



Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction/Background
2. Methods
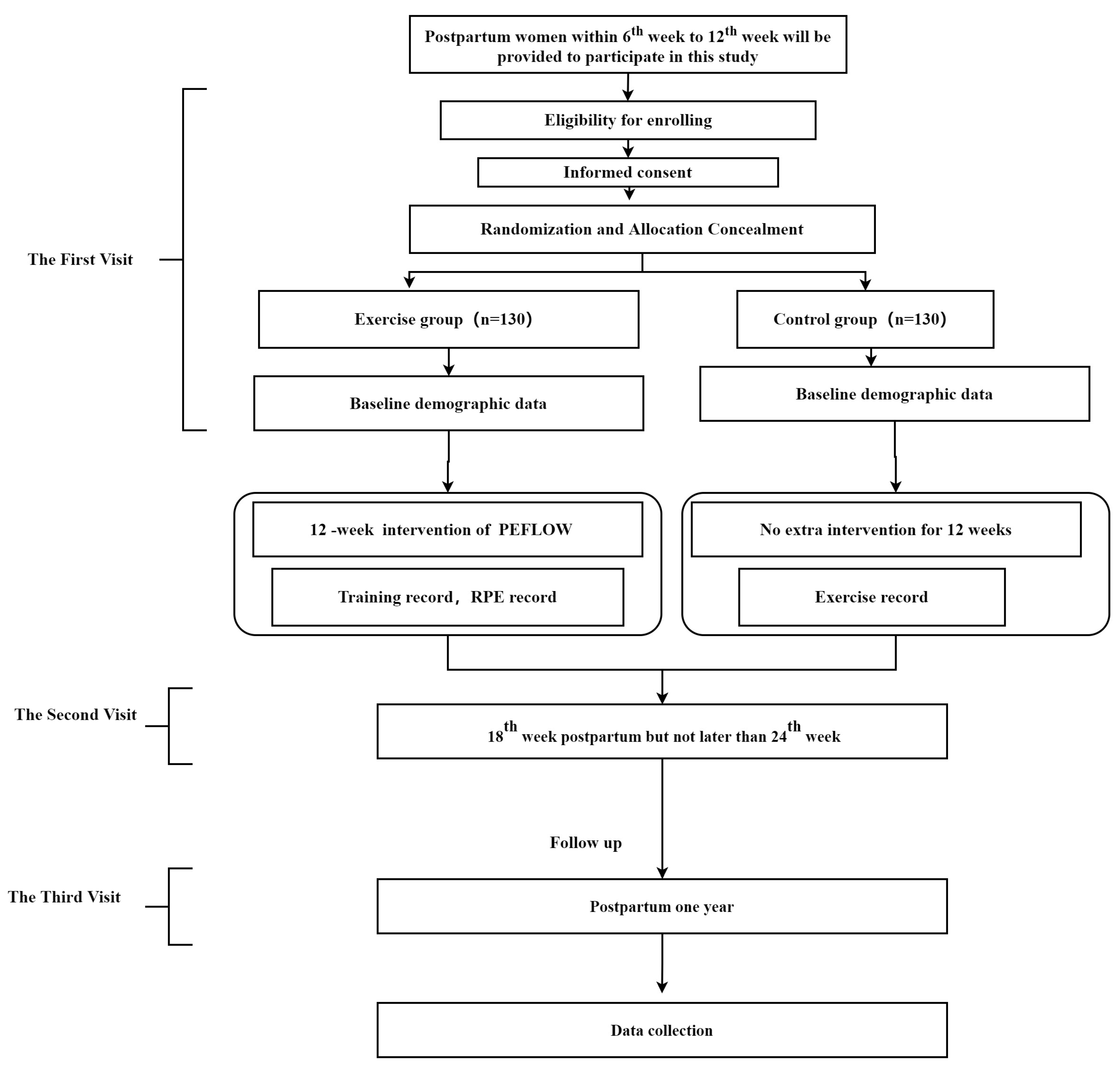
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Site Investigators and Roles
2.5. Randomization and Allocation Concealment
2.6. Assessment Schedule
2.7. Interventions
3. Data Collection and Management
- (1)
- The International Physical Activity Questionnaire Score-Short Form (IPAQ-SF), which were recommended as a cost-effective method to assess physical activity by nine questions recording the activity of four levels of intensities in short forms: vigorous-intensity, moderate-intensity, walking, and sitting [31];
- (2)
- The Pelvic Floor Distress Inventory Questionnaire-20 (PFDI-20) and Pelvic Floor Impact Questionnaire-7 (PFIQ-7), which were designed to comprehensively evaluate to what extent the lower urinary tract, lower gastrointestinal tract, and pelvic organ prolapse symptoms affect the quality of life of women who suffer from PFD [32];
- (3)
- (4)
- The Pittsburgh Sleep Quality Index (PSQI), which was developed in 1989 and accepted as the most common measure of sleep quality [36].
4. Outcomes of the Study
4.1. Sample Analysis
4.2. Statistical Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, L.; Wenjia, L.O.U. Current situation of female pelvic floor rehabilitation in China. Chin. J. Fam. Plan. Gynecotokol. 2020, 12, 3–4, 8. (In Chinese) [Google Scholar]
- Lan, Z.H.U.; Wenjia, L.O.U. Pay attention to female sexual dysfunction diseases. J. Pract. Obstet. Gynecol. 2018, 34, 401–402. (In Chinese) [Google Scholar]
- Ferreira, C.H.J.; Barbosa, P.B.; Souza, F.D.O.; Antônio, F.I.; Franco, M.M.; Bø, K. Inter-rater reliability study of the modified Oxford Grading Scale and the Peritron manometer. Physiotherapy 2011, 97, 132–138. [Google Scholar] [CrossRef] [PubMed]
- El-Haieg, D.O.; Madkour, N.M.; Basha, M.A.A.; Ahmad, R.A.; Sadek, S.M.; Al-Molla, R.M.; Tantwy, E.F.; Almassry, H.N.; Altaher, K.M.; Mahmoud, N.E.M.; et al. Magnetic resonance imaging and 3-dimensional transperineal ultrasound evaluation of pelvic floor dysfunction in symptomatic women: A prospective comparative study. Ultrasonography 2019, 38, 355–364. [Google Scholar] [CrossRef]
- Bump, R.C.; Mattiasson, A.; Bo, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; Shull, B.L.; Smith, A.R. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef]
- Borello-France, D.F.; Handa, V.L.; Brown, M.B.; Goode, P.; Kreder, K.; Scheufele, L.L.; Weber, A.M.; Pelvic Floor Disorders Network. Pelvic-floor muscle function in women with pelvic organ prolapse. Phys. Ther. 2007, 87, 399–407. [Google Scholar] [CrossRef]
- Gilchrist, A.S.; Campbell, W.; Steele, H.; Brazell, H.; Foote, J.; Swift, S. Outcomes of observation as therapy for pelvic organ prolapse: A study in the natural history of pelvic organ prolapse. Neurourol. Urodyn. 2013, 32, 383–386. [Google Scholar] [CrossRef]
- Miedel, A.; Ek, M.; Tegerstedt, G.; Maehle-Schmidt, M.; Nyren, O.; Hammarstrom, M. Short-term natural history in women with symptoms indicative of pelvic organ prolapse. Int. Urogynecol. J. 2011, 22, 461–468. [Google Scholar] [CrossRef]
- Sigurdardottir, T.; Steingrimsdottir, T.; Geirsson, R.T.; Halldorsson, T.I.; Aspelund, T.; Bo, K. Can postpartum pelvic floor muscle training reduce urinary and anal incontinence?: An assessor-blinded randomized controlled trial. Am. J. Obstet. Gynecol. 2020, 222, 247.e1–247.e8. [Google Scholar] [CrossRef]
- Min, L.; Chunxue, Y.; Qiubo, L.; Xudong, D.; Yan, Z.; Guifang, Z.; Kejia, H.; Tianzi, G.; Qing, F. Effectiveness of intravaginal electrical stimulation combined with electromyography biofeedback-mediated pelvic floor muscle training for postpartum symptomatic pelvic organ prolapse: Protocol for the PROSPECT randomized trial. Trials 2022, 23, 131. [Google Scholar] [CrossRef]
- Bo, K.; Angles-Acedo, S.; Batra, A.; Braekken, I.H.; Chan, Y.L.; Jorge, C.H.; Kruger, J.; Yadav, M.; Dumoulin, C. International urogynecology consultation chapter 3 committee 2; conservative treatment of patient with pelvic organ prolapse: Pelvic floor muscle training. Int. Urogynecol. J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Kegel, A.H. Progressive resistance exercise in the functional restoration of the perineal muscles. Am. J. Obstet. Gynecol. 1948, 56, 238–248. [Google Scholar] [CrossRef]
- Iglesia, C.B.; Smithling, K.R. Pelvic Organ Prolapse. Am. Fam. Physician 2017, 96, 179–185. [Google Scholar]
- Zachovajeviene, B.; Siupsinskas, L.; Zachovajevas, P.; Venclovas, Z.; Milonas, D. Effect of diaphragm and abdominal muscle training on pelvic floor strength and endurance: Results of a prospective randomized trial. Sci. Rep. 2019, 9, 19192. [Google Scholar] [CrossRef] [PubMed]
- Oliva-Lozano, J.M.; Muyor, J.M. Core Muscle Activity During Physical Fitness Exercises: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4306. [Google Scholar] [CrossRef] [PubMed]
- Brennen, R.; Lin, K.Y.; Denehy, L.; Frawley, H.C. The Effect of Pelvic Floor Muscle Interventions on Pelvic Floor Dysfunction After Gynecological Cancer Treatment: A Systematic Review. Phys. Ther. 2020, 100, 1357–1371. [Google Scholar] [CrossRef] [PubMed]
- Tenfelde, S.; Logan, R.; Abernethy, M. Yoga from the pelvic floor. Beginnings 2014, 34, 24–26. [Google Scholar]
- Fozzatti, C.; Herrmann, V.; Palma, T.; Riccetto, C.L.; Palma, P.C. Global Postural Re-education: An alternative approach for stress urinary incontinence? Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 152, 218–224. [Google Scholar] [CrossRef]
- Fozzatti, M.C.; Palma, P.; Herrmann, V.; Dambros, M. Impact of global postural reeducation for treatment of female stress urinary incontinence. Rev. Assoc. Med. Bras. 2008, 54, 17–22. [Google Scholar] [CrossRef]
- Liu, T.; Hou, X.; Xie, B.; Wu, J.; Yang, X.; Sun, X.; Wang, J. Pelvic incidence: A study of a spinopelvic parameter in MRI evaluation of pelvic organ prolapse. Eur. J. Radiol. 2020, 132, 109286. [Google Scholar] [CrossRef]
- Teodori, R.M.; Negri, J.R.; Cruz, M.C.; Marques, A.P. Global Postural Re-education: A literature review. Rev. Bras. Fisioter. 2011, 15, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Dufour, S.; Wu, M. No. 397—Conservative Care of Urinary Incontinence in Women. J. Obstet. Gynaecol. Can. 2020, 42, 510–522. [Google Scholar] [CrossRef] [PubMed]
- Talley, K.M.C.; Wyman, J.F.; Bronas, U.; Olson-Kellogg, B.J.; McCarthy, T.C. Defeating Urinary Incontinence with Exercise Training: Results of a Pilot Study in Frail Older Women. J. Am. Geriatr. Soc. 2017, 65, 1321–1327. [Google Scholar] [CrossRef] [PubMed]
- Virtuoso, J.F.; Menezes, E.C.; Mazo, G.Z. Effect of Weight Training with Pelvic Floor Muscle Training in Elderly Women with Urinary Incontinence. Res. Q. Exerc. Sport 2019, 90, 141–150. [Google Scholar] [CrossRef]
- Bo, K. Physiotherapy management of urinary incontinence in females. J. Physiother. 2020, 66, 147–154. [Google Scholar] [CrossRef]
- Dumoulin, C.; Morin, M.; Danieli, C.; Cacciari, L.; Mayrand, M.H.; Tousignant, M.; Abrahamowicz, M. Group-Based vs Individual Pelvic Floor Muscle Training to Treat Urinary Incontinence in Older Women: A Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1284–1293. [Google Scholar] [CrossRef]
- Gao, L.; Zhang, D.; Wang, S.; Jia, Y.; Wang, H.; Sun, X.; Wang, J. Effect of the App-Based Video Guidance on Prenatal Pelvic Floor Muscle Training Combined with Global Postural Re-education for Stress Urinary Incontinence Prevention: A Protocol for a Multicenter, Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 12929. [Google Scholar] [CrossRef]
- Gasquet, I.; Tcherny-Lessenot, S.; Gaudebout, P.; Bosio, L.G.B.; Klein, P.; Haab, F. Influence of the severity of stress urinary incontinence on quality of life, health care seeking, and treatment: A national cross-sectional survey. Eur. Urol. 2006, 50, 818–825. [Google Scholar] [CrossRef]
- de Andrade, R.L.; Bo, K.; Antonio, F.I.; Driusso, P.; Mateus-Vasconcelos, E.C.L.; Ramos, S.; Julio, M.P.; Ferreira, C.H.J. An education program about pelvic floor muscles improved women’s knowledge but not pelvic floor muscle function, urinary incontinence or sexual function: A randomised trial. J. Physiother. 2018, 64, 91–96. [Google Scholar] [CrossRef]
- Arney, B.E.; Glover, R.; Fusco, A.; Cortis, C.; de Koning, J.J.; van Erp, T.; Jaime, S.; Mikat, R.P.; Porcari, J.P.; Foster, C. Comparison of RPE (Rating of Perceived Exertion) Scales for Session RPE. Int. J. Sports Physiol. Perform. 2019, 14, 994–996. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Barber, M.D.; Walters, M.D.; Bump, R.C. Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7). Am. J. Obstet. Gynecol. 2005, 193, 103–113. [Google Scholar] [CrossRef]
- Isidori, A.M.; Pozza, C.; Esposito, K.; Giugliano, D.; Morano, S.; Vignozzi, L.; Corona, G.; Lenzi, A.; Jannini, E.A. Development and validation of a 6-item version of the female sexual function index (FSFI) as a diagnostic tool for female sexual dysfunction. J. Sex. Med. 2010, 7, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Chedraui, P.; Perez-Lopez, F.R.; Sanchez, H.; Aguirre, W.; Martinez, N.; Miranda, O.; Plaza, M.S.; Schwager, G.; Narvaez, J.; Quintero, J.C.; et al. Assessment of sexual function of mid-aged Ecuadorian women with the 6-item Female Sexual Function Index. Maturitas 2012, 71, 407–412. [Google Scholar] [CrossRef]
- Sonbahar, A.E.; Culha, M.G.; Jannini, E. The validity and reliability of the Turkish version of the 6-item female sexual function index (FSFI-6) and the relationship between climacturia and female sexual dysfunction. Int. J. Impot. Res. 2021, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Oleksy, L.; Wojciechowska, M.; Mika, A.; Antos, E.; Bylina, D.; Kielnar, R.; Pruszczynski, B.; Stolarczyk, A. Normative values for Glazer Protocol in the evaluation of pelvic floor muscle bioelectrical activity. Medicine 2020, 99, e19060. [Google Scholar] [CrossRef]
- Kobak, W.H.; Rosenberger, K.; Walters, M.D. Interobserver variation in the assessment of pelvic organ prolapse. Int. Urogynecol. J. Pelvic Floor Dysfunct. 1996, 7, 121–124. [Google Scholar] [CrossRef]
- Martinez-Romero, M.T.; Ayala, F.; De Ste, C.M.; Vera-Garcia, F.J.; Sainz, D.B.P.; Santonja-Medina, F.; Sanchez-Meca, J. A Meta-Analysis of the Reliability of Four Field-Based Trunk Extension Endurance Tests. Int. J. Environ. Res. Public Health 2020, 17, 3088. [Google Scholar] [CrossRef]
- Blomquist, J.L.; Carroll, M.; Munoz, A.; Handa, V.L. Pelvic floor muscle strength and the incidence of pelvic floor disorders after vaginal and cesarean delivery. Am. J. Obstet. Gynecol. 2020, 222, 62.e1–62.e8. [Google Scholar] [CrossRef]
- Deshmukh, A.S.; Steenberg, D.E.; Hostrup, M.; Birk, J.B.; Larsen, J.K.; Santos, A.; Kjobsted, R.; Hingst, J.R.; Scheele, C.C.; Murgia, M.; et al. Deep muscle-proteomic analysis of freeze-dried human muscle biopsies reveals fiber type-specific adaptations to exercise training. Nat. Commun. 2021, 12, 304. [Google Scholar] [CrossRef] [PubMed]
- Viseux, F.; Lemaire, A.; Barbier, F.; Charpentier, P.; Leteneur, S.; Villeneuve, P. How can the stimulation of plantar cutaneous receptors improve postural control? Review and clinical commentary. Neurophysiol. Clin. 2019, 49, 263–268. [Google Scholar] [CrossRef] [PubMed]
- de Tayrac, R.; Schantz, C. Childbirth pelvic floor trauma: Anatomy, physiology, pathophysiology and special situations—CNGOF perineal prevention and protection in obstetrics guidelines. Gynecol. Obstet. Fertil. Senol. 2018, 46, 900–912. [Google Scholar] [CrossRef] [PubMed]
- Wieland, L.S.; Shrestha, N.; Lassi, Z.S.; Panda, S.; Chiaramonte, D.; Skoetz, N. Yoga for treating urinary incontinence in women. Cochrane Database Syst. Rev. 2019, 2, CD012668. [Google Scholar] [CrossRef]
- Tuttle, L.J.; Autry, T.; Kemp, C.; Lassaga-Bishop, M.; Mettenleiter, M.; Shetter, H.; Zukowski, J. Hip exercises improve intravaginal squeeze pressure in older women. Physiother. Theory Pract. 2020, 36, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Gomes, C.S.; Pedriali, F.R.; Urbano, M.R.; Moreira, E.H.; Averbeck, M.A.; Almeida, S.H.M. The effects of Pilates method on pelvic floor muscle strength in patients with post-prostatectomy urinary incontinence: A randomized clinical trial. Neurourol. Urodyn. 2018, 37, 346–353. [Google Scholar] [CrossRef]
- Nygaard, I.E.; Wolpern, A.; Bardsley, T.; Egger, M.J.; Shaw, J.M. Early postpartum physical activity and pelvic floor support and symptoms 1 year postpartum. Am. J. Obstet. Gynecol. 2021, 224, 193.e1–193.e19. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Week | 8-Scetion Program | Week | 8-Scetion Program | |
|---|---|---|---|---|
| Warm-ups | Pelvic floor perception, try to feel the contraction of pelvic floor muscles at different positions, including standing, lying and sitting position. | |||
| Main Progressive Exercises | 1 |
| 7 |
|
| 2 |
| 8 |
| |
| 3 |
| 9 |
| |
| 4 |
| 10 |
| |
| 5 |
| 11 |
| |
| 6 |
| 12 |
| |
| Cooling Down | Dynamic stretching, including upper and lower limbs, waist, back, and abdomen stretching and pelvic floor muscle relaxation with mini foam axis. | |||
| EG | CG | EG | CG | EG | CG | ||
|---|---|---|---|---|---|---|---|
| Baseline screen, Informed consent, Randomization |  | ||||||
| The follow-up visits | The First | The Second | The Third | ||||
| Demographic data collection | ◯ | ◯ | |||||
| The MOS | ● | ● | ● | ● | ● | ● | |
| POP-Q stage | ● | ● | ● | ● | ● | ● | |
| Cough stress test | ● | ● | ● | ● | ● | ● | |
| Vaginal relaxity | ● | ● | ● | ● | ● | ● | |
| Pelvic floor electrophysiological test | ◎ | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Pelvic floor ultrasound | ◎ | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Spine X-ray | ◎ | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Body Composition | ◎ | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Hand grip test | ◎ | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Trunk endurance test | ◎ | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Questionnaires | PFDI-20 | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| PFIQ-7 | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| FSFI-6 | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| IPAQ-SF | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| PSQI | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | |
| Training record | ✷ | ✷(if any) | |||||
| RPE | ✷ | ||||||
| Adverse Event | ☐ | ☐ | |||||
| Testing Items | Indicators | Compute Value | Score Value |
|---|---|---|---|
| POP-Q | Stage 0 | 0 | |
| Stage I | 1 | ||
| Stage II | 2 | ||
| Stage III | 3 | ||
| Stage IV | 4 | ||
| Cough stress test | Yes | 1 | |
| No | 0 | ||
| Vaginal relaxation | ≥4 fingers | 4 | |
| >3 fingers, and <4 fingers | 3 | ||
| =3 fingers | 2 | ||
| >2 fingers, and <3 fingers | 1 | ||
| ≤2 fingers | 0 | ||
| Pelvic floor electrophysiological test [40] | <20 cm2Hg | 1 | |
| ≥20 cm2Hg | 0 | ||
| * Total Score 1 | |||
| PFDI-20 | - | Comprehensive score | |
| PFIQ-7 | - | Comprehensive score | |
| FSFI-6 | - | Comprehensive score | |
| * Total Score 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, H.; Zhang, D.; Gao, L.; Liu, H.; Di, Y.; Xie, B.; Jiao, W.; Sun, X. Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 11073. https://doi.org/10.3390/ijerph191711073
Zhu H, Zhang D, Gao L, Liu H, Di Y, Xie B, Jiao W, Sun X. Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(17):11073. https://doi.org/10.3390/ijerph191711073
Chicago/Turabian StyleZhu, Hongmei, Di Zhang, Lei Gao, Huixin Liu, Yonghui Di, Bing Xie, Wei Jiao, and Xiuli Sun. 2022. "Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 17: 11073. https://doi.org/10.3390/ijerph191711073
APA StyleZhu, H., Zhang, D., Gao, L., Liu, H., Di, Y., Xie, B., Jiao, W., & Sun, X. (2022). Effect of Pelvic Floor Workout on Pelvic Floor Muscle Function Recovery of Postpartum Women: Protocol for a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(17), 11073. https://doi.org/10.3390/ijerph191711073