; Zhang, M.; Zhou, Y. The potential of virtual tourism in the recovery of tourism industry during the COVID-19 pandemic. Curr. Issues Tour. 2022, 25, 441–457. [Google Scholar] [CrossRef]
- Zhang, S.N.; Li, Y.Q.; Ruan, W.Q.; Liu, C.H. Would you enjoy virtual travel? The characteristics and causes of virtual tourists’ sentiment under the influence of the COVID-19 pandemic. Tour. Manag. 2022, 88, 104429. [Google Scholar] [CrossRef]
- Rahim, N.Z.A.; Nasaruddin, N.I.S.; Shah, N.B.A.; Halim, F.H.; Samah, K.A.F.A.; Saman, F.I.; Rum, S.F.M. Aftermath of pandemic Covid-19 on tourism industry: A review on virtual tourism platform. AIP Conf. Proc. 2021, 2347, 020173. [Google Scholar]
- Akhtar, N.; Khan, N.; Mahroof Khan, M.; Ashraf, S.; Hashmi, M.S.; Khan, M.M.; Hishan, S.S. Post-COVID 19 Tourism: Will Digital Tourism Replace Mass Tourism? Sustainability 2021, 13, 5352. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, H.; Guo, Z.; Huang, M.; Pan, Y.; Guo, Y. Online reservation intention of tourist attractions in the COVID-19 context: An extended technology acceptance model. Sustainability 2022, 14, 10395. [Google Scholar] [CrossRef]
| Factor and Item | EFA (Round1 N = 700) | EFA (Round2 N = 773) | t | Probability | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Loading | Eigenvalue | Variance Explained (%) | Mean | Loading | Eigenvalue | Variance Explained (%) | |||
| 3.93 | 7.66 | 51.06 | 4.03 | 6.94 | 46.27 | −2.35 | 0.019 | ||
| Moti1 relax in a beautiful location | 3.93 | 0.85 | 4.09 | 0.78 | ||||||
| Moti2 visit scenic spots to exercise my muscles and bones | 3.86 | 0.84 | 3.95 | 0.78 | ||||||
| Moti3 enjoy the beautiful natural scenery | 3.95 | 0.83 | 4.11 | 0.84 | ||||||
| Moti4 visit sunny places and relieve my anxiety regarding the epidemic | 3.98 | 0.83 | 3.98 | 0.76 | ||||||
| 3.40 | 1.87 | 12.43 | 3.68 | 1.75 | 11.63 | −6.78 | 0.000 | ||
| Pull1 The online booking for ticket reduces risks. | 3.61 | 0.74 | 3.85 | 0.74 | ||||||
| Pull2 The scenic spot is equipped with hardware and software for epidemic prevention and control, which dispels my worries. | 3.20 | 0.86 | 3.51 | 0.83 | ||||||
| Pull3 The scenic spot uses big data to fully understand the health status of tourists. | 3.26 | 0.87 | 3.60 | 0.88 | ||||||
| Pull4 The scenic spot implements time-based and decentralized tours, which are relatively safe. | 3.49 | 0.84 | 3.78 | 0.83 | ||||||
| 3.40 | 1.24 | 8.25 | 3.59 | 1.21 | 8.05 | −4.42 | 0.000 | ||
| Moti10 seek novelty | 2.77 | 0.62 | 2.94 | 0.67 | ||||||
| Moti11 increase knowledge through travel | 3.43 | 0.84 | 3.58 | 0.82 | ||||||
| Moti12 experience a different culture and life | 3.66 | 0.83 | 3.86 | 0.79 | ||||||
| Moti13 spend a happy time with family/friends | 3.74 | 0.71 | 3.99 | 0.60 | ||||||
| 3.14 | 1.08 | 7.17 | 3.43 | 1.11 | 7.40 | −5.84 | 0.000 | ||
| Moti6 enjoy the beautiful scenery alone | 3.15 | 0.83 | 3.41 | 0.81 | ||||||
| Moti7 easier to find an angle to avoid the crowd when taking pictures | 3.24 | 0.82 | 3.43 | 0.86 | ||||||
| Moti8 take advantage of the recent free time to travel | 3.05 | 0.73 | 3.47 | 0.67 | ||||||
| Round1: KMO = 0.92, Bartlett’s test of sphericity: χ2 = 8151.98, p < 0.000, α = 0.93, 78.92%; KMO = 0.91, Bartlett’s test of sphericity: χ2 = 7011.28, p < 0.000, α = 0.92, 73.35%; | ||||||||||
| 3.83 | 1.47 | 13.40 | 3.59 | 5.23 | 47.57 | 6.29 | 0.000 | ||
| Intra1 I worry about contracting COVID-19 while travelling in scenic spots. | 3.77 | 0.77 | 3.57 | 0.85 | ||||||
| Intra2 I am worried about contracting COVID-19 while using transportation facilities. | 3.98 | 0.78 | 3.72 | 0.84 | ||||||
| Intra3 I am afraid of COVID-19 and worried about becoming infected. | 3.75 | 0.72 | 3.46 | 0.62 | ||||||
| Intra4 I don’t like taking risks; I cherish life. | 3.80 | 0.83 | 3.60 | 0.82 | ||||||
| 3.71 | 1.16 | 10.52 | 3.33 | 1.00 | 9.07 | 9.75 | 0.000 | ||
| Inter1 hard to find a companion | 3.62 | 0.82 | 3.36 | 0.76 | ||||||
| Inter2 My family and friends disagree with my intention to travel now. | 3.94 | 0.74 | 3.49 | 0.75 | ||||||
| Inter3 I am worried about being criticized by others for travelling now. | 3.58 | 0.80 | 3.14 | 0.72 | ||||||
| 4.00 | 5.02 | 45.69 | 3.69 | 1.38 | 12.57 | 8.07 | 0.000 | ||
| Struct2 Hotels, restaurants, etc. are risky. | 3.82 | 0.67 | 3.67 | 0.75 | ||||||
| Struct3 The external environment is too complicated. | 4.01 | 0.85 | 3.65 | 0.83 | ||||||
| Struct4 encounter many difficulties and inconveniences | 4.07 | 0.85 | 3.71 | 0.77 | ||||||
| Struct6 I can travel anytime, and I don’t have to do it now. | 4.02 | 0.71 | 3.72 | 0.70 | ||||||
| Round1: KMO = 0.87, Bartlett’s test of sphericity: χ2 =3686.50, p < 0.000, α = 0.93, 69.59%; Round2: KMO = 0.88, Bartlett’s test of sphericity: χ2 =4310.292, p < 0.000, α = 0.92, 69.21% | ||||||||||
| Factor and Items | EFA (Round1 N = 700) | EFA (Round2 N = 773) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | Loading | Eigenvalue | Variance Explained (%) | Mean | Loading | Eigenvalue | Variance Explained (%) | |
| 4.39 | 2.60 | 86.72 | 4.19 | 2.48 | 82.67 | ||
| Ob1 I feel obligated to stay at home to support epidemic prevention and control. | 4.32 | 0.91 | 4.10 | 0.90 | ||||
| Ob2 I feel obligated to ensure adherence to the restrictions of home isolation so as to respect others. | 4.41 | 0.95 | 4.23 | 0.93 | ||||
| Ob3 I feel obligated to main vigilance in the critical period of epidemic prevention. | 4.44 | 0.93 | 4.25 | 0.90 | ||||
| Round1: KMO = 0.74, Bartlett’s test of sphericity: χ2 = 1650.92, p < 0.000; Round2: KMO = 0.74, Bartlett’s test of sphericity: χ2 = 1394.93, p < 0.000 | ||||||||
| 2.84 | 3.22 | 40.23 | 3.03 | 2.99 | 37.35 | ||
| Cop1 I am always in good health and have a strong immune system; so, I will be fine when traveling. | 3.04 | 0.79 | 3.20 | 0.83 | ||||
| Cop2 I wear a mask and wash my hands in time; so, I don’t have to worry about infection. | 2.81 | 0.87 | 3.04 | 0.86 | ||||
| Cop3 I try not to think too much about the health risks every time I travel. | 2.67 | 0.75 | 2.84 | 0.74 | ||||
| 3.20 | 1.37 | 17.12 | 2.90 | 1.49 | 18.63 | ||
| Cop6 I believe that any health issues I might encounter during travelling will be miraculously cured in the future. | 3.51 | 0.76 | 3.42 | 0.68 | ||||
| Cop7 God will protect me from the virus. | 2.90 | 0.82 | 2.79 | 0.85 | ||||
| Cop8 If it’s your destiny to get infected during your trip, there is little you can do. | 2.39 | 0.58 | 2.50 | 0.74 | ||||
| 3.65 | 1.12 | 14.04 | 3.73 | 1.17 | 14.56 | ||
| Cop4 Wait in line at least 1.5 m apart from another person and try to avoid crowded areas. | 3.59 | 0.84 | 3.69 | 0.84 | ||||
| Cop5 Seek information on the progress of epidemic prevention and control. | 3.71 | 0.85 | 3.77 | 0.88 | ||||
| Round1: KMO = 0.73, Bartlett’s test of sphericity: χ2 = 1787.81, p < 0.000,α = 0.78, 71.38%; Round2: KMO = 0.71, Bartlett’s test of sphericity: χ2 = 1790.70, p < 0.000, α = 0.75, 70.55% | ||||||||
| 2.22 | 2.49 | 82.87 | 2.93 | 2.48 | 82.81 | ||
| Atti1 Travelling now is suitable. | 2.11 | 0.93 | 2.83 | 0.92 | ||||
| Atti2 Travelling now is pleasant. | 2.49 | 0.90 | 3.14 | 0.88 | ||||
| Atti3 Travelling now is safe. | 2.07 | 0.91 | 2.83 | 0.92 | ||||
| Round1: KMO = 0.74, Bartlett’s test of sphericity: χ2 =1280.30, p < 0.000; Round2: KMO = 0.74, Bartlett’s test of sphericity: χ2 =1432.42, p < 0.000 | ||||||||
| 3.00 | 3.86 | 77.15 | 3.56 | 3.46 | 69.14 | ||
| Intent1 I plan to go to an urban park. | 3.26 | 0.84 | 3.74 | 0.76 | ||||
| Intent2 I plan to taste nearby cuisine. | 2.95 | 0.85 | 3.53 | 0.77 | ||||
| Intent3 I desire to visit short-distance tourist attractions. | 2.86 | 0.92 | 3.48 | 0.88 | ||||
| Intent4 I desire to travel to low-risk destinations. | 2.92 | 0.90 | 3.47 | 0.86 | ||||
| Intent5 I intend to visit natural scenic spots. | 3.02 | 0.89 | 3.58 | 0.87 | ||||
| Round1: KMO = 0.87, Bartlett’s test of sphericity: χ2 = 2724.70, p < 0.000; Round2: KMO = 0.85, Bartlett’s test of sphericity: χ2 = 2209.42, p < 0.000 | ||||||||
| Constructs | Round1 (N = 700) | Round2 (N = 773) | ||||||
|---|---|---|---|---|---|---|---|---|
| Travelled (n = 27) | Didn’t Travel (n = 673) | Overall Mean | One-Way ANOVA | Travelled (n = 190) | Didn’t Travel (n = 583) | Overall Mean | One-Way ANOVA | |
| Intrapersonal | 3.60 | 3.84 | 3.83 | 2.810 | 3.45 | 3.63 | 3.59 | 8.017 |
| Interpersonal | 3.78 | 3.71 | 3.71 | 0.195 | 3.11 | 3.40 | 3.33 | 21.607 |
| Structural | 3.81 | 3.98 | 3.98 | 1.728 | 3.46 | 3.76 | 3.69 | 25.425 |
| Relaxation | 4.43 | 3.91 | 3.93 | 8.204 | 4.25 | 3.96 | 4.03 | 21.389 |
| Pull motives | 4.04 | 3.36 | 3.39 | 15.612 | 3.73 | 3.34 | 3.43 | 22.548 |
| Ordinary motives | 3.85 | 3.38 | 3.40 | 7.214 | 3.78 | 3.53 | 3.60 | 15.132 |
| Peak shifting motives | 3.77 | 3.12 | 3.14 | 11.169 | 3.73 | 3.34 | 3.43 | 29.035 |
| Perceived obligation | 4.35 | 4.39 | 4.39 | 0.142 | 4.12 | 4.22 | 4.19 | 2.713 |
| Holiday spirit and denial | 3.44 | 2.82 | 2.84 | 14.678 | 3.24 | 2.96 | 3.03 | 19.016 |
| Religious faith and wish | 3.54 | 3.19 | 3.20 | 3.483 | 2.98 | 2.87 | 2.90 | 1.858 |
| Adaptive response | 4.35 | 4.39 | 4.39 | 0.142 | 3.73 | 3.73 | 3.73 | 0.005 |
| Attitude | 3.04 | 2.19 | 2.22 | 24.329 | 3.34 | 2.80 | 2.93 | 56.096 |
| Intention | 3.91 | 2.97 | 3.00 | 27.466 | 3.88 | 3.46 | 3.56 | 48.613 |
| Structural Relations | Standardized Coefficient (b) | t-Value | p | Contrast | ||||
|---|---|---|---|---|---|---|---|---|
| Round1 | Round2 | Round1 | Round2 | Round1 | Round2 | Round1 | Round2 | |
| H1 constraints → holiday spirit and denial | −0.22 | −0.13 | −5.16 | −3.25 | *** | *** | √ | √ |
| Constraints → religious faith and wish | 0.07 | 0.20 | 1.40 | 3.60 | 0.16 | *** | × | √ |
| constraints → adaptive response | 0.28 | 0.32 | 5.67 | 6.67 | *** | *** | √ | √ |
| H2 constraints → attitude | −0.31 | −0.36 | −6.94 | −8.88 | *** | *** | √ | √ |
| H3 constraints → intention | −0.05 | 0.05 | −1.17 | 1.15 | 0.24 | 0.25 | × | × |
| H4 motivation → holiday spirit and denial | 0.60 | 0.49 | 11.62 | 10.15 | *** | *** | √ | √ |
| motivation → religious | 0.44 | 0.38 | 7.73 | 5.76 | *** | *** | √ | √ |
| motivation → adaptive response | 0.48 | 0.37 | 9.10 | 7.50 | *** | *** | √ | √ |
| H5 motivation → attitude | 0.38 | 0.44 | 5.78 | 8.52 | *** | *** | √ | √ |
| H6 motivation → intention | 0.36 | 0.56 | 5.61 | 8.79 | *** | *** | √ | √ |
| H7 holiday spirit and denial → attitude | 0.21 | 0.24 | 4.37 | 5.99 | *** | *** | √ | √ |
| religious faith and wish → attitude | 0.09 | 0.09 | 1.89 | 2.12 | 0.06 | 0.03 | √ | √ |
| adaptive response → attitude | 0.06 | −0.03 | 1.24 | −0.72 | 0.21 | 0.47 | × | × |
| H8 holiday spirit and denial → intention | 0.12 | 0.08 | 2.69 | 2.03 | *** | 0.04 | √ | √ |
| religious faith and wish → intention | 0.11 | 0.01 | 2.55 | 0.11 | 0.01 | 0.91 | √ | × |
| adaptive response → intention | 0.07 | 0.00 | 1.62 | 0.08 | 0.11 | 0.94 | × | × |
| H9 perceived obligation → attitude | −0.23 | −0.06 | −7.08 | −1.85 | *** | 0.06 | √ | √ |
| H10 perceived obligation → intention | −0.03 | 0.02 | −0.96 | 0.66 | 0.34 | 0.51 | × | × |
| H11 attitude → intention | 0.29 | 0.24 | 6.06 | 4.52 | *** | *** | √ | √ |
| Mediating Effects | Total Effects | Direct Effect (CI) | Indirect Effects (CI) | Mediation Hypotheses |
|---|---|---|---|---|
| Round 1 (N = 700) | ||||
| constraint-attitude-intention | −0.346 * | −0.105 (−0.318 to 0.068) | −0.241 * (−0.391 to −0. 099) | full mediation |
| motivation-attitude-intention | 0.841 * | 0.435 * (0.267 to 0.636) | 0.406 * (0.294 to 0.561) | partial mediation |
| obligation-attitude-intention | −0.129 ** | −0.040 (−0.134 to 0.049) | −0.090 ** (−0.143 to −0.048) | full mediation |
| Round 2 (N = 773) | ||||
| constraint-attitude-intention | −0.055 ** | 0.056 (−0.046 to 0.158) | −0.111 ** (−0.181 to −0.048) | full mediation |
| motivation-attitude-intention | 0.702 * | 0.535* (0.412 to 0.701) | 0.167 ** (0.094 to 0.246) | partial mediation |
| obligation-attitude-intention | 0.005 | 0.017(−0.054 to 0.086) | −0.011 (−0.028 to 0.003) | Non-significant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, C.; Zhang, J.; Qian, L.; Zhang, Y. Risk, Obligation, and Public Noncompliance with Mobility Directives in China during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 11505. https://doi.org/10.3390/ijerph191811505
Zheng C, Zhang J, Qian L, Zhang Y. Risk, Obligation, and Public Noncompliance with Mobility Directives in China during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(18):11505. https://doi.org/10.3390/ijerph191811505
Chicago/Turabian StyleZheng, Chunhui, Jia Zhang, Lili Qian, and Yuling Zhang. 2022. "Risk, Obligation, and Public Noncompliance with Mobility Directives in China during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 18: 11505. https://doi.org/10.3390/ijerph191811505
APA StyleZheng, C., Zhang, J., Qian, L., & Zhang, Y. (2022). Risk, Obligation, and Public Noncompliance with Mobility Directives in China during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(18), 11505. https://doi.org/10.3390/ijerph191811505