
Severity and Treatment Difficulty of Impacted Maxillary Canine among Orthodontic Patients in Riyadh, Saudi Arabia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Panoramic Radiographs
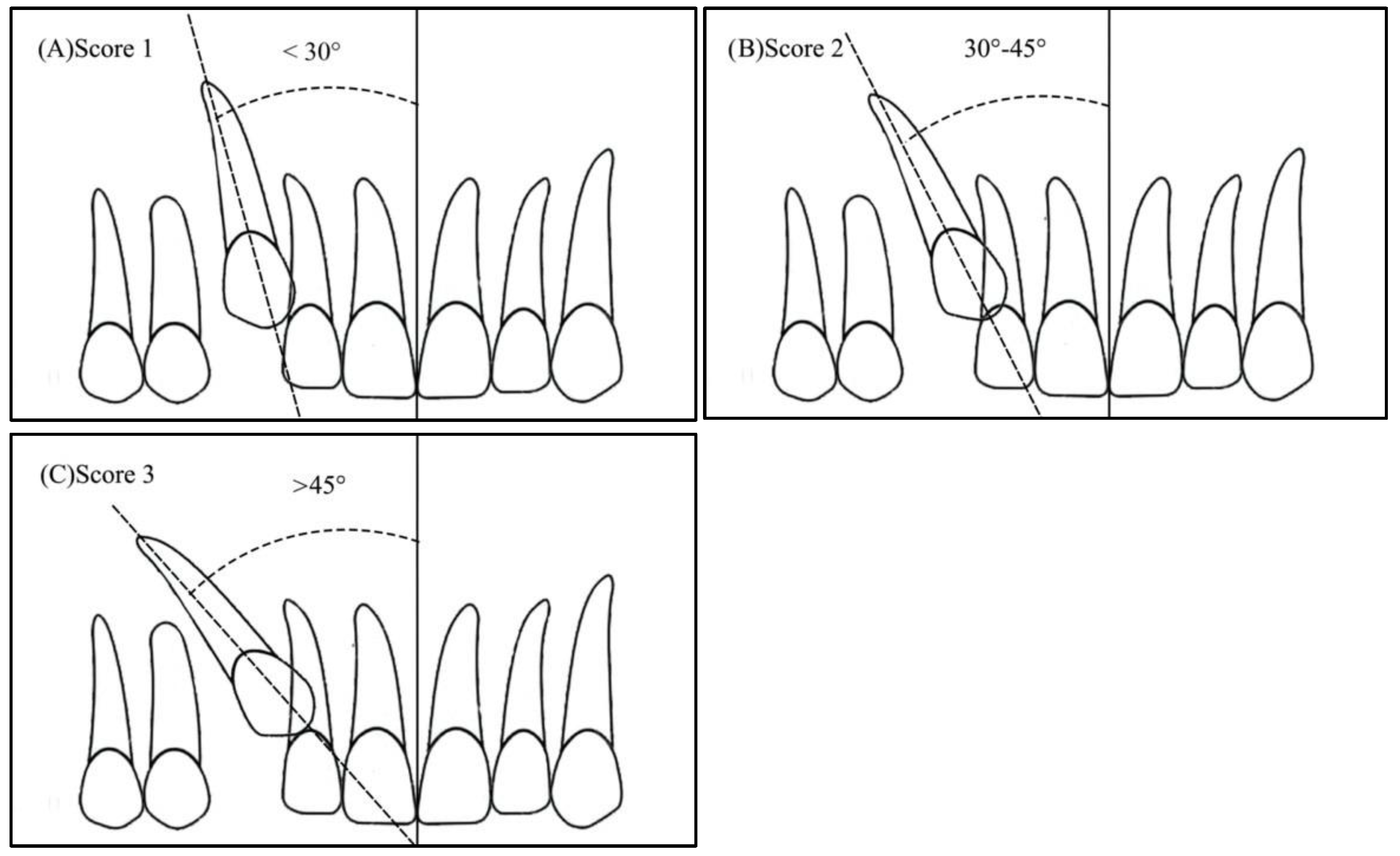
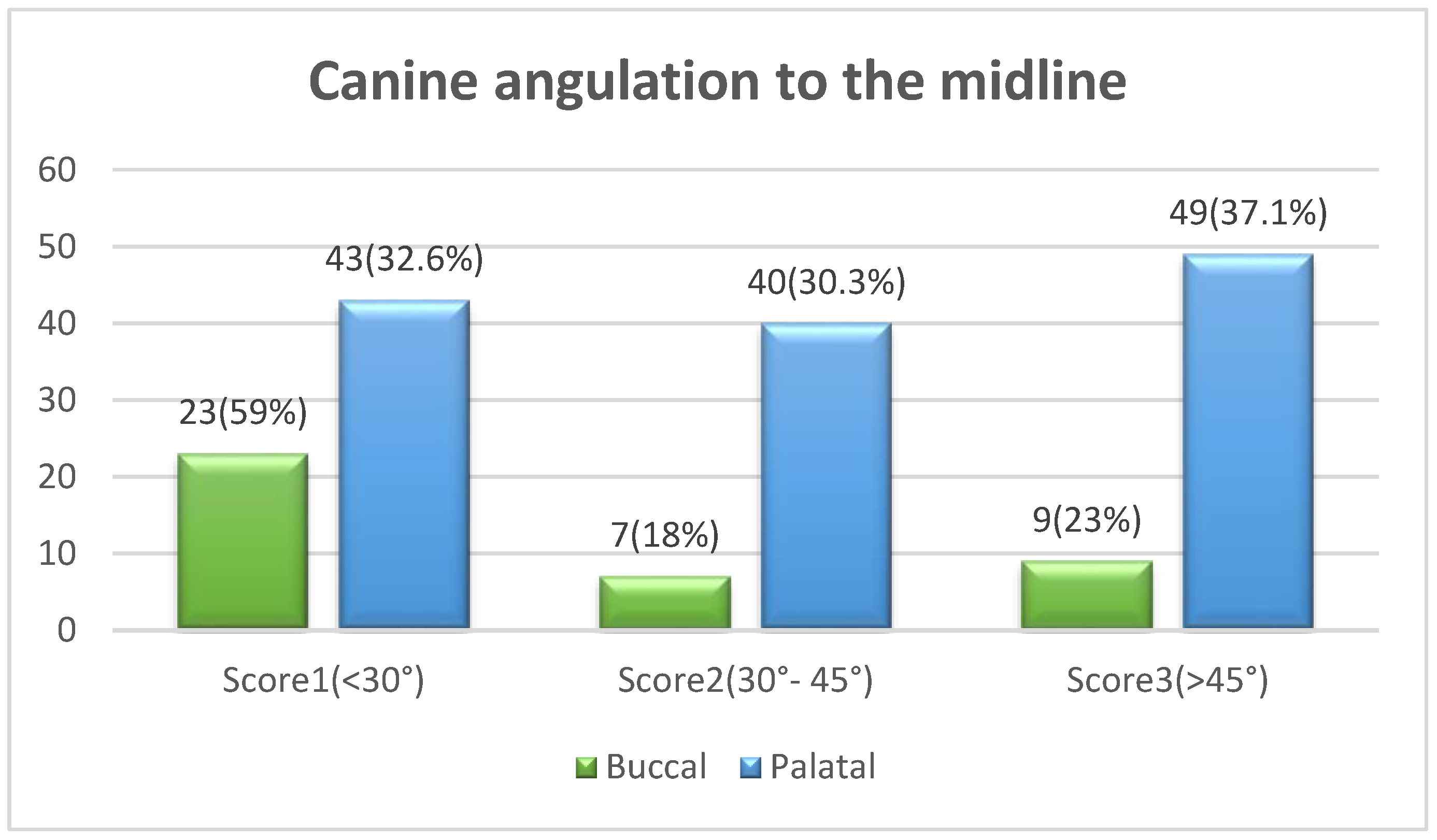
- Angulation between the midsagittal plane and the long axis of the impacted tooth is as follows: score 1—mild (<30°), score 2—moderate (30°–45°), and score 3—severe (˃45°) (Figure 1);
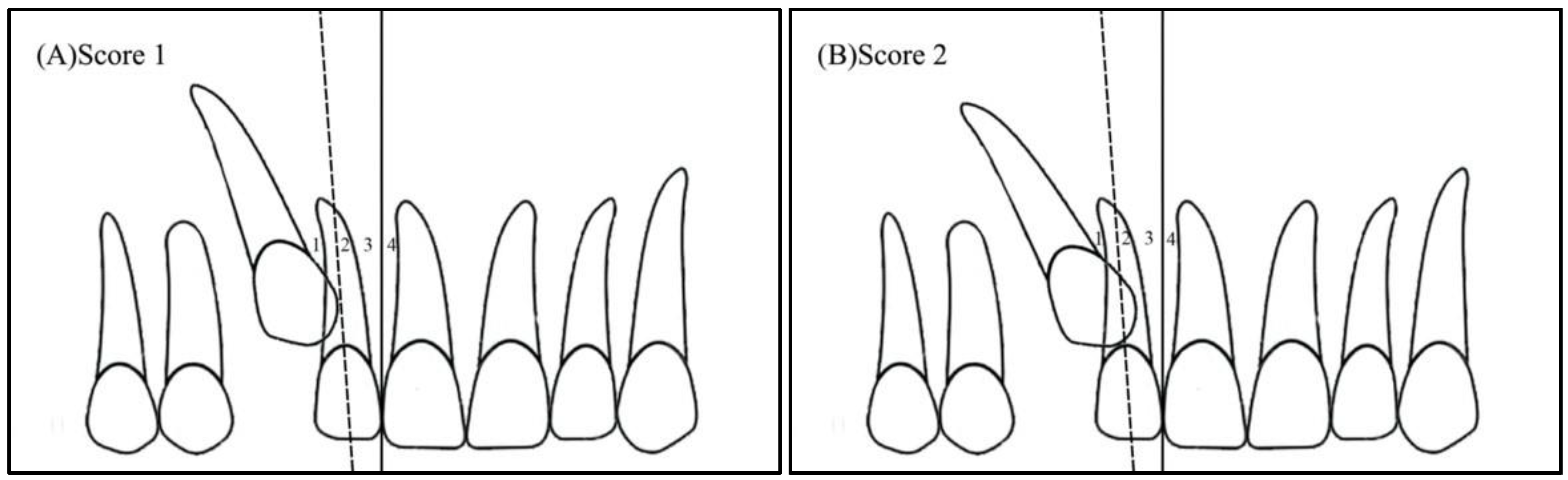
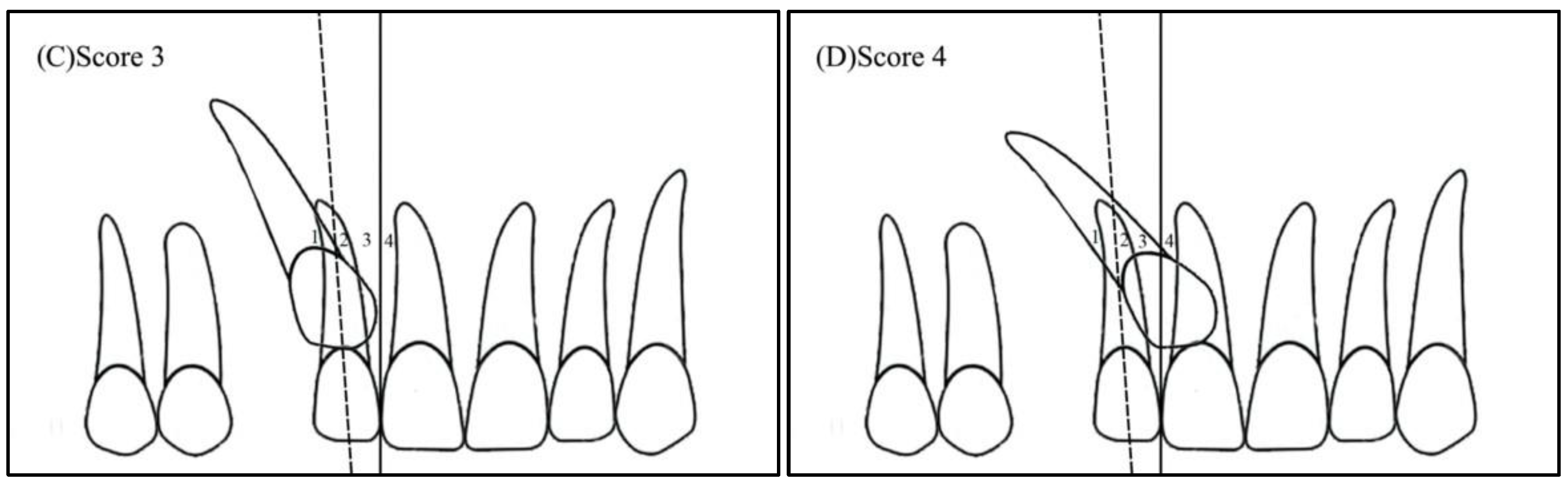
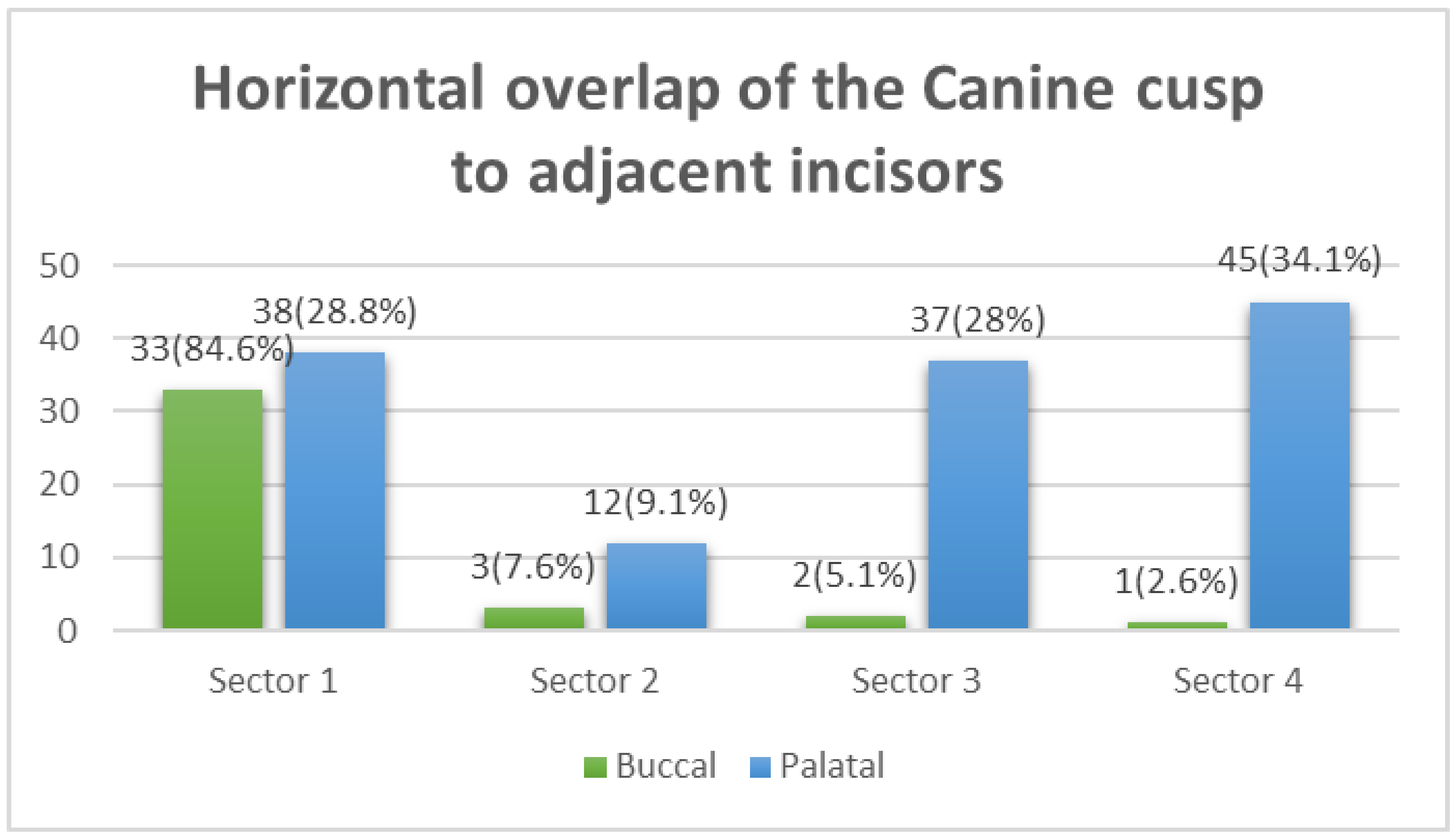
- Horizontal overlap: Sector 1 (canine overlapping less than half the width of the lateral incisor), Sector 2 (canine overlapping half the width of the lateral incisor), Sector 3 (canine completely overlapping the lateral incisor), and Sector 4 (enclosed all areas mesial to Sector 3) (Figure 2);
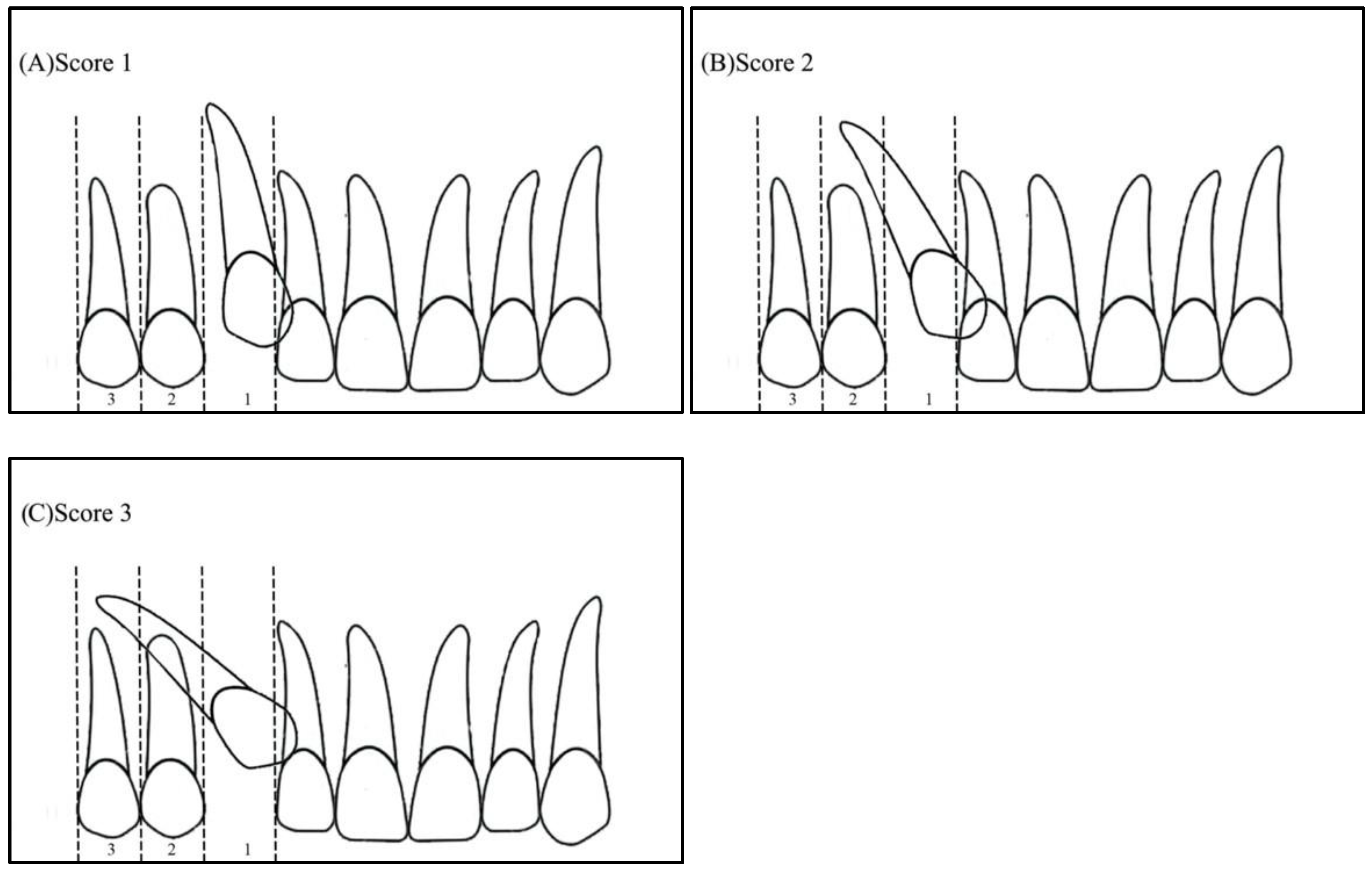
- Apex position: score 1 (in the area of canine apex), score 2 (in the area of the first premolar apex), and score 3 (in the area of the second premolar apex) (Figure 3);
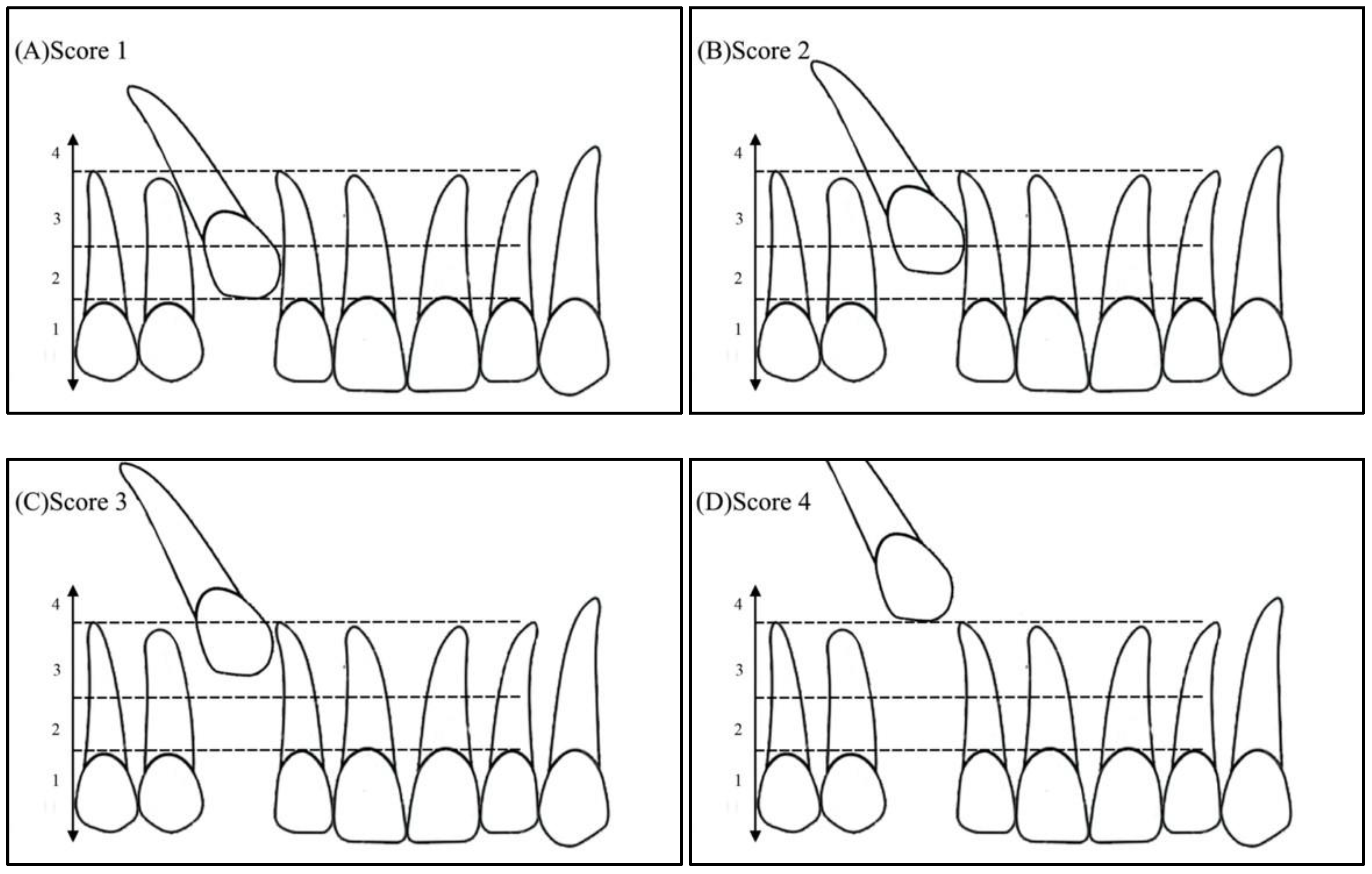
- Vertical overlap: score 1 (canine cusp tip at the level of the cementoenamel junction of the adjacent incisor), score 2 (canine cusp tip at the middle of the root of the adjacent incisor), score 3 (canine cusp tip within the apical third of the root of the adjacent incisor), and score 4 (canine cusp tip above the apical third of the root of the adjacent incisor) (Figure 4).
2.2. Treatment Difficulty Index for Unerupted Maxillary Canine
2.3. Statistical Analysis
- Descriptive statistics (mean, standard deviation, frequencies, and percentages) were used to quantify the quantitative and categorical variables;
- Pearson’s chi-square test, followed by the deviance test, was used to observe the associations between the categorical variables;
- An independent t-test was used to examine gender differences in the treatment difficulty index.
3. Results
3.1. The Severity of the Impacted Canine
3.2. The Total Treatment Difficulty Index
4. Discussion
5. Conclusions
- Maxillary canine impaction was higher in younger females (14–18 y) compared to males of the same age;
- The severity of IMC was not found to be different between males and females, or across age groups;
- Palatal impactions were found to be more severe than buccal impactions due to the worsening horizontal position and larger angulation to the midline;
- The horizontal overlap of the IMC cusp tip (sectors) revealed a significant association with the bucco-palatal position of the impacted canine. Most of the buccally positioned IMC cases were located in Sector 1, while over two thirds of the palatally positioned impactions were located in Sectors 3 and 4;
- Although canine impaction was found to be higher in females, males had higher treatment difficulty index scores and, thus, were characterized by relatively higher expected treatment difficulty.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alamri, A.; Alshahrani, N.; Al-Madani, A.; Shahin, S.; Nazir, M. Prevalence of impacted teeth in Saudi patients attending dental clinics in the Eastern province of Saudi Arabia: A radiographic retrospective study. Sci. World J. 2020, 2020, 8104904. [Google Scholar] [CrossRef] [PubMed]
- Alassiry, A. Radiographic assessment of the prevalence, pattern and position of maxillary canine impaction in Najran (Saudi Arabia) population using orthopantomograms—A cross-sectional, retrospective study. Saudi Dent. J. 2020, 32, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Schour, I. Development and growth of teeth. Oral Surg. Oral Med. Oral Pathol. 1948, 1, 346–354. [Google Scholar] [CrossRef]
- Ericson, S.; Kurol, J. Radiographic assessment of maxillary canine eruption in children with clinical signs of eruption disturbance. Eur. J. Orthod. 1986, 8, 133–140. [Google Scholar] [CrossRef] [PubMed]
- AL-Mayali, A.M.Y.; Nahidh, M.; Alnajar, H.A.; Fahad, A.H. Impaction prevalence of permanent teeth pattern from orthodontic view. Eurasian J. Biosci. 2020, 14, 2823–2828. [Google Scholar]
- Ericson, S.; Kurol, J. Resorption of maxillary lateral incisors caused by ectopic eruption of the canines. A clinical and radiographic analysis of predisposing factors. Am. J. Orthod. Dentofacial Orthop. 1988, 94, 503–513. [Google Scholar] [CrossRef]
- Becker, A.; Zilberman, Y.; Tsur, B. Root length of lateral incisors adjacent to palatally-displaced maxillary cuspids. Angle Orthod. 1984, 54, 218–225. [Google Scholar]
- Schroder, A.G.D.; Guariza-Filho, O.; de Araujo, C.M.; Ruellas, A.C.; Tanaka, O.M.; Porporatti, A.L. To what extent are impacted canines associated with root resorption of the adjacent tooth?: A systematic review with meta-analysis. J. Am. Dent. Assoc. 2018, 149, 765–777.e8. [Google Scholar]
- Litsas, G.; Acar, A. A review of early displaced maxillary canines: Etiology, diagnosis and interceptive treatment. Open Dent. J. 2011, 5, 39–47. [Google Scholar] [CrossRef]
- Chapokas, A.R.; Almas, K.; Schincaglia, G.P. The impacted maxillary canine: A proposed classification for surgical exposure. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 222–228. [Google Scholar]
- Alqerban, A.; Jacobs, R.; Fieuws, S.; Willems, G. Comparison of two cone beam computed tomographic systems versus panoramic imaging for localization of impacted maxillary canines and detection of root resorption. Eur. J. Orthod. 2011, 33, 93–102. [Google Scholar] [PubMed]
- Signorelli, L.; Patcas, R.; Peltomäki, T.; Schätzle, M. Radiation dose of cone-beam computed tomography compared to conventional radiographs in orthodontics. J. Orofac. Orthop. 2016, 77, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.S.; Scott, P.; Heidari, N.; Dibiase, A.T. Influence of radiographic position of ectopic canines on the duration of orthodontic treatment. Angle Orthod. 2009, 79, 442–446. [Google Scholar] [CrossRef]
- Ericson, S.; Kurol, J. Radiographic examination of ectopically erupting maxillary canines. Am. J. Orthod. Dentofac. Orthop. 1987, 91, 483–492. [Google Scholar] [CrossRef]
- Lindauer, S.J.; Rubenstein, L.K.; Hang, W.M.; Andersen, W.C.; Isaacson, R.J. Canine impaction identified early with panoramic radiographs. J. Am. Dent. Assoc. 1992, 123, 91–97. [Google Scholar] [CrossRef]
- Power, S.M.; Short, M.B. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favourable eruption. Br. J. Orthod. 1993, 20, 215–223. [Google Scholar] [CrossRef]
- Shehare, N.; Tarvade, S.; Kaurani, H. Canine impaction: Diagnosis and management. Int. J. Orthod. Rehabil. 2021, 12, 126–130. [Google Scholar] [CrossRef]
- Al-Abdallah, M.; AlHadidi, A.; Hammad, M.; Dar-Odeh, N. What factors affect the severity of permanent tooth impaction? BMC Oral Health 2018, 18, 184. [Google Scholar] [CrossRef]
- Pitt, S.; Hamdan, A.; Rock, P. A treatment difficulty index for unerupted maxillary canines. Eur. J. Orthod. 2006, 28, 141–144. [Google Scholar] [CrossRef]
- Alhammadi, M.S.; Asiri, H.A.; Almashraqi, A.A. Incidence, severity and orthodontic treatment difficulty index of impacted canines in Saudi population. J. Clin. Exp. Dent. 2018, 10, e327–e334. [Google Scholar] [CrossRef]
- Hou, R.; Kong, L.; Ao, J.; Liu, G.; Zhou, H.; Qin, R.; Hu, K. Investigation of impacted permanent teeth except the third molar in Chinese patients through an X-ray study. J. Oral. Maxillofac. Surg. 2010, 68, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Zahrani, A.A. Impacted cuspids in a Saudi population: Prevalence, etiology and complications. Egypt. Dent. J. 1993, 39, 367–374. [Google Scholar] [PubMed]
- El Beshlawy, D.M. Radiographic assessment of impacted maxillary canine position using CBCT: A comparative study of 2 methods. Egypt. Dent. J. 2019, 65, 3393–3402. [Google Scholar] [CrossRef]
- Rodríguez-Cárdenas, Y.A.; Arriola-Guillén, L.E.; Aliaga-Del Castillo, A.; Ruíz-Mora, G.A.; Janson, G.; Cevidanes, L.; Ruellas, A.C.; Yatabe, M.; Silveira, H.L.D. Three-dimensional changes in root angulation of buccal versus palatal maxillary impacted canines after orthodontic traction: A retrospective before and after study. Int. Orthod. 2021, 19, 216–227. [Google Scholar] [CrossRef]
- Alfaleh, W.; Al Thobiani, S. Evaluation of impacted maxillary canine position using panoramic radiography and cone beam computed tomography. Saudi Dent. J. 2021, 33, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Son, W.S.; Yamaguchi, T.; Maki, K.; Kim, S.S.; Park, S.B.; Kim, Y.I. Assessment of the root apex position of impacted maxillary canines on panoramic films. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 489–493. [Google Scholar] [CrossRef]
- Jain, S.; Debbarma, S. Patterns and prevalence of canine anomalies in orthodontic patients. Med. Pharm. Rep. 2019, 92, 72–78. [Google Scholar] [CrossRef]
- Diop Ba, K.; Diouf, J.S.; Badiane, A.; Ngom, P.I.; Diagne, F. Orthopantomographic analysis of the intraosseus position of the maxillary canines. Int. Orthod. 2019, 17, 324–332. [Google Scholar] [CrossRef]
- Gunardi, O.J.; Danudiningrat, C.P.; Rizqiawan, A.; Mulyawan, I.; Amir, M.S.; Kamadjaja, D.B.; Sumarta, N.P.M.; Anugraha, G.; Fessi, R.A.; Barus, L.; et al. Decision-making criteria of odontectomy or surgical exposure in impacted maxillary canine based on treatment difficulty index modification. Eur. J. Dent. 2022. [Google Scholar] [CrossRef]
- Miresmaeili, A.; Basafa, M.; Mahvelati Shamsabadi, R.; Farhadian, N.; Moghymbeigi, A.; Mollabashi, V. Treatment decision analysis for palatally-displaced canines based on orthodontists’ opinion and CBCT. Int. Orthod. 2017, 15, 625–639. [Google Scholar] [CrossRef]
- Bolooki, H.; Hameed, O.; Sherriff, M.; Minhas, G. Positional factors affecting the surgical management of impacted permanent mandibular canines. J. Orthod. 2022, 14653125221084318. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Score | Weight |
|---|---|---|
| Age | ||
| Less than 12 years | 1 | 1.5 |
| 12–15 years | 2 | |
| 15–18 years | 3 | |
| Over 18 years | 4 | |
| Angulation to midline | ||
| Less than 30 degrees | 1 | 1 |
| 30–45 degrees | 2 | |
| Over 45 degrees | 3 | |
| Vertical position | ||
| Canine cusp tip at the level of the amelocemental junction of the adjacent incisor | 1 | 1.5 |
| Canine cusp tip at the middle of the root of the adjacent incisor | 2 | |
| Canine cusp tip within the apical third of the adjacent incisor | 3 | |
| Canine cusp tip above the apical third of the adjacent incisor | 4 | |
| Bucco-palatal position | ||
| Buccal | 1 | 1 |
| Palatal | 1 | |
| Horizontal position | ||
| Canine overlapping less than half the width of the lateral incisor | 1 | 2 |
| Canine overlapping over half the width of the lateral incisor | 2 | |
| Canine completely overlapping the lateral incisor | 3 | |
| Canine overlapping up to half the width of the central incisor | 4 | |
| Alignment of upper incisors | ||
| Incisors spaced | 1 | 0.5 |
| Incisors well-aligned | 2 | |
| Incisors crowded | 3 | |
| Space between the upper lateral incisor and upper first premolar | ||
| Over 7 mm | 1 | 1 |
| 4–7 mm | 2 | |
| 2–4 mm | 3 | |
| 0–2 mm | 4 | |
| Midline | ||
| Midline coincident with lower | 1 | 1 |
| Midline displaced | 2 | |
| Rotation | ||
| Rotation absent | 1 | 1 |
| Rotation present | 2 | |
| Variable | Total | Male | Female | |||||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | p-Value | ||
| Age groups | 14–18 | 103 | 60.2 | 37 | 51.4 | 66 | 66.7 | 0.044 * |
| 19–30 | 68 | 39.8 | 35 | 48.6 | 33 | 33.3 | ||
| Impacted upper canine side | Right | 89 | 52 | 41 | 56.9 | 48 | 48.5 | 0.274 |
| left | 82 | 48 | 31 | 43.1 | 51 | 51.5 | ||
| Bucco-lingual position | Buccal | 39 | 22.8 | 17 | 23.6 | 22 | 22.2 | 0.486 |
| Palatal | 132 | 77.2 | 55 | 76.4 | 77 | 77.8 | ||
| Parameters | Score | Gender | Age Group (Years) | Bucco-Lingual Position | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Male | Female | 14–18 | 19–30 | Buccal | Palatal | p-Value | ||||
| No (%) | No (%) | No (%) | p-Value | No (%) | No (%) | p-Value | No (%) | No (%) | p-Value | ||
| Tooth angulation to the midline | <30° | 66 (38.6) | 24 (33.3) | 42 (42.4) | 0.185 | 43 (41.7) | 23 (33.8) | 0.402 | 23 (59) | 43 (32.6) | 0.012 * |
| 30–45° | 47 (27.5) | 18 (25.0) | 29 (29.3) | 29 (28.2) | 18 (26.5) | 7 (18) | 40 (30.3) | ||||
| >45° | 58 (33.9) | 30 (41.7) | 28 (28.3) | 31 (30.1) | 27 (39.7) | 9 (23) | 49 (37.1) | ||||
| Horizontal overlap of the canine cusp to adjacent incisors | <1/2 of the lateral incisor | 71 (41.5) | 26 (36.1) | 45 (45.5) | 0.418 | 42 (40.8) | 29 (42.6) | 0.705 | 33 (84.6) | 38 (28.8) | <0.001 ** |
| Up to 1/2 of the lateral incisor | 15 (8.8) | 6 (8.3) | 9 (9.1) | 11 (10.7) | 4 (5.9) | 3 (7.7) | 12 (6.3) | ||||
| >1/2 of the lateral incisor | 39 (22.8) | 16 (22.2) | 23 (23.2) | 24 (23.3) | 15 (21.1) | 2 (5.1) | 37 (28) | ||||
| Up to 1/2 of the central incisor | 46 (26.9) | 24 (33.3) | 22 (22.2) | 26 (25.2) | 20 (29.4) | 1 (2.6) | 45 (34) | ||||
| Apex position | Canine position | 8 (4.7) | 3 (4.2) | 5 (5.1) | 0.643 | 5 (4.8) | 3 (4.4) | 0.907 | 0 (0) | 8 (6.1) | 0.098 |
| First premolar | 101 (59.1) | 40 (55.6) | 61 (61.6) | 62 (60.2) | 39 (57.4) | 28 (71.8) | 73 (55.3) | ||||
| Second premolar | 62 (36.3) | 29 (40.3) | 33 (33.3) | 36 (35.0) | 26 (38.2) | 11 (28.2) | 51 (38.6) | ||||
| Vertical position relative to the adjacent incisor | At the level of CEJ | 36 (21.1) | 14 (19.4) | 22 (22.2) | 0.495 | 22 (21.4) | 14 (20.6) | 0.170 | 9 (23.1) | 27 (20.5) | 0.752 |
| In the middle of the root | 112 (65.5) | 50 (69.4) | 62 (62.6) | 70 (68.0) | 42 (61.8) | 23 (58.9) | 89 (67.4) | ||||
| Within the apical third | 20 (11.7) | 6 (8.3) | 14 (14.1) | 11 (10.7) | 9 (13.2) | 6 (15.4) | 14 (10.6) | ||||
| Above the apex | 3 (1.8) | 2 (2.8) | 1 (1.0) | 0 | 3 (4.4) | 1 (2.6) | 2 (1.5) | ||||
| Components of the Difficulty Index (Weighted Scores) | Total | Male | Female | ||||
|---|---|---|---|---|---|---|---|
| Mean (±SD) | Range | Mean (±SD) | Range | Mean (±SD) | Range | p-Value | |
| Age | 4.68 (1.2) | 1.5–6 | 4.81 (1.3) | 1.5–6 | 4.59 (1.2) | 3–6 | 0.246 |
| Angulation to the midline | 1.95 (0.85) | 1–3 | 2.08 (0.9) | 1–3 | 1.86 (0.8) | 1–3 | 0.089 |
| Vertical position | 2.91 (0.94) | 1.5–6 | 2.92 (0.9) | 1.5–6 | 2.91 (1) | 1.5–6 | 0.959 |
| Bucco-lingual position | 1 | 1 | 1 | 1–1 | 1 | 1–1 | 0 |
| Horizontal position | 4.7 (0.85) | 2–8 | 5.06 (2.5) | 2–8 | 4.44 (2.5) | 2–8 | 0.12 |
| Alignment of the upper incisors | 0.88 (0.28) | 0.5–1.5 | 0.9 (0.3) | 0.5–1.5 | 0.86 (0.3) | 0.5–1.5 | 0.368 |
| Canine space | 2.73 (0.85) | 1–4 | 2.72 (0.9) | 1–4 | 2.73 (0.8) | 1–4 | 0.97 |
| Midline | 1.77 (0.42) | 1–2 | 1.79 (0.5) | 1–2 | 1.76 (0.4) | 1–2 | 0.602 |
| Rotation | 1.51 (0.50) | 1–2 | 1.57 (0.5) | 1–2 | 1.47 (0.5) | 1–2 | 0.178 |
| Total difficulty index | 22.13 (4) | 14.5–31.5 | 22.85 (3.8) | 15.5-31 | 21.62 (4) | 14.5–31.5 | 0.046 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baidas, L.F.; Alshihah, N.; Alabdulaly, R.; Mutaieb, S. Severity and Treatment Difficulty of Impacted Maxillary Canine among Orthodontic Patients in Riyadh, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 10680. https://doi.org/10.3390/ijerph191710680
Baidas LF, Alshihah N, Alabdulaly R, Mutaieb S. Severity and Treatment Difficulty of Impacted Maxillary Canine among Orthodontic Patients in Riyadh, Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(17):10680. https://doi.org/10.3390/ijerph191710680
Chicago/Turabian StyleBaidas, Laila Fawzi, Nada Alshihah, Rwan Alabdulaly, and Sara Mutaieb. 2022. "Severity and Treatment Difficulty of Impacted Maxillary Canine among Orthodontic Patients in Riyadh, Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 17: 10680. https://doi.org/10.3390/ijerph191710680
APA StyleBaidas, L. F., Alshihah, N., Alabdulaly, R., & Mutaieb, S. (2022). Severity and Treatment Difficulty of Impacted Maxillary Canine among Orthodontic Patients in Riyadh, Saudi Arabia. International Journal of Environmental Research and Public Health, 19(17), 10680. https://doi.org/10.3390/ijerph191710680