
Advantages of and Barriers to Crafting New Technology in Healthcare Organizations: A Qualitative Study in the COVID-19 Context


Abstract
:1. Introduction
1.1. New Technological and Nurses’ Adaptive Expertise
1.2. Job Crafting and Adaptive Expertise
1.3. Human Resource Management Practices and Adoption Job Crafting
1.4. Theoretical Framework and Propositions
2. Materials and Methods
- Do you currently use technological tools (for example, telemedicine, mobile health, electronic medical records, Santé Québec files, and new software platforms)?
- Could these technologies lead to you rethinking or reconfiguring your work, your role, and your tasks? How?
- Do you think that technological innovations could reduce your work overload?
- Do you use new technology to facilitate communication or collective work?
3. Results
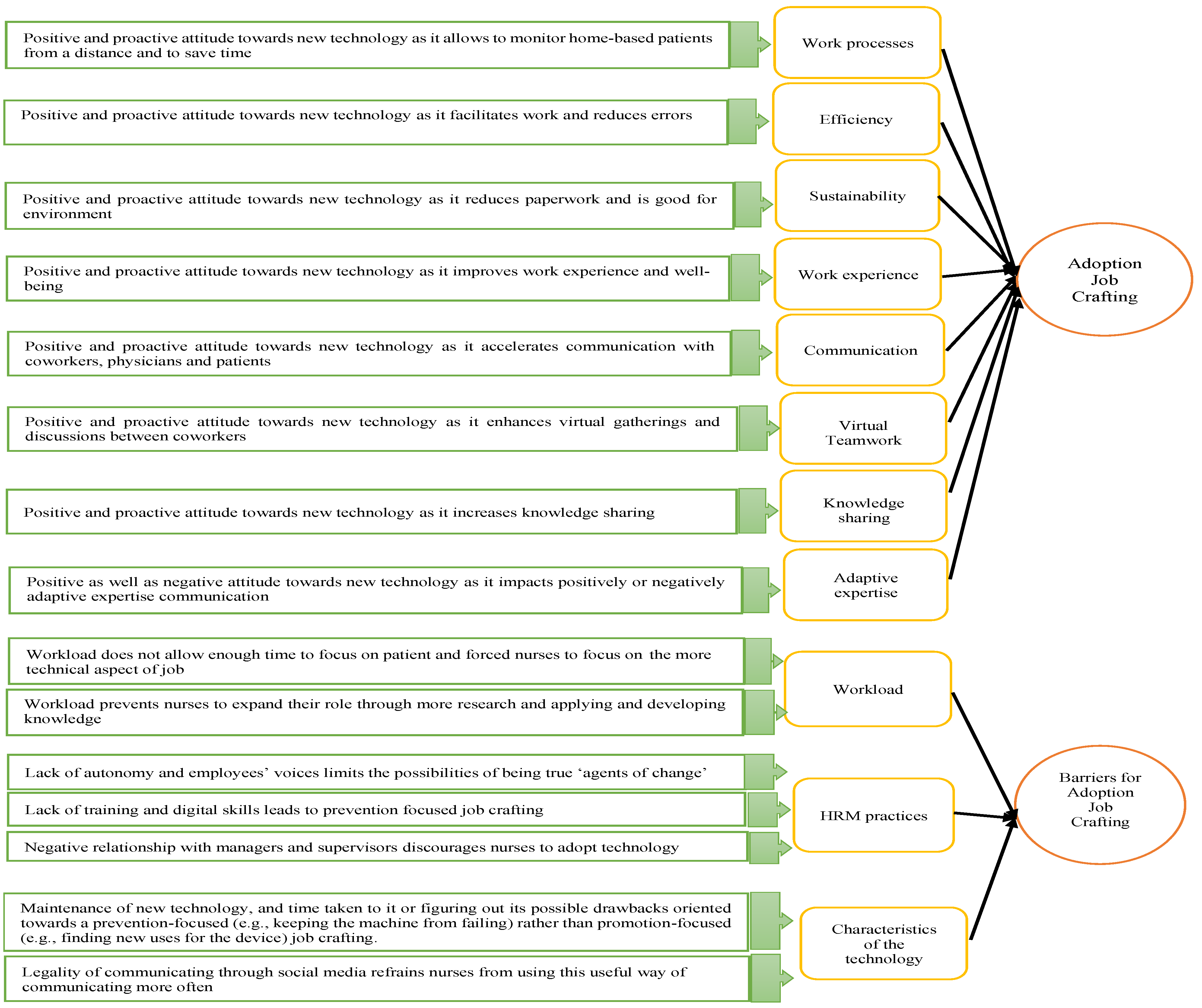
3.1. Advantages of Adoption Job Crafting Behaviors
3.1.1. Adoption Job Crafting Improves Work Processes, Reduces Errors, and Enhances Work Experience
“The device did it before, the problem is that I had to move there to go and see. Now I am able to get these measurements remotely, so I would be able to plug into my computer and then go and see”.(Oceane, inhalotherapist)
“Just as now, above each bed, there is a pressure cuff that can be programmed, so it will take the pressure regularly. So just go pick it up and see if everything is okay”.(Sabrina, Nurse)
“Of course, when they installed pressure monitors for us at the head of each bed, it was more pleasant because we didn’t have to run after a pressure device”.
“I think we could save time and energy with certain technological tools (….), it did help to save time, it becomes less stressful”.(Émili, nurse)
“Sometimes we have apps on our phone that calculate for us, if we’ve done it before, to see if it works, to make sure it’s reliable”.(Mélodie, nurse)
“I would tell you that the paperwork you have to do a good three, four hours certainly (….). Then it is good for the environment too, if we are able to leave the paper and do our electronic notes… If it would be completely electronic, it would reduce the workload, it would be really fun”.(Sabrina, Nurse)
3.1.2. Adoption Job Crafting Increases Communication, Virtual Teamwork, and Knowledge Sharing
“Depending on the platform, I would say yes. For instance, we were talking about Teams earlier, it is so interesting to be able to work on a tool live. We’re able to see each other, talk to each other, to work in document mode…this is extraordinary.”(Jeanne, senior nursing advisor)
“I have a patient with bulbar amyotrophic lateral sclerosis, well for sure speech gets more and more difficult because of his ALS. But it’s good because we can text him”.(Oceane, inhalotherapist)
“Sometimes there are exchanges about good practices, about what’s new in our field”.(Michelle, nurse)
3.1.3. Adoption Job Crafting Enhances Relationship with Patients and Adaptive Expertise
“It allows for a better evaluation, when I look at all the mental health telemedicine there has been since the pandemic. It allows us to pursue follow-ups with patients (…) while they’re staying home. So, it really removed accessibility and treatment adherence barriers, plus it’s less expensive”.(Megane, nurse)
“It’s like the use of Internet or cellphones. I’ve seen…currently, there are nurses who contact patients via Facebook or their cellphone number. The cell phone has become a working tool (…) It creates problems with other nurses who don’t like to get involved with that. I’m not paid to answer my phone 24 h/24 h. I need my private life. It is a demand that is created by individuals who try to give themselves importance and don’t know how to set their limits with patients, and who want some favors. In our deontology, we have to keep our professional distances. Because eventually we cannot favor one patient over another”.(Judith, nurse)
“It would probably be done remotely, I would verify the patient’s pulse, then I would click on my computer: yes, everything is ok, it can take it and then the machine can give it to the patient (…) It would be convenient but then again, we get more distant from our patient!”.(Marie Claude, nurse)
“Yes, there is a lack of human warmth, but at the same time in a period of a pandemic like that, the risk is quite great (…) Because you know I agree that we need human warmth, that we need somebody, but at the same time there is a big risk for the rest of the population. So, at such times I think it’s important that the risks are kept to a minimum”.(Melodie, nurse)
“But at the same time, there are studies that prove that if there is no human contact, recovery does not happen the right way. But there might be a way to bring that with… a bit like babies in incubators with hands, so maybe with a stretcher and then the hand near the window, you put your hand through the gain, through a glove in a window, maybe it’s not great but it would be less dangerous for the staff, then with a robot doing other care. To limit as much as possible”.(Melodie, nurse)
“If we get robots to move around and go check on patients instead of nurses…the robot isn’t going to catch COVID-19! Which is why technology can help a lot”.(Marie-Claude, nurse)
3.2. Barriers to Adoption Job Crafting Behaviors
3.2.1. Due to a Heavy Workload
“(…) if we had the time to be an expert for each patient, well we wouldn’t have this problem of: “I look, then I print out what I’ve read, then hey, doctor, fend for yourself.” Y’know? Because I don’t have time to think anymore, you know? Because I no longer have the time to act, I no longer have the time to investigate the file, to do a complex case search”.(Constance, nurse)
“At some point you lose your judgement, because you work like a robot”.(France, coordinating nurse)
“It is not because we have a lot of technology that we will ultimately reduce the number of staff on the floor, because a patient is not a machine, it’s not just that in the patient’s pathology either. The patient is more and more complex. We need people who think and are able to connect the dots…”.(Christelle, nurse)
3.2.2. Due to a Lack of Human Resource Management Practices
Lack of Autonomy and Employees’ Voices
“If there are things that already exist, it’s okay to use them, but it doesn’t necessarily match what you need. You know, they wouldn’t like us to create new tools but at the same time it is… We have to adapt it to our own needs (…) we won’t have the right to create something that belongs to us ‘there’”.(Laurence, chief nurse)
“You know, I’m the person who will set up, who will do the techniques, who will say: we could do that, we will change that (…)—Does your boss take a positive view of this innovative spirit?—I don’t know… she didn’t tell me. But she didn’t tell me otherwise that it wasn’t right, so I dare believe it’s fine!”.(Oceane, inhalotherapist)
Lack of Training and Digital Skills
“But I still come back to saying that sometimes it would be nice for us to get some help with training, to help us adapt to these new technologies to use them well”.(Sabine, nurse)
“People are lazy. If someone does their job for them… there’s always some people who will find a way to do something else, anything instead of working… going on the Internet, texting…”.(Karine, nurse)
“The danger still remains that there are some nurses who… will rely on the fact that the machine is doing its job, but who won’t necessarily use this time to develop and push that other side of our profession. Because right now, that’s kind of what’s happening. They will concentrate on the technique; hurry quickly and then go do something else (…) There is a risk that employees do not use this the right way.—Could this risk be reduced with training?—Yes, I think so”.(Laurence, chief nurse)
“Well, we have to admit that in hospital centers we are given a lot of training as it pertains to equipment…”.(Eric, nursing care advisor)
“I didn’t really have any training; it was during my days (….) I learned to use the software, but I didn’t have any training as such there”.(Sabine, Nurse)
“… But rarely will we get training at a professional level. We need to go and find it by ourselves, because it’s pretty rare that we’ll get any interesting training offered by the employer”.(Eric, nursing care advisor)
Negative Relationship with Managers and Supervisors
“This is what we do in our job, we are like caught in a whirlwind and we say to ourselves: it can never get better. It’s like we’re discouraged by all of this. It takes a lot of energy for little changes like that. So, we have become somewhat resigned in our job”.(Christelle, nurse)
“There are many solutions, nurses are full of ideas, but up there, it gets blocked”.(Blandine, nurse)
“So, it’s a big adaptation. It doesn’t look that bad, but for someone who’s used to their routine and then does a lot of things like that… there’s resistance. At this moment you need to see why there is resistance, what is causing the problem, then it is necessary that the worries, the questions are resolved and then they have become aware a little of their technique, in their way of doing things too, but it’s not necessarily a good time for the whole team”.(Laurence, chief nurse)
“You really need to convince them about the necessity of change”.(Monique, chief nurse)
“For sure this will need to be done gradually. There are a lot of people who are reluctant to change”.(Marie-Claude, nurse)
“In the beginning it was Zoom, and then wasn’t Zoom anymore, it was Teams. It’s always different from one to the other…and I’m not from your generation, for me it’s complicated. I have to figure out where the microphone is again, how everything works, etc., etc. Ok now I finally got comfortable working with Teams, but don’t come to back to me six months from now with another gimmick which you know will basically be the same thing… eventually I’m still going to need to adapt to it all over again. I think it’s a waste of time”.(Adele, nursing care advisor)
3.2.3. Due to the Characteristics of the Technology
“Because sometimes devices that do not work well can also cause frustration: we rely on that to succeed in doing something and then in the end it doesn’t work (…) So it has repercussions. The fact that someone fails in something and then they go looking for their colleague to help, well the colleague she does not do her job during that time. She’s going to help you know? So, it’s falling behind too. So, it has different repercussions”.(Laurence, chief nurse)
“Well, most of the time yes, I find it easier but sometimes it’s a little frustrating to see … it’s always all about having to search, get by, the frustration of wasting time with it. Sometimes I have to ask the secretary why it’s not working; can I do such and such a thing… it’s mostly that”.(Sabine, nurse)
“Technology is not adapted to nurses’ work” and that there is a “lack of IT tools at work” where they “don’t even have Wi-Fi”.(Michelle, nurse)
“It is a bit stressful because, (….), they have to go to two systems… that’s good complicated”.(Blandine, nurse)
4. Discussion
4.1. Theoretical Contributions
4.2. Practical Implications
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ćwiklicki, M.; Klich, J.; Chen, J. The adaptiveness of the healthcare system to the fourth industrial revolution: A preliminary analysis. Futures 2020, 122, 102602. [Google Scholar] [CrossRef]
- Strudwick, G.; Wiljer, D.; Inglis, F. Nursing and Compassionate Care in a Technological World: A Discussion Paper; AMS Healthcare: Toronto, ON, Canada, 2020. [Google Scholar] [CrossRef]
- Meskó, B.; Hetényi, G.; Győrffy, Z. Will artificial intelligence solve the human resource crisis in healthcare? BMC Health Serv. Res. 2018, 18, 545. [Google Scholar] [CrossRef] [PubMed]
- Collings, D.G.; McMackin, J.; Nyberg, A.J.; Wright, P.M. Strategic Human Resource Management and COVID-19: Emerging Challenges and Research Opportunities. J. Manag. Stud. 2021, 58, 1378–1382. [Google Scholar] [CrossRef]
- Sergeeva, A.; Huysman, M.; Faraj, S. Losing touch: How robots transform the practice of surgery. In Proceedings of the Academy of Management Annual Meeting Proceedings, Chicago, IL, USA, 10–14 August 2018. [Google Scholar] [CrossRef]
- Vrontis, D.; Christofi, M.; Pereira, V.; Tarba, S.; Makrides, A.; Trichina, E. Artificial intelligence, robotics, advanced technologies and human resource management: A systematic review. Int. J. Hum. Resour. Manag. 2021, 33, 1237–1266. [Google Scholar] [CrossRef]
- Kraus, S.; Schiavone, F.; Pluzhnikova, A.; Invernizzi, A.C. Digital transformation in healthcare: Analyzing the current state-of-research. J. Bus. Res. 2021, 123, 557–567. [Google Scholar] [CrossRef]
- Taiminen, H.S.M.; Saraniemi, S.; Parkinson, J. Incorporating digital self services into integrated mental health care: A physician’s perspective. Eur. J. Mark. 2018, 52, 2234–2250. [Google Scholar] [CrossRef]
- Vila, C.; Ugarte, D.; Ríos, J.; Abellán, J.V. Project-based collaborative engineering learning to develop Industry 4.0 skills within a PLM framework. Procedia Manuf. 2017, 13, 1269–1276. [Google Scholar] [CrossRef]
- Pepito, J.A.; Locsin, R. Can nurses remain relevant in a technologically advanced future? Int. J. Nurs. Sci. 2019, 6, 106–110. [Google Scholar] [CrossRef]
- Carnevale, J.B.; Hatak, I. Employee adjustment and well-being in the era of Covid-19: Implications for human resource management. J. Bus. Res. 2020, 116, 183–187. [Google Scholar] [CrossRef]
- Ajzen, I. Nature and operation of attitudes. Annu. Rev. Psychol. 2001, 52, 27–58. [Google Scholar] [CrossRef]
- Lapointe, L.; Rivard, S.A. Multilevel Model of Resistance to Information Technology Implementation. MIS Q. 2005, 29, 461–491. [Google Scholar] [CrossRef]
- Cucciniello, M.; Lapsley, I.; Nasi, G. Managing health care in the digital world: A comparative analysis. Health Serv. Manag. Res. 2016, 29, 132–142. [Google Scholar] [CrossRef]
- Holford, W.D. The algorithmic workplace and its enactive effect on the future of professions. Futures 2020, 122, 102609. [Google Scholar] [CrossRef]
- Park, D.H.L.; Kim, W.; Kang, H. Organizational support and adaptive performance: The revolving structural relationships between job crafting, work engagement and adaptive performance. Sustainability 2020, 12, 4872. [Google Scholar] [CrossRef]
- Archibald, M.; Barnard, A. Futurism in nursing: Technology, robotics and the fundamentals of care. J. Clin. Nurs. 2018, 27, 2473–2480. [Google Scholar] [CrossRef]
- Petrou, P.; Demerouti, E.; Schaufeli, W.B. Crafting the change: The role of employee job crafting behaviors for successful organizational change. J. Manag. 2018, 44, 1766–1792. [Google Scholar] [CrossRef]
- Lichtenthaler, W.P.; Fischbach, A. Leadership, job crafting, and employee health performance. Leadersh. Organ. Dev. J. 2018, 39, 620–632. [Google Scholar] [CrossRef]
- Bruning, P.F.; Campion, M.A. Exploring job crafting: Diagnosing and responding to the ways employees adjust their jobs. Bus. Horiz. 2019, 62, 625–635. [Google Scholar] [CrossRef]
- Lazazzara, A.; Tims, M. de Gennaro, D. The process of reinventing a job: A meta–synthesis of qualitative job crafting research. J. Vocat. Behav. 2020, 116, 103267. [Google Scholar] [CrossRef]
- Bruning, P.F.; Campion, M.A. A Role–resource Approach–avoidance Model of Job Crafting: A Multimethod Integration and Extension of Job Crafting Theory. Acad. Manag. J. 2018, 61, 499–522. [Google Scholar] [CrossRef]
- Zhang, F.; Parker, S.K. Reorienting job crafting research: A hierarchical structure of job crafting concepts and integrative review. J. Organ. Behav. 2018, 40, 126–146. [Google Scholar] [CrossRef]
- Meijerink, J.; Bos-Nehles, A.; de Leede, J. How employees’ pro-activity translates high-commitment HRM systems into work engagement: The mediating role of job crafting. Int. J. Hum. Resour. Manag. 2018, 31, 2893–2918. [Google Scholar] [CrossRef]
- Rudolph, C.W.; Katz, I.M.; Lavigne, K.N.; Zacher, H. Job crafting: A meta-analysis of relationships with individual differences, job characteristics, and work outcomes. J. Vocat. Behav. 2017, 102, 112–138. [Google Scholar] [CrossRef]
- Wrzesniewski, A.; Dutton, J.E. Crafting a job: Revisioning employees as active crafters of their work. Acad. Manag. Rev. 2001, 26, 179–201. [Google Scholar] [CrossRef]
- Kniffin, K.M.; Narayanan, J.; Anseel, F.; Antonakis, J.; Ashford, S.; Bakker, A.B.; vanvugt, M. COVID-19 and the Workplace: Implications, Issues, and Insights for Future Research and Action. Am. Psychol. 2020, 76, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Eden, R.; Burton-Jones, A.; Casey, V.; Draheim, M. Digital transformation requires workforce transformation. MIS Q. Exec. 2019, 18, 1–17. [Google Scholar] [CrossRef]
- Bakker, A.B. Job crafting among health care professionals: The role of work engagement. J. Nurs. Manag. 2017, 26, 321–331. [Google Scholar] [CrossRef]
- Booth, R.G.; Strudwick, G.; McBride, S.; O’Connor, S.; Lopez, A.L.S. How the nursing profession should adapt for a digital future. BMJ 2021, 373, n1190. [Google Scholar] [CrossRef]
- Baudier, P.; Kondrateva, G.; Ammi, C. The future of Telemedicine Cabin? The case of the French students’ acceptability. Futures 2020, 122, 102595. [Google Scholar] [CrossRef]
- Liang, H.-F.; Wu, K.-M.; Weng, C.-H.; Hsieh, H.-W. Nurses’ views on the potential use of robots in the pediatric unit. J. Pediatr. Nurs. 2019, 47, e58–e64. [Google Scholar] [CrossRef] [PubMed]
- Pulakos, E.D.; Arad, S.; Donovan, M.A.; Plamondon, K.E. Adaptability in the workplace: Development of a taxonomy of adaptive performance. J. Appl. Psychol. 2000, 85, 612–624. [Google Scholar] [CrossRef]
- Fuller, A.; Unwin, L. Job Crafting and identity in low-grade work: How hospital porters redefine the value of their work and expertise. Vocat. Learn. 2017, 10, 307–324. [Google Scholar] [CrossRef]
- Mattarelli, E.; Tagliaventi, M.R. How offshore professionals’ job dissatisfaction can promote further offshoring: Organizational outcomes of job crafting. J. Manag. Stud. 2015, 52, 585–620. [Google Scholar] [CrossRef]
- Lichtenthaler, P.W.; Fischbach, A. A meta-analysis on promotion-and prevention-focused job crafting. Eur. J. Work. Organ. Psychol. 2018, 28, 30–50. [Google Scholar] [CrossRef]
- Peng, J.; Li, M.; Wang, Z.; Lin, Y. Transformational leadership and employees’ reactions to organizational change: Evidence from a meta-analysis. J. Appl. Behav. Sci. 2020, 57, 369–397. [Google Scholar] [CrossRef]
- Bateman, T.S.; Crant, J.M. The proactive component of organizational behavior: A measure and correlates. J. Organ. Behav. 1993, 14, 103–118. [Google Scholar] [CrossRef]
- Esteves, T.; Pereira Lopes, M. Leading to crafting: The relation between leadership perception and nurses’ job crafting. West. J. Nurs. Res. 2017, 39, 763–783. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E. Multiple levels in job demands-resources theory: Implications for employee well-being and performance. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Tims, M.; Bakker, A.B.; Derks, D. The impact of job crafting on job demands, job resources, and well-being. J. Occup. Health Psychol. 2013, 18, 230–240. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; De Jong, J. Sociocultural and ecological views of trauma: Replacing cognitive-emotional models. In Facilitating Resilience and Recovery Following Trauma; Guilford Press: New York, NY, USA, 2014; 346p, pp. 69–90. Available online: https://doi.org/11245/1.400933 (accessed on 22 June 2022).
- Mansour, S.; Nogues, S.; Tremblay, D.-G. Psychosocial safety climate as a mediator between high-performance work practices and service recovery performance: An international study in the airline industry. Int. J. Hum. Resour. Manag. 2021, 1–35. [Google Scholar] [CrossRef]
- Hobfoll, S.E. Conservation of resource caravans and engaged settings. J. Occup. Organ. Psychol. 2011, 84, 116–122. [Google Scholar] [CrossRef]
- Halbesleben, J.R.; Neveu, J.-P.; Paustian-Underdahl, S.C.; Westman, M. Getting to the “COR” understanding the role of resources in conservation of resources theory. J. Manag. 2014, 40, 1334–1364. [Google Scholar] [CrossRef]
- Davis, F.D. A Technology Acceptance Model for Empirically Testing New End User Information Systems: Theory and Results. Ph.D. Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 1986. [Google Scholar]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Krippendorff, K. Content Analysis: An Introduction to Its Methodology; Sage Publications: Thousand Oaks, NP, USA, 1980. [Google Scholar]
- Sandelowski, M. Qualitative analysis: What it is and how to begin? Res. Nurs. Health 1995, 18, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngäs, H. The qualitative content analysis. J. Adv. Nurs. 2007, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Gioia, D.A.; Corley, K.G.; Hamilton, A. Seeking qualitative rigor in inductive research: Notes on the Gioia methodology. Organ. Res. Methods 2012, 16, 15–31. [Google Scholar] [CrossRef]
- Drisko, J.; Maschii, T. Content Analysis; Oxford Press: New York, NY, USA, 2016; p. 208. [Google Scholar]
- Landaeta, R.E.; Mun, J.H.; Rabadi, G. Identifying sources of resistance to change in healthcare. Int. J. Healthc. Technol. Manag. 2008, 9, 75–96. [Google Scholar] [CrossRef]
- Van Den Heuvel, M.; Demerouti, E.; Peeters, M. The job crafting intervention: Effects on job resources, self-efficacy, and affective well-being. J. Occup. Organ. Psychol. 2015, 88, 511–532. [Google Scholar] [CrossRef]
- Mansour, S.; Tremblay, D.-G. The mediating role of work engagement between psychosocial safety climate and organisational citizenship behaviours: A study in the nursing and health sector in Quebec. Int. J. Hum. Resour. Dev. Manag. 2018, 18, 51–71. [Google Scholar] [CrossRef]
- Mansour, S.; Tremblay, D.-G. Work–family conflict/family–work conflict, job stress, burnout and intention to leave in the hotel industry in Quebec (Canada): Moderating role of need for family friendly practices as “resource passageways”. Int. J. Hum. Resour. Manag. 2018, 29, 2399–2430. [Google Scholar] [CrossRef]
- Faraj, S.; Pachidi, S.; Sayegh, K. Working and organizing in the age of the learning algorithm. Inf. Organ. 2018, 28, 62–70. [Google Scholar] [CrossRef]

{kind=link}
| Sample’s Characteristics | n | % | |
|---|---|---|---|
| Gender | Male | 3 | 7.14 |
| Female | 39 | 92.86 | |
| Age | 20–30 | 4 | 9.5 |
| 31–40 | 10 | 40.48 | |
| 41–50 | 17 | 38.1 | |
| 51–60 | 7 | 16.16 | |
| 61–70 | 4 | 9.52 | |
| Position | Nurse | 35 | 83.33 |
| Inhalotherapist | 1 | 2.38 | |
| Nursing Care Advisor | 3 | 7.14 | |
| Head Nurse | 3 | 7.14 | |
| Employer | Hospital | 34 | 80.95 |
| Clinic | 4 | 9.5 | |
| University Hospital Center | 3 | 7.14 | |
| Community Center | 1 | 2.38 | |
| Seniority in Profession | 1–5 years | 1 | 2.38 |
| 6–10 years | 5 | 11.9 | |
| 11–15 years | 9 | 21.42 | |
| 16–20 years | 9 | 21.42 | |
| 21–25 years | 4 | 9.5 | |
| 26–30 years | 6 | 14.28 | |
| 31 years and over | 5 | 11.9 | |
| N.A | 3 | 7.14 | |
| Seniority in Position | 1–5 years | 22 | 52.38 |
| 6–10 years | 9 | 21.42 | |
| 11–15 years | 5 | 11.9 | |
| 16–20 years | 2 | 4.76 | |
| N.A | 4 | 9.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mansour, S.; Nogues, S. Advantages of and Barriers to Crafting New Technology in Healthcare Organizations: A Qualitative Study in the COVID-19 Context. Int. J. Environ. Res. Public Health 2022, 19, 9951. https://doi.org/10.3390/ijerph19169951
Mansour S, Nogues S. Advantages of and Barriers to Crafting New Technology in Healthcare Organizations: A Qualitative Study in the COVID-19 Context. International Journal of Environmental Research and Public Health. 2022; 19(16):9951. https://doi.org/10.3390/ijerph19169951
Chicago/Turabian StyleMansour, Sari, and Sarah Nogues. 2022. "Advantages of and Barriers to Crafting New Technology in Healthcare Organizations: A Qualitative Study in the COVID-19 Context" International Journal of Environmental Research and Public Health 19, no. 16: 9951. https://doi.org/10.3390/ijerph19169951
APA StyleMansour, S., & Nogues, S. (2022). Advantages of and Barriers to Crafting New Technology in Healthcare Organizations: A Qualitative Study in the COVID-19 Context. International Journal of Environmental Research and Public Health, 19(16), 9951. https://doi.org/10.3390/ijerph19169951