
The Meaning of “Hygiene” and Its Linked Practices in a Low-Income Urban Community in Bangladesh

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Sites and Household Selection
2.2. Data Collection
2.2.1. Observations
2.2.2. In-Depth Interviews
2.3. Data Analysis
2.4. Ethics
3. Results
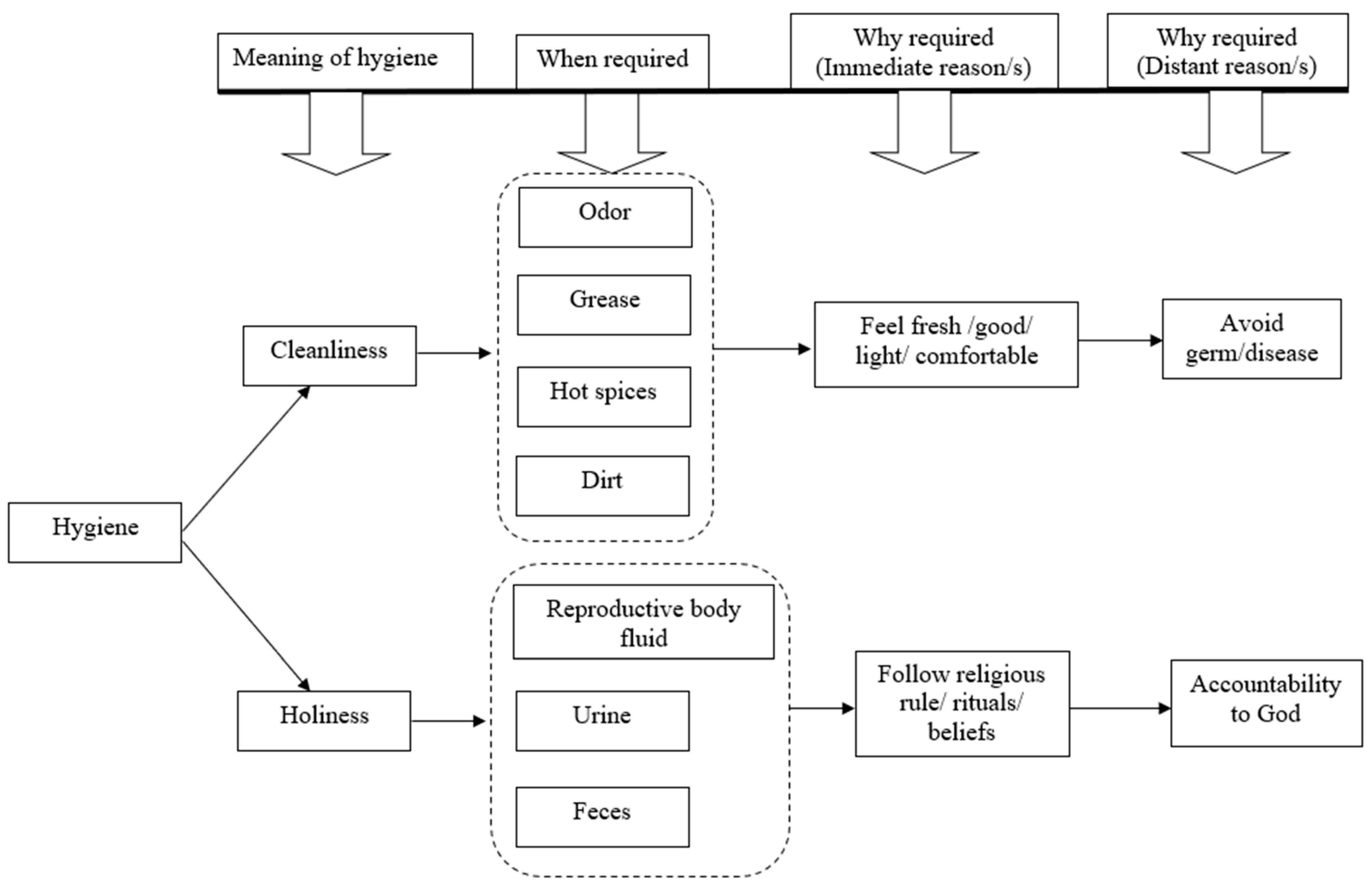
3.1. The Concept of Hygiene
3.2. Cleanliness
3.3. Holiness
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jamison, D.T.; Breman, J.G.; Measham, A.R.; Alleyne, G.; Claeson, M.; Evans, D.B.; Jha, P.; Mills, A.; Musgrove, P. Disease Control Priorities in Developing Countries; The World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Freeman, M.C.; Stocks, M.E.; Cumming, O.; Jeandron, A.; Higgins, J.P.; Wolf, J.; Pruss-Ustun, A.; Bonjour, S.; Hunter, P.R.; Fewtrell, L.; et al. Hygiene and health: Systematic review of handwashing practices worldwide and update of health effects. Trop. Med. Int. Health 2014, 19, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.; Johnston, R.; Freeman, M.C.; Ram, P.K.; Slaymaker, T.; Laurenz, E.; Pruss-Ustun, A. Handwashing with soap after potential faecal contact: Global, regional and country estimates. Int. J. Epidemiol. 2019, 48, 1204–1218. [Google Scholar] [CrossRef] [PubMed]
- Chittleborough, C.R.; Nicholson, A.L.; Basker, E.; Bell, S.; Campbell, R. Factors influencing hand washing behaviour in primary schools: Process evaluation within a randomized controlled trial. Health Educ. Res. 2012, 27, 1055–1068. [Google Scholar] [CrossRef] [PubMed]
- Handwashing. A Family Activity. Available online: https://www.cdc.gov/handwashing/handwashing-family.html (accessed on 22 June 2022).
- Why Handwashing with Soap Is the Most Effective Way to Stop Viruses. Available online: https://www.gavi.org/vaccineswork/why-washing-your-hands-so-important-during-pandemic (accessed on 22 June 2022).
- Curtis, V.A.; Danquah, L.O.; Aunger, R.V. Planned, motivated and habitual hygiene behaviour: An eleven country review. Health Educ. Res. 2009, 24, 655–673. [Google Scholar] [CrossRef]
- White, S.; Thorseth, A.H.; Dreibelbis, R.; Curtis, V. The determinants of handwashing behaviour in domestic settings: An integrative systematic review. Int. J. Hyg. Environ. Health 2020, 227, 113512. [Google Scholar] [CrossRef]
- Germ Theory. Available online: https://curiosity.lib.harvard.edu/contagion/feature/germ-theory (accessed on 22 June 2022).
- Douglas, M. Purity and Danger: An Analysis of Concepts of Pollution and Taboo; Routledge: Oxfordshire, UK, 1966. [Google Scholar]
- Curtis, V. The Dangers of Dirt: Household Hygiene and Health; SL Curtis: Istanbul, Turkey, 1998. [Google Scholar]
- Curtis, V.; Biran, A.; Deverell, K.; Hughes, C.; Bellamy, K.; Drasar, B. Hygiene in the home: Relating bugs and behaviour. Soc. Sci. Med. 2003, 57, 657–672. [Google Scholar] [CrossRef]
- Curtis, V.; Kanki, B.; Cousens, S.; Sanou, A.; Diallo, I.; Mertens, T. Dirt and diarrhoea: Formative research in hygiene promotion programmes. Health Policy Plan 1997, 12, 122–131. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sultana, R.; Tamason, C.C.; Carstensen, L.S.; Ferdous, J.; Hossain, Z.Z.; Begum, A.; Jensen, P.K.M. Water usage, hygiene and diarrhea in low-income urban communities-A mixed method prospective longitudinal study. MethodsX 2019, 6, 2822–2837. [Google Scholar] [CrossRef]
- WHO; Safety WP. WHO Guidelines on Hand Hygiene in Health Care; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Cousens, S.; Kanki, B.; Toure, S.; Diallo, I.; Curtis, V. Reactivity and repeatability of hygiene behaviour: Structured observations from Burkina Faso. Soc. Sci. Med. 1996, 43, 1299–1308. [Google Scholar] [CrossRef]
- Orner, K.; Naughton, C.; Stenstrom, T.; Mihelcic, J.; Verbyla, M. Water and Sanitation for the 21st Century: Health and Microbiological Aspects of Excreta and Wastewater Management (Global Water Pathogen Project); UNESCO: London, UK, 2018. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Creswell, J.W.; Miller, D.L. Determining validity in qualitative inquiry. Theory Pract. 2000, 39, 124–130. [Google Scholar] [CrossRef]
- Chowdhury, F.; Khan, I.A.; Patel, S.; Siddiq, A.U.; Saha, N.C.; Khan, A.I.; Saha, A.; Cravioto, A.; Clemens, J.; Qadri, F. Diarrheal illness and healthcare seeking behavior among a population at high risk for diarrhea in Dhaka, Bangladesh. PLoS ONE 2015, 10, e0130105. [Google Scholar] [CrossRef]
- Jarman, A.F.; Long, S.E.; Robertson, S.E.; Nasrin, S.; Alam, N.H.; McGregor, A.J.; Levine, A.C. Sex and Gender Differences in Acute Pediatric Diarrhea: A Secondary Analysis of the DHAKA Study. J. Epidemiol. Glob. Health 2018, 8, 42–47. [Google Scholar] [CrossRef]
- Esrey, S.A.; Potash, J.B.; Roberts, L.; Shiff, C. Effects of improved water supply and sanitation on ascariasis, diarrhoea, dracunculiasis, hookworm infection, schistosomiasis, and trachoma. Bull. World Health Organ. 1991, 69, 609. [Google Scholar] [PubMed]
- Van der Hoek, W.; Konradsen, F.; Ensink, J.H.; Mudasser, M.; Jensen, P.K. Irrigation water as a source of drinking water: Is safe use possible? Trop. Med. Int. Health 2001, 6, 46–54. [Google Scholar] [CrossRef]
- Stelmach, R.D.; Clasen, T. Household water quantity and health: A systematic review. Int. J. Environ. Res. Public Health 2015, 12, 5954–5974. [Google Scholar] [CrossRef]
- Boyer, P.; Lienard, P. Why ritualized behavior? Precaution Systems and action parsing in developmental, pathological and cultural rituals. Behav. Brain Sci. 2006, 29, 595–613. [Google Scholar] [CrossRef]
- Foucault, M. Michel Foucault: Key Concepts, 1st ed.; Routledge: New York, NY, USA, 2011. [Google Scholar]
- Bühler, G.; Müller, F.M. Chapter 5. In The Laws of Manu; Clarendon Press: Oxford, UK, 1886; Volume 25. [Google Scholar]
- Khuan, N.W.; Shaban, R.Z.; van de Mortel, T. The influence of religious and cultural beliefs on hand hygiene behaviour in the United Arab Emirates. Infect. Dis. Health 2018, 23, 225–236. [Google Scholar] [CrossRef]
- Method of Istinja: Method of Cleansing the Excretory Organs. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwi5p6ms-drzAhXEjdgFHfWHD_wQFnoECAUQAQ&url=https%3A%2F%2Fdata2.dawateislami.net%2FData%2FBooks%2FDownload%2Fen%2Fpdf%2F2011%2F551-1.pdf&usg=AOvVaw0KcgEPhTKQpJsdvxY9RBFb (accessed on 20 March 2022).
- Parveen, S.; Islam, M.S.; Begum, M.; Alam, M.-U.; Sazzad, H.M.; Sultana, R.; Rahman, M.; Gurley, E.S.; Hossain, M.J.; Luby, S.P. It’s not only what you say, it’s also how you say it: Communicating nipah virus prevention messages during an outbreak in Bangladesh. BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef]
- Blum, L.S.; Khan, R.; Nahar, N.; Breiman, R.F. In-depth assessment of an outbreak of Nipah encephalitis with person-to-person transmission in Bangladesh: Implications for prevention and control strategies. Am. J. Trop. Med. Hyg. 2009, 80, 96–102. [Google Scholar] [CrossRef]
- WHO. Guidelines on Hand Hygiene in Health Care: First Global Patient Safety Challenge Clear Care is Safer Care. Available online: https://www.ncbi.nlm.nih.gov/books/NBK143998/ (accessed on 20 March 2022).
- Akhter, S.; Bashar, F.; Kamruzzaman, M.; Mahmood, N.; Rahman, A.; Anwar, I.; Hawkes, S. A Rapid Ethnographic Assessment of Cultural and Social Perceptions and Practices About COVID-19 in Bangladesh: What the Policy Makers and Program Planners Should Know. Qual. Health Res. 2022, 32, 10497323221091516. [Google Scholar] [CrossRef]
- Tamason, C.C.; Bessias, S.; Villada, A.; Tulsiani, S.M.; Ensink, J.H.; Gurley, E.S.; Jensen, P.K.M. Measuring domestic water use: A systematic review of methodologies that measure unmetered water use in low-income settings. Trop. Med. Int. Health 2016, 21, 1389–1402. [Google Scholar] [CrossRef]
- Muniina, K.; Maksimovic, C.; Graham, N. A novel approach for estimating urban water end use characteristics of cities in the developing world. Urban Water J. 2017, 14, 750–757. [Google Scholar] [CrossRef]
- Milton, A.H.; Rahman, H.; Smith, W.; Shrestha, R.; Dear, K. Water consumption patterns in rural Bangladesh: Are we underestimating total arsenic load? J. Water Health 2006, 4, 431–436. [Google Scholar] [CrossRef]
- Suen, L.K.; So, Z.Y.; Yeung, S.K.; Lo, K.Y.; Lam, S.C. Epidemiological investigation on hand hygiene knowledge and behaviour: A cross-sectional study on gender disparity. BMC Public Health 2019, 19, 1–14. [Google Scholar] [CrossRef]
- Mariwah, S.; Hampshire, K.; Kasim, A. The impact of gender and physical environment on the handwashing behaviour of university students in Ghana. Trop. Med. Int. Health 2012, 17, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Elkhawaga, G.; El-Masry, R. Knowledge, Beliefs and Self-reported Practices of Hand Hygiene among Egyptian Medical Students: Does Gender Difference Play a Role? J. Public Health Dev. Ctries. 2017, 3, 418–425. [Google Scholar]
- Eriksson, K.; Dickins, T.E.; Strimling, P. Global sex differences in hygiene norms and their relation to sex equality. PLoS Glob. Public Health 2022, 2, e0000591. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Population (%) |
|---|---|
| Total Participants | 32 |
| Gender | |
| Male | 8 (25) |
| Female | 24 (75) |
| Age | |
| 18–30 | 11 (34) |
| 31–45 | 15 (47) |
| 46–60 | 5 (16) |
| 60+ | 1 (3) |
| Religion | |
| Muslim | 32 (100) |
| Non-Earning | |
| Housewife | 16 (50) |
| Unemployed | 1 (3) |
| Earning | |
| Garment/Factory Worker | 7 (22) |
| Small Business Employee | 3 (9) |
| Service Holder | 2 (6) |
| Day Laborer | 2 (6) |
| Beggar | 1 (3) |
| Education | |
| No Education | 7 (22) |
| Did Not Complete Primary Education | 7 (22) |
| Completed Primary Education | 12 (38) |
| Completed Secondary Education | 3 (9) |
| Completed Higher Secondary Education | 1 (3) |
| Graduate | 2 (6) |
| A. Cleanliness of Body and Home |
| “Suppose, I make myself, my room, and my bed clean. I wash all the utensils in my room; this is beautiful to me. I clean my body and I bathe using soap and water, put oil on my head, wash my clothes, these make me feel good. [What is the benefit of this cleaning?] The benefit is my body feels clean and I feel good. [Consider not washing yourself, what happens then?] I sweat during cooking. When my husband will ask for food, my child will ask for food, should I serve them with these hands? I wash myself, and I serve food. Then it feels clean and good to serve. [Is there any other reason for cleanliness?] No, not at all… Cleanliness is part of faith.” (A female participant.) |
| “Suppose, I dust off the room with a broom, pull ashes from the cooking stove, won’t it (hands and legs) get dirty? Then I will have to rinse my hands and feet. This type of dirty work requires rinsing of hands and feet.” (A female participant.) |
| B. Cleanliness of Hands |
| “To clean my cooking utensils, I scrub them with ashes, so black ash smears on my hands. Then I use soap to remove the black ash…soap helps to remove the stain. I use soap, because when my hands look black, it (ash/dirt) can smear on my face, cloth and eyes if I touch them, won’t it? … I use soap during bath to remove dirt and I feel good. If I cut fish, then I have to use soap as my hands stink. Suppose, you came and sat with me, you would say “move, you smell of fish”, won’t you say that? But if (I) wash my hands with soap it will not stink. Although nobody would get that stink (after defecation), it’s for my own sake and for my own conscience (I wash with soap after defecation). If I touch something or cut vegetables (without washing with soap after defecation), I feel bad myself thinking that, something can smear on my hand (after defecation), something can happen inside (my body). If I cook the food it can be spoilt, it can stink and if (someone) eats that food, his/her stomach can get upset.” (A female participant.) |
| “After cutting fish my hands get a fishy stench. After washing the cloth used for menstruation or after cleaning the child’s feces, it feels dirty and (I) feel uneasy that my hands are dirty. Nothing should be done or touched without washing those hands with soap. [Why, what happens if you touch anything (without washing)?] If I touch, I feel bad myself, there might be germ or (you know) dirt is dirt. It doesn’t feel good within me. That is why I wash my hands with soap.” (A female participant.) |
| A. Activities That Were Considered Unholy |
| “(After intercourse a bath is needed to be taken) This (bath) is separate (than normal bath). This has to be done within the (same) night. Body has to return to holiness, since (I) cannot touch anything with an unholy body, I cannot do any task. I do not even broom the floor. Whatever I do, I do it after bathing. The body is unholy after that (intercourse)…ablution is required separately (during bath) and religious verses have to be recited to make the body holy. Two to three times ablution is required (during bath). At first, I have to perform the ablution and then pour water on the body, and after completing the bath I need to perform ablution again to make the body holy. (During bathing, someone) can use soap, but it is not mandatory, using only water can make the body holy.” (A female participant.) |
| “During that time (religious bath after menstruation) I need two big buckets of water. I need to wash my hair, cut nails, clean genital properly otherwise, my prayer (namaj) will not be guaranteed… During that time, clothes need to be washed properly and thoroughly, three times (with water) otherwise it will not be holy. It (religious bath) has separate rules- starting with performing ablution, followed by pouring water down the whole body, then smearing soap on the body, again pouring water to clean the soap and finally perform ablution again… The body will become holy after the ablution. Regular bathing does not always require soap, so I do not use soap every day for a regular bath.” (A female participant.) |
| “So, my wife stays home from Thursday to Friday. She stays a bit unholy on Thursdays. During that time (intercourse), the room, for example, the bed and bedsheets remain impure/unclean/unholy. We change the bedsheets and put new sheets on, moreover, the bedsheets are washed on Friday. So, if Allah wants it (everything) will be holy then.” (A male participant.) |
| B. Genital and Anal Cleansing |
| “Usually when I go to the toilet, I do not use soap, but I do use a separate piece of cloth to clean myself. I use a cloth (wet the cloth with water) rather than using excess water. Yes, whether I defecate or urinate, I use cloth. After every two to three days I wash the cloth and dry it. Many people use soap but I usually just use the cloth” (A female participant.) |
| “Suppose cleanliness of prayer (namaj) includes using water dhila kulukh after urination. This way I became holy. Suppose I went to the toilet, washed my hands, this way I became clean and my body became holy. If I am not praying (namaj), it is okay if my body is unholy. If I am praying (namaj) 5 times a day, if I step on dirt or touch the chickens, I need to wash my hands with soap and then perform ablution. Moreover, if I have dirt on me (in fingers/nails), my prayer will not be accepted.” (A male participant.) |
| “Brother (referring to the interviewer), I do not use (after urination) water: there is no reason to it. Brother, you know it is the devils… It is because we Muslims are supposed to be pure and holy all the time. I do not even perform the regular prayers, so I do not even use water (after urination). Actually, it has become a habit, so I do not bother taking water (to use after urination).” (A male participant.) |
| C. Religious Motivations For Cleansing Practices |
| “I wipe the floor everyday as I perform prayer (namaj) every day at my house. Moreover, the floor and bed gets dirty with dust as children get on the floor with dust on their feet.” (A female participant.) |
| “Yes, after both defecating and urinating, I wash both hands, legs and then perform ablution. It is said to always stay in the state of holiness and purity by being in the state of ablution-because you never know when death will come. I can die anytime, even now, leaving all my work. That is why I stay in the ablution state, since dying while in the state of ablution will give me a lot of spiritual reward by the almighty.” (A female participant.) |
| “People perform ablution to stay holy and pure for regular prayer (namaj). If you can keep yourself always in ablution mode, it is good for you. Otherwise, people take bath only once a day, it is not possible to take bath five times a day. Therefore, ablution is the solution to remain holy. Moreover, if a Muslim man keeps himself always in holy state, it is good for him. No one can say when death will come. That is why, I think it is best to keep oneself in the holy state all the time.” (A male participant.) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sultana, R.; Nahar, N.; Rimi, N.A.; Swarna, S.T.; Khan, S.; Saifullah, M.K.; Kabir, H.; Jensen, P.K.M. The Meaning of “Hygiene” and Its Linked Practices in a Low-Income Urban Community in Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 9823. https://doi.org/10.3390/ijerph19169823
Sultana R, Nahar N, Rimi NA, Swarna ST, Khan S, Saifullah MK, Kabir H, Jensen PKM. The Meaning of “Hygiene” and Its Linked Practices in a Low-Income Urban Community in Bangladesh. International Journal of Environmental Research and Public Health. 2022; 19(16):9823. https://doi.org/10.3390/ijerph19169823
Chicago/Turabian StyleSultana, Rebeca, Nazmun Nahar, Nadia Ali Rimi, Sayeda Tasnuva Swarna, Shifat Khan, Md. Khaled Saifullah, Humayun Kabir, and Peter Kjær Mackie Jensen. 2022. "The Meaning of “Hygiene” and Its Linked Practices in a Low-Income Urban Community in Bangladesh" International Journal of Environmental Research and Public Health 19, no. 16: 9823. https://doi.org/10.3390/ijerph19169823
APA StyleSultana, R., Nahar, N., Rimi, N. A., Swarna, S. T., Khan, S., Saifullah, M. K., Kabir, H., & Jensen, P. K. M. (2022). The Meaning of “Hygiene” and Its Linked Practices in a Low-Income Urban Community in Bangladesh. International Journal of Environmental Research and Public Health, 19(16), 9823. https://doi.org/10.3390/ijerph19169823