
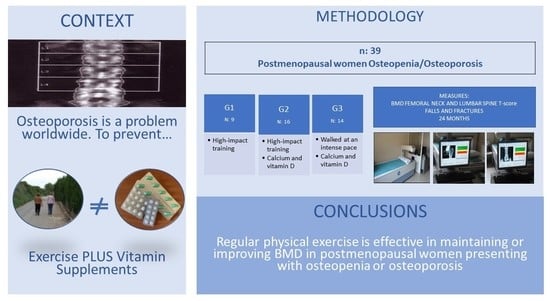
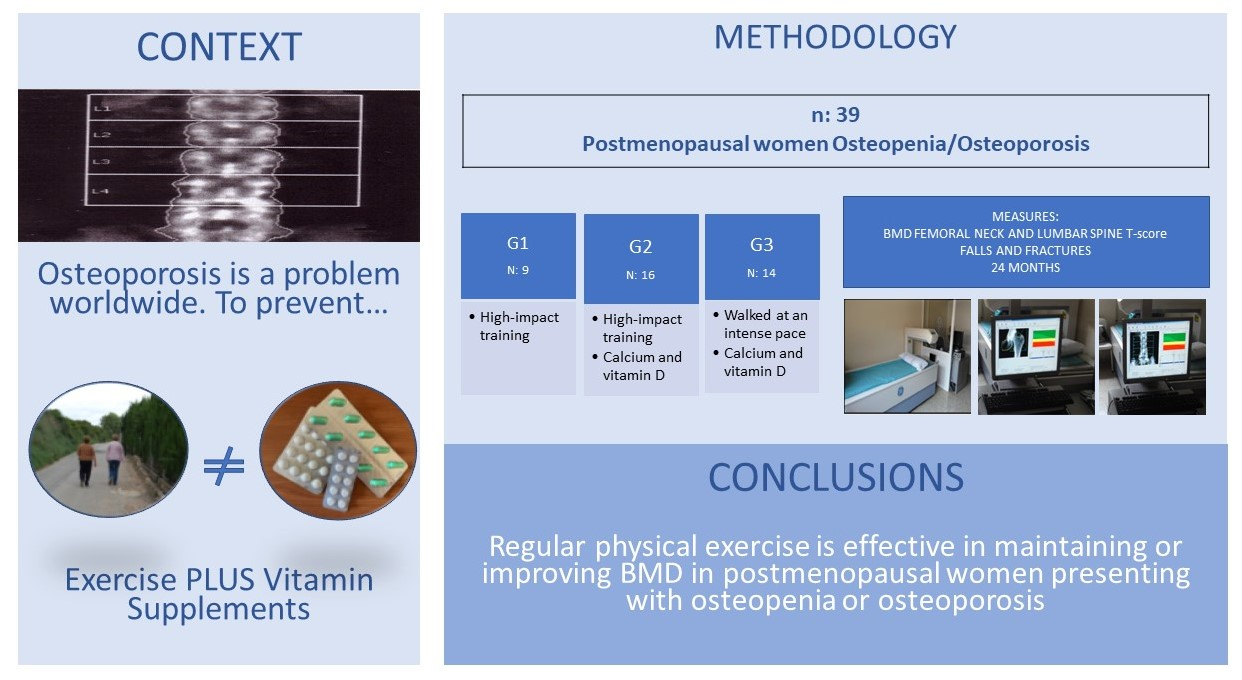
Effects of Three Interventions Combining Impact or Walking at Intense Pace Training, with or without Calcium and Vitamin Supplements, to Manage Postmenopausal Women with Osteopenia and Osteoporosis

 , and
, and
Abstract
1. Introduction
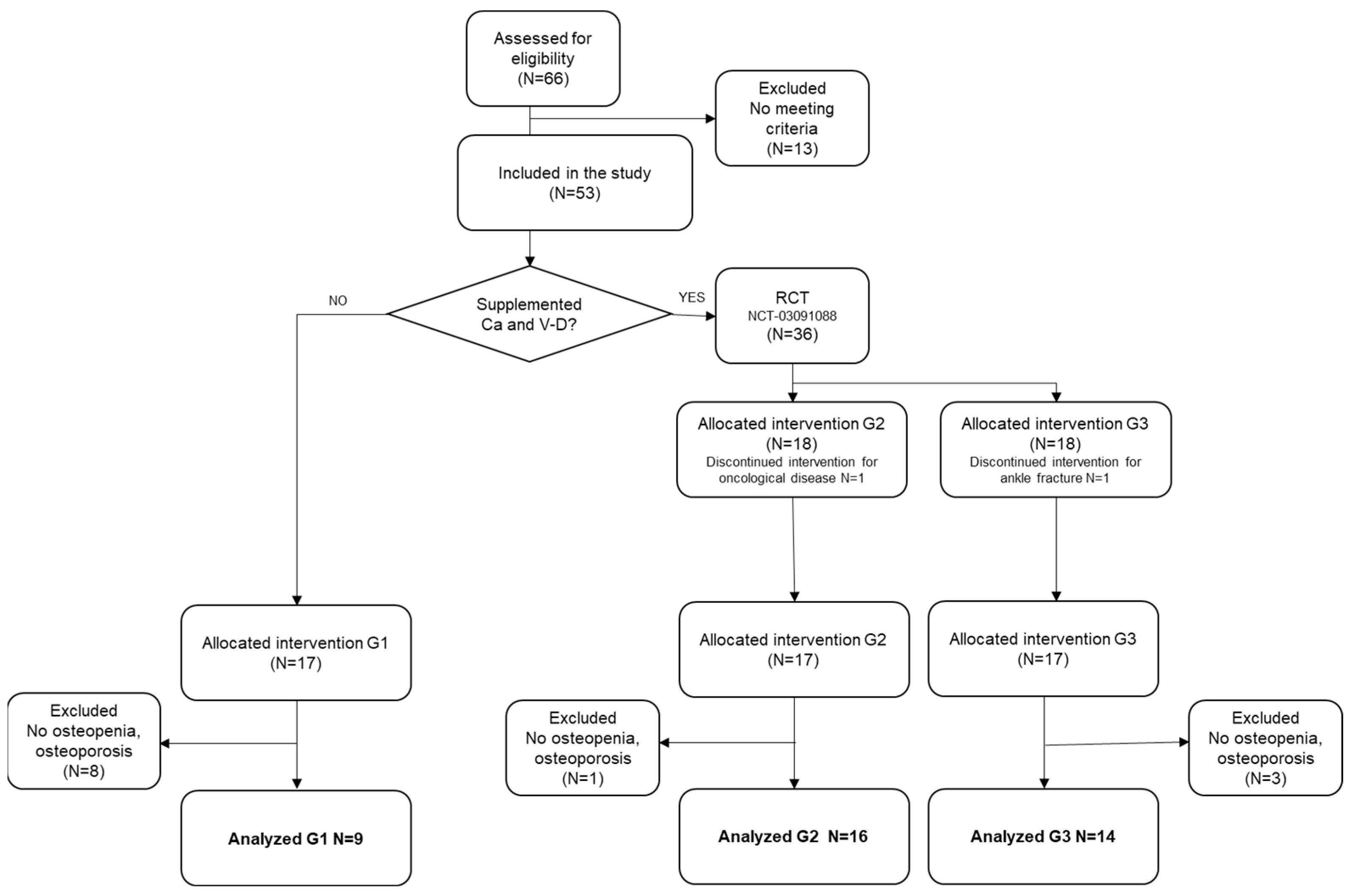
2. Materials and Methods
2.1. Methods
2.2. Interventions
2.3. Measures
2.4. Data Analysis
3. Results
Effects of the Interventions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.-Y. European Guidance for the Diagnosis and Management of Osteoporosis in Postmenopausal Women. Osteoporos. Int. 2019, 30, 3–44. [Google Scholar] [CrossRef] [PubMed]
- Sözen, T.; Özışık, L.; Başaran, N.Ç. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef]
- Szamatowicz, M. How can gynaecologists cope with the silent killer—Osteoporosis? Menopause Rev. 2016, 15, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Torpy, J.M.; Lynm, C.; Glass, R.M. Osteopenia and Preventing Fractures. JAMA 2006, 296, 2644. [Google Scholar] [CrossRef][Green Version]
- Boskey, A.L.; Imbert, L. Bone quality changes associated with aging and disease: A review. Ann. N. Y. Acad. Sci. 2017, 1410, 93–106. [Google Scholar] [CrossRef]
- Compston, J. Bone quality: What is it and how is it measured? Arq. Bras. Endocrinol. Metabol. 2006, 50, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Melton, L.J. Pidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef]
- Pouresmaeili, F.; Dehghan, B.K.; Kamarehei, M.; Meng, G.Y. A comprehensive overview on osteoporosis and its risk factors. Ther. Clin. Risk Manag. 2018, 14, 2029–2049. [Google Scholar] [CrossRef]
- Dionyssiotis, Y.; Paspati, I.; Trovas, G.; Galanos, A.; Lyritis, G.P. Association of physical exercise and calcium intake with bone mass measured by quantitative ultrasound. BMC Women’s Health 2010, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Gambacciani, M.; Levancini, M. Management of postmenopausal osteoporosis and the prevention of fractures. Panminerva Med. 2014, 56, 115–131. [Google Scholar] [PubMed]
- Pavone, V.; Testa, G.; Giardina, S.M.C.; Vescio, A.; Restivo, D.A.; Sessa, G. Pharmacological Therapy of Osteoporosis: A Systematic Current Review of Literature. Front. Pharmacol. 2017, 8, 803. [Google Scholar] [CrossRef] [PubMed]
- Howe, T.E.; Shea, B.; Dawson, L.J.; Downie, F.; Murray, A.; Ross, C.; Harbour, R.T.; Caldwell, L.M.; Creed, G. Exercise for preventing and treating osteoporosis in postmenopausal women. Cochrane Database Syst. Rev. 2011, 7, CD000333. [Google Scholar] [CrossRef] [PubMed]
- García-Gomáriz, C.; Blasco, J.-M.; Macián-Romero, C.; Guillem-Hernández, E.; Igual-Camacho, C. Effect of 2 years of endurance and high-impact training on preventing osteoporosis in postmenopausal women: Randomized clinical trial. Menopause 2018, 25, 301–306. [Google Scholar] [CrossRef]
- García-Gomariz, C.; Igual-Camacho, C.; Hernández-Guillen DBlasco, J.M. Efectos de un programa de ejercicio combinado de impacto, fuerza y resistencia en la prevención de osteoporosis; de mujeres posmenopáusicas. Fisioterapia 2019, 41, 4–11. [Google Scholar] [CrossRef]
- Turner, P.A. Osteoporosis-its causes and prevention: An update. Physiother. Theory Pract. 2000, 16, 135–149. [Google Scholar] [CrossRef]
- Xu, J.; Lombardi, G.; Jiao, W.; Banfi, G. Effects of Exercise on Bone Status in Female Subjects, from Young Girls to Postmenopausal Women: An Overview of Systematic Reviews and Meta-Analyses. Sports Med. 2016, 46, 1165–1182. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.H. Homeostatic control of bone structure: An application of feedback theory. Bone 1991, 12, 203–217. [Google Scholar] [CrossRef]
- Subirats, B.; Subirats Vila, G.; Soteras Martínez, I. Exercise prescription: Indications, dosage and side effects. Med. Clin. 2018, 138, 18–24. [Google Scholar]
- Paula, A.; Lirani-Galvão, R.; Lazaretti-Castro, M. Physical approach for prevention and treatment of osteoporosis Abordagem física para prevenção e tratamento de osteoporose. Arq. Bras. Endocrinol. Metab. 2010, 54, 171–178. [Google Scholar]
- Bouvard, B.; Annweiler, C.; Legrand, E. Osteoporosis in older adults. Jt. Bone Spine 2021, 88, 105135. [Google Scholar] [CrossRef]
- Bolton, K.L.; Egerton, T.; Wark, J.; Wee, E.; Matthews, B.; Kelly, A.; Craven, R.; Kantor, S.; Bennell, K.L. Effects of exercise on bone density and falls risk factors in post-menopausal women with osteopenia: A randomised controlled trial. J. Sci. Med. Sport 2012, 15, 102–109. [Google Scholar] [CrossRef]
- Stolzenberg, N.; Belavý, D.L.; Rawer, R.; Felsenberg, D. Whole-body vibration versus proprioceptive training on postural control in post-menopausal osteopenic women. Gait Posture 2013, 38, 416–420. [Google Scholar] [CrossRef]
- Küçükçakır, N.; Altan, L.; Korkmaz, N. Effects of Pilates exercises on pain, functional status and quality of life in women with postmenopausal osteoporosis. J. Bodyw. Mov. Ther. 2013, 17, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Tomas, C.; Chulvi-Medrano, I.; Carrasco, J.J.; Alakhdar, Y. Effect of a 1-year elastic band resistance exercise program on cardiovascular risk profile in postmenopausal women. Menopause 2018, 25, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Sosa Henríquez, M. Osteoporosis: El dilema de su definición. Med. Clin. 2005, 124, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Furlini, G.; Zati, A.; Mauro, G.L. The Effectiveness of Physical Exercise on Bone Density in Osteoporotic Patients. BioMed Res. Int. 2018, 2018, 4840531. [Google Scholar] [CrossRef] [PubMed]
- Nery, C.; Raduan, F.C.; Catena, F.; Mann, T.S.; De Andrade, M.A.P.; Baumfeld, D. Plantar plate radiofrequency and Weil osteotomy for subtle metatarsophalangeal joint instablity. J. Orthop. Surg. Res. 2015, 10, 180. [Google Scholar] [CrossRef]
- Hingorjo, M.R.; Zehra, S.; Saleem, S.; Qureshi, M.A. Serum Interleukin-15 and its relationship with adiposity Indices before and after short-term endurance exercise. Pak. J. Med. Sci. 2018, 34, 1125–1131. [Google Scholar] [CrossRef]
- Jürimäe, T.; Meema, K.; Karelson, K.; Purge, P.; Jürimäe, J. Intensity of Nordic Walking in young females with different peak O2consumption. Clin. Physiol. Funct. Imaging 2009, 29, 330–334. [Google Scholar] [CrossRef]
- Sandoval, L.; Capuñay, J.; Varela, L. Caídas en el adulto mayor: Estudio de una serie de pacientes de consultorio externo de medicina del Hospital Nacional Cayetano Heredia. Rev. Med. Hered. 1996, 7, 119–124. [Google Scholar] [CrossRef]
- Beninato, M.; Parikh Plummer, L. Use of the International Classification of Functioning, Disability and Health as a framework for analyzing the Stroke Impact Scale-16 relative to falls. Physiother. Theory Pract. 2014, 30, 149–156. [Google Scholar] [CrossRef]
- Kanis, J.A.; Seeman, E.; Johnell, O.; Rizzoli, R.; Delmas, P. The perspective of the International Osteoporosis Foundation on the official positions of the International Society for Clinical Densitometry. Osteoporos. Int. 2005, 16, 456–459. [Google Scholar] [CrossRef]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Maeda, S.S.; Lazaretti-Castro, M. An overview on the treatment of postmenopausal osteoporosis. Arq. Bras. Endocrinol. Metabol. 2014, 58, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Chodzko-Zajko, W.J. Exercise and Physical Activity for Older Adults. Kinesiol. Rev. 2014, 3, 101–106. [Google Scholar] [CrossRef]
- Zhao, R.; Zhang, M.; Zhang, Q. The Effectiveness of Combined Exercise Interventions for Preventing Postmenopausal Bone Loss: A Systematic Review and Meta-analysis. J. Orthop. Sports Phys. Ther. 2017, 47, 241–251. [Google Scholar] [CrossRef]
- Watson, S.L.; Weeks, B.K.; Weis, L.J.; Harding, A.T.; Horan, S.A.; Beck, B.R. High-Intensity Resistance and Impact Training Im-proves Bone Mineral Density and Physical Function in Postmenopausal Women With Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial. J. Bone Miner. Res. 2018, 33, 211–220. [Google Scholar] [CrossRef]
- Senderovich, H.; Tang, H.; Belmont, S. The Role of Exercises in Osteoporotic Fracture Prevention and Current Care Gaps. Where Are We Now? Recent Updates. Rambam Maimonides Med. J. 2017, 8, e0032. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; A Michaleff, Z.; Howard, K.; Clemson, L.; Hopewell, S.; E Lamb, S. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 2019, CD012424. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Compston, J.; Cooper, C.; Harvey, N.; Johansson, H.; Odén, A.; McCloskey, E.V. SIGN Guidelines for Scotland: BMD Versus FRAX Versus QFracture. Calcif. Tissue Res. 2015, 98, 417–425. [Google Scholar] [CrossRef]
- Curtis, E.; Moon, R.J.; Harvey, N.; Cooper, C. The impact of fragility fracture and approaches to osteoporosis risk assessment worldwide. Bone 2017, 104, 29–38. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Baseline | p-Value | ||||||
|---|---|---|---|---|---|---|---|
| G1 (n = 9) | G2 (n = 16) | G3 (n = 14) | |||||
| Sample descriptors | |||||||
| Menopausal age (years) | 51.0 (2.7) | 49.4 (5.2) | 51.1 (4.9) | 0.56 | |||
| Age (years) | 60.3 (6.9) | 64.9 (7.1) | 59.4 (6.3) | 0.07 | |||
| Body mass index BI (kg/m2) | 25.7 (1.9) | 25.8 (3.1) | 27.4 (4.6) | 0.39 | |||
| Weight BI (kg) | 65.5 (8.5) | 62.3 (7.4) | 63.5 (7.4) | 0.80 | |||
| Weight AI (kg) | 63.4 (8.3) | 63.6 (7.9) | 62.7 (7.0) | 0.29 | |||
| T-Score | |||||||
| Femoral neck | −0.756 (0.746) | −0.786 (0.656) | −1.079 (0.830) | 0.47 | |||
| Lumbar spine | −1.479 (0.254) | −1.913 (1.061) | −2.307 (0.793) | 0.08 | |||
| Risk factors osteoporosis | Yes | No | Yes | No | Yes | No | |
| Family history osteoporosis | 1 | 8 | 2 | 14 | 3 | 11 | 0.73 |
| Previous fractures | 1 | 8 | 1 | 15 | 1 | 13 | 0.90 |
| Frequent falls | 2 | 7 | 4 | 12 | 3 | 11 | 0.97 |
| Body mass index < 18.5 kg/m2 | 0 | 9 | 1 | 15 | 1 | 14 | 0.72 |
| Corticosteroids | 0 | 9 | 1 | 15 | 1 | 13 | 0.72 |
| Rheumatoid arthritis | 0 | 9 | 1 | 15 | 1 | 13 | 0.72 |
| Hyperthyroidism | 1 | 8 | 1 | 15 | 3 | 11 | 0.20 |
| Early menopause (<45 years) | 0 | 0 | 2 | 14 | 2 | 12 | 0.50 |
| Amenorrhea (>12 months) | 0 | 9 | 1 | 15 | 2 | 12 | 0.43 |
| Ovarian removal (no treatment) | 1 | 8 | 1 | 15 | 3 | 11 | 0.45 |
| Alcohol (>2 units/day) | 0 | 9 | 0 | 16 | 0 | 14 | 1.00 |
| Smokers | 3 | 6 | 0 | 16 | 0 | 14 | 0.00 |
| Physical activity (<30 min) | 0 | 9 | 0 | 16 | 0 | 14 | 1.00 |
| No calcium intake in diet | 0 | 9 | 0 | 16 | 0 | 14 | 1.00 |
| No sun | 0 | 9 | 0 | 16 | 0 | 14 | 1.00 |
| Humped parents | 0 | 9 | 4 | 12 | 3 | 11 | 0.26 |
| >40 years | 9 | 0 | 16 | 0 | 14 | 0 | 1.00 |
| Loss of more than 3 cm | 0 | 9 | 4 | 12 | 3 | 11 | 0.26 |
| T-Score BL | T-Score EI | T-Score BC | Time | Group | Time × Group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Body Area | n | Mean (SD) | Mean (SD) | Mean (SD) | BC% | F | p-Value | F | p-Value | F | p-Value |
| Femoral neck | 1.32 | 0.259 | 0.98 | 0.384 | 1.48 | 0.241 | |||||
| G1 | 9 | −0.756 (0.746) | −0.811 (0.680) | −0.056 (0.229) | −7.3% | ||||||
| G2 | 16 | −0.786 (0.656) | −0.602 (0.708) | 0.184 (0.430) | 23.4% | ||||||
| G3 | 14 | −1.079 (0.830) | −1.014 (0.695) | 0.064 (0.266) | 6.0% | ||||||
| Lumbar spine | 4.51 | 0.041 2–3 | 2.61 | 0.081 | 2.33 | 0.112 | |||||
| G1 | 9 | −1.479 (0.254) | −1.577 (0.471) | −0.100 (0.630) | −6.8% | ||||||
| G2 | 16 | −1.913 (1.061) | −1.383 (0.920) | 0.529 (0.785) | 27.7% | ||||||
| G3 | 14 | −2.307 (0.793) | −2.000 (0.748) | 0.307 (0.634) | 13.3% | ||||||
| G1 (n = 9) | G2 (n = 16) | G3 (n = 14) | χ2 | p-Value | Cramer V | p-Value | |
|---|---|---|---|---|---|---|---|
| Falls (last 2 years) | 3.21 | 0.201 | 0.29 | 0.213 | |||
| Fallers | 0 (0.0%) | 1 (6.3%) | 3 (21.4%) | ||||
| Non-fallers | 9 (100%) | 15 (93.8%) | 11 (78.6%) | ||||
| Fractures (last 2 years) | 6.77 | 0.034 | 0.42 | 0.037 | |||
| Participants with fracture | 1 (11.1%) | 1 (6.3%) | 6 (42.9%) | ||||
| Participants with no fracture | 8 (88.9%) | 15 (93.8%) | 8 (57.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Gomariz, C.; Igual-Camacho, C.; Sanchís-Sales, E.; Hernández-Guillén, D.; Blasco, J.-M. Effects of Three Interventions Combining Impact or Walking at Intense Pace Training, with or without Calcium and Vitamin Supplements, to Manage Postmenopausal Women with Osteopenia and Osteoporosis. Int. J. Environ. Res. Public Health 2022, 19, 11215. https://doi.org/10.3390/ijerph191811215
García-Gomariz C, Igual-Camacho C, Sanchís-Sales E, Hernández-Guillén D, Blasco J-M. Effects of Three Interventions Combining Impact or Walking at Intense Pace Training, with or without Calcium and Vitamin Supplements, to Manage Postmenopausal Women with Osteopenia and Osteoporosis. International Journal of Environmental Research and Public Health. 2022; 19(18):11215. https://doi.org/10.3390/ijerph191811215
Chicago/Turabian StyleGarcía-Gomariz, Carmen, Celedonia Igual-Camacho, Enrique Sanchís-Sales, David Hernández-Guillén, and José-M. Blasco. 2022. "Effects of Three Interventions Combining Impact or Walking at Intense Pace Training, with or without Calcium and Vitamin Supplements, to Manage Postmenopausal Women with Osteopenia and Osteoporosis" International Journal of Environmental Research and Public Health 19, no. 18: 11215. https://doi.org/10.3390/ijerph191811215
APA StyleGarcía-Gomariz, C., Igual-Camacho, C., Sanchís-Sales, E., Hernández-Guillén, D., & Blasco, J.-M. (2022). Effects of Three Interventions Combining Impact or Walking at Intense Pace Training, with or without Calcium and Vitamin Supplements, to Manage Postmenopausal Women with Osteopenia and Osteoporosis. International Journal of Environmental Research and Public Health, 19(18), 11215. https://doi.org/10.3390/ijerph191811215