
Clinical Applications of Artificial Intelligence and Machine Learning in Children with Cleft Lip and Palate—A Systematic Review


 ,
,  ,
,  ,
,  , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Rationale and Objectives
1.2. Research Questions
- What are the current clinical applications of deep learning/artificial intelligence in patients with CLP?
- What is the diagnostic performance of AI and ML models being utilized on CLP patients?
2. Materials and Methods
2.1. Research Design
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- −
- The articles that dealt with AI and its application in the context of CLP.
- −
- The journal articles which present some predictability or observable outcomes using Machine learning techniques in children with CLP.
- −
- Original articles, Case-control studies, longitudinal observational studies, and retrospective cross-sectional studies that involves artificial intelligent or machine learning neural network methods in children with CLP.
2.2.2. Exclusion Criteria
- −
- Unpublished articles that have been uploaded with only manuscripts.
- −
- Articles that contain only abstracts without their full text.
- −
- Journal articles which were published in languages other than English.
- −
- Book chapters, magazine prints, blog posts, editorials, case reports and case series.
2.3. Information Sources
2.4. Search Strategy
2.5. Study Selection and Data Collection Process
2.6. Data Extraction
2.7. Data Items
- (a)
- Population—Children with Cleft lip and palate of either sex, and of any ethnicity.
- (b)
- Intervention—The applications of AI/ML techniques in diagnosis and treatment prediction in children with CLP.
- (c)
- Comparison—Human intelligence/other diagnostic methods which does not involve AI models.
- (d)
- Outcomes—Diagnostic accuracy and prediction of treatment outcome in children with CLP.
2.8. Diagnostic Accuracy Measures
2.9. Characteristics for Diagnostic Comparisons
- (i)
- Index test: the sensitivity and specificity of clinically trained AI/machine learning models are tested using an index test and evaluating parameters.
- (ii)
- Reference standards: any other assessment techniques such as Mel frequency for hypernasality, lateral cephalometric radiographic evaluation by clinicians.
- (iii)
- Target conditions: Unilateral CLP, Bilateral CLP, Unilateral Cleft lip and alveolus, Unilateral cleft lip, Hypernasality, Dental characteristics and sagittal relationship in children with CLP.
2.10. Risk of Bias Assessment
2.11. Additional Synthesis
3. Results
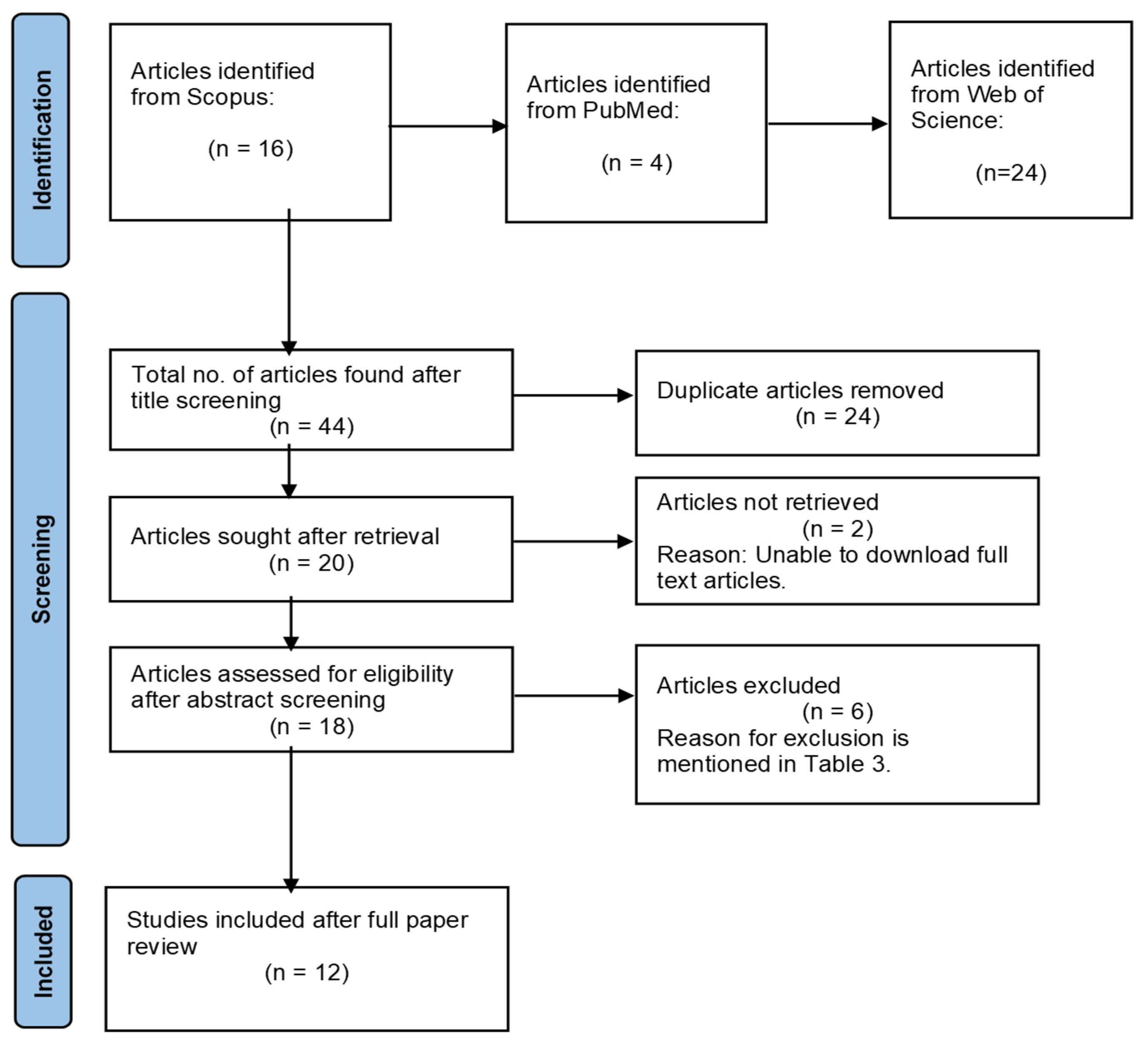
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Results of Risk of Bias Studies
3.4. Clinical Applications of AI
3.5. Genetic Risk Assessment
3.6. Dental Characteristics and Sagittal Jaw Relationship
3.7. Hypernasality Detection
3.8. CLP Surgery
3.9. Diagnosis and Prediction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANB | A-point, nasion, B-point |
| ANN | Artificial neural network |
| BCLP | Bilateral CLP |
| CLP | cleft lip and palate |
| CNN | Convolutional neural network |
| COP | Cant of occlusal plane |
| CSR | Cascaded shaped regression |
| DNN | Deep neural network |
| DRNN | Deep recurrent neural network |
| DT | Decision tree |
| FH | Frankfort horizontal |
| GD | Group display |
| IIA | Inter-incisal angle |
| IMPA | Incisor mandibular plane angle |
| k-NN | k-nearest neighbor |
| L1 | Lower central incisor |
| LOP | Lower occlusal plane |
| LR | Logistic regression |
| LSTM | Long short-term memory |
| MLP | Multi-layer perceptron |
| NA | Nasion to point-A |
| NB | Naive Bayesian |
| NB | Nasion to point-B |
| NC | Non-cleft |
| NLD | Non-linear dynamics |
| NSCLP ± P | Non-syndromic cleft lip and palate with or without palate |
| OB | Overbite |
| OJ | Overjet |
| PSD | Power spectrum density |
| RF | Random forest |
| SN | Sella nasion |
| SNA | Sella, nasion, A-point |
| SNB | Sella, nasion, B-point |
| SNPs | Single nucleotide polymorphism |
| SVM | Support vector machine |
| U1 | Upper central Incisor |
| UCL | Unilateral cleft lip |
| UCLA | Unilateral cleft lip and alveolus |
| UCLP | Unilateral CLP |
| UID | Upper incisor display |
| UOP | Upper occlusal plane, |
| VGG | Visual Geometry Group |
References
- Dixon, M.J.; Marazita, M.L.; Beaty, T.H.; Murray, J.C. Cleft lip and palate: Understanding genetic and environmental influences. Nat. Rev. Genet. 2011, 12, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Chawla, O.; Deacon, S.A.; Ireland, A.J.; Sandy, J.R. Cleft lip and palate at a glance. Orthod. Update 2015, 8, 78–84. [Google Scholar] [CrossRef]
- Schutte, B.C.; Murray, J.C. The many faces and factors of orofacial clefts. Hum. Mol. Genet. 1999, 8, 1853–1859. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.C. Gene/environment causes of cleft lip and/or palate. Clin. Genet. 2002, 61, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Cobourne, M.T. The complex genetics of cleft lip and palate. Eur. J. Orthod. 2004, 26, 7–16. [Google Scholar] [CrossRef]
- Shetye, P.R. Update on treatment of patients with cleft—Timing of orthodontics and surgery. Semin. Orthod. 2016, 22, 45–51. [Google Scholar] [CrossRef]
- Al-Kharboush, G.H.; Al-Balkhi, K.M.; Al-Moammar, K. The prevalence of specific dental anomalies in a group of Saudi cleft lip and palate patients. Saudi Dent. J. 2015, 27, 75–80. [Google Scholar] [CrossRef]
- Shetye, P.R.; Evans, C.A. Midfacial morphology in adult unoperated complete unilateral cleft lip and palate patients. Angle Orthod. 2006, 76, 810–816. [Google Scholar]
- Rocha, M.O.; Oliveira, D.D.; Costa, F.O.; Pires, L.R.; Diniz, A.R.; Soares, R.V. Plaque index and gingival index during rapid maxillary expansion of patients with unilateral cleft lip and palate. Dent. Press J. Orthod. 2017, 22, 43–48. [Google Scholar] [CrossRef]
- Wehby, G.L.; Goco, N.; Moretti-Ferreira, D.; Felix, T.; Richieri-Costa, A.; Padovani, C.; Queiros, F.; Guimaraes, C.V.N.; Pereira, R.; Litavecz, S.; et al. Oral cleft prevention program (OCPP). BMC Pediatr. 2012, 12, 184. [Google Scholar] [CrossRef]
- Kuroe, K.; Iino, S.; Shomura, K.; Okubo, A.; Sugihara, K.; Ito, G. Unilateral advancement of the maxillary minor segment by distraction osteogenesis in patients with repaired unilateral cleft lip and palate: Report of two cases. Cleft Palate Craniofac. J. 2003, 40, 317–324. [Google Scholar] [CrossRef]
- Lee, H.; Nguyen, A.; Hong, C.; Hoang, P.; Pham, J.; Ting, K. Biomechanical effects of maxillar expansion on a patient with cleft palate: A finite element analysis. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.K.; Kajii, T.S.; Matsuno, M.K.; Kato, Y.S.; Iida, J. Multivariate analysis of factors affectingdental arch relationships in Japanese unilateral cleftlip and palate patients at Hokkaido University Hospital. Orthod. Waves 2008, 67, 45–53. [Google Scholar] [CrossRef]
- Asif, J.A.; Alam, M.K.; Imanishi, T.; Mukai, A.; Yusa, T.; Haque, S.; Pohchi, A. Treatment outcome and factors affecting dental arch relationship in Malay children with unilateral cleft lip and palate (UCLP). J. Hard Tissue Biol. 2016, 25, 371–376. [Google Scholar] [CrossRef]
- Haque, S.; Alam, M.K.; Khamis, M.F. The effect of various factors on the dental arch relationship in non-syndromic unilateral cleft lip and palate children assessed by new approach: A retrospective study. BMC Pediatr. 2017, 17, 119. [Google Scholar] [CrossRef] [PubMed]
- Haque, S.; Alam, M.K.; Khamis, M.F. Treatment outcome of Bangladeshi UCLP patients based on both phenotype and postnatal treatment factors using Modified Huddart Bodenham (mHB) Index. Cleft Palate Craniofac. J. 2018, 55, 966–973. [Google Scholar] [CrossRef]
- Alam, M.K.; Kajii, T.S.; Sato, Y.; Iida, J. Clinical investigation of congenital factor affecting craniofacial morphology of unilateral cleft lip and palate in Japanese patients. Pesqui. Bra. Odontopediatr. Clín. Integr. 2019, 19, 4642. [Google Scholar] [CrossRef]
- Batwa, W.; Almarhoon, H.A.; Almoammar, K.A.; Alqahtani, N.; Albarakati, S.F.; Al-Jewair, T. Dento- skeletal characteristics of cleft patients with missing teeth. Clin. Cosmet. Investig. Dent. 2018, 10, 237–244. [Google Scholar] [CrossRef]
- Alam, M.K.; Alfawzan, A.A. Dental Characteristics of Different Types of Cleft and Non-cleft Individuals. Front. Cell Dev. Biol. 2020, 8, 789. [Google Scholar] [CrossRef]
- Haque, S.; Khamis, M.F.; Alam, M.K.; Ahmad, W.M. Effects of multiple factors on treatment outcome in the three-dimensional maxillary arch morphometry of children with unilateral cleft lip and palate. J. Craniofac. Surg. 2020, 31, e534–e538. [Google Scholar] [CrossRef]
- Parveen, S.; Shetty, R.; Husain, A.; Mascarenhas, R.; D’Souza, N.; Shetty, N.K. Three-dimensional assessment of alveolar bone thickness in individuals with nonsyndromic unilateral complete cleft lip and palate. J. Cleft Lip Palate Craniofac. Anom. 2018, 5, 106. [Google Scholar] [CrossRef]
- Neill, D.B. Using artificial intelligence to improve hospital inpatient care. IEEE Intell. Syst. 2013, 28, 92–95. [Google Scholar] [CrossRef]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Khanagar, S.B.; Al-Ehaideb, A.; Maganur, P.C.; Vishwanathaiah, S.; Patil, S.; Baeshen, H.A.; Sarode, S.C.; Bhandi, S. Developments, application, and performance of artificial intelligence in dentistry—A systematic review. J. Dent. Sci. 2021, 16, 508–522. [Google Scholar] [CrossRef] [PubMed]
- Heidbuchel, K.L.; Kuijpers-Jagtman, A.M. Maxillary and mandibular dental-arch dimensions and occlusion in bilateral cleft lip and palate patients from 3 to 17 years of age. Cleft Palate Craniofac. J. 1997, 34, 21–26. [Google Scholar] [CrossRef]
- Del Guercio, F.; Meazzini, M.C.; Garattini, G.; Morabito, A.; Semb, G.; Brusati, R. A cephalometric inter centre comparison of patients with unilateral cleft lip and palate at 5 and 10 years of age. Eur. J. Orthod. 2010, 32, 24–27. [Google Scholar] [CrossRef]
- Gopinath, V.K.; Ab Rani Samsudin, S.N.F.; Noor, M.; Sharab, H.Y.M. Facial profile and maxillary arch dimensions in unilateral cleft lip and palate children in the mixed dentition stage. Eur. J. Dent. 2017, 11, 76. [Google Scholar] [CrossRef]
- Silva Filho, O.G.; Calvano, F.; Assunção, A.G.; Cavassan, A.O. Craniofacial morphology in children with complete unilateral cleft lip and palate: A comparison of two surgical protocols. Angle Orthod. 2001, 71, 274–284. [Google Scholar]
- Schleyer, T.K.; Thyvalikakath, T.P.; Spallek, H.; Torres-Urquidy, M.H.; Hernandez, P.; Yuhaniak, J. Clinical computing in general dentistry. J. Am. Med. Inf. Assoc. 2006, 13, 344–352. [Google Scholar] [CrossRef]
- Patro, S.; Sahu, K.K. Normalization: A preprocessing stage. arXiv 2015, arXiv:1503.06462. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis; The Joanna Briggs Institute: Adelaide, Australia, 2020; Chapter 5; Available online: https://synthesismanual.jbi.global (accessed on 1 January 2021).
- Orozco-Arroyave, J.R.; Belalcazar-Bolanos, E.A.; Arias-Londoño, J.D.; Vargas-Bonilla, J.F.; Skodda, S.; Rusz, J.; Daqrouq, K.; Hönig, F.; Nöth, E. Characterization methods for the detection of multiple voice disorders: Neurological, functional, and laryngeal diseases. IEEE J. Biomed Health Inform. 2015, 19, 1820–1828. [Google Scholar] [CrossRef] [PubMed]
- Dubey, A.K.; Prasanna, S.M.; Dandapat, S. Detection and assessment of hypernasality in repaired cleft palate speech using vocal tract and residual features. J. Acoust. Soc. Am. 2019, 146, 4211–4223. [Google Scholar] [CrossRef] [PubMed]
- Phan, M.; Conte, F.; Khandelwal, K.D.; Ockeloen, C.W.; Bartzela, T.; Kleefstra, T.; van Bokhoven, H.; Rubini, M.; Zhou, H.; Carels, C.E. Tooth agenesis and orofacial clefting: Genetic brothers in arms? Hum. Genet. 2016, 135, 1299–1327. [Google Scholar] [CrossRef] [PubMed]
- Mathiyalagan, N.; Miles, L.B.; Anderson, P.J.; Wilanowski, T.; Grills, B.L.; McDonald, S.J.; Keightley, M.C.; Charzynska, A.; Dabrowski, M.; Dworkin, S. Meta-analysis of Grainyhead-like dependent transcriptional networks: A roadmap for identifying novel conserved genetic pathways. Genes 2019, 10, 876. [Google Scholar] [CrossRef]
- Lim, J.; Tanikawa, C.; Kogo, M.; Yamashiro, T. Determination of prognostic factors for orthognathic surgery in children with cleft lip and/or palate. Orthod. Craniofac. Res. 2021, 24, 153–162. [Google Scholar] [CrossRef]
- Carvajal-Castaño, H.A.; Orozco-Arroyave, J.R. Articulation Analysis in the Speech of Children with Cleft Lip and Palate. In Iberoamerican Congress on Pattern Recognition; Springer: Cham, Switzerland, 2019; pp. 575–585. [Google Scholar]
- Zhang, Y.; Pei, Y.; Guo, Y.; Chen, S.; Xu, T.; Zha, H. Cleft Volume Estimation and Maxilla Completion Using Cascaded Deep Neural Networks. In International Workshop on Machine Learning in Medical Imaging; Springer: Cham, Switzerland, 2020; pp. 332–341. [Google Scholar]
- Tanikawa, C.; Lee, C.; Lim, J.; Oka, A.; Yamashiro, T. Clinical applicability of automated cephalometric landmark identification: Part I—Patient-related identification errors. Orthod Craniofac Res. 2021, 24, 43–52. [Google Scholar] [CrossRef]
- Orozco-Arroyave, J.R.; Arias-Londoño, J.D.; Vargas-Bonilla, J.F.; Nöth, E. Automatic detection of hypernasal speech signals using nonlinear and entropy measurements. In Proceedings of the Thirteenth Annual Conference of the International Speech Communication Association, Portland, OR, USA, 9–13 September 2012. [Google Scholar]
- Mathad, V.C.; Chapman, K.; Liss, J.; Scherer, N.; Berisha, V. Deep learning-based prediction of hypernasality for clinical applications. In Proceedings of the ICASSP 2020–2020 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Barcelona, Spain, 4–8 May 2020; pp. 6554–6558. [Google Scholar]
- Machado, R.A.; de Oliveira Silva, C.; Martelli-Junior, H.; das Neves, L.T.; Coletta, R.D. Machine learning in prediction of genetic risk of non-syndromic oral clefts in the Brazilian population. Clin. Oral. Investig. 2021, 25, 1273–1280. [Google Scholar] [CrossRef]
- Zhang, S.J.; Meng, P.; Zhang, J.; Jia, P.; Lin, J.; Wang, X.; Chen, F.; Wei, X. Machine learning models for genetic risk assessment of infants with non-syndromic orofacial cleft. Genom. Proteom. Bioinform. 2018, 16, 354–364. [Google Scholar] [CrossRef]
- Alam, M.K.; Alfawzan, A.A.; Haque, S.; Mok, P.L.; Marya, A.; Venugopal, A.; Jamayet, N.B.; Siddiqui, A.A. Sagittal Jaw Relationship of Different Types of Cleft and Non-cleft Individuals. Front. Pediatr. 2021, 9, 651951. [Google Scholar] [CrossRef]
- Wang, X.; Yang, S.; Tang, M.; Yin, H.; Huang, H.; He, L. Hypernasality net: Deep recurrent neural network for automatic hypernasality detection. Int. J. Med. Inform. 2019, 129, 1–2. [Google Scholar] [CrossRef]
- Golabbakhsh, M.; Abnavi, F.; Kadkhodaei Elyaderani, M.; Derakhshandeh, F.; Khanlar, F.; Rong, P.; Kuehn, D.P. Automatic identification of hypernasality in normal and cleft lip and palate patients with acoustic analysis of speech. J. Acoust. Soc. Am. 2017, 141, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Tang, M.; Yang, S.; Yin, H.; Huang, H.; He, L. Automatic hypernasality detection in cleft palate speech using cnn. Circuits Syst. Signal Process 2019, 38, 3521–3547. [Google Scholar] [CrossRef]
- Orozco-Arroyave, J.R.; Vargas-Bonilla, J.F.; Vásquez-Correa, J.C.; Castellanos-Dominguez, C.G.; Nöth, E. Automatic detection of hypernasal speech of children with cleft lip and palate from Spanish vowels and words using classical measures and nonlinear analysis. Rev. Fac. Ing. Univ. Antioq. 2016, 80, 109–123. [Google Scholar] [CrossRef]
- Li, Y.; Cheng, J.; Mei, H.; Ma, H.; Chen, Z.; Li, Y. CLPNet: Cleft Lip and Palate Surgery Support with Deep Learning. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 3666–3672. [Google Scholar]
- Shafi, N.; Bukhari, F.; Iqbal, W.; Almustafa, K.M.; Asif, M.; Nawaz, Z. Cleft prediction before birth using deep neural network. J. Health Inform. 2020, 26, 2568–2585. [Google Scholar] [CrossRef]
- Aggarwal, R.; Sounderajah, V.; Martin, G.; Ting, D.S.; Karthikesalingam, A.; King, D.; Ashrafian, H.; Darzi, A. Diagnostic accuracy of deep learning in medical imaging: A systematic review and meta-analysis. NPJ Digit. Med. 2021, 4, 65. [Google Scholar] [CrossRef]
- Nilsson, N.J. Artificial Intelligence: A New Synthesis, 1st ed.; Morgan Kaufmann: San Francisco, CA, USA, 1998; pp. 1–7. [Google Scholar]
- Hung, H.C.; Wang, Y.C.; Wang, Y.C. Applications of Artificial Intelligence in Orthodontics. Taiwan J. Orthod. 2020, 32, 3. [Google Scholar]
- Mossey, P.A.; Shaw, W.C.; Munger, R.G.; Murray, J.C.; Murthy, J.; Little, J. Global oral health inequalities: Challenges in the prevention and management of orofacial clefts and potential solutions. Adv. Dent. Res. 2011, 23, 247–258. [Google Scholar] [CrossRef]
- Dhillon, H.; Chaudhari, P.K.; Dhingra, K.; Kuo, R.F.; Sokhi, R.K.; Alam, M.K.; Ahmad, S. Current Applications of Artificial Intelligence in Cleft Care: A Scoping Review. Front. Med. 2021, 8, 676490. [Google Scholar] [CrossRef]
- Ye, B.; Wu, Y.; Zhou, Y.; Jing, H.; Hu, J.; Zhang, G. A comparative cephalometric study for adult operated cleft palate and unoperated cleft palate patients. J. Craniomaxillofac. Surg. 2015, 43, 1218–1223. [Google Scholar] [CrossRef]
- Aras, I.; Baykal, D.; Bulut, M.; Dogan, S. Evaluation of mandibular hard and soft tissues in cleft patients. J. Istanb Univ. Fac. Dent. 2017, 51, 14–22. [Google Scholar] [CrossRef]
- Arshad, A.I.; Alam, M.K.; Khamis, M.F. Assessment of complete unilateral cleft lip and palate patients: Assessment of complete unilateral cleft lip and palate patients: Determination of factors effecting dental arch relationships. Int. J. Ped. Otorhinolaryngol. 2017, 92, 70–74. [Google Scholar] [CrossRef]
- Johnson, C.M., Jr.; Toriumi, D.M.; Daniel, R.K. Open structure rhinoplasty. Plast. Reconstr. Surg. 1990, 3, 594. [Google Scholar] [CrossRef]
- Kajii, T.S.; Alam, M.K.; Milkoya, T.; Oyama, A.; Matsuno, M.K.; Kato, Y.S. Congenital and postnatal factors including malocclusion in Japanese unilateral cleft lip and patient- determination using logistic regression analysis. Cleft Palate Craniofac. J. 2013, 50, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Baker, N.C.; Sipes, N.S.; Franzosa, J.; Belair, D.G.; Abbott, B.D.; Judson, R.S. Characterizing cleft palate toxicants using ToxCast data, chemical structure, and the biomedical literature. Birth Defects Res. 2020, 112, 19–39. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Nos | Keyword Strings | Results Obtained in Scopus (S) | Results Obtained in PubMed (P) | Results Obtained in Web of Science (W) | Articles Screened from Results According to Title (S + P + W) |
|---|---|---|---|---|---|
| 1 | Craniofacial anomaly + Oral clefts * + Artificial intelligence * | 0 | 2 | 0 | 02 |
| 2 | Artificial intelligence * + Cleft lip and palate * + automated landmarks | 01 | 0 | 01 | 02 |
| 3 | Oral cleft * + Machine learning * + prediction | 02 | 0 | 03 | 05 |
| 4 | Neural network * + Deep learning * + Cleft lip and palate * | 03 | 0 | 06 | 09 |
| 5 | Machine learning * + clefts * + sagittal relationship | 01 | 0 | 0 | 01 |
| 6 | Machine learning * + Genetic risk + Oral clefts * | 01 | 01 | 03 | 05 |
| 7 | Artificial intelligence * + anatomical variations + Cleft lip and palate * | 0 | 0 | 0 | 0 |
| 8 | Automatic detection + hypernasal speech + Cleft lip and palate * | 05 | 0 | 06 | 11 |
| 9 | Cleft Lip and Palate * + Surgery + Deep learning * | 02 | 01 | 02 | 05 |
| 10 | Facial morphology + oral clefts * + Machine learning * | 0 | 0 | 0 | 0 |
| 11 | Maxillofacial defect + Machine learning * + orofacial clefts * | 0 | 0 | 0 | 0 |
| 12 | Speech recognition + Artificial intelligence * + Oral clefts * | 0 | 0 | 0 | 0 |
| 13 | Artificial intelligence * + Orthognathic surgery + Prognostics factors | 01 | 0 | 01 | 02 |
| 14 | Artificial intelligence * + Dental characteristics + clefts * | 0 | 0 | 02 | 02 |
| Total | 16 | 04 | 24 | 44 |
| Test outcome (index test) | Disease status (reference standard result) | |
| True positives (a) | False positives (b) | Test positives (a + b) |
| False negatives (c) | True negatives (d) | Test negatives (c + d) |
| Index test positive (T+) | Index test negative (T−) | |
| Author Name with Year of Publication | Title of the Article | Reason for Exclusion |
|---|---|---|
| Orozco-Arroyave et al. [32] | Characterization methods for the detection of multiple voice disorders: Neurological, functional, and laryngeal diseases | The authors did not use any of the AI or machine learning techniques in this study. |
| Dubey et al. [33] | Detection and assessment of hypernasality in repaired cleft palate speech using vocal tract and residual features | The authors used different methods for detection and assessment of hypernasality in children with CLP but no AI or machine learning methods involved in the study. |
| Phan et al. [34] | Tooth agenesis and orofacial clefting: genetic brothers in arms? | This is a review paper on tooth agenesis and orofacial clefting based on genetic loci but did not mention about any AI models. |
| Mathiyalagan et al. [35] | Meta-Analysis of Grainyhead-Like Dependent Transcriptional Networks: A Roadmap for Identifying Novel Conserved Genetic Pathways | The meta-analysis was done to identify the genes causing oral clefting but no AI or Machine learning techniques used in this study |
| Lim et al. [36] | Determination of prognostic factors for orthognathic surgery in children with cleft lip and/or palate | Unable to download the full content of this study. |
| Carvajal-Castaño and Orozco-Arroyave, [37] | Articulation Analysis in the Speech of Children with Cleft Lip and Palate | This article is a chapter from the book “Progress in Pattern Recognition Image Analysis, Computer Vision and Applications”. |
| Zhang et al. [38] | Cleft Volume Estimation and Maxilla Completion Using Cascaded Deep Neural Networks | This paper is a chapter from the book “Machine Learning in Medical Imaging”. |
| Tanikawa et al. [39] | Clinical applicability of automated cephalometric landmark identification: Part I—Patient-related identification errors | Unable to download the full text article. |
| Author | Target Condition | Sample Size | AI Technique and Method Employed | Findings |
|---|---|---|---|---|
| Machado et al. [42] | Genetic risk assessment in non-syndromic CLP | 722 Brazilian subjects with NSCL ± P and 866 without NSCL ± P | RF and multi-layer NN. The genetic risk of NSCL ± P in the Brazilian population was developed by putting 72 known SNPs to RF, which was then used to identify important SNPs. Multiple regression was used to assess the interactions between the SNPs. | 13 SNPs were found to be highly predictive to detect NSCL ± P. The combination of these SNPs was able to split the controls from NSCL ± P with highest accuracy rate of 94.5%. |
| Zhang et al. [43] | 504 East asians,103 Han Chinese and 279 Uyghur Chinese with CLP | SVM, LR, NB, DT, RF, k-NN, and ANN. Machine learning techniques were used to validate the diagnostic ability of 43 SNP candidates in assessing genetic risk in Chinese populations. After manual selection, a panel of 24 SNPs was assessed for risk assessment efficiency. Each time the LR-based model was trained, an SNP was removed or added in a sequential manner. | In the Han population, the LR model produced the greatest results for genetic risk assessment, whereas the SVM produced better results in the Uyghur group. The relative risk score methodology produced the greatest results in the Uyghur population. SNPs in three genes involved in folic acid and vitamin A production were found to play a critical role in the occurrence of NSCL ± P. | |
| Alam et al. [44] | Sagittal jaw relationship in cleft and non-cleft individuals | 123 Saudi Arabian patients 21 BCLP, 41 UCLP, 13 UCL, 9 UCLA and 31 NC individuals | AI driven WebCeph software. The LCRs of patients were used to measure 4 different parameters such as SNA, SNB, ANB and Wits appraisal. | The comparison of sagittal development among different types of clefts with NC subjects revealed significant smaller SNA, ANB angles and Wits appraisal. However, there was no significant variation observed in SNB angle between cleft and non-cleft subjects. Also, there was no significant difference found in terms of gender and types of clefts. |
| Alam and Alfawzan [19] | Dental characteristics in cleft and non- cleft individuals | 123 Saudi Arabian subjects 92 cleft and 31 non-cleft individuals | AI driven lateral cephalometric analysis was done using WebCeph software. 14 different dental characteristics such as OJ, OB U1 to FH, U1 to SN U1 to UOP, IMPA L1 to LOP, IIA, COP U1 to NA (mm), U1 to NA (degree), L1 to NB (mm), L1 to NB (degree), UID were evaluated. | Significant disparities among cleft and NC subjects were found in relation to Overjet, U1 to FH, U1 to SN, U1 to IMPA, IIA, U1 to NA (degree) and L1 to NB (degree). However, no significant differences were observed between cleft and NC in relation to OB, U1 to UOP, L1 to LOP, COP, U1 to NA (mm), L1 to NB (mm) and UID. AI based cephalometric assessment showed 95.6% accuracy. |
| Wang et al. [45] | Detection of Hypernasality in cleft palate patients | 144 Chinese patients (72 with hypernasality and 72 controls) | LSTM-DRNN method which is used for automatic detection of hypernasal speech, vocal cords related feature mining, classification ability and analysis of hypernasality- sensitive vowels. | LSTM-DRNN achieved highest 91.10% accuracy in automatic hypernasal speech detection compared with shallow classifiers. The GD spectrum and PSD have shown 93.35% and 90.26% accuracy, respectively. |
| Golabbakhsh et al. [46] | 15 CLP patients and 15 controls (Iranian population) | SVM. Automatic detection of hypernasality with acoustic analysis of Speech. Mel frequency, bionet wavelet transform entropy. | When combined with SVM, Mel frequency and bionet wavelet transform energy 85% of the accuracy have been achieved in identifying hypernasality. | |
| Wang et al. [47] | 62 Children and 48 adults (Chinese patients) | CNN. Hypernasality detection. | A hypernasality detection accuracy of 93.34% was achieved with CNN compared with state-of-the-art literature. | |
| Orozco-Arroyave et al. [48] | South American children with CLP | SVM. Automatic identification of hypernasal speech of Spanish vowels using classical and non-linear analysis | The NLD analysis provide relevant information and can be used as an alternative classical Mel frequency in automatic detection of hypernasality in Spanish vowels. The greater accuracy of 95.4% was achieved with only NLD features. | |
| Orozco-Arroyave et al. [40] | Spanish subjects Cases 130 Controls 108 German subjects Cases 429 Controls 39 | A SVM was used to determine whether a voice recording is hypernasal or healthy. | It was found that the combination of NLD features and entropy measurements yield best results. The addition of information provided by the five vowels in the discriminating process results in an improvement in system performance for each vowel. | |
| Mathad et al. [41] | 75 cases 251 controls (American population) | A DNN classifier was created to distinguish between nasal and non-nasal speech sounds using a healthy voice corpus. | The proposed DNN method employs forced-alignment, which could lead to incorrect segmentation and impact the hypernasality estimator’s effectiveness. | |
| Li et al. [49] | Cleft lip and palate surgery | 2568 CLP cases (Chinese population) | Deep learning technique for CLP surgery. Train the model to locate surgical incisions and markers. State-of-the-art Hour glass architecture and residual learning models were used to create strong baseline dataset. | CLPNet-Light and VGG are significantly better than two CSR-based techniques. The CLPNet-Light is 2.5 times higher than CLPNet which has strong robustness and can be used to train the model to aid in surgical marker localization. |
| Shafi et al. [50] | Prediction of oral cleft | 1000 Pakistani subjects (500 cases and 500 controls) | DNN. A questionnaire was designed to collect information on 36 input characteristics from mothers, half of whom had cleft babies and the other half were controls. Data was gathered and various prediction models were used. The precision of the results obtained with each were assessed. | On test data, the MLP model with three hidden layers and 28 perceptrons in each provided the highest classification accuracy rate of 92.6%. |
| No | Authors | Country | Study Design | Sample Size (n) | Quality Assessment (%) | Risk of Bias Rating |
|---|---|---|---|---|---|---|
| 1 | Machado et al. [42] | Brazil | Retrospective Case control | 1588 | 90.0 | LOW |
| 2 | Zhang et al. [43] | China | Retrospective Case control | 171 | 90.0 | LOW |
| 3 | Alam et al. [44] | Saudi Arabia | Retrospective Case control | 123 | 80.0 | LOW |
| 4 | Alam and Alfawzan [19] | Saudi Arabia | Retrospective Case control | 123 | 80.0 | LOW |
| 5 | Wang et al. [45] | China | Retrospective Case control | 144 | 60.0 | MODERATE |
| 6 | Golabbakhsh et al. [46] | Iran | Retrospective Case-control | 30 | 80.0 | LOW |
| 7 | Wang et al. [47] | China | Retrospective Case control | 110 | 80.0 | LOW |
| 8 | Orozco-Arroyave et al. [48] | South America | Retrospective Case control | 238 | 80.0 | LOW |
| 9 | Orozco-Arroyave et al. [40] | South America | Retrospective Case control | 202 | 90.0 | LOW |
| 10 | Mathad et al. [41] | South America | Retrospective Case control | 326 | 50.0 | HIGH |
| 11 | Li et al. [49] | China | Retrospective | 2568 | 50.0 | HIGH |
| 12 | Shafi et al. [50] | Pakistan | Prospective | 1000 | 70.0 | LOW |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huqh, M.Z.U.; Abdullah, J.Y.; Wong, L.S.; Jamayet, N.B.; Alam, M.K.; Rashid, Q.F.; Husein, A.; Ahmad, W.M.A.W.; Eusufzai, S.Z.; Prasadh, S.; et al. Clinical Applications of Artificial Intelligence and Machine Learning in Children with Cleft Lip and Palate—A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10860. https://doi.org/10.3390/ijerph191710860
Huqh MZU, Abdullah JY, Wong LS, Jamayet NB, Alam MK, Rashid QF, Husein A, Ahmad WMAW, Eusufzai SZ, Prasadh S, et al. Clinical Applications of Artificial Intelligence and Machine Learning in Children with Cleft Lip and Palate—A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(17):10860. https://doi.org/10.3390/ijerph191710860
Chicago/Turabian StyleHuqh, Mohamed Zahoor Ul, Johari Yap Abdullah, Ling Shing Wong, Nafij Bin Jamayet, Mohammad Khursheed Alam, Qazi Farah Rashid, Adam Husein, Wan Muhamad Amir W. Ahmad, Sumaiya Zabin Eusufzai, Somasundaram Prasadh, and et al. 2022. "Clinical Applications of Artificial Intelligence and Machine Learning in Children with Cleft Lip and Palate—A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 17: 10860. https://doi.org/10.3390/ijerph191710860
APA StyleHuqh, M. Z. U., Abdullah, J. Y., Wong, L. S., Jamayet, N. B., Alam, M. K., Rashid, Q. F., Husein, A., Ahmad, W. M. A. W., Eusufzai, S. Z., Prasadh, S., Subramaniyan, V., Fuloria, N. K., Fuloria, S., Sekar, M., & Selvaraj, S. (2022). Clinical Applications of Artificial Intelligence and Machine Learning in Children with Cleft Lip and Palate—A Systematic Review. International Journal of Environmental Research and Public Health, 19(17), 10860. https://doi.org/10.3390/ijerph191710860