
Intravenous Morphine Infusion versus Thoracic Epidural Infusion of Ropivacaine with Fentanyl after the Ravitch Procedure—A Single-Center Cohort Study



Abstract
:1. Introduction
2. Methods
2.1. Trial Design, Setting
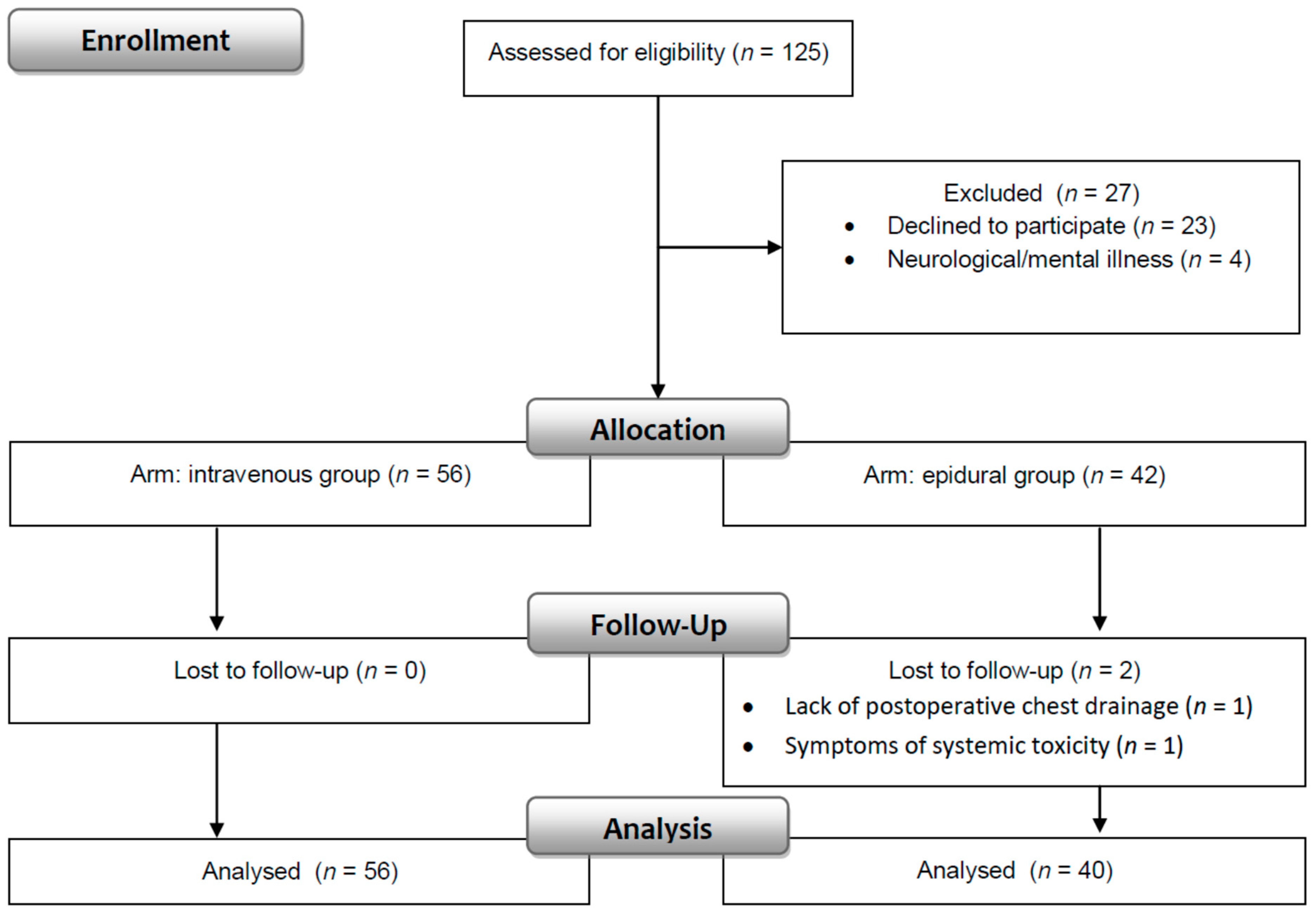
2.2. Participants
2.3. Interventions
2.3.1. Drugs
2.3.2. Epidural Catheter
2.3.3. Patient Monitoring by Nurses
2.3.4. Nurse-Controlled Analgesia
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Patients
3.2. Average and Maximum Postoperative Pain
3.3. Analgesic Consumption
3.4. Anxiety
3.5. Side Effects
3.6. Patient Satisfaction
4. Discussion
Limitations
5. Conclusions
6. Practical Implications of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CONSORT 2010 | Updated guidelines for reporting parallel group randomized trials |
| NRS | Numerical Rating Scale |
| PONV | Postoperative nausea and vomiting |
| STAI | The State-Trait Anxiety Inventory for adolescents |
| STAI-C | The State-Trait Anxiety Inventory for children between 9 and 14 years of age |
References
- Ghafoor, T.; Edsell, M.; Hunt, I. Anaesthesia for the surgical correction of chest wall deformities. BJA Educ. 2020, 20, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Buchwald, J.; Ligarski, D.; Polewczyk, T. Long-term results after the modified Ravitch procedure performed in children and adolescents—A one-time procedure without the need to use additional support of the sternum. A retrospective study. Kardiochir. Torakochir. Pol. 2020, 17, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Kolettas, A.; Lazaridis, G.; Baka, S.; Mpoukovinas, I.; Karavasilis, V.; Kioumis, I.; Pitsiou, G.; Papaiwannou, A.; Lampaki, S.; Karavergou, A.; et al. Postoperative pain management. J. Thorac. Dis. 2015, 7 (Suppl. 1), S62–S72. [Google Scholar] [CrossRef] [PubMed]
- Baratta, J.L.; Schwenk, E.S.; Viscusi, E.R. Clinical consequences of inadequate pain relief: Barriers to optimal pain management. Plast. Reconstr. Surg. 2014, 134 (Suppl. 2), 15S–21S. [Google Scholar] [CrossRef]
- Gan, T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention. J. Pain Res. 2017, 10, 2287–2298. [Google Scholar] [CrossRef]
- Gai, N.; Naser, B.; Hanley, J.; Peliowski, A.; Hayes, J.; Aoyama, K. A practical guide to acute pain management in children. J. Anesth. 2020, 34, 421–433. [Google Scholar] [CrossRef]
- Schwenk, E.S.; Mariano, E.R. Designing the ideal perioperative pain management plan starts with multimodal analgesia. Korean J. Anesthesiol. 2018, 71, 345–352. [Google Scholar] [CrossRef]
- Mijatovic, D.; Bhalla, T.; Farid, I. Post-thoracotomy analgesia. Saudi J. Anaesth. 2021, 15, 341–347. [Google Scholar] [CrossRef]
- Papic, J.C.; Finnell, S.M.; Howenstein, A.M.; Breckler, F.; Leys, C.M. Postoperative opioid analgesic use after Nuss versus Ravitch pectus excavatum repair. J. Pediatr. Surg. 2014, 49, 919–923. [Google Scholar] [CrossRef]
- Rettig, R.L.; Yang, C.J.; Ashfaq, A.; Sydorak, R.M. Cryoablation is associated with shorter length-of-stay and reduced opioid use after the Ravitch procedure. J. Pediatr. Surg. 2022, 57, 1258–1263. [Google Scholar] [CrossRef]
- Mangat, S.; Hance, L.; Ricketts, K.J.; Phillips, M.R.; Mclean, S.E. The impact of an enhanced recovery perioperative pathway for pediatric pectus deformity repair. Pediatr. Surg. Int. 2020, 36, 1035–1045. [Google Scholar] [CrossRef] [PubMed]
- Tomaszek, L.; Fenikowski, D.; Gawron, D.; Komotajtys, H. Comparative efficacy of continuous infusion of bupivacaine/fentanyl and ropivacaine/fentanyl for paediatric pain control after the Ravitch procedure and thoracotomy. A prospective randomized study. Biomed. Pap. Med. Fac. Univ. Palacky. Olomouc. Czech. Repub. 2019, 163, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Loftus, P.D.; Elder, C.T.; Russell, K.W.; Spanos, S.P.; Barnhart, D.C.; Scaife, E.R.; Skarda, D.E.; Rollins, M.D.; Meyers, R.L. Paravertebral regional blocks decrease length of stay following surgery for pectus excavatum in children. J. Pediatr. Surg. 2016, 51, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Pilkington, M.; Harbaugh, C.M.; Hirschl, R.B.; Geiger, J.D.; Gadepalli, S.K. Use of cryoanalgesia for pain management for the modified ravitch procedure in children. J. Pediatr. Surg. 2020, 55, 1381–1384. [Google Scholar] [CrossRef]
- Heo, M.H.; Kim, J.Y.; Kim, J.H.; Kim, K.W.; Lee, S.I.; Kim, K.T.; Park, J.S.; Choe, W.J.; Kim, J.H. Epidural analgesia versus intravenous analgesia after minimally invasive repair of pectus excavatum in pediatric patients: A systematic review and meta-analysis. Korean J. Anesthesiol. 2021, 74, 449–458. [Google Scholar] [CrossRef]
- Sujka, J.A.; Dekonenko, C.; Millspaugh, D.L.; Doyle, N.M.; Walker, B.J.; Leys, C.M.; Ostlie, D.J.; Aguayo, P.; Fraser, J.D.; Alemayehu, H.; et al. Epidural versus PCA Pain Management after Pectus Excavatum Repair: A Multi-Institutional Prospective Randomized Trial. Eur. J. Pediatric Surg. 2020, 30, 465–471. [Google Scholar] [CrossRef]
- Man, J.Y.; Gurnaney, H.G.; Dubow, S.R.; DiMaggio, T.J.; Kroeplin, G.R.; Adzick, N.S.; Muhly, W.T. A retrospective comparison of thoracic epidural infusion and multimodal analgesia protocol for pain management following the minimally invasive repair of pectus excavatum. Paediatr. Anaesth. 2017, 27, 1227–1234. [Google Scholar] [CrossRef]
- Gupta, A.; Jay, M.A.; Williams, G. Evolving pediatric epidural practice: An institution’s clinical experience over 20 years-A retrospective observational cohort study. Paediatr. Anaesth. 2019, 30, 25–33. [Google Scholar] [CrossRef]
- Cravero, J.P.; Agarwal, R.; Berde, C.; Birmingham, P.; Coté, C.J.; Galinkin, J.; Isaac, L.; Kost-Byerly, S.; Krodel, D.; Maxwell, L.; et al. The Society for Pediatric Anesthesia recommendations for the use of opioids in children during the perioperative period. Paediatr. Anaesth. 2019, 29, 547–571. [Google Scholar] [CrossRef] [PubMed]
- Walker, B.J.; Long, J.B.; Sathyamoorthy, M.; Birstler, J.; Wolf, C.; Bosenberg, A.T.; Flack, S.H.; Krane, E.J.; Sethna, N.F.; Suresh, S.; et al. Complications in Pediatric Regional Anesthesia: An Analysis of More than 100,000 Blocks from the Pediatric Regional Anesthesia Network. Anesthesiology 2019, 129, 721–732. [Google Scholar] [CrossRef]
- Steward, J.D. A simplified scoring system for the post-operative recovery room. Can. Anaesth. Soc. J. 1975, 22, 111–113. [Google Scholar] [CrossRef]
- Craig, D.; Carli, F. Bromage motor blockade score—A score that has lasted more than a lifetime. Can. J. Anaesth. 2018, 65, 837–838. [Google Scholar] [CrossRef] [PubMed]
- Jaworowska, A. STAI-C—State-Trait Inventory for Children; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2005. (In Polish) [Google Scholar]
- Wrześniewski, K.; Sosnowski, T.; Jaworowska, A.; Fecenec, D. State-Trait Inventory STAI. Polish Adaptation of STAI; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2011. (In Polish) [Google Scholar]
- Lenhard, W.; Lenhard, A. Computation of Effect Sizes. Available online: https://www.psychometrica.de/effect_size.html (accessed on 14 August 2022).
- Weber, T.; Mätzl, J.; Rokitansky, A.; Klimscha, W.; Neumann, K.; Deusch, E.; Medical Research Society. Superior postoperative pain relief with thoracic epidural analgesia versus intravenous patient-controlled analgesia after minimally invasive pectus excavatum repair. J. Thorac. Cardiovasc. Surg. 2007, 134, 865–870. [Google Scholar] [CrossRef]
- Nuss, D.; Kelly, R.E.; Croitoru, D.P.; Katz, M.E. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J. Pediatr. Surg. 1998, 33, 545–552. [Google Scholar] [CrossRef]
- Nasr, A.; Fecteau, A.; Wales, P.W. Comparison of the Nuss and the Ravitch procedure for pectus excavatum repair: A meta-analysis. J. Pediatr. Surg. 2010, 45, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Wordliczek, J.; Zajączkowska, R.; Dziki, A.; Jackowski, M.; Richter, P.; Woroń, J.; Misiołek, H.; Dobrogowski, J.; Paśnik, K.; Wallner, G.; et al. Postoperative pain relief in general surgery—Recommendations of the Association of Polish Surgeons, Polish Society of Anaesthesiology and Intensive Therapy, Polish Association for the Study of Pain and Polish Association of Regional Anaesthesia and Pain Treatment. Pol. J. Surg. 2019, 91, 47–68. [Google Scholar] [CrossRef]
- Zahn, J.; Eberl, S.; Rödle, W.; Rascher, W.; Neubert, A.; Toni, I. Metamizole Use in Children: Analysis of Drug Utilisation and Adverse Drug Reactions at a German University Hospital between 2015 and 2020. Paediatr. Drugs 2022, 24, 45–56. [Google Scholar] [CrossRef]
- Fieler, M.; Eich, C.; Becke, K.; Badelt, G.; Leimkühler, K.; Messroghli, L.; Boethig, D.; Sümpelmann, R. Metamizole for postoperative pain therapy in 1177 children: A prospective, multicentre, observational, postauthorisation safety study. Eur. J. Anaesthesiol. 2015, 32, 839–843. [Google Scholar] [CrossRef]
- Witschi, L.; Reist, L.; Stammschulte, T.; Erlenwein, J.; Becke, K.; Stamer, U. Perioperative Anwendung von Metamizol und anderen Nichtopioidanalgetika bei Kindern: Ergebnisse einer Umfrage [Perioperative use of metamizole and other nonopioid analgesics in children: Results of a survey]. Der Anaesthesist 2019, 68, 152–160. [Google Scholar] [CrossRef]
- Schwenkglenks, M.; Gerbershagen, H.J.; Taylor, R.S.; Pogatzki-Zahn, E.; Komann, M.; Rothaug, J.; Volk, T.; Yahiaoui-Doktor, M.; Zaslansky, R.; Brill, S.; et al. Correlates of satisfaction with pain treatment in the acute postoperative period: Results from the international PAIN OUT registry. Pain 2014, 155, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Espinel, A.G.; Shah, R.K.; McCormick, M.E.; Krakovitz, P.R.; Boss, E.F. Patient satisfaction in pediatric surgical care: A systematic review. Otolaryngol. Head Neck Surg. 2014, 150, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J.; Belani, K.G.; Bergese, S.; Chung, F.; Diemunsch, P.; Habib, A.S.; Jin, Z.; Kovac, A.L.; Meyer, T.A.; Urman, R.D.; et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2020, 131, 411–448. [Google Scholar] [CrossRef] [PubMed]
- Howard, R.F.; Lloyd-Thomas, A.; Thomas, M.; Williams, D.G.; Saul, R.; Bruce, E.; Peters, J. Nurse-controlled analgesia (NCA) following major surgery in 10,000 patients in a children’s hospital. Paediatr. Anaesth. 2010, 20, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Aronson, L.A.; Parker, G.C.; Valley, R.; Norfleet, E.A. Acute Horner syndrome due to thoracic epidural analgesia in a paediatric patient. Paediatr. Anaesth. 2000, 10, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Valois, T.; Ranger, M.; Raghavendran, S. Horner’s syndrome following thoracic epidural analgesia in children: A report of two cases. Acute Pain 2006, 8, 83–86. [Google Scholar] [CrossRef]
- Zadra, N.; Giusti, F. Horner syndrome due to thoracic epidural analgesia in children. Paediatr. Anaesth. 2000, 10, 573. [Google Scholar] [CrossRef]
- Tomaszek, L.; Fenikowski, D.; Komotajtys, H.; Gawron, D. Ropivacaine/Fentanyl vs. Bupivacaine/Fentanyl for Pain Control in Children after Thoracic Surgery: A Randomized Study. Pain Manag. Nurs. 2019, 20, 390–397. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Procedure | Name of Drug, Route, and Dose | |
|---|---|---|
| Premedication | midazolam hydrochloride (p.o.) 0.2–0.5 mg/kg | |
| Antiemetic prophylaxis | ondansetron hydrochloride (i.v.) 0.1 mg/kg up to 4 mg | |
| Pre-emptive analgesia | paracetamol (i.v.) 15 mg/kg; | |
| 1 non-steroidal anti-inflammatory drug: ibuprofen (p.r.) 10 mg/kg or ketoprofen (i.v.) 1 mg/kg | ||
| Induction of anesthesia | fentanyl (i.v.) 1–5 μg/kg | |
| propofol (i.v.) 3–5 mg/kg | ||
| 2 rocuronium bromide (i.v.) 1 mg/kg or pancuronium bromide (i.v) 0.1 mg/kg | ||
| Maintenance of anesthesia | desfluranum 8–10 vol% in an oxygen/air mixture | |
| Intraoperative analgesia | ||
| –intravenous group | fentanyl (i.v.) every 20–30 min; 1–5 μg/kg | |
| –epidural group | 2% lidocaine 2 mg/kg | |
| After 15 min | ||
| 1% ropivacaine 1–3 mg/kg | ||
| After 60 min | ||
| 0.2% ropivacaine with fentanyl 5 µg/mL; 0.1 mL/kg/per hour | ||
| Postoperative analgesia | ||
| –intravenous group | morphine 0.02–0.06 mg/kg per hour | |
| –epidural group | 0.2% ropivacaine with fentanyl 5 µg/mL; 0.1 mL/kg per hour | |
| –both groups | paracetamol (i.v.) every 6 h; maximum of 60 mg/kg daily | |
| ibuprofen (p.r.) every 8 h 10 mg/kg; up to 30 mg/kg daily or ketoprofen (i.v.) every 8 h 1 mg/kg; maximum of 200 mg daily | ||
| metamizole (rescue drug) 20 mg/kg; maximum of 2.5 g daily | ||
| 3 tramadol (i.v.) 1–2 mg/kg; maximum of 400 mg daily | ||
| Antiemetic treatment | 4 ondansetron hydrochloride (i.v.) every 8 h up to the second postoperative day; 0,1 mg/kg up to 4 mg | |
| 5 metoclopramide hydrochloride (i.v.) 0.1–0.2 mg/kg | ||
| 6 dexamethasone (i.v.) 0.15 mg/kg up to 5 mg | ||
| Variable | Intravenous | Epidural | p Value | |
|---|---|---|---|---|
| n = 56 | n = 40 | |||
| Age (years) | 14 [13; 16] | 14 [12; 15] | 0.20 | |
| Body height (cm) | 171 [164; 177] | 168 [158; 176] | 0.36 | |
| Body weight (kg) | 54 [45; 60] | 52 [44; 58] | 0.14 | |
| BMI | 18 [17; 20] | 17 [16; 19] | 0.08 | |
| Gender | Female | 6 (10.7) | 6 (15.0) | 0.54 |
| Male | 50 (89.3) | 34 (85.0) | ||
| ASA | 1 | 52 (92.9) | 27 (67.5) | 0.002 |
| 2 | 4 (7.1) | 13 (32.5) | ||
| Perioperative gabapentin | 28 (50) | 20 (50) | 1.00 | |
| Before induction | Heart rate (beat min−1) | 86 [77; 94] | 95 [86; 108] | 0.001 |
| Systolic blood pressure (mmHg) | 117 [105; 126] | 105 [94; 120] | 0.0002 | |
| Diastolic blood pressure (mmHg) | 70 [60; 76] | 60 [50; 70] | 0.018 | |
| Oxygen saturation (%) | 98 [98; 99] | 99 [98; 99] | 0.06 | |
| Duration of anesthesia (min) | 195 [178; 209] | 195 [167; 212] | 0.72 | |
| Duration of surgery (min) | 140 [126; 153] | 120 [105; 142] | 0.004 | |
| Duration of extubating (min) | 15 [10; 20] | 15 [10; 20] | 0.40 | |
| Pain | Intravenous | Epidural | Z | p Value | Effect Sizes |
|---|---|---|---|---|---|
| (Postoperative Days 0–3) | n = 56 | n = 40 | |||
| Average pain | |||||
| At rest | 0.2 [0.1; 0.4] | 0.4 [0.2; 0.9] | −2.97 | 0.003 | 0.6 |
| During deep breathing | 0.2 [0.1; 0.3] | 0.3 [0.1; 0.4] | −2.27 | 0.023 | 0.5 |
| During coughing | 0.2 [0.1; 0.4] | 0.4 [0.3; 0.5] | −2.43 | 0.015 | 0.5 |
| Maximal pain | |||||
| At rest | 1.2 [0.7; 2.2] | 2.0 [1.0; 3.5] | −3.29 | 0.001 | 0.7 |
| During deep breathing | 0.7 [0.5; 1.2] | 1.2 [0.7; 2.0] | −2.85 | 0.004 | 0.6 |
| During coughing | 1.0 [0.5; 1.5] | 1.5 [1.0; 1.7] | −2.98 | 0.003 | 0.6 |
| Anxiety | Intravenous | Epidural | p Value |
|---|---|---|---|
| n = 56 | n = 40 | ||
| Trait (sten) | 5 [3; 6] | 5 [4; 6] | 0.12 |
| State preoperative (sten) | 6 [5; 7] | 7 [6; 8] | 0.06 |
| State postoperative (sten) | 5 [4; 6] | 6 [4; 7] | 0.07 |
| Variable | Intravenous | Epidural | p Value |
|---|---|---|---|
| n = 56 | n = 40 | ||
| Nausea and vomiting | 28 (50.0) | 28 (70.0) | 0.05 |
| Urinary retention-bladder catheterization | 3 (5.4) | 0 (0.0) | 0.26 |
| Pruritus | 2 (3.6) | 3 (7.5) | 0.64 |
| Bradycardia | 2 (3.6) | 4 (10.0) | 0.23 |
| Dizziness | 1 (1.8) | 1 (2.5) | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fenikowski, D.; Tomaszek, L. Intravenous Morphine Infusion versus Thoracic Epidural Infusion of Ropivacaine with Fentanyl after the Ravitch Procedure—A Single-Center Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 11291. https://doi.org/10.3390/ijerph191811291
Fenikowski D, Tomaszek L. Intravenous Morphine Infusion versus Thoracic Epidural Infusion of Ropivacaine with Fentanyl after the Ravitch Procedure—A Single-Center Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(18):11291. https://doi.org/10.3390/ijerph191811291
Chicago/Turabian StyleFenikowski, Dariusz, and Lucyna Tomaszek. 2022. "Intravenous Morphine Infusion versus Thoracic Epidural Infusion of Ropivacaine with Fentanyl after the Ravitch Procedure—A Single-Center Cohort Study" International Journal of Environmental Research and Public Health 19, no. 18: 11291. https://doi.org/10.3390/ijerph191811291
APA StyleFenikowski, D., & Tomaszek, L. (2022). Intravenous Morphine Infusion versus Thoracic Epidural Infusion of Ropivacaine with Fentanyl after the Ravitch Procedure—A Single-Center Cohort Study. International Journal of Environmental Research and Public Health, 19(18), 11291. https://doi.org/10.3390/ijerph191811291