
High Temperatures and Cardiovascular-Related Morbidity: A Scoping Review

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
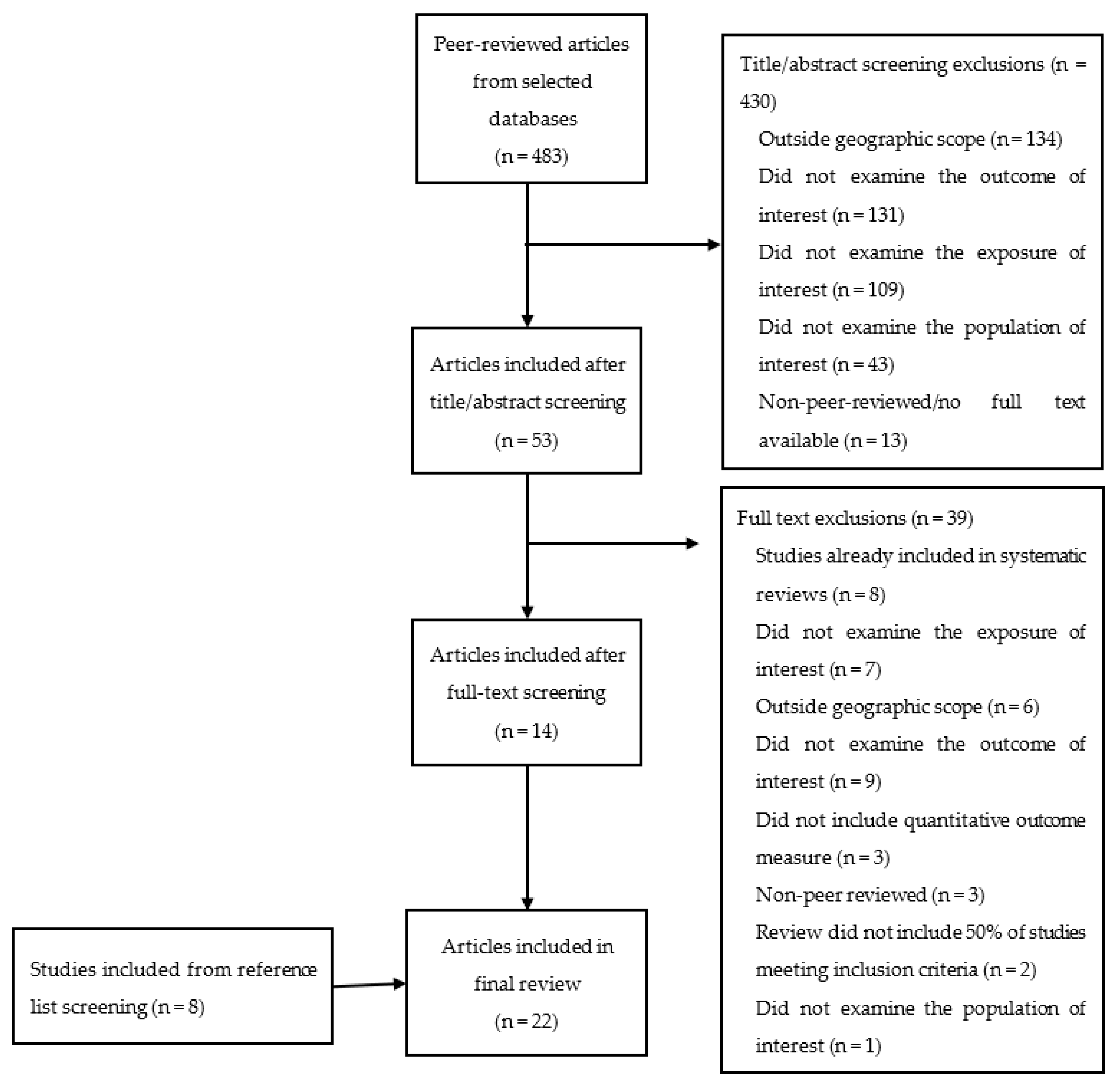
2.2. Eligibility Criteria and Screening Process
2.3. Data Extraction
2.4. Synthesis of Results
3. Results
3.1. Study Designs and Data Analysis
3.2. Populations and Locations
3.3. Exposures
3.4. Risk Factors and Confounders
3.5. Outcomes
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Research Gaps
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohen, S.; Bush, E.; Zhang, X.; Gillett, N.; Bonsal, B.; Derksen, C.; Flato, G.; Greenan, B.; Watson, E. Synthesis of Findings for Canada’s Regions; Chapter 8 in Canada’s Changing Climate Report; Bush EaL, D.S., Ed.; Government of Canada: Ottawa, ON, Canada, 2019; pp. 424–443. [Google Scholar]
- Ebi, K.L.; Capon, A.; Berry, P.; Broderick, C.; de Dear, R.; Havenith, G.; Honda, Y.; Kovats, R.S.; Ma, W.; Malik, A.; et al. Hot weather and heat extremes: Health risks. Lancet 2021, 398, 698–708. [Google Scholar] [CrossRef]
- The Intergovernmental Panel on Climate Change. Global Warming of 1.5 Degrees Celsius. Special Report. Summary for Policy Makers. 2018. Available online: https://www.ipcc.ch/sr15/chapter/spm/ (accessed on 19 July 2021).
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8, 40. [Google Scholar] [CrossRef]
- Moghadamnia, M.T.; Ardalan, A.; Mesdaghinia, A.; Keshtkar, A.; Naddafi, K.; Yekaninejad, M.S. Ambient temperature and cardiovascular mortality: A systematic review and meta-analysis. PeerJ 2017, 5, e3574. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; FitzGerald, G.; Guo, Y.; Jalaludin, B.; Tong, S. Impact of heatwave on mortality under different heatwave definitions: A systematic review and meta-analysis. Environ. Int. 2016, 89–90, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Mengersen, K.; Wang, X.; Ye, X.; Guo, Y.; Pan, X.; Tong, S. Daily average temperature and mortality among the elderly: A meta-analysis and systematic review of epidemiological evidence. Int. J. Biometeorol. 2012, 56, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Xu, Z.; Bambrick, H.; Prescott, V.; Wang, N.; Zhang, Y.; Su, H.; Tong, S.; Hu, W. Cardiorespiratory effects of heatwaves: A systematic review and meta-analysis of global epidemiological evidence. Environ. Res. 2019, 177, 108610. [Google Scholar] [CrossRef] [PubMed]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Huynen, M.M.; Martens, P.; Schram, D.; Weijenberg, M.P.; Kunst, A.E. The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ. Health Perspect. 2001, 109, 463–470. [Google Scholar] [CrossRef]
- Basu, R.; Samet, J.M. Relation between elevated ambient temperature and mortality: A review of the epidemiologic evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef]
- Gabriel, K.M.; Endlicher, W.R. Urban and rural mortality rates during heat waves in Berlin and Brandenburg, Germany. Environ. Pollut. 2011, 159, 2044–2050. [Google Scholar] [CrossRef]
- Gouveia, N.; Hajat, S.; Armstrong, B. Socioeconomic differentials in the temperature-mortality relationship in Sao Paulo, Brazil. Int. J. Epidemiol. 2003, 32, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Kovats, R.S.; Hajat, S. Heat stress and public health: A critical review. Ann. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. Urban Population (% of total population)-Canada-United Nations Population Division. World Urbanization Prospects. 2018. Available online: https://data.worldbank.org/indicator/SP.URB.TOTL.IN.ZS?end=2019&locations=CA&start=2011 (accessed on 19 July 2021).
- Phung, D.; Thai, P.K.; Guo, Y.; Morawska, L.; Rutherford, S.; Chu, C. Ambient temperature and risk of cardiovascular hospitalization: An updated systematic review and meta-analysis. Sci. Total Environ. 2016, 550, 1084–1102. [Google Scholar] [CrossRef]
- Canadian Institute for Health Information. Inpatient Hospitalizations, Surgeries, Newborns and Childbirth Indicators, 2016–2017. 2018. Available online: https://www.cihi.ca/sites/default/files/document/hospch-hosp-2016-2017-snapshot_en.pdf (accessed on 5 November 2020).
- Thériault, L.; Stonebridge, C.; Browarski, S. The Canadian Heart Health Strategy: Risk Factors and Future Cost Implications. 2010. Available online: https://www.conferenceboard.ca/e-library/abstract.aspx?did=3447 (accessed on 5 November 2020).
- Public Health Agency of Canada. Prevalence of Chronic Diseases among Canadian Adults. 2019. Available online: https://www.canada.ca/en/public-health/services/chronic-diseases/prevalence-canadian-adults-infographic-2019.html (accessed on 14 June 2021).
- Climate Atlas of Canada. Urban Heat Island Effect. 2022. Available online: https://climateatlas.ca/urban-heat-island-effect (accessed on 5 July 2022).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Hajat, S.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. Effects of ambient temperature on the incidence of myocardial infarction. Heart 2009, 95, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklov, J.; Hajat, S.; Sauerborn, R. Effects of Air Temperature on Climate-Sensitive Mortality and Morbidity Outcomes in the Elderly; a Systematic Review and Meta-analysis of Epidemiological Evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef]
- Sun, Z.; Chen, C.; Xu, D.; Li, T. Effects of ambient temperature on myocardial infarction: A systematic review and meta-analysis. Environ. Pollut. 2018, 241, 1106–1114. [Google Scholar] [CrossRef]
- Turner, L.R.; Barnett, A.G.; Connell, D.; Tong, S. Ambient temperature and cardiorespiratory morbidity: A systematic review and meta-analysis. Epidemiology 2012, 23, 594–606. [Google Scholar] [CrossRef] [PubMed]
- Adeyeye, T.E.; Insaf, T.Z.; Al-Hamdan, M.Z.; Nayak, S.G.; Stuart, N.; DiRienzo, S.; Crosson, W.L. Estimating policy-relevant health effects of ambient heat exposures using spatially contiguous reanalysis data. Environ. Health 2019, 18, 35. [Google Scholar] [CrossRef] [PubMed]
- Rowland, S.T.; Boehme, A.K.; Rush, J.; Just, A.C.; Kioumourtzoglou, M.A. Can ultra short-term changes in ambient temperature trigger myocardial infarction? Environ. Int. 2020, 143, 105910. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.; Talbott, E.O.; Kan, H.; Prins, C.A.; Xu, X. The effects of heat stress and its effect modifiers on stroke hospitalizations in Allegheny County, Pennsylvania. Int. Arch. Occup. Environ. Health 2014, 87, 557–565. [Google Scholar] [CrossRef]
- Chen, T.; Sarnat, S.E.; Grundstein, A.J.; Winquist, A.; Chang, H.H. Time-series Analysis of Heat Waves and Emergency Department Visits in Atlanta, 1993 to 2012. Environ. Health Perspect. 2017, 125, 057009. [Google Scholar] [CrossRef] [PubMed]
- Sohail, H.; Kollanus, V.; Tiittanen, P.; Schneider, A.; Lanki, T. Heat, Heatwaves and Cardiorespiratory Hospital Admissions in Helsinki, Finland. Int. J. Environ. Res. Public Health 2020, 17, 7892. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Solanas, E.; Basagana, X. Temporal changes in the effects of ambient temperatures on hospital admissions in Spain. PLoS ONE 2019, 14, e0218262. [Google Scholar] [CrossRef]
- Corcuera Hotz, I.; Hajat, S. The Effects of Temperature on Accident and Emergency Department Attendances in London: A Time-Series Regression Analysis. Int. J. Environ. Res. Public Health 2020, 17, 1957. [Google Scholar] [CrossRef] [PubMed]
- Isaksen, T.B.; Yost, M.G.; Hom, E.K.; Ren, Y.; Lyons, H.; Fenske, R.A. Increased hospital admissions associated with extreme-heat exposure in King County, Washington, 1990–2010. Rev. Environ. Health 2015, 30, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, E.; Gasparrini, A.; Wang, X.; Chen, H.; Yagouti, A.; Fleury, M.D.; Cakmak, S. Extreme ambient temperatures and cardiorespiratory emergency room visits: Assessing risk by comorbid health conditions in a time series study. Environ. Health A Glob. Access Sci. Source 2014, 13, 5. [Google Scholar] [CrossRef]
- Bai, L.; Li, Q.; Wang, J.; Lavigne, E.; Gasparrini, A.; Copes, R.; Yagouti, A.; Burnett, R.T.; Goldberg, M.S.; Villeneuve, P.J.; et al. Hospitalizations from Hypertensive Diseases, Diabetes, and Arrhythmia in Relation to Low and High Temperatures: Population-Based Study. Sci. Rep. 2016, 6, 30283. [Google Scholar] [CrossRef]
- Bayentin, L.; El Adlouni, S.; Ouarda, T.B.; Gosselin, P.; Doyon, B.; Chebana, F. Spatial variability of climate effects on ischemic heart disease hospitalization rates for the period 1989-2006 in Quebec, Canada. Int. J. Health Geogr. 2010, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Gebhard, C.; Gebhard, C.E.; Stahli, B.E.; Maafi, F.; Bertrand, M.J.; Wildi, K.; Fortier, A.; Galvan Onandia, Z.; Toma, A.; Zhang, Z.W.; et al. Weather and risk of ST-elevation myocardial infarction revisited: Impact on young women. PLoS ONE 2018, 13, e0195602. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Conde, J.; Ois, A.; Gomis, M.; Rodriguez-Campello, A.; Cuadrado-Godia, E.; Subirana, I.; Roquer, J. Weather as a trigger of stroke. Daily meteorological factors and incidence of stroke subtypes. Cereb. Dis. 2008, 26, 348–354. [Google Scholar] [CrossRef]
- Pintaric, S.; Zeljkovic, I.; Pehnec, G.; Nesek, V.; Vrsalovic, M.; Pintaric, H. Impact of meteorological parameters and air pollution on emergency department visits for cardiovascular diseases in the city of Zagreb, Croatia. Arh. Hig. Rada. Toksikol. 2016, 67, 240–246. [Google Scholar] [CrossRef]
- Guirguis, K.; Gershunov, A.; Tardy, A.; Basu, R. The Impact of Recent Heat Waves on Human Health in California. J. Appl. Meteorol. Clim. 2014, 53, 3–19. [Google Scholar] [CrossRef]
- Fuhrmann, C.M.; Sugg, M.M.; Konrad, C.E., 2nd; Waller, A. Impact of Extreme Heat Events on Emergency Department Visits in North Carolina (2007–2011). J. Commun. Health 2016, 41, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Zacharias, S.; Koppe, C.; Mücke, H.-G. Influence of Heat Waves on Ischemic Heart Diseases in Germany. Climate 2014, 2, 133–152. [Google Scholar] [CrossRef]
- Kenney, W.L.; Craighead, D.H.; Alexander, L.M. Heat waves, aging, and human cardiovascular health. Med. Sci Sports Exerc. 2014, 46, 1891–1899. [Google Scholar] [CrossRef]
- Revich, B.; Shaposhnikov, D. Excess mortality during heat waves and cold spells in Moscow, Russia. Occup. Environ. Med. 2008, 65, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Vu, A.; Rutherford, S.; Phung, D. Heat Health Prevention Measures and Adaptation in Older Populations-A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4370. [Google Scholar] [CrossRef] [PubMed]
- Manfroi, W.C.; Peukert, C.; Berti, C.B.; Noer, C.; Gutierres Dde, A.; Silva, F.T. Acute myocardial infarction: The first manifestation of ischemic heart disease and relation to risk factors. Arq. Bras. Cardiol. 2002, 78, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Havenith, G. Temperature Regulation, Heat Balance and Climatic Stress. In Extreme Weather Events and Public Health Responses; Kirch, W., Bertollini, R., Menne, B., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; pp. 69–80. [Google Scholar]
- Appelros, P.; Stegmayr, B.; Terent, A. Sex differences in stroke epidemiology: A systematic review. Stroke 2009, 40, 1082–1090. [Google Scholar] [CrossRef]
- Gifford, R.M.; Todisco, T.; Stacey, M.; Fujisawa, T.; Allerhand, M.; Woods, D.R.; Reynolds, R.M. Risk of heat illness in men and women: A systematic review and meta-analysis. Environ. Res. 2019, 171, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Wolff, R.; Yu, W.; Vaneckova, P.; Pan, X.; Tong, S. Ambient temperature and morbidity: A review of epidemiological evidence. Environ. Health Perspect. 2012, 120, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Phelan, P.E.; Kaloush, K.; Miner, M.; Golden, J.; Phelan, B.; Silva, H.; Taylor, R.A. Urban Heat Island: Mechanisms, Implications, and Possible Remedies. Ann. Rev. Environ. Res. 2015, 40, 285–307. [Google Scholar] [CrossRef]


{kind=link}
| Study | Study Design | Location and Study Period | Sample Size | Exposure | Outcome | Risk Factors and Confounders | Key Findings |
|---|---|---|---|---|---|---|---|
| Adeyeye et al. [26] | Case crossover | EDs and hospitals in New York State, USA Summer months 2008–2012 | nheat stress = 8703 ndehydration = 59,828 nCVD = 827,051 | Ambient temperature (maximum, heat index) Measured daily | Risk Ratio CVD, heat stress, and dehydration | Risk factors/effect modifiers: urbanicity, race, ethnicity, pre-existing chronic illnesses, ozone, PM2.5, the month of exposure Confounders: individual time-invariant factors, day of the week, season |
-For every 1 °C increase in maximum temperature, the risk for ED visits statistically significantly increased after a lag of 4–7 days. -Presence of pre-existing CVD was not associated with high temperatures and heat stress/dehydration. |
| Bai et al. [35] | Time series | Hospitals in Ontario, Canada 1996–2013 | nhypertension = 50,788; narrhytmia = 345,052 | Ambient temperature (average: mild heat between optimum temperature and 97.5th percentile) and extreme heat (higher than the 97.5th percentile). Measured hourly | Cumulative relative risk; attributable fraction Hypertension, arrhythmia | Risk factors/effect modifiers: age, sex, comorbid conditions, intake of anti-hypertensive medications Confounders: NO2, O3, humidity, influenza, holiday effects, day of the week | -High temperatures were not statistically significantly associated with hypertension or arrythmia hospitalizations in Ontario. |
| Bayentin et al. [36] | Time series | Hospitals in Quebec, Canada 1989–2006 | 15 health regions | Ambient temperature (average) Measured daily | Percent change IHD | Risk factors/effect modifiers: age, sex, health region, dew-point temperature Confounders: relative humidity, precipitation, atmospheric pressure, ground snow, time trends, day of the season |
-Hot episodes during summer months were associated with increases in IHD hospital admissions but also showed decreased risks in particular regions. -Differences in risk were present for women aged 45–64 compared to men of the same age. |
| Bhaskaran et al. [22] | Systematic review | Hospitals and EDs in North America, Europe, Asia, Australia Searched database inception-2009 | 19 studies | Ambient temperature (minimum, maximum, or average) | Narrative synthesis MI | Assessed studies for adjustment for air pollution and other potential confounders | -Both hot and cold weather appeared to have detrimental effects on the short-term risk of MI. |
| Bunker et al. [23] | Systematic review and meta-analysis | Hospitals in North America, South America, Europe, Asia, Australia Searched databases 1 January 1975–24 July 2015 | ncerebrovasular = 8 studies included in meta-analysis ncardiovascular = 11 studies included in meta-analysis | Ambient temperature, apparent temperature, diurnal temperature range | Percent change in risk Total cerebrovascular, ischemic stroke, haemorrhage, total CVD, MI | Risk factors/effect modifiers: age Confounders: lag days, temperature variables, type of hospital admission, outcome classification |
-Ambient temperature was not found to statistically significantly increase the risk for cerebrovascular or cardiovascular morbidity -There was a significant association between ambient temperature and CVD and cerebrovascular mortality. |
| Chen et al. [29] | Time series | EDs in Atlanta metropolitan area, USA Warm season between 1993 and 2012 | N = 9,856,015 | Heat waves (temperatures exceeding 98th percentile for 2 or more consecutive days) Measured daily | Relative risk Total circulatory, hypertension, IHD, dysrhythmia, congestive heart failure, ischemic stroke | Risk factors/effect modifiers: continuous air temperature, dew-point temperature, CVD subtype Confounders: day of the week, holidays, and time trends |
-Minimum and maximum temperature during heat waves can increase the morbidity risk of specific CVDs. -Minimum temperature-defined heat waves were associated with statistically significant increases in ED visits for total circulatory disease, hypertension, IHD, dysrhythmia, and ischemic stroke. -Maximum temperature-defined heat waves were statistically significantly associated with increases in hypertension and ischemic stroke. -Some CVDs are associated with immediate changes in morbidity, while others displayed a one-day lag. |
| Fuhrmann et al. [41] | t-test | EDs in North Carolina, USA Warm season between 2007 and 2011 | N = 100 counties in North Carolina | Heat waves (at least one heat product issued and verified across four or more NWS county warning areas for five or more consecutive days) Measured daily | Percent change Total CVD, IHD, AMI, dysrhythmia, heart failure, hemorrhagic stroke, ischemic stroke, aneurysm, hypotension | Confounders: day of the week, day in season | -The number of ED visits for total CVD was significantly elevated during all three heat waves; however, examining specific subtypes of CVD, only the risk of hypotension and IHD statistically significantly increased, and only during specific heat waves. |
| Gebhard et al. [37] | Single centre retrospective study | Montreal Heart Institute in Montreal, Canada 2010–2014 | N = 2199 | Ambient temperature (maximal, >15 °C); season; daylight (>12 h) Measured daily | Relative risk STEMI | Risk factors/effect modifiers: cardiovascular risk factors, age, sex Confounders: total rain, total snowfall, relative humidity, wind speed | -The effect of high temperatures on STEMI was age and sex-dependent. High temperatures may be associated with an increased risk of STEMI among young women less than 55 years, compared to older women or men. |
| Guirguis et al. [40] | Observational study using canonical correlation | Acute care facilities in California, USA Warm season between 1999 and 2009 | N = 6 California subregions | Heat waves (periods where there is a significant correlation between temperature and health outcomes in addition to strong temperature and health anomalies) Measured daily | Percent change Total CVD, IHD, AMI, dysrhythmia, hypertension, ischemic stroke | Risk factors/effect modifiers: age, race/ethnicity Confounders: viral activity, weekends and holidays, long-term trends | -On average, hospital admissions increased 7% on peak heat wave days, with statistically significant increases in admissions for total CVD and all subtypes excluding essential hypertension. |
| Ha et al. [28] | Case crossover | Hospitals in Allegheny County, USA Warm season between 1994 and 2000 | N = 12,195 | Extreme heat (temperature greater than the 95th percentile); heat waves (two or more consecutive heat days) Measured daily | Odds ratio Total stroke, ischemic stroke, hemorrhagic stroke | Risk factors/effect modifiers: type of stroke; gender; age Confounders: time-invariant factors, air pollution, relative humidity |
-Heat waves had a greater effect on stroke hospitalizations than heat days, demonstrating a lag effect for total stroke and ischemic stroke. -Hemorrhagic stroke does not appear to be affected by high temperatures. -Men and those 80 years and older may be more susceptible to stroke hospitalization during heat days or heat waves than the general population. |
| Hotz and Hajat [32] | Time series | EDs in Greater London, UK April 2007–March 2012 | n = 13,400,000 | Ambient temperature (average) Measured daily | Percent change Total CVD, cerebrovascular disease | Risk factors/effect modifiers: deprivation levels, age Confounders: influenza, PM10, ozone, day of the week, public holidays, humidity | -There was a small but statistically significant increase in cardiac and cerebrovascular ED visits associated with a 1 °C increase in daily average temperatures. |
| Isaksen et al. [33] | Time series | King County hospitals in Washington, USA Warm season between 1990 and 2010 | N = 752,151 | Extreme heat (day with the temperature reaching the 99th percentile) Measured daily | Relative risk/percent change Circulatory disease, total CVD, IHD, cerebrovascular disease | Risk factors/effect modifiers: age, gender, nighttime temperature Confounders: SES, synoptic weather type, admission source, admission type |
-Heat, expressed as humidex, was statistically significantly associated with increased hospital admissions for circulatory disease and CVD, but only among those 85 years or older. CVD admissions also significantly decreased among those 45–64 years old. -No significant association between high temperatures and IHD or cerebrovascular disease for age groups studied. |
| Jimenez-Conde et al. [38] | Observational study | Hospital del Mar in Barcelona, Spain 2001–2003 | N = 1286 | Ambient temperature (minimum, average, maximum) Measured daily | Relative risk All strokes, non-lacunar strokes, lacunar strokes, intracerebral hemorrhage | Risk factors/effect modifiers: stroke subtype Confounders: season, air pressure variations, daily meteorological variables |
-Temperature change did not have a significant effect on stroke incidence after controlling for meteorological variables. -Most variations in incidence could be explained by variations in air pressure as opposed to temperature. |
| Lavigne et al. [34] | Time series | EDs in Toronto, Canada 2002–2010 | nrespiratory = 562,738 nCVD = 292,666 | Extreme temperature (day with the temperature reaching the 99th percentile) Measured daily | Relative risk CVD, respiratory disease | Risk factors/effect modifiers: comorbid health conditions Confounders: influenza, air pollution, relative humidity, seasonal effects, sub-seasonal cycles, and long-term trends | -Underlying hypertension or cardiac diseases did not significantly increase the risk of CVD or respiratory ED visits during extreme temperatures; however, underlying diabetes significantly increased the risk of CVD ED visits. |
| Martínez-Solanas and Basagaña [31] | Time series | Hospitals in Spain 1997–2013 | ncardiovascular = 4,475,984 ncerebrovascular = 1,320,418 | Extreme temperature (day with the temperature reaching the 99th percentile) Measured daily | Percent change Total CVD, cerebrovascular disease | Risk factors/effect modifiers: age, sex Confounders: seasonality, day of the week, holidays, influenza |
-Heat days were associated with a statistically significant decrease in CVD hospitalizations. -Cerebrovascular hospitalizations increased for most age groups; however, were not statistically significant. |
| Phung et al. [16] | Systematic review and meta-analysis | Hospitals in North America, Europe, Australia, Asia Does not state the publication range searched for eligible studies | N = 64 studies | Ambient temperature/heat wave/cold spell | Pooled relative risk Total CVD | Confounding included in the quality appraisal of studies | -There was a statistically significant increase in CVD hospitalizations during a heat wave; however, these findings did not extend to heat exposure (i.e., high temperatures that do not reach heat wave intensity or duration). |
| Pintaric et al. [39] | Observational study | University hospital EDs in Zagreb, Croatia 2008–2010 | N = 20,228 at 2 sites | Atmospheric temperature (average) Measured daily | Spearman’s rank correlation Total CVD | Confounders: air pollution, seasons, atmospheric pressure, relative humidity | -Temperature was statistically significantly negatively correlated with CVD-related ED visits. |
| Rowland et al. [27] | Time stratified case-crossover | Hospitals in New York State, USA 2000–2015 | n = 791,695 admissions | Ambient temperature (average) Measured hourly | Percent change AMI | Risk factors/effect modifiers: age, sex, time of day, season, relative humidity, first/recurrent status Confounders: residential ZIP code, year, month, day of the week, hour of day |
-Increases in hourly ambient temperature may be associated with an increased risk of MI among men and those experiencing first MI. -Temperature demonstrated a decreasing risk as lag time increased. -While high temperatures may be associated with an increased risk of MI in the afternoon, evening, and night, it had a protective effect against MIs occurring in the morning. |
| Sohail et al. [30] | Time series | Hospitals in Helsinki, Finland June 2001–August 2017 | Does not state | Ambient temperature (average), heat wave (four or more consecutive days with the temperature reaching the 90th percentile or three or more consecutive days with the temperature reaching the 95th percentile) Measured daily | Percent change Total CVD, AMI, IHD, cerebrovascular disease, arrhythmia | Risk factors/effect modifiers: age Confounders: NO2, O3, PM10, PM2.5, relative humidity, barometric pressure, pollen | -Ambient temperature was not significantly associated with any changes in disease outcomes; however, heat waves appeared to be statistically significantly associated with an increased risk of AMI among those 65–74 years and a decreased risk of arrhythmia and cerebrovascular disease hospitalizations among those less than 75 years and 18–64 years, respectively. |
| Sun et al. [24] | Systematic review and meta-analysis | Hospitals in North America, Europe, Asia Search conducted 31 August 2017, and included studies from database inception to search date | N = 13 studies included in the meta-analysis for heat exposure | Ambient temperature (minimum, average, maximum) | Pooled relative risk AMI | Risk factors/effect modifiers: temperature, latitude, lag days Confounding included in the quality appraisal of studies |
-Increasing ambient temperature was found to be statistically significantly associated with AMI hospitalizations. -A one degree increase in latitude was statistically significantly associated with a decreased risk of AMI during exposure to high ambient temperature. |
| Turner et al. [25] | Systematic review and meta-analysis | Hospitals in North America, Europe, Australia, Asia Search conducted October 2010–January 2012 and included studies from database inception to current search | N = 21 studies | Ambient temperature | Pooled relative risk Total CVD, stroke, acute coronary syndrome/MI | Risk factors/effect modifiers: lagged effects, latitude Confounding included in the quality appraisal of studies | -No apparent association was found between increases in ambient temperature and cardiovascular morbidity. |
| Zacharias et al. [42] | t-test | Hospitals in 19 regions in Germany 2001–2010 | N = 14,959,190 | Heat wave (three or more consecutive days with the temperature exceeding the 97.5th percentile) Measured hourly | Percent change IHD | Risk factors/effect modifiers: gender, subgroups of ischemic diseases, geographic region Confounders: long-term trends, seasonal fluctuations | -Heat waves had no observed influence on hospital admissions due to IHD, although authors did report a significant increase in IHD mortality. |
| Exposures | Total CVD | Hypertension | Hypotension | IHD | AMI | Dysrhythmia | Heart Failure | Cerebrovascular Disease | Heat Stress and Dehydration | Total Respiratory |
|---|---|---|---|---|---|---|---|---|---|---|
| Ambient temperature | 6 | 1 | 0 | 2 | 6 | 1 | 0 | 5 | 1 | 0 |
| Apparent temperature | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 |
| Atmospheric temperature | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Heat wave | 5 | 2 | 2 | 5 | 3 | 4 | 2 | 5 | 0 | 0 |
| Heat day | 3 | 1 | 0 | 1 | 0 | 1 | 0 | 3 | 0 | 1 |
| High-Temperature Exposure | Cardiovascular Disease | Statistical Significance | |||
|---|---|---|---|---|---|
| Significant (+) | Nonsignificant (+) | Significant (−) | Nonsignificant (−) | ||
| Ambient temperature | Total CVD | Adeyeye et al. [26]: lag4,6,7 Hotz and Hajat [32] | Bunker et al. [23] Sohail et al. [30]: 65–74 | Adeyeye et al. [26]: lag0–1 | Phung et al. [16] Sohail et al. [30]: 18–64, 75+ Turner et al. [25] |
| Hyper/hypotension | Adeyeye et al. [26] a Bai et al. [35] | ||||
| Ischemic Heart Disease | Bayentin et al. [36]: women 45–64 compared to men 45–64 | Sohail et al. [30] | |||
| Acute Myocardial Infarction | Bhaskaran et al. [22]: 7/13 studies Gebhard et al. [37]: women ≤ 55 years Rowland et al. [27]: lag0–5 (males, all ages, afternoon, evening, night, first-time AMI) Sun et al. [24] | Rowland et al. [27]: lag0–5 (females), lag0–47 (females, males, all ages, night MI, first MI) Sohail et al. [30]: 65–74, 75+ Turner et al. [25] | Gebhard et al. [37]: men ≤ 55 years during temperatures > 15 °C or daylight > 12 h Rowland et al. [27]: lag0–5 and lag0–47 (morning MI) | Adeyeye et al. [26] a Bunker et al. [23] Gebhard et al. [37]: men ≤ 55 years during spring/summer Rowland et al. [27]: lag0–5 (recurrent MI), lag0–47 (afternoon MI, evening MI, recurrent MI) Sohail et al. [30]: 18–64 years | |
| Dysrhythmia | Sohail et al. [30]: 65–74 | Sohail et al. [30]: 18–64, 75+ | |||
| Heart Failure | Adeyeye et al. [26] a | ||||
| Total Stroke | Hotz and Hajat [32] | Bunker et al. [23] Sohail et al. [30] Turner et al. [25] | |||
| Ischemic Stroke | Bunker et al. [23] | Jimenez-Conde et al. [38] | |||
| Hemorrhagic Stroke | Jimenez-Conde et al. [38] | Bunker et al. [23] | |||
| Apparent temperature | Total CVD | Adeyeye et al. [26]: lag4,6,7 | Bunker et al. [23] | Adeyeye et al. [26]: lag0–1 | Adeyeye et al. [26]: lag2 |
| Acute Myocardial Infarction | Bunker et al. [23] | ||||
| Total Stroke | Bunker et al. [23] | ||||
| Ischemic Stroke | Bunker et al. [23] | ||||
| Hemorrhagic Stroke | Bunker et al. [23] | ||||
| Atmospheric temperature | Total CVD | Pintaric et al. [39] | |||
| Heat day | Total CVD | Isaksen et al. [33]: percent change in hospitalizations among those 85 years+, circulatory and cardiovascular | Lavigne et al. [34] b: lag0–1 respiratory ED visit | Isaksen et al. [33]: percent change in hospitalizations among those 45–64 years, cardiovascular Martínez-Solanas and Basagaña [31]: 16–84 years | Isaksen et al. [33]: RR estimate, the percent change in hospitalizations among those 45–84 years, circulatory Lavigne et al. [34] b: CVD ED, lag0–13 respiratory ED visit Martínez-Solanas and Basagaña [31]: 85+ years |
| Hyper/hypotension | Lavigne et al. [34] b Bai et al. [35] | ||||
| Ischemic Heart Disease | Isaksen et al. [33]: percent change in hospitalizations among those 65–85+ years | Isaksen et al. [33]: RR estimate, the percent change in hospitalizations among those 45–64 years | |||
| Dysrhythmia | Bai et al. [35]: compared to minimum morbidity temperature percentile | Bai et al. [35]: compared to the 75th percentile | |||
| Total Stroke | Ha et al. [28]: lag 2 | Isaksen et al. [33]: RR estimate, percent change in hospitalizations among those 45–64 and 85+ years Ha et al. [28]: lag2 Martínez-Solanas and Basagaña [31]: 16–64 years, 85+ years | Ha et al. [28]: lag0,1,3 Isaksen et al. [33]: percent change in hospitalizations among those 65–84 years Martínez-Solanas and Basagaña [31]: 75–84 years | ||
| Ischemic Stroke | Ha et al. [28]: lag2–3 | Ha et al. [28]: lag0–1 | |||
| Hemorrhagic Stroke | Ha et al. [28] | ||||
| Heat wave | Total CVD | Chen et al. [29]: heat wave defined by minimum temperature Fuhrmann et al. [41] Guirguis et al. [40] Phung et al. [16] | Chen et al. [29]: heat wave defined by the maximum temperature Sohail et al. [30]: 65–74 (all, short heat waves defined by 90th percentile), 75+ (long heat waves defined by 90th percentile; heat waves defined by 95th percentile) | Sohail et al. [30]: 18–64 (all, short, long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 65–74 (long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 75+ (all, short heat waves defined by 90th percentile) | |
| Hyper/hypotension | Chen et al. [29]: heat wave defined by the maximum temperature, lag0; heat wave defined by minimum temperature, lag1 Fuhrmann et al. [41]: 2007 heat wave | Chen et al. [29]: heat wave defined by the maximum temperature, lag1; heat wave defined by minimum temperature, lag0 Fuhrmann et al. [41]: 2008 and 2011 heat wave Guirguis et al. [40] | |||
| Ischemic Heart Disease | Fuhrmann et al. [41]: 2007 and 2008 heat wave Guirguis et al. [40] Chen et al. [29]: heat wave defined by minimum temperature | Fuhrmann et al. [41]: 2011 heat wave Chen et al. [29]: heat wave defined by the maximum temperature, lag0 Sohail et al. [30]: 18–64 (short heat waves defined by 90th percentile), 65–74 (all, short heat waves defined by 90th percentile; heat waves defined by 95th percentile), 75+ (short heat waves defined by 90th percentile; heat waves defined by 95th percentile) Zacharias et al. [42]: ±2.5% excess hospital admissions | Chen et al. [29]: heat wave defined by the maximum temperature, lag1 Sohail et al. [30]: 18–64 (all, long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 65–74 (long heat waves defined by 90th percentile), 75+ (all, long heat waves defined by 90th percentile) Zacharias et al. [42]: ±2.5% excess hospital admissions | ||
| Acute Myocardial Infarction | Guirguis et al. [40] Sohail et al. [30]: 65–74 (short heat waves defined by 90th percentile) | Fuhrmann et al. [41] Sohail et al. [30]: 18–64 (short heat waves defined by 90th percentile), 65–74 (all heat waves defined by 90th percentile; heat waves defined by 95th percentile), 75+ (short heat waves defined by 90th percentile; heat waves defined by 95th percentile) | Sohail et al. [30]: 18–64 (all, long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 65–74 (long heat waves defined by 90th percentile), 75+ (all, long heat waves defined by 90th percentile) | ||
| Dysrhythmia | Guirguis et al. [40] Chen et al. [29]: heat waves defined by minimum temperature, lag0 | Chen et al. [29]: heat waves defined by minimum temperature, lag1 Fuhrmann et al. [41] Sohail et al. [30]: 75+ (long heat waves defined by 90th percentile) | Sohail et al. [30]: 18–64 (all heat waves defined by 90th percentile), 75+ (short heat waves defined by 90th percentile) | Chen et al. [29]: heat waves defined by the maximum temperature Sohail et al. [30]: 18–64 (short, long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 65–74 (all, short, long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 75+ (all heat waves defined by 90th percentile; heat waves defined by 95th percentile) | |
| Heart Failure | Chen et al. [29]: heat waves defined by minimum temperature lag1 | Chen et al. [29]: heat waves defined by minimum temperature, lag0 Fuhrmann et al. [41] | Chen et al. [29]: heat waves defined by the maximum temperature | ||
| Total Stroke | Ha et al. [28]: lag2 | Ha et al. [28]: lag1,3 Sohail et al. [30]: 18–64 (all, short heat waves defined by 90th percentile), 65–74 (all, short, long heat waves defined by 90th percentile; heat waves defined by 95th percentile), 75+ (all, short, long heat waves defined by 90th percentile; heat waves defined by 95th percentile) | Sohail et al. [30]: 18–64 (heat waves defined by 95th percentile) | Ha et al. [28]: lag0 Sohail et al. [30]: 18–64 (long heat waves defined by 90th percentile) | |
| Ischemic Stroke | Chen et al. [29]: heat waves defined by the maximum temperature, lag0 Guirguis et al. [40] Ha et al. [28]: lag2,3 | Chen et al. [29]: heat waves defined by minimum temperature; heat waves defined by the maximum temperature at lag1 Fuhrmann et al. [41] | Ha et al. [28]: lag0,1 | ||
| Hemorrhagic Stroke | Fuhrmann et al. [41]: 2008 Ha et al. [28]: lag0–2 | Fuhrmann et al. [41]: 2007, 2011 Ha et al. [28]: lag3 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicci, K.R.; Maltby, A.; Clemens, K.K.; Vicedo-Cabrera, A.M.; Gunz, A.C.; Lavigne, É.; Wilk, P. High Temperatures and Cardiovascular-Related Morbidity: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 11243. https://doi.org/10.3390/ijerph191811243
Cicci KR, Maltby A, Clemens KK, Vicedo-Cabrera AM, Gunz AC, Lavigne É, Wilk P. High Temperatures and Cardiovascular-Related Morbidity: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(18):11243. https://doi.org/10.3390/ijerph191811243
Chicago/Turabian StyleCicci, Kendra R., Alana Maltby, Kristin K. Clemens, Ana Maria Vicedo-Cabrera, Anna C. Gunz, Éric Lavigne, and Piotr Wilk. 2022. "High Temperatures and Cardiovascular-Related Morbidity: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 18: 11243. https://doi.org/10.3390/ijerph191811243
APA StyleCicci, K. R., Maltby, A., Clemens, K. K., Vicedo-Cabrera, A. M., Gunz, A. C., Lavigne, É., & Wilk, P. (2022). High Temperatures and Cardiovascular-Related Morbidity: A Scoping Review. International Journal of Environmental Research and Public Health, 19(18), 11243. https://doi.org/10.3390/ijerph191811243