
Impoverishment Effect of Hydatid Disease and Precision Medical Assistance Pattern of Government: Evidence from Yushu in China


Abstract
:1. Introduction
2. Materials and Methods
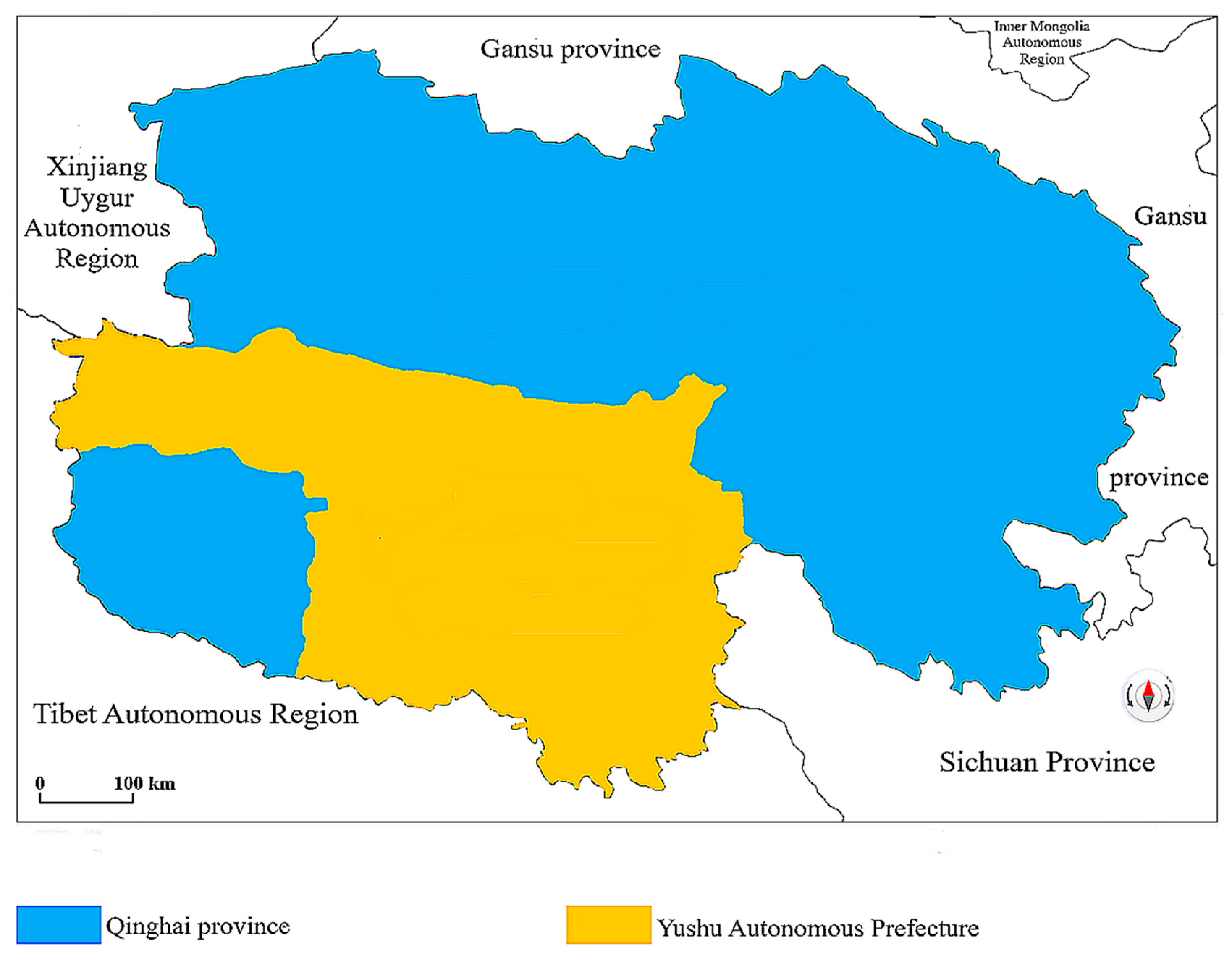
2.1. Materials
2.2. Research Methods
3. Results
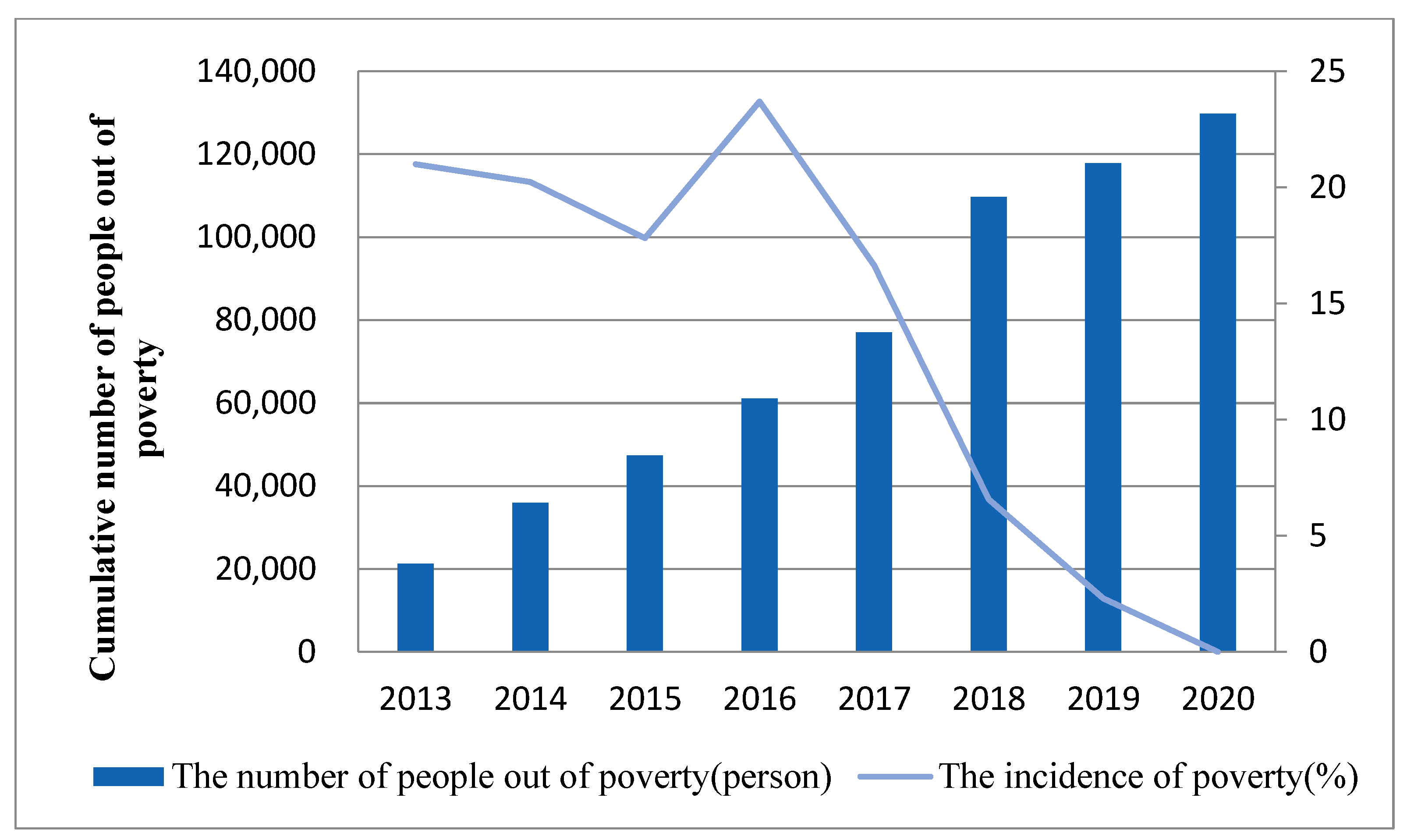
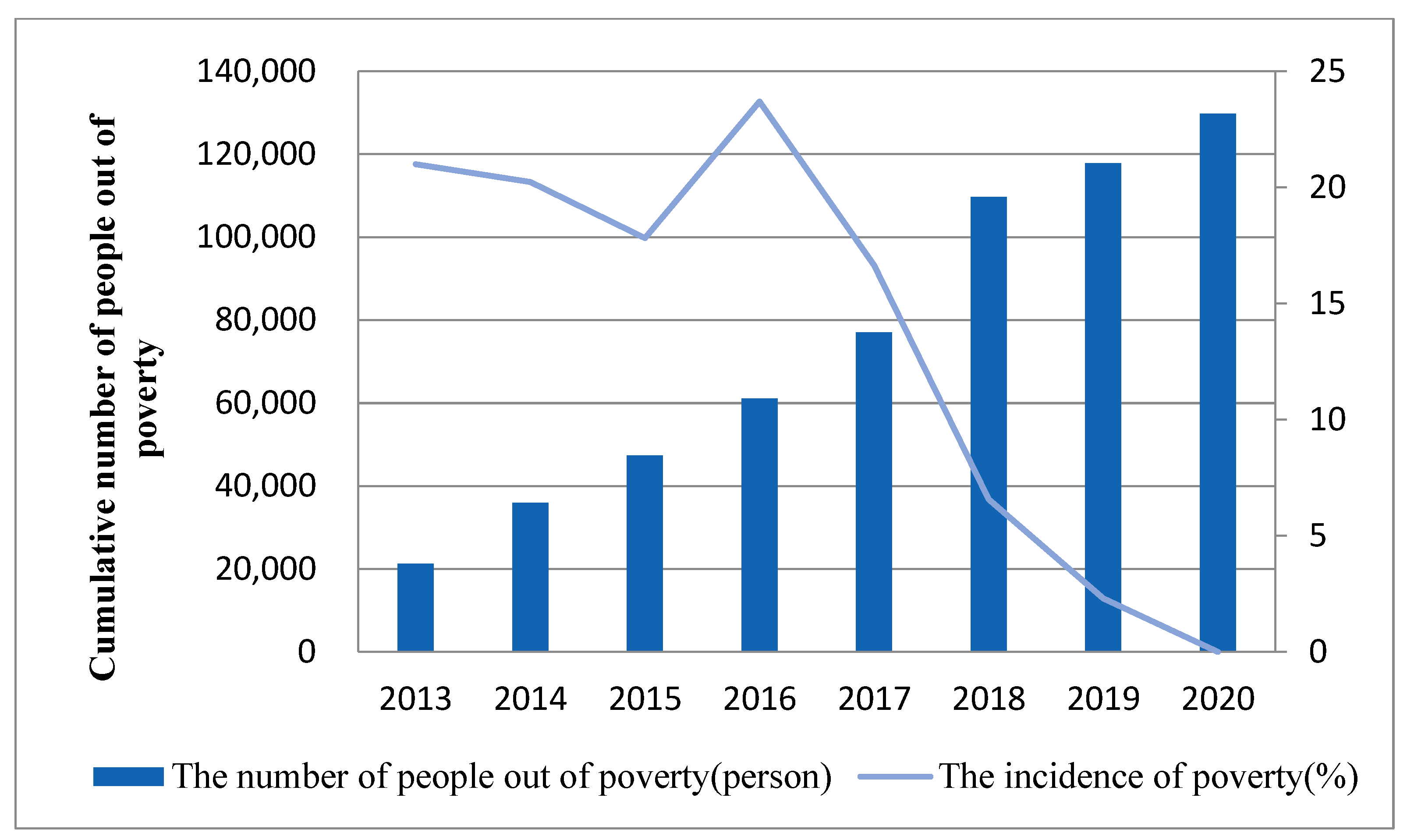
3.1. Relationship between the Hydatid Disease and Poverty
3.2. The Detection Rates of Hydatid Disease
3.3. Effect of Health Services
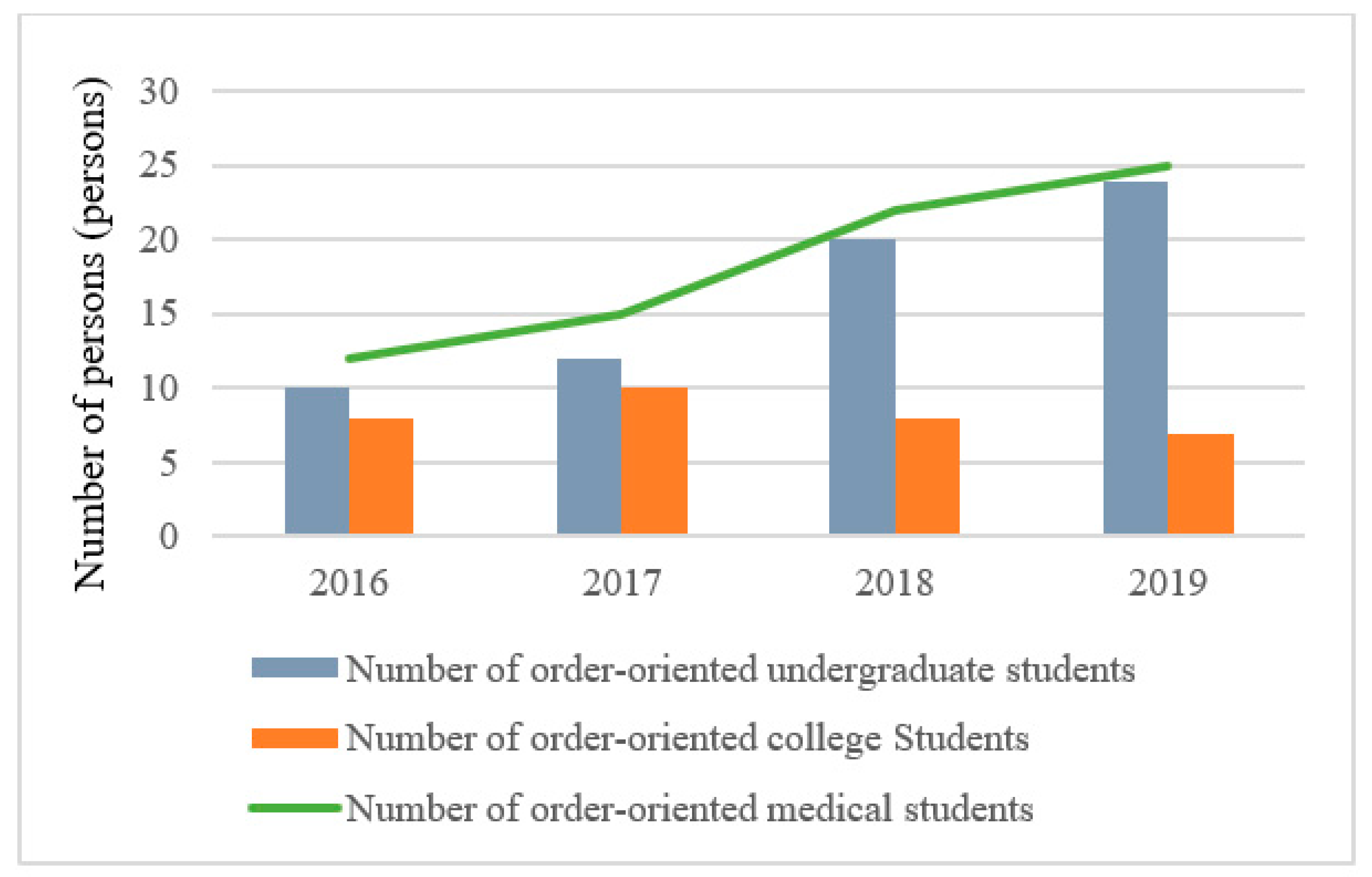
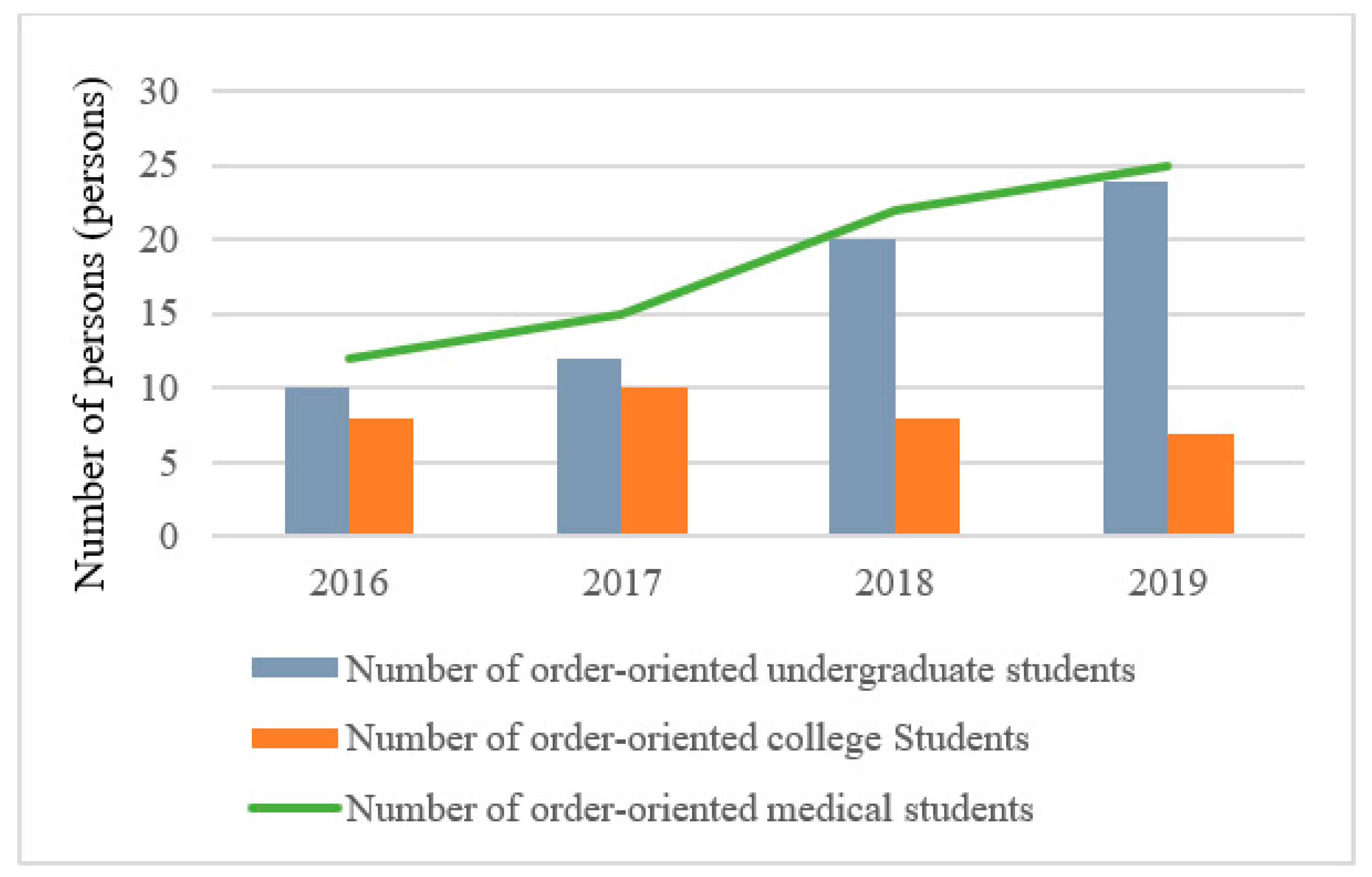
3.4. Scale of Medical Backbone Team
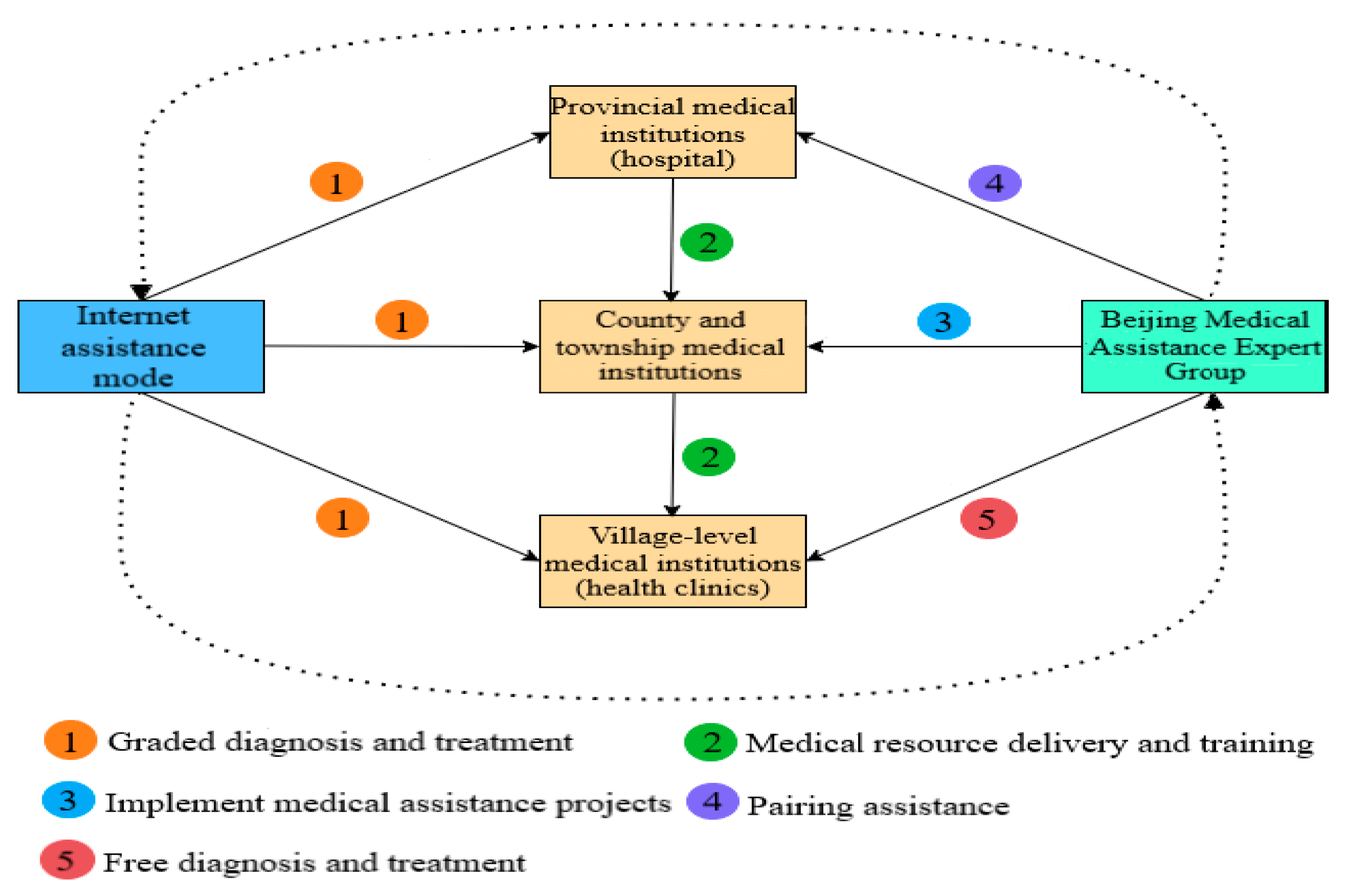
3.5. Precision Medical Assistance Pattern of Government
4. Discussion
4.1. Effectiveness of Medical Assistance in Poverty Alleviation
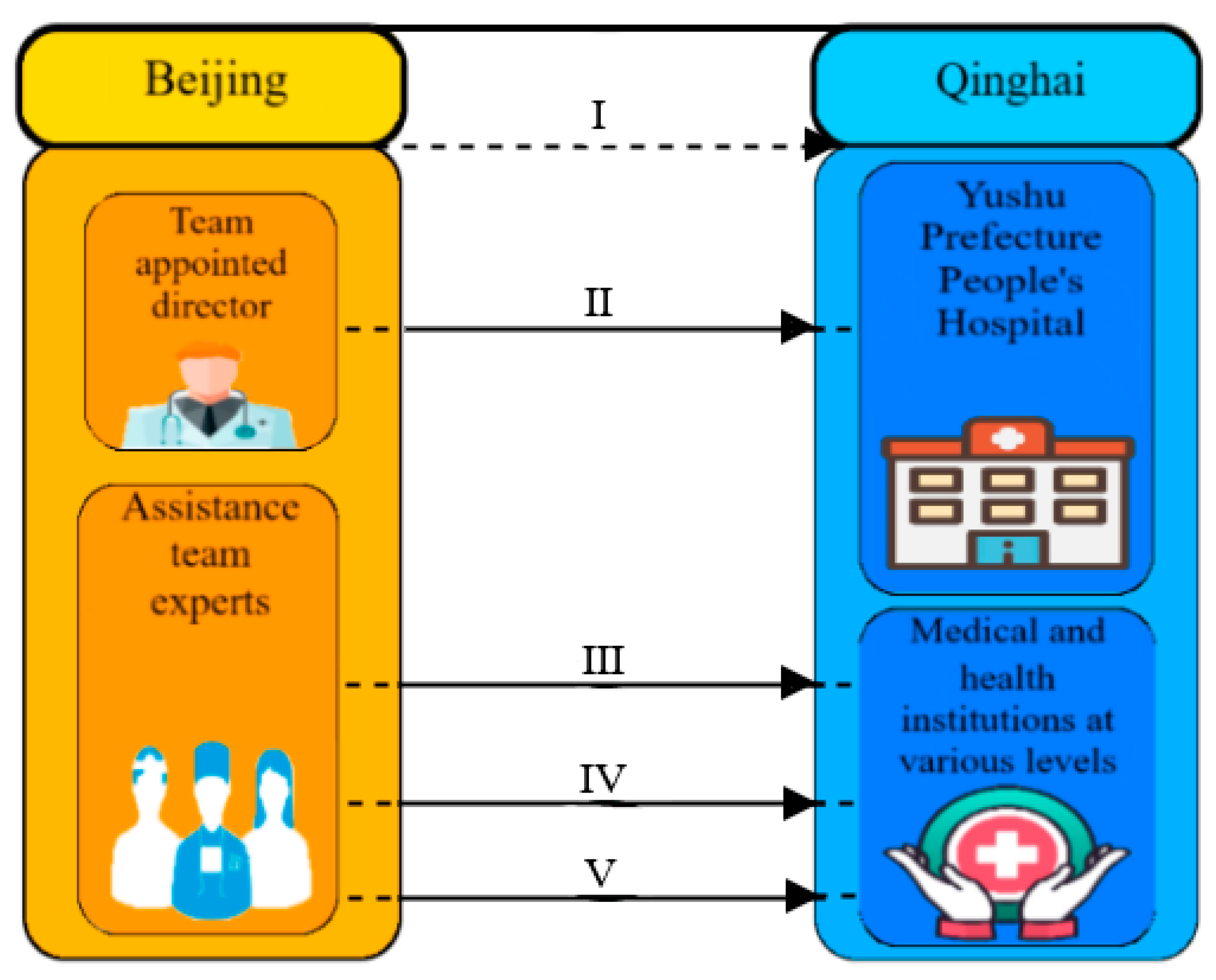
4.2. A Three-Level Diagnosis and Treatment Framework
4.2.1. Longitudinally Medical Assistance with Dean as the Core, Team as the Focus and Reform as the Goal
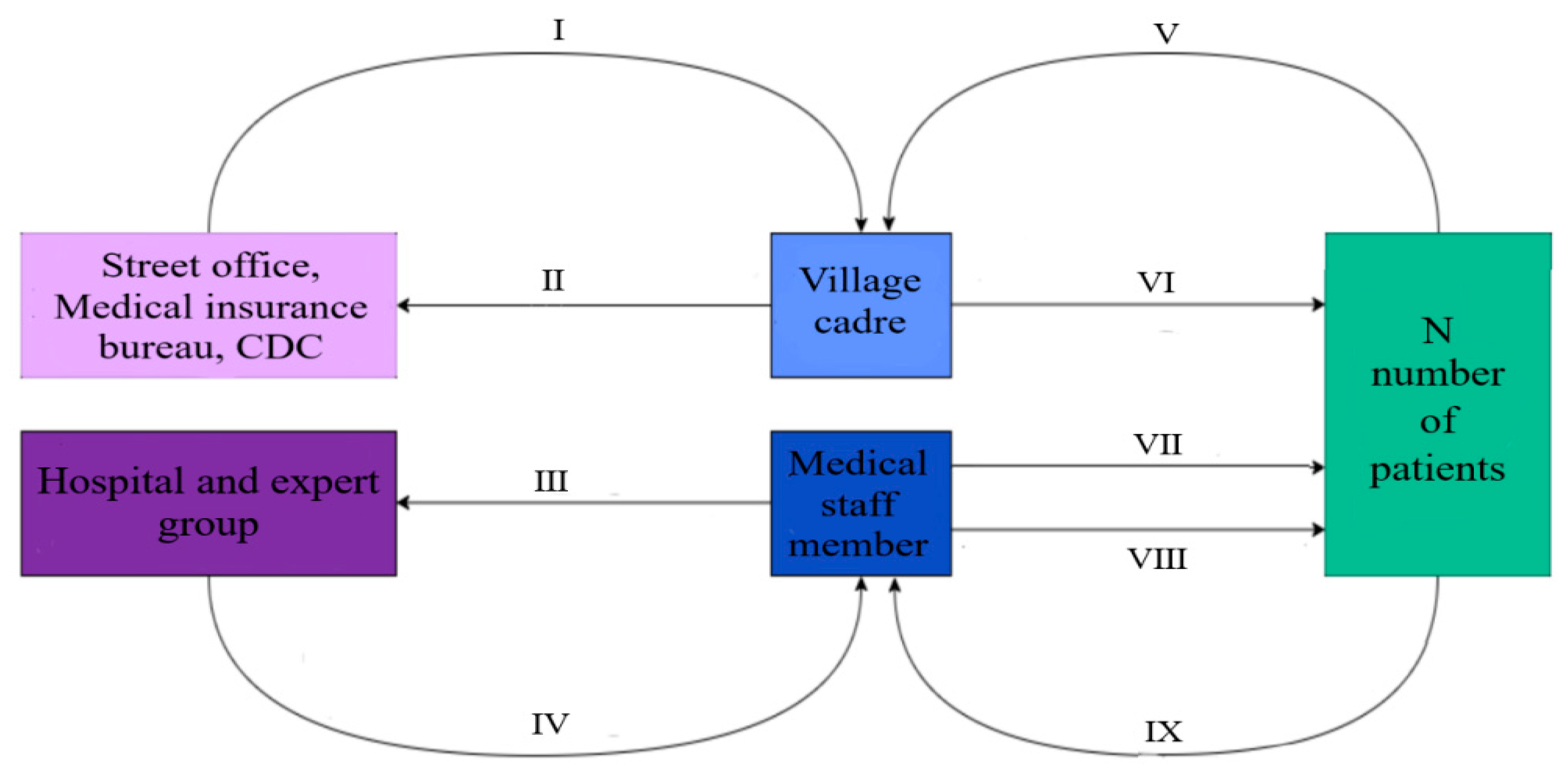
4.2.2. Horizontal Medical Assistance of “1 Village Cadre + 1 Medical Staff + N Patients”
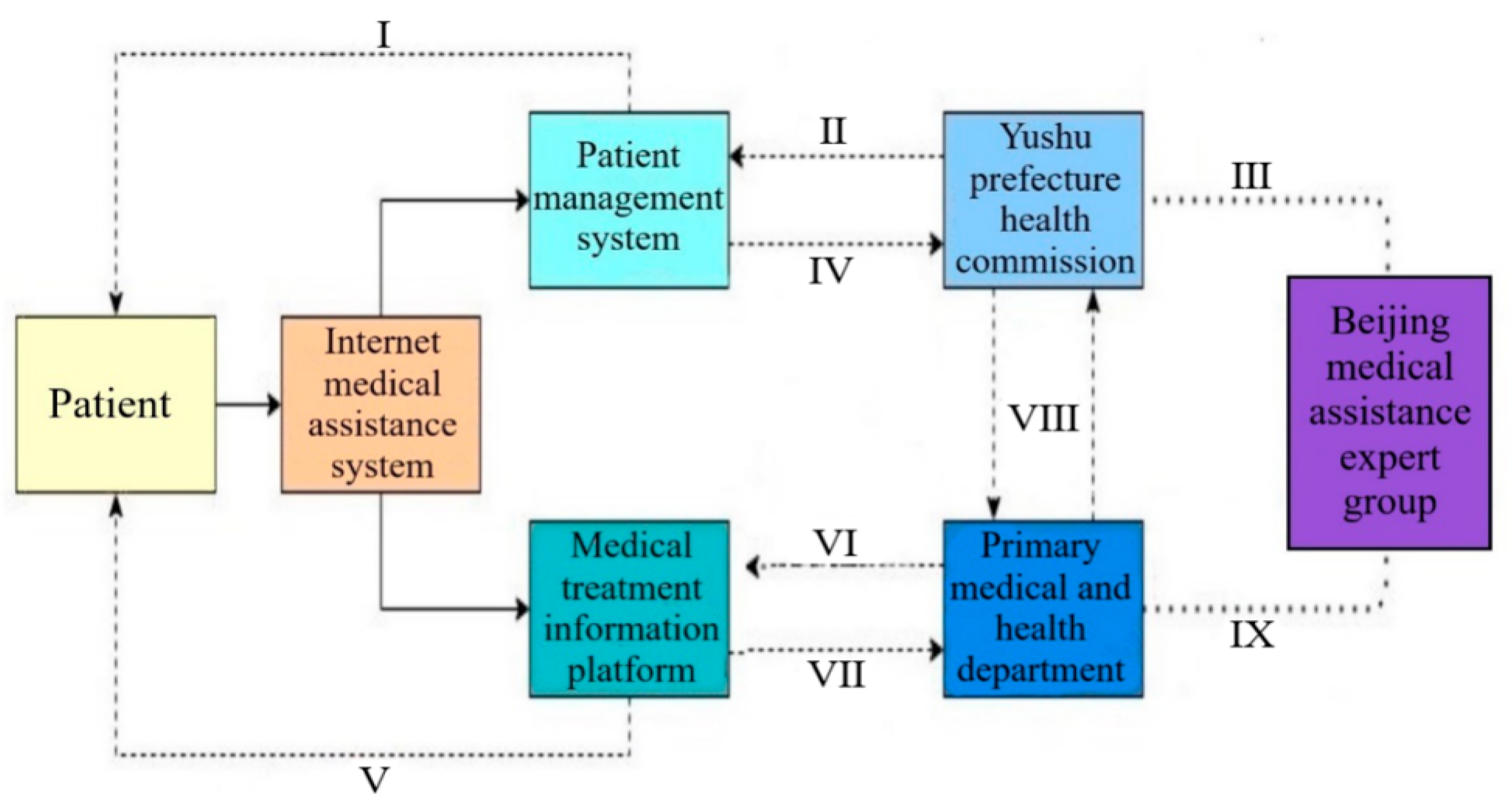
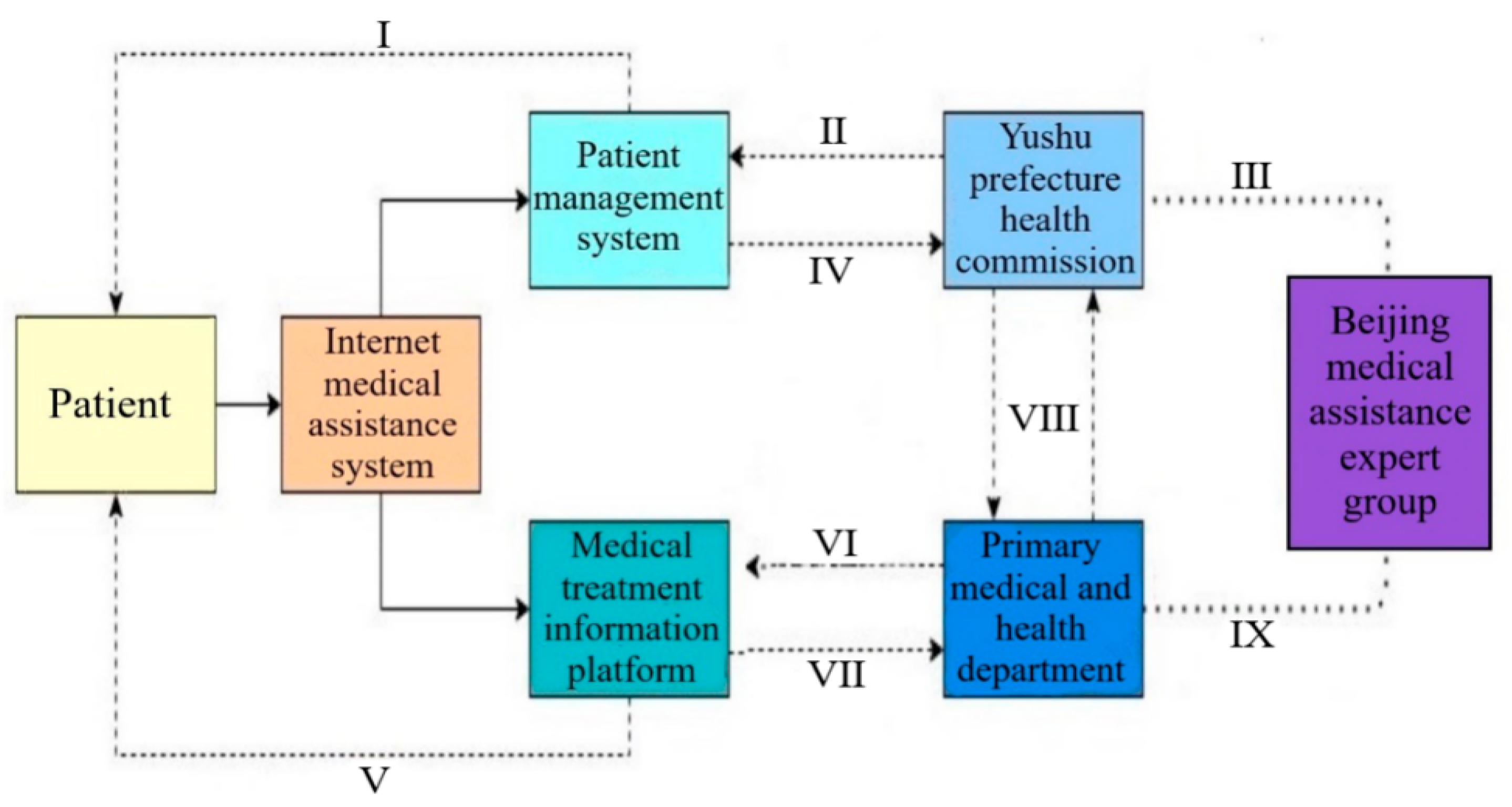
4.3. Internet Online Medical Assistance
5. Conclusions
6. Suggestions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhattacharyya, S. The historical origins of poverty in developing countries. In Oxford Handbook of the Social Science of Poverty; Oxford University Press: Oxford, UK, 2016; pp. 270–292. [Google Scholar]
- Kagan, L.J.; Aiello, A.E.; Larson, E. The role of the home environment in the transmission of infectious diseases. J. Community Health 2002, 27, 247–267. [Google Scholar] [CrossRef] [PubMed]
- Frolkis, A.; Dieleman, L.A.; Barkema, H.W.; Panaccione, R.; Ghosh, S.; Fedorak, R.N.; Madsen, K.; Kaplan, G.G.; Alberta IBD Consortium. Environment and the inflammatory bowel diseases. Can. J. Gastroenterol. 2013, 27, 102859. [Google Scholar] [CrossRef] [PubMed]
- Kristiansson, M.; Sörman, K.; Tekwe, C.; Calderón-Garcidueñas, L. Urban air pollution, poverty, violence and health–Neurological and immunological aspects as mediating factors. Environ. Res. 2015, 140, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Li, R.H. Research on Prevention Mechanism of “Poverty-Disease” Vicious Cycle. Chin. Health Econ. 2020, 39, 27–29. [Google Scholar]
- Zheng, Y.Y.; Meng, X.Y.; Li, Q.; Zhao, Z.J.; Gan, P.C.; Zou, X.; Shen, H.T.; Pu, G.L.; Zhang, X.Y. Effect Evaluation of the 12th Five-Year Plan for Endemic Disease Prevention and Control in Huzhu County, Qinghai Province. Chin. J. Epidemiol. 2017, 36, 145. [Google Scholar]
- Sichuan Provincial Department of Finance and Sichuan Provincial Committee of Agriculture and Industry Joint Investigation Team. New Exploration of Comprehensive Financial Poverty Alleviation in Poverty-stricken Areas: Investigation on the Pilot Work of Poverty Alleviation and Comprehensive Prevention and Control of Kashin-Beck Disease in Aba Prefecture, Sichuan Province. Newsl. Work. Rural. Areas 2012, 14, 43–45. [Google Scholar]
- Wang, Z.X.; Ji, G.X. Analysis of epidemic situation and related factors of brucellosis in Qingzhou City from 2011 to 2017. China Health Care Nutr. 2020, 30, 286. [Google Scholar]
- Wang, Y.; Wilkinson, M.; Ng, E.; Cheng, K. Primary care reform in china. Br. J. Gen. Pract. 2012, 62, 546–547. [Google Scholar] [CrossRef]
- Lee, E.W.; Park, J.H. Egalitarian health policy preference and its related factors in korea: National representative sample survey. J. Korean Med. Sci. 2015, 30, 676–681. [Google Scholar] [CrossRef]
- Waters, K.P.; Zuber, A.; Willy, R.M.; Kiriinya, R.N.; Waudo, A.N.; Oluoch, T.; Kimani, F.M.; Riley, P.L. Kenya’s health workforce information system: A model of impact on strategic human resources policy, planning and management. Int. J. Med. Inform. 2013, 82, 895–902. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, G.; Li, L. The Spatial Impact of Atmospheric Environmental Policy on Public Health Based on the Mediation Effect of Air Pollution in China. Environ. Sci. Pollut. Res. 2022, 21501, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Q.; Wang, Z.T.; Ma, P.C. Situation analysis and thinking about poverty caused by illnesses in rural areas-Based on research data of 1214 families whose poverty is caused by illnesses in 9 Provinces in West China. Economist 2016, 10, 71–81. [Google Scholar]
- Wang, H.; Ma, S.M.; Cao, D.P.; Zhao, H.L.; Wu, H.Y. Research progress of echinococcosis in Qinghai. Chin. High Alt. Med. Biol. 1999, 6, 46–50. [Google Scholar]
- Lin, Y.G.; Lu, M.K.; Hong, L.X. A review of the current status of Echinococcus and echinococcosis, with notes on some informative achievements in China. Chin. J. Zoonoses 2012, 28, 616–627. [Google Scholar]
- Liu, Y.; Wang, H.J. Progress in clinical diagnosis and treatment of hepatic echinococcosis in Qinghai. World Latest Med. Inf. 2019, 19, 114–115. [Google Scholar]
- Fisher, J.A.; Patenaude, G.; Giri, K.; Lewis, K.; Meir, P.; Pinho, P.; Rounsevell, M.D.; Williams, M. Understanding the relationships between ecosystem services and poverty alleviation: A conceptual framework. Ecosyst. Serv. 2014, 7, 34–45. [Google Scholar] [CrossRef]
- Zhong, B.; Wang, Q. Comprehensive prevention and control of echinococcosis to help Shiqu run a well-off society. Mod.Prev. Med. 2020, 47, 4417–4421. [Google Scholar]
- Jun, H.E. Qinghai echinococcosis prevention and control special investment of 200 million yuan. China Health 2017, 7, 105–106. [Google Scholar]
- Tian, X.; Yu, Y. Main practice and effect analysis of counterpart support mode of medical talents’ group aid to Tibet. Tibet. Stud. 2017, 4, 97–102. [Google Scholar]
- Zhu, Z.F.; Chen, H. Summary and reflection on the 5-year work of “group-based” medical assistance to Tibet Autonomous Region People’s Hospital. Chin. J. Clin. 2020, 14, 161–162. [Google Scholar]
- Shan, M.X. Necessity of establishing residents’ health records. J. Clin. Med. 2016, 3, 10058. [Google Scholar]
- Zhang, Z.; Zhang, G.; Su, B. The Spatial Impacts of Air Pollution and Socio-Economic Status on Public Health: Empirical Evidence from China. Socio-Econ. Plan. Sci. 2022, 83, 101167. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Town Name | Respondents Nummer | Case | Detection Rate (%) | |||
|---|---|---|---|---|---|---|
| Year | 2017 | 2020 | 2017 | 2020 | 2017 | 2020 |
| Chengwen Town | 623 | 615 | 41 | 6 | 6.58 | 0.98 |
| Xiewu Town | 456 | 458 | 23 | 3 | 5.04 | 0.66 |
| Zhenqin Town | 562 | 571 | 32 | 4 | 5.69 | 0.70 |
| Qingshuihe Town | 570 | 562 | 51 | 6 | 8.95 | 1.07 |
| Zhaduo Town | 459 | 452 | 34 | 2 | 7.41 | 0.44 |
| Gaduo Town | 432 | 429 | 23 | 3 | 5.32 | 0.70 |
| Labu Town | 325 | 351 | 22 | 3 | 6.77 | 0.85 |
| Sum | 3427 | 3438 | 226 | 27 | 6.59 | 0.79 |
| Variable | Mean | Median | Minimum | Maximum |
|---|---|---|---|---|
| Respondents number in 2017 | 489.57 | 456 | 325 | 623 |
| Respondents number in 2020 | 491.14 | 458 | 351 | 615 |
| Case in 2017 | 32.29 | 32 | 22 | 51 |
| Case in 2020 | 3.86 | 3 | 2 | 6 |
| Detection rate in 2017 (%) | 6.54 | 6.59 | 5.04 | 8.95 |
| Detection rate in 2020 (%) | 0.77 | 0.70 | 0.44 | 1.07 |
| 2017 | 2020 | |
|---|---|---|
| Mean | 6.54375 | 0.77375 |
| Variance | 1.58325536 | 0.03879821 |
| Observations | 8 | 8 |
| Hypothesized Mean Difference | 0 | |
| df | 7 | |
| t Stat | 12.814103 | |
| P(T ≤ t) one-tail | 2.0441 × 10−6 | |
| t Critical one-tail | 1.89457861 | |
| P(T ≤ t) two-tail | 4.0882 × 10−6 | |
| t Critical two-tail | 2.36462425 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, Y. Impoverishment Effect of Hydatid Disease and Precision Medical Assistance Pattern of Government: Evidence from Yushu in China. Int. J. Environ. Res. Public Health 2022, 19, 9990. https://doi.org/10.3390/ijerph19169990
Xue Y. Impoverishment Effect of Hydatid Disease and Precision Medical Assistance Pattern of Government: Evidence from Yushu in China. International Journal of Environmental Research and Public Health. 2022; 19(16):9990. https://doi.org/10.3390/ijerph19169990
Chicago/Turabian StyleXue, Yaozu. 2022. "Impoverishment Effect of Hydatid Disease and Precision Medical Assistance Pattern of Government: Evidence from Yushu in China" International Journal of Environmental Research and Public Health 19, no. 16: 9990. https://doi.org/10.3390/ijerph19169990
APA StyleXue, Y. (2022). Impoverishment Effect of Hydatid Disease and Precision Medical Assistance Pattern of Government: Evidence from Yushu in China. International Journal of Environmental Research and Public Health, 19(16), 9990. https://doi.org/10.3390/ijerph19169990