
Polish Translation and Validation of the Voice Handicap Index (VHI-30)

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Translation from English to Polish
2.2. Setting
2.3. Participants
2.4. Psychometric and Statistical Analyses
3. Results
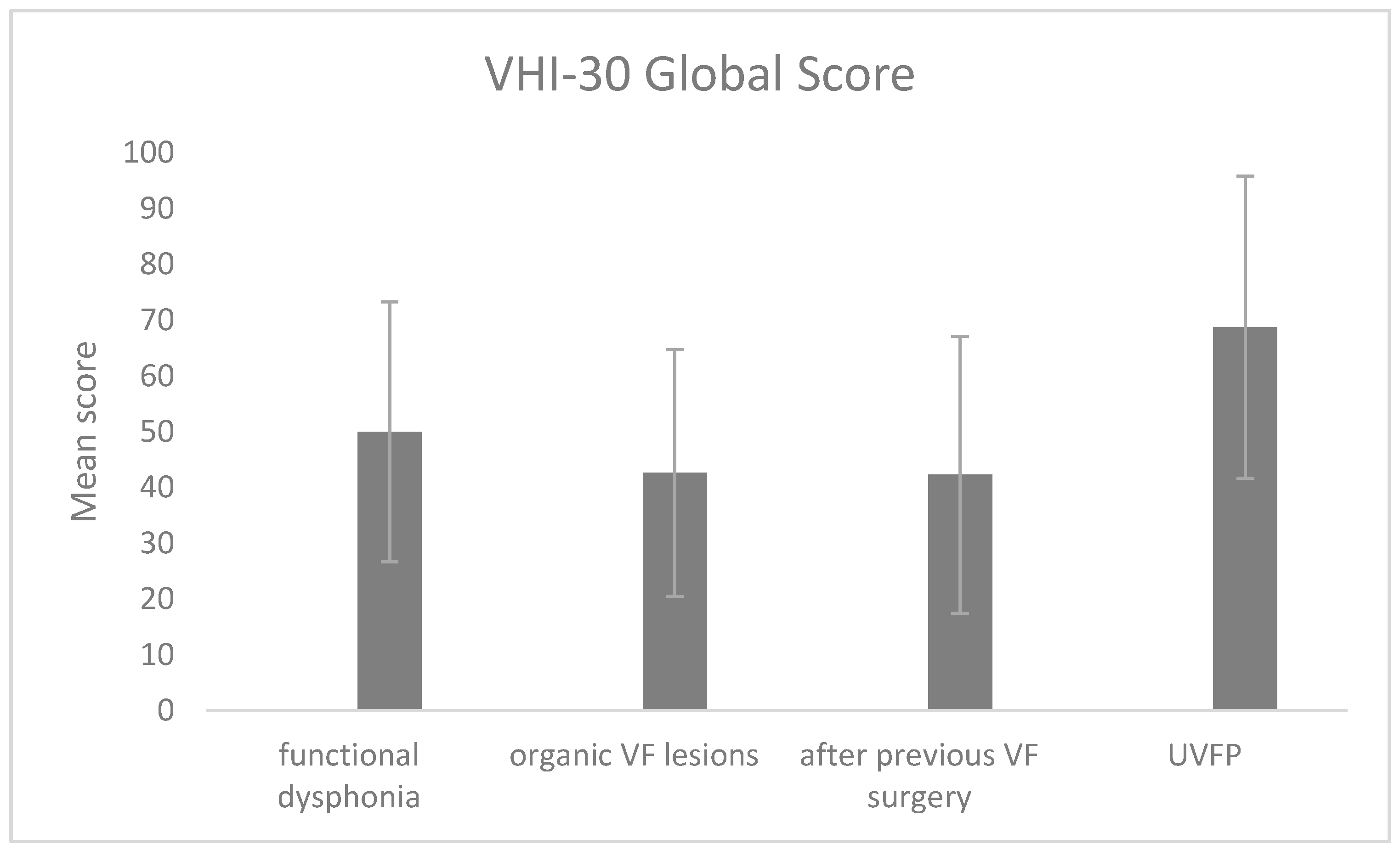
3.1. VHI-POL Items, Subscales, and Global Score
3.2. Criterion Validity
3.3. Internal Consistency
3.4. Reproducibility and Agreement
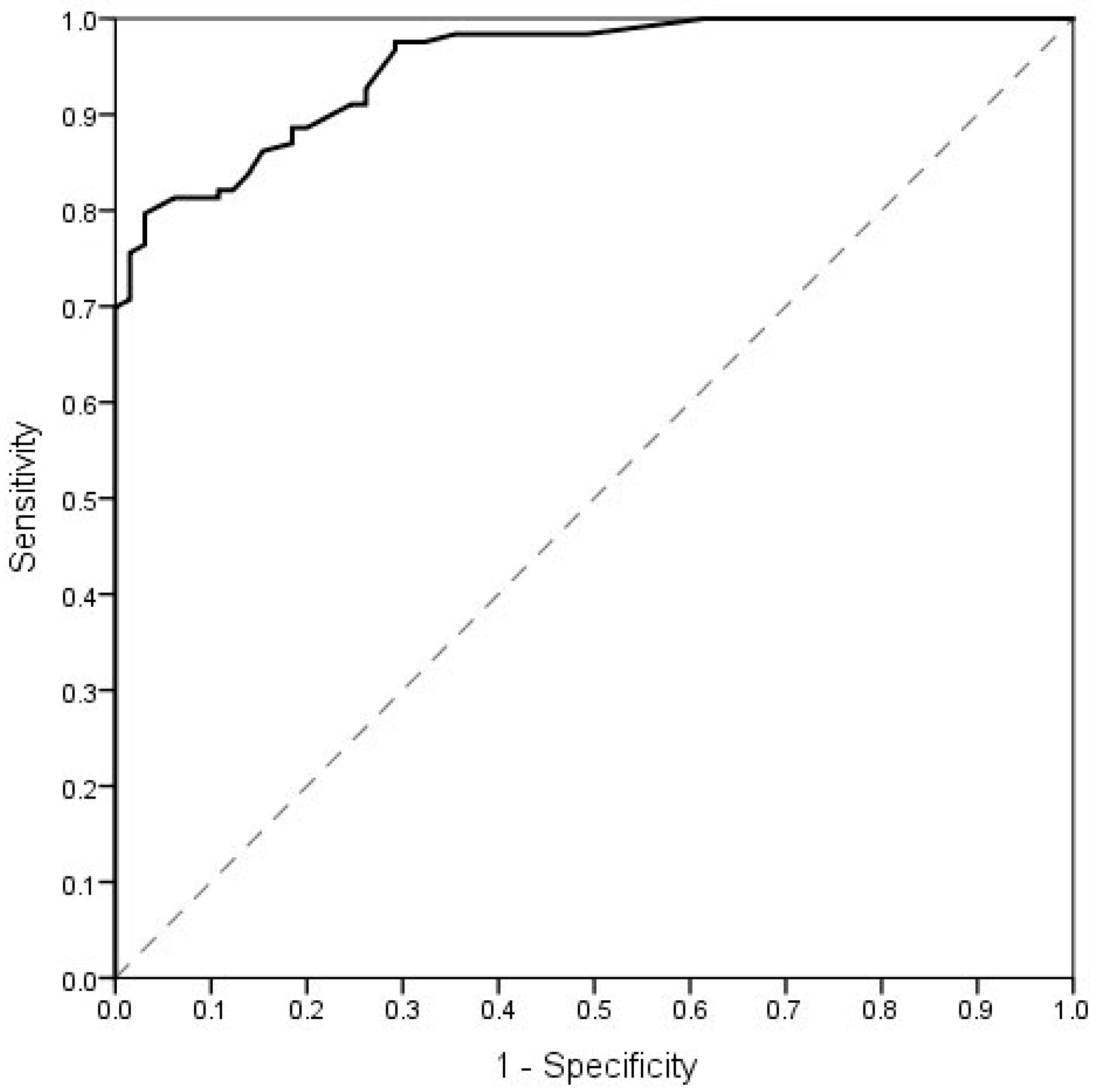
3.5. Cut-Off Value for VHI-POL Global Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arffa, R.E.; Krishna, P.; Gartner-Schmidt, J.; Rosen, C.A. Normative values for the Voice Handicap Index-10. J. Voice 2012, 26, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Sotirovic, J.; Grgurevic, A.; Mumovic, G.; Grgurevic, U.; Pavicevic, L.; Peric, A.; Erdoglija, M.; Milojevic, M. Adaptation and validaton of the Voice Handicap Index (VHI)-30 into Serbian. J. Voice 2016, 30, 758.e1–758.e6. [Google Scholar] [CrossRef]
- Behlau, M.; Dos Santos, L.D.M.A.; Oliveira, G. Cross-cultural adaptation and validation of the voice handicap index into Brazilian Portuguese. J. Voice 2011, 25, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Dejonckere, P.H.; Bradley, P.; Clemente, P.; Cornut, G.; Crevier-Buchman, L.; Friedrich, G.; De Heyning, P.; Remacle, M.; Woisard, V. A basic protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Eur. Arch. Otorhinolaryngol. 2001, 258, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, B.; Johnson, A.; Grywalski, C.; Silbergleit, A.; Jacobson, G.; Benninger, M.S.; Newman, C.W. The Voice Handicap Index (VHI): Development and validation. Am. J. Speech-Lang. Pathol. 1997, 6, 66–70. [Google Scholar] [CrossRef]
- Hogikyan, N.D.; Sethuraman, G. Validation of new instrument to measure Voice-Related Quality of Life (V-RQOL). J. Voice 1999, 13, 557–569. [Google Scholar] [CrossRef]
- Ma, E.P.-M.; Yiu, E.M.-L. Voice activities and participation profile: Assessing the impact of voice disorders on daily activities. J. Speech Lang. Hear. Res. 2001, 44, 511–524. [Google Scholar] [CrossRef]
- Deary, I.J.; Wilson, J.A.; Carding, P.N.; MacKenzie, K. VoiSS: A patient -derived Voice Symptom Scale. J. Psychosom. Res. 2003, 54, 483–489. [Google Scholar] [CrossRef]
- Lam, P.K.; Chan, K.M.; Ho, W.K.; Kwong, E.; Yiu, E.M.; Wei, W.I. Cross-cultural adaptation and validation of the Chinese Voice Handicap Index-10. Laryngoscope 2006, 116, 1192–1198. [Google Scholar] [CrossRef]
- Nawka, T.; Verdonck-de Leeuw, I.M.; De Bodt, M.; Guimaraes, I.; Holmberg, E.B.; Rosen, C.A.; Schindler, A.; Woisard, V.; Whurr, R.; Konerding, U. Item reduction of the Voice Handicap Index based on the original version and the European translations. Folia Phoniatr. Logop. 2009, 61, 37–48. [Google Scholar] [CrossRef]
- Nawka, T.; Wiesman, U.; Gonnermann, U. Validation of the German version of the Voice Handicap Index. HNO 2003, 51, 921–930. [Google Scholar] [CrossRef]
- Hakkesteegt, M.M.; Wieringa, M.H.; Gerritsma, E.J.; Feenstra, L. Reproducibility of the Dutch version of the Voice Handicap Index. Folia Phoniatr. Logop. 2006, 58, 132–138. [Google Scholar] [CrossRef]
- Nunez-Batalla, F.; Corte-Santoz, P.; Senariz-Gonzalez, B.; Llorente-Pendas, J.L.; Gorriz-Gil, C.; Suarez-Nieto, C. Adaptation and validation to the Spanish of the Voice Handicap Index (VHI-30) and its shortened version (VHI-10). Acta Otorrinolaringol. Esp. 2007, 58, 386–392. [Google Scholar] [CrossRef]
- Schindler, A.; Ottaviani, F.; Mozzanica, F.; Bachmann, C.; Favero, E.; Schettino, I.; Ruoppolo, G. Cross-cultural adaptation and validation of the Voice Handicap Index into Italian. J. Voice 2010, 24, 708–717. [Google Scholar] [CrossRef]
- Helidoni, M.E.; Murry, T.; Moschandreas, J.; Lionis, C.; Printza, A.; Velegrakis, G.A. Cross-cultural adaptation and validation of the Voice Handicap Index into Greek. J. Voice 2010, 24, 221–227. [Google Scholar] [CrossRef]
- Malki, K.H.; Mesallam, T.A.; Farahat, M.; Bukhari, M.; Murry, T. Validation and cultural modification of Arabic Voice Handicap Index. Eur. Arch. Otorhinolaryngol. 2010, 267, 1743–1751. [Google Scholar] [CrossRef]
- Bonetti, A.; Bonetti, L. Cross-cultural adaptation and validation of the Voice Handicap Index into Croatian. J. Voice 2013, 27, 130.e7–130.e14. [Google Scholar] [CrossRef]
- Moradi, N.; Pourshahbaz, A.; Soltani, M.; Javadipour, S.; Hashemi, H.; Soltaninejad, N. Cross-cultural equivalence and evaluation of psychometric properties of voice handicap index into Persian. J. Voice 2013, 27, 258.e15–258.e22. [Google Scholar] [CrossRef]
- Trinite, B.; Sokolovs, J. Adaptation and validation of the Voice Handicap Index in Latvian. J. Voice 2014, 28, 452–457. [Google Scholar] [CrossRef]
- Frajkova, Z.; Krizekova, A.; Missikova, V.; Tedla, M. Translation, cross-cultural validation of the Voice Handicap Index (VHI-30) in Slovak language. J. Voice 2016, 36, 145.e1–145.e6. [Google Scholar] [CrossRef]
- Verdonck-de Leeuw, I.M.; Kuik, D.J.; De Bodt, M.; Guimaraes, I.; Holmberg, E.B.; Nawka, T.; Rosen, C.A.; Schindler, A.; Whurr, R.; Woisard, V. Validation of the voice handicap index by assessing equivalence of European translations. Folia Phoniatr. Logop. 2008, 60, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Hsiung, M.-W.; Pai, L.; Wang, H.-W. Correlation between Voice Handicap Index and voice laboratory measurements in dysphonic patients. Eur. Arch. Otolaryngol. 2002, 259, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Woisard, V.; Bodin, S.; Yardeni, E.; Puech, M. The Voice Handicap Index: Correlation between subjective patient response and quantitative assessment of voice. J. Voice 2007, 5, 623–631. [Google Scholar] [CrossRef]
- Sielska-Badurek, E.; Rzepakowska, A.; Sobol, M.; Osuch-Wójcikiewicz, E.; Niemczyk, K. Adaptation and Validation of the Voice- Related Quality of Life Measure Into Polish. J. Voice 2016, 30, 773.e7–773.e12. [Google Scholar] [CrossRef]
- Pruszewicz, A.; Obrębowski, A.; Wiskirska-Woźnica, B.; Wojnowski, W. Complex voice assessment: Polish version of the Voice Handicap Index (VHI). Otolaryngol. Pol. 2004, 58, 547–549. [Google Scholar]
- de Vet, H.C.W.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine. A Practical Guide; University Press: Cambridge, UK, 2011. [Google Scholar]
- Speyer, R.; Bogaardt, H.C.A.; Passos, V.L.; Roodenburg, N.; Zumach, A.; Heijnen, M.A.M.; Baijens, L.W.J.; Fleskens, S.; Brunings, J.W. Maximum phonation time: Variability and reliability. J. Voice 2010, 24, 281–284. [Google Scholar] [CrossRef]
- Nicastri, M.; Chiarella, G.; Gallo, L.V. Catalano, M.; Cassandro, E. Multidimensional Voice Program (MDVP) and amplitude variation parameters in euphonic adult subjects. Normative study. Acta Otorhinolaryngol. Ital. 2004, 24, 337–341. [Google Scholar]
- Hirano, M. Psycho-acoustic evaluation of voice. In Clinical Examination of Voice; Arnold, G.E., Winckel, F., Wyke, B.D., Eds.; Springer: New York, NY, USA, 2018; pp. 81–84. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988; pp. 79–80. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory; Mc Graw Hill: New York, NY, USA, 1994. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 8, 307–310. [Google Scholar] [CrossRef]
- Rosen, C.A.; Lee, A.S.; Osborne, J.; Zullo, T.; Murry, T. Development and validation of the Voice Handicap Index-10. Laryngoscope 2004, 114, 1549–1556. [Google Scholar] [CrossRef]
- Amir, O.; Ashkenazi, O.; Leibovitzh, T.; Michael, O.; Tavor, Y.; Wolf, M. Applying the Voice Handicap Index (VHI) to dysphonic and nondysphonic Hebrew speakers. J. Voice 2006, 20, 318–324. [Google Scholar] [CrossRef]
- Kooijman, P.; Thomas, G.; Graamans, K.; de Jong, F. Psychological impact of the teacher’s voice throughout the career. J. Voice 2007, 21, 316–324. [Google Scholar] [CrossRef]
- Niebudek-Bogusz, E.; Kuzańska, A.; Woźnicka, E.; Śliwińska-Kowalska, M. Assessment of the Voice Handicap Index as screening tool in dysphonic patients. Folia Phoniatr. Logop. 2011, 63, 269–272. [Google Scholar] [CrossRef]
- Schindler, A.; Mozzanica, F.; Vedrody, M.; Maruzzi, P.; Ottaviani, F. Correlation between the Voice Handicap Index and voice measurements in four groups of patients with dysphonia. Otolaryngol. Head Neck Surg. 2009, 141, 762–769. [Google Scholar] [CrossRef]
- Dehqan, A.; Yadegari, F.; Scherer, R.C.; Dabirmoghadam, P. Correlation of VHI-30 to acoustic measurements across three common voice disorders. J. Voice 2017, 31, 34–40. [Google Scholar] [CrossRef]
- Karlsen, T.; Sandvik, L.; Heimdal, J.H.; Aarstad, H.J. Acoustic voice analysis and maximum phonation time in relation to Voice Handicap Index score and larynx disease. J. Voice 2020, 34, 161.e27–161.e35. [Google Scholar] [CrossRef]
- Wheeler, K.M.; Collins, S.P.; Sapienza, C.M. The relationship between VHI scores and specific acoustic measures of mildly disordered voice production. J. Voice 2006, 20, 308–317. [Google Scholar] [CrossRef]
- Fujiki, R.B.; Thibeault, S. Examining relationship between GRBAS ratings and acoustic, aerodynamic and patient-reported voice measures in adults with voice disorders. J. Voice 2021. [Google Scholar] [CrossRef]
- Ng, E.; Law, T.; Tang, E.C.; Ho, F.N.; Tong, M.C.; Lee, K.Y. The Cutoff Point and Diagnostic Accuracy of the Voice Handicap Index in Cantonese-Speaking Population. J. Voice 2021, 35, 163–168. [Google Scholar] [CrossRef]
- Behlau, M.; Madazio, G.; Moreti, F.; Oliveira, G.; Dos Santos, L.d.M.; Paulinelli, B.R.; Couto, E.d.B., Jr. Efficiency and Cutoff Values of Self-Assessment Instruments on the Impact of a Voice Problem. J. Voice 2016, 30, 506.e9–506.e18. [Google Scholar] [CrossRef] [PubMed]
- Moradi, N.; Pourshahbaz, A.; Soltani, M.; Javadipour, S. Cutoff point at Voice Handicap Index used to screen voice disorders among persian speakers. J. Voice 2013, 27, 130.e1–130.e5. [Google Scholar] [CrossRef] [PubMed]
- Tafiadis, D.; Helidoni, M.E.; Chronopoulos, S.K.; Kosma, E.I.; Ziavra, N.; Velegrakis, G.A. Cross-cultural Adaptation and Validation of the Greek Voice Handicap Index-10 (GVHI-10) With Additional Receiver Operating Characteristic Analysis. J. Voice 2020, 34, 304.e1–304.e8. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Number of Item | Study Group | Control Group | ||||
|---|---|---|---|---|---|---|
| Range | M | SD | Range | M | SD | |
| VHI_1 | 0–4 | 1.64 | 1.00 | 0–3 | 0.46 | 0.73 |
| VHI_2 | 0–4 | 1.75 | .98 | 0–3 | 0.52 | 0.80 |
| VHI_3 | 0–4 | 1.99 | 1.20 | 0–3 | 0.62 | 0.88 |
| VHI_4 | 0–4 | 2.35 | 0.96 | 0–3 | 0.71 | 0.89 |
| VHI_5 | 0–4 | 1.68 | 1.16 | 0–4 | 0.48 | 0.94 |
| VHI_6 | 0–4 | 1.20 | 1.15 | 0–3 | 0.11 | 0.47 |
| VHI_7 | 0–4 | 1.81 | 1.24 | 0–2 | 0.11 | 0.40 |
| VHI_8 | 0–4 | 1.23 | 1.24 | 0–1 | 0.03 | 0.17 |
| VHI_9 | 0–4 | 1.41 | 1.15 | 0–2 | 0.18 | 0.43 |
| VHI_10 | 0–4 | 2.01 | 1.26 | 0–2 | 0.12 | 0.42 |
| VHI_11 | 0–4 | 1.13 | 1.16 | 0–1 | 0.06 | 0.24 |
| VHI_12 | 0–4 | 1.44 | 1.11 | 0–2 | 0.31 | 0.66 |
| VHI_13 | 0–4 | 1.87 | 1.02 | 0–2 | 0.32 | 0.64 |
| VHI_14 | 0–4 | 2.24 | 1.05 | 0–2 | 0.31 | 0.61 |
| VHI_15 | 0–4 | 1.59 | 1.23 | 0–2 | 0.12 | 0.45 |
| VHI_16 | 0–4 | 1.44 | 1.19 | 0–1 | 0.02 | 0.12 |
| VHI_17 | 0–4 | 2.12 | 1.10 | 0–2 | 0.37 | 0.60 |
| VHI_18 | 0–4 | 1.92 | 1.21 | 0–2 | 0.28 | 0.63 |
| VHI_19 | 0–4 | 1.07 | 1.15 | 0–2 | 0.03 | 0.25 |
| VHI_20 | 0–4 | 1.77 | 1.18 | 0–2 | 0.17 | 0.45 |
| VHI_21 | 0–4 | 2.06 | 1.18 | 0–3 | 0.38 | 0.74 |
| VHI_22 | 0–4 | 0.80 | 1.18 | 0–0 | 0.00 | 0.00 |
| VHI_23 | 0–4 | 2.52 | 1.23 | 0–2 | 0.28 | 0.63 |
| VHI_24 | 0–4 | 1.38 | 1.31 | 0–2 | 0.05 | 0.28 |
| VHI_25 | 0–4 | 1.12 | 1.23 | 0–1 | 0.02 | 0.12 |
| VHI_26 | 0–4 | 1.91 | 1.03 | 0–2 | 0.43 | 0.73 |
| VHI_27 | 0–4 | 1.55 | 1.22 | 0–2 | 0.34 | 0.67 |
| VHI_28 | 0–4 | 1.42 | 1.20 | 0–2 | 0.25 | 0.53 |
| VHI_29 | 0–4 | 1.27 | 1.17 | 0–2 | 0.08 | 0.32 |
| VHI_30 | 0–4 | 1.41 | 1.32 | 0–1 | 0.02 | 0.12 |
| Emotional subscale | 0–39 | 15.48 | 10.03 | 0–12 | 1.43 | 2.46 |
| Functional subscale | 0–38 | 13.62 | 9.20 | 0–14 | 2.11 | 2.95 |
| Physical subscale | 0–37 | 20.00 | 8.00 | 0–15 | 3.61 | 4.49 |
| Global score | 2–107 | 49.11 | 25.67 | 0–31 | 7.16 | 9.02 |
| MDVP Parameter | VHI-E | VHI-F | VHI-P | VHI Global |
|---|---|---|---|---|
| F0 | 0.15 | 0.12 | 0.16 | 0.15 |
| Jitt | 0.17 | 0.22 * | 0.23 * | 0.23 * |
| RAP | 0.18 | 0.23 * | 0.21 * | 0.23 * |
| PPQ | 0.18 | 0.23 * | 0.23 * | 0.24 * |
| sPPQ | 0.12 | 0.18 | 0.20 * | 0.18 |
| vF0 | 0.14 | 0.16 | 0.23 * | 0.19 * |
| Shim | 0.19 * | 0.24 * | 0.19 * | 0.22 * |
| APQ | 0.23 * | 0.26 ** | 0.23 * | 0.25 ** |
| sAPQ | 0.18 | 0.22 * | 0.23 * | 0.22 * |
| vAm | 0.18 | 0.16 | 0.24 * | 0.20 * |
| NHR | −0.02 | 0.02 | 0.04 | 0.01 |
| SPI | 0.08 | 0.07 | 0.01 | 0.07 |
| VHI Subscale and Scale | G | R | B | A | S |
|---|---|---|---|---|---|
| Emotional | 0.27 ** | 0.25 ** | 0.24 ** | 0.34 *** | 0.29 ** |
| Functional | 0.26 ** | 0.26 ** | 0.31 ** | 0.36 *** | 0.26 ** |
| Physical | 0.35 *** | 0.36 *** | 0.31 ** | 0.26 ** | 0.34 ** |
| Global score | 0.30 ** | 0.31 ** | 0.29 ** | 0.34 ** | 0.32 ** |
| Test M (SD) | Retest M (SD) | Mean Difference | SD | Limits of Agreement | % Agreement | |
|---|---|---|---|---|---|---|
| VHI-E | 16.00 (10.32) | 17.16 (11.54) | −1.16 | 5.44 | 9.51; −11.83 | 95.7% |
| VHI-F | 13.74 (9.29) | 14.54 (9.70) | −0.80 | 4.99 | 8.98; −10.57 | 94.2% |
| VHI-P | 20.65 (7.47) | 20.80 (7.99) | −0.14 | 4.18 | 8.04; −8.33 | 94.2% |
| VHI-30 Global score | 50.39 (25.38) | 52.49 (27.93) | −2.10 | 12.65 | 22.68; −26.89 | 92.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miaśkiewicz, B.; Gos, E.; Dębińska, M.; Panasiewicz-Wosik, A.; Kapustka, D.; Nikiel, K.; Włodarczyk, E.; Domeracka-Kołodziej, A.; Krasnodębska, P.; Szkiełkowska, A. Polish Translation and Validation of the Voice Handicap Index (VHI-30). Int. J. Environ. Res. Public Health 2022, 19, 10738. https://doi.org/10.3390/ijerph191710738
Miaśkiewicz B, Gos E, Dębińska M, Panasiewicz-Wosik A, Kapustka D, Nikiel K, Włodarczyk E, Domeracka-Kołodziej A, Krasnodębska P, Szkiełkowska A. Polish Translation and Validation of the Voice Handicap Index (VHI-30). International Journal of Environmental Research and Public Health. 2022; 19(17):10738. https://doi.org/10.3390/ijerph191710738
Chicago/Turabian StyleMiaśkiewicz, Beata, Elżbieta Gos, Małgorzata Dębińska, Aleksandra Panasiewicz-Wosik, Dorota Kapustka, Katarzyna Nikiel, Elżbieta Włodarczyk, Anna Domeracka-Kołodziej, Paulina Krasnodębska, and Agata Szkiełkowska. 2022. "Polish Translation and Validation of the Voice Handicap Index (VHI-30)" International Journal of Environmental Research and Public Health 19, no. 17: 10738. https://doi.org/10.3390/ijerph191710738
APA StyleMiaśkiewicz, B., Gos, E., Dębińska, M., Panasiewicz-Wosik, A., Kapustka, D., Nikiel, K., Włodarczyk, E., Domeracka-Kołodziej, A., Krasnodębska, P., & Szkiełkowska, A. (2022). Polish Translation and Validation of the Voice Handicap Index (VHI-30). International Journal of Environmental Research and Public Health, 19(17), 10738. https://doi.org/10.3390/ijerph191710738