
Lowered Quality of Life in Long COVID Is Predicted by Affective Symptoms, Chronic Fatigue Syndrome, Inflammation and Neuroimmunotoxic Pathways


 , and
, and 
Abstract
:1. Introduction
2. Methods
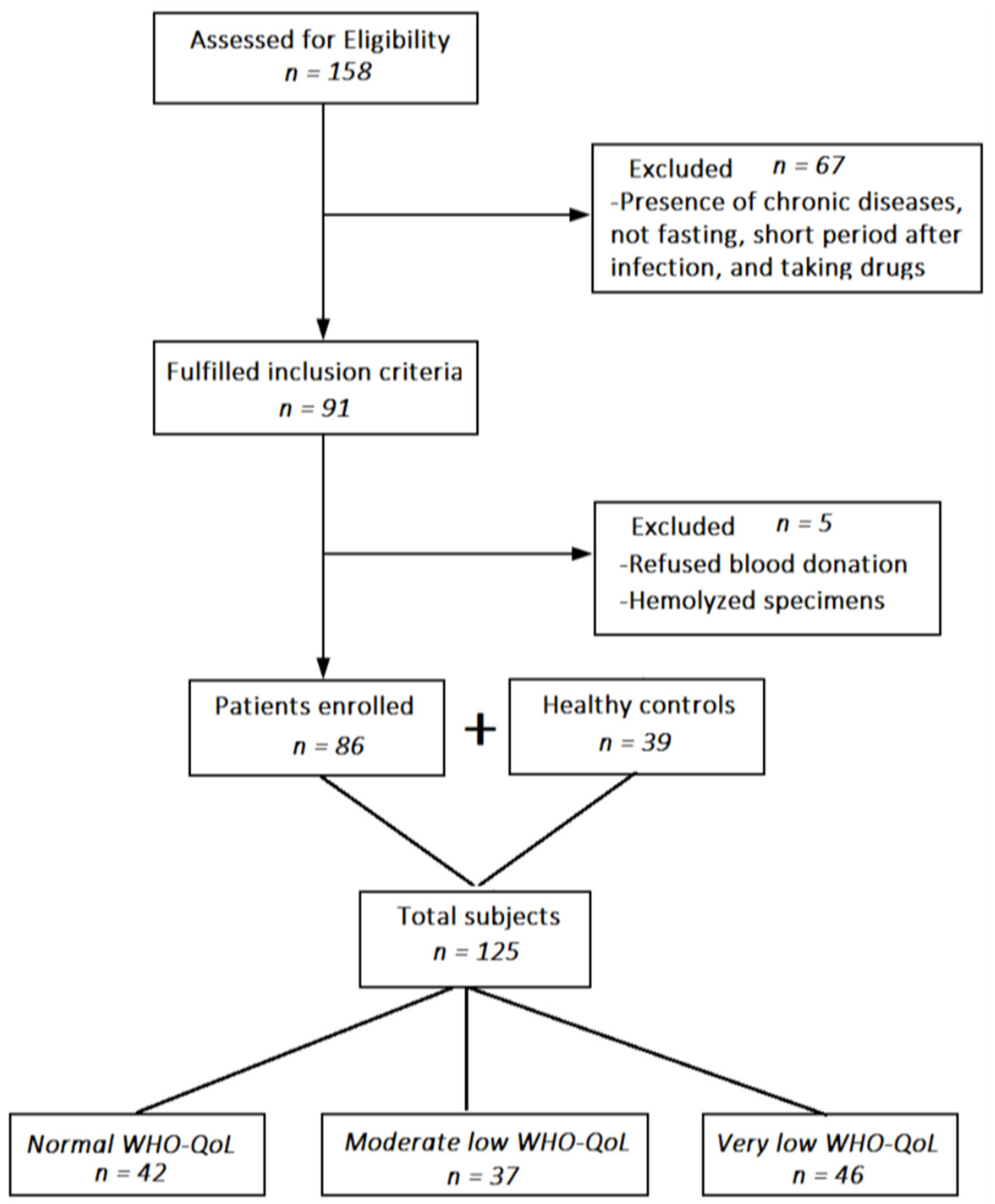
2.1. Participants
2.2. Clinical Assessments
2.3. Biomarker Assessments
2.4. Statistics
2.5. Avoiding Bias
3. Results
3.1. Results of Cluster Analysis
3.2. The Physio-Affective Phenome Scores and Biomarkers in WHO-QoL Clusters
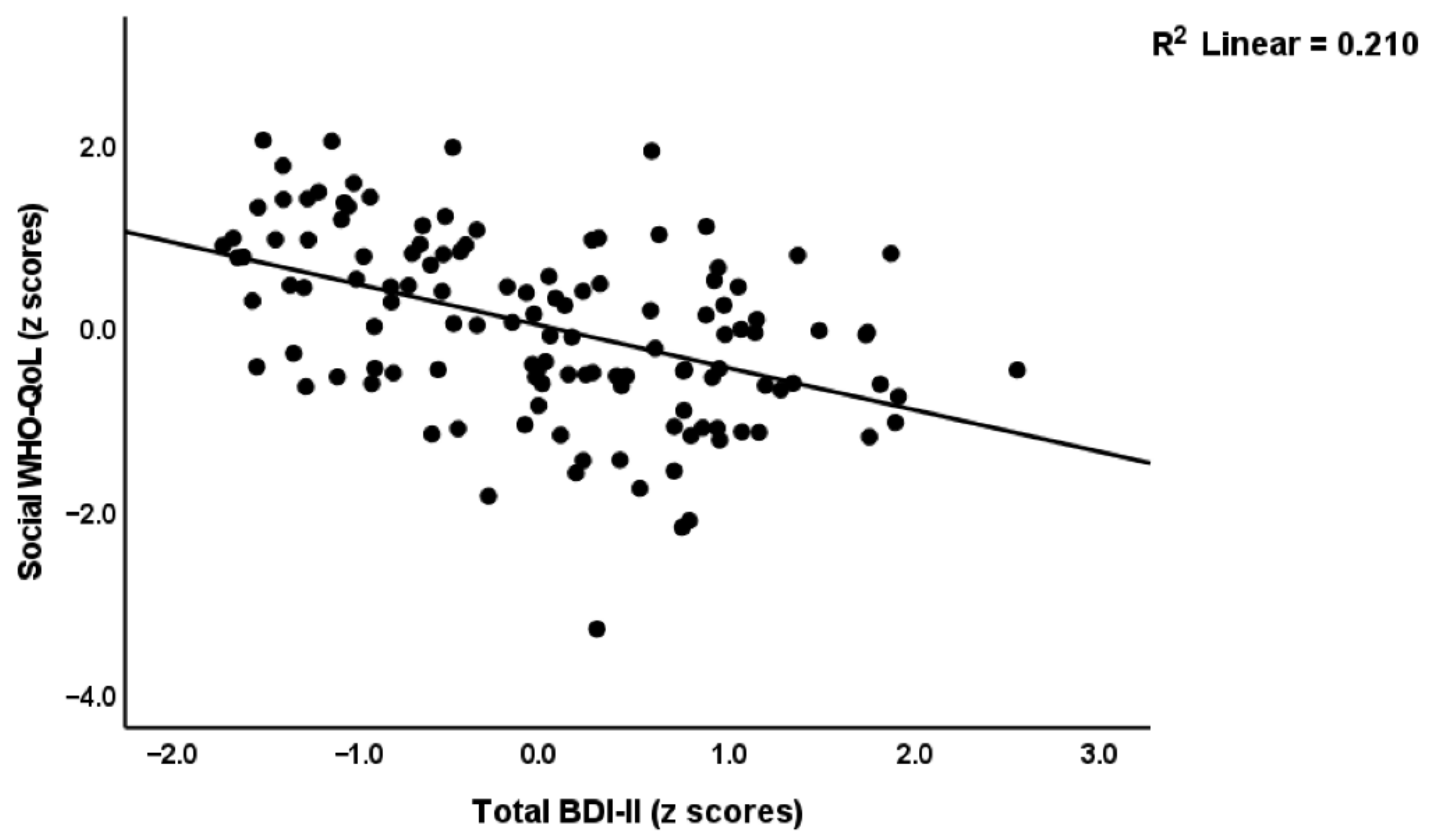
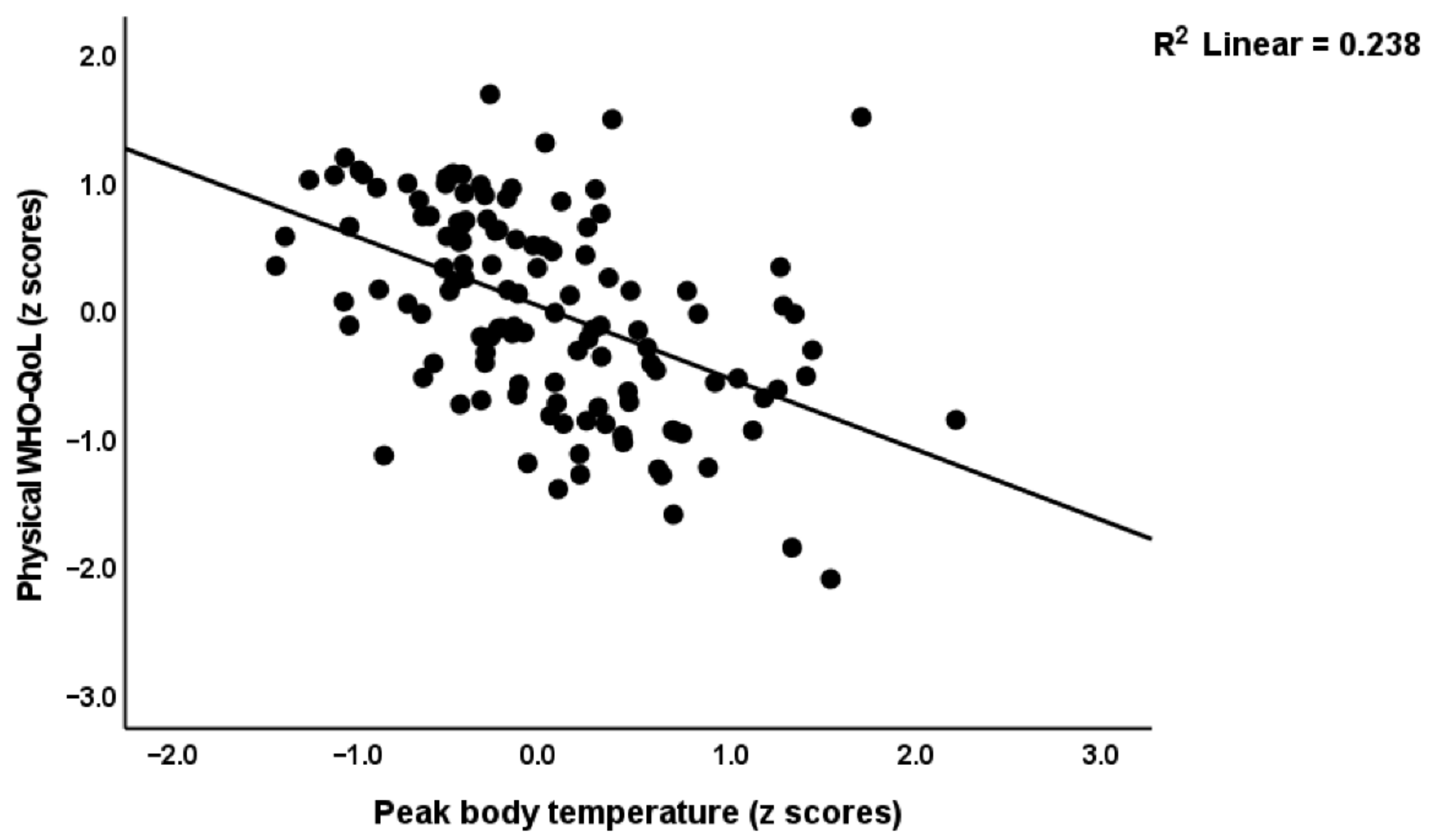
3.3. Associations of the Physio-Affective Phenome with WHO-QoL Scores
3.4. Associations of the Biomarkers with WHO-QoL Scores
4. Discussion
4.1. Lowered HR-Qol in Long COVID
4.2. The Physio-Affective Phenome of Long COVID Predict Lowered HR-QoL
4.3. Lowered HR-Qol in Long COVID Is Predicted by Neuroimmunotoxic and Oxidative Pathways
4.4. The Effects of SARS-CoV-2 Infection on Lowered HR-QoL in Long COVID Are Mediated by Acute and Chronic Immune-Inflammatory Processes
4.5. Additional Explanatory Variables
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bastug, A.; Aslaner, H.; Aybar Bilir, Y.; Kemirtlek, N.; Gursoy, F.M.; Bastug, S.; Bodur, H. Multiple system inflammatory syndrome associated with SARS-CoV-2 infection in an adult and an adolescent. Rheumatol. Int. 2021, 41, 993–1008. [Google Scholar] [CrossRef] [PubMed]
- Vora, S.M.; Lieberman, J.; Wu, H. Inflammasome activation at the crux of severe COVID-19. Nat. Rev. Immunol. 2021, 21, 694–703. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus 6 October 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Badenoch, J.B.; Rengasamy, E.R.; Watson, C.; Jansen, K.; Chakraborty, S.; Sundaram, R.D.; Hafeez, D.; Burchill, E.; Saini, A.; Thomas, L.; et al. Persistent neuropsychiatric symptoms after COVID-19: A systematic review and meta-analysis. Brain Commun. 2021, 4, fcab297. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Al-Rubaye, H.T.; Almulla, A.F.; Al-Hadrawi, D.S.; Maes, M. Chronic fatigue, depression and anxiety symptoms in Long COVID are strongly predicted by neuroimmune and neuro-oxidative pathways which are caused by the inflammation during acute infection. medRxiv 2022. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Al-Rubabaye, H.K.; Al-Hadrawi, D.S.; Almulla, A.F.; Maes, M. Long-COVID post-viral chronic fatigue syndrome and affective symptoms are associated with oxidative damage, lowered antioxidant defenses and inflammation: A proof of concept and mechanism study. medRxiv 2022. [Google Scholar] [CrossRef]
- Renaud-Charest, O.; Lui, L.M.W.; Eskander, S.; Ceban, F.; Ho, R.; Di Vincenzo, J.D.; Rosenblat, J.D.; Lee, Y.; Subramaniapillai, M.; McIntyre, R.S. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J. Psychiatr. Res. 2021, 144, 129–137. [Google Scholar] [CrossRef]
- Titze-de-Almeida, R.; da Cunha, T.R.; Dos Santos Silva, L.D.; Ferreira, C.S.; Silva, C.P.; Ribeiro, A.P.; de Castro Moreira Santos Júnior, A.; de Paula Brandão, P.R.; Silva, A.P.B.; da Rocha, M.C.O.; et al. Persistent, new-onset symptoms and mental health complaints in Long COVID in a Brazilian cohort of non-hospitalized patients. BMC. Infect. Dis. 2022, 22, 133. [Google Scholar] [CrossRef]
- Sandler, C.X.; Wyller, V.B.B.; Moss-Morris, R.; Buchwald, D.; Crawley, E.; Hautvast, J.; Katz, B.Z.; Knoop, H.; Little, P.; Taylor, R.; et al. Long COVID and Post-infective Fatigue Syndrome: A Review. Open Forum Infect. Dis. 2021, 8, ofab440. [Google Scholar] [CrossRef]
- Al-Jassas, H.K.; Al-Hakeim, H.K.; Maes, M. Intersections between pneumonia, lowered oxygen saturation percentage and immune activation mediate depression, anxiety, and chronic fatigue syndrome-like symptoms due to COVID-19: A nomothetic network approach. J. Affect. Disord. 2022, 297, 233–245. [Google Scholar] [CrossRef]
- Al-Hadrawi, D.S.; Al-Rubaye, H.T.; Almulla, A.F.; Al-Hakeim, H.K.; Maes, M. Lowered oxygen saturation and increased body temperature in acute COVID-19 largely predict chronic fatigue syndrome and affective symptoms due to LONG COVID: A precision nomothetic approach. medRxiv 2022. [Google Scholar] [CrossRef]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol. Biol. 2015, 1282, 1–23. [Google Scholar] [CrossRef] [PubMed]
- V’Kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2021, 19, 155–170. [Google Scholar] [CrossRef]
- Tsang, H.F.; Chan, L.W.C.; Cho, W.C.S.; Yu, A.C.S.; Yim, A.K.Y.; Chan, A.K.C.; Ng, L.P.W.; Wong, Y.K.E.; Pei, X.M.; Li, M.J.W.; et al. An update on COVID-19 pandemic: The epidemiology, pathogenesis, prevention and treatment strategies. Expert Rev. Anti Infect. Ther. 2021, 19, 877–888. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Sagulkoo, P.; Plaimas, K.; Suratanee, A.; Colado Simão, A.N.; Vissoci Reiche, E.M.; Maes, M. Immunopathogenesis and immunogenetic variants in COVID-19. Curr. Pharm. Des. 2022. [Google Scholar] [CrossRef] [PubMed]
- Yalcinkaya, M.; Liu, W.; Islam, M.N.; Kotini, A.G.; Gusarova, G.A.; Fidler, T.P.; Papapetrou, E.P.; Bhattacharya, J.; Wang, N.; Tall, A.R. Modulation of the NLRP3 inflammasome by SARS-CoV-2 Envelope protein. Sci. Rep. 2021, 11, 24432. [Google Scholar] [CrossRef]
- Maes, M.; Tedesco Junior, W.L.D.; Lozovoy, M.A.B.; Mori, M.T.E.; Danelli, T.; Almeida, E.R.D.; Tejo, A.M.; Tano, Z.N.; Reiche, E.M.V.; Simão, A.N.C. In COVID-19, NLRP3 inflammasome genetic variants are associated with critical disease and these effects are partly mediated by the sickness symptom complex: A nomothetic network approach. Mol. Psychiatry 2022, 27, 1945–1955. [Google Scholar] [CrossRef]
- Zhao, N.; Di, B.; Xu, L.-L. The NLRP3 inflammasome and COVID-19: Activation, pathogenesis and therapeutic strategies. Cytokine Growth Factor Rev. 2021, 61, 2–15. [Google Scholar] [CrossRef]
- Tharakan, S.; Nomoto, K.; Miyashita, S.; Ishikawa, K. Body temperature correlates with mortality in COVID-19 patients. Crit Care 2020, 24, 298. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.H.; Stoyanov, D. False dogmas in mood disorders research: Towards a nomothetic network approach. World J. Psychiatry 2022, 12, 651–667. [Google Scholar] [CrossRef] [PubMed]
- Maes, M. Precision Nomothetic Medicine in Depression Research: A New Depression Model, and New Endophenotype Classes and Pathway Phenotypes, and A Digital Self. J. Pers. Med. 2022, 12, 403. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Kubera, M.; Kotańska, M. Aberrations in the Cross-Talks Among Redox, Nuclear Factor-κB, and Wnt/β-Catenin Pathway Signaling Underpin Myalgic Encephalomyelitis and Chronic Fatigue Syndrome. Front. Psychiatry 2022, 13, 822382. [Google Scholar] [CrossRef]
- Muñoz-Corona, C.; Gutiérrez-Canales, L.G.; Ortiz-Ledesma, C.; Martínez-Navarro, L.J.; Macías, A.E.; Scavo-Montes, D.A.; Guaní-Guerra, E. Quality of life and persistence of COVID-19 symptoms 90 days after hospital discharge. J. Int. Med. Res. 2022, 50, 3000605221110492. [Google Scholar] [CrossRef]
- Case, K.R.; Wang, C.P.; Hosek, M.G.; Lill, S.F.; Howell, A.B.; Taylor, B.S.; Bridges, J.; MacCarthy, D.J.; Winkler, P.; Tsevat, J. Health-related quality of life and social determinants of health following COVID-19 infection in a predominantly Latino population. J. Patient Rep. Outcomes 2022, 6, 72. [Google Scholar] [CrossRef]
- Malik, P.; Patel, K.; Pinto, C.; Jaiswal, R.; Tirupathi, R.; Pillai, S.; Patel, U. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)-A systematic review and meta-analysis. J. Med. Virol. 2022, 94, 253–262. [Google Scholar] [CrossRef]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O’Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising long COVID: A living systematic review. BMJ Glob. Health 2021, 6, e005427. [Google Scholar] [CrossRef]
- Nandasena, H.M.R.K.G.; Pathirathna, M.L.; Atapattu, A.M.M.P.; Prasanga, P.T.S. Quality of life of COVID 19 patients after discharge: Systematic review. PLoS ONE 2022, 17, e0263941. [Google Scholar] [CrossRef]
- Maes, M.; Vojdani, A.; Galecki, P.; Kanchanatawan, B. How to Construct a Bottom-Up Nomothetic Network Model and Disclose Novel Nosological Classes by Integrating Risk Resilience and Adverse Outcome Pathways with the Phenome of Schizophrenia. Brain Sci. 2020, 10, 645. [Google Scholar] [CrossRef]
- Maes, M.; Kanchanatawan, B. In (deficit) schizophrenia, a general cognitive decline partly mediates the effects of neuro-immune and neuro-oxidative toxicity on the symptomatome and quality of life. CNS Spectr. 2021, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Vojdani, A.; Sirivichayakul, S.; Barbosa, D.S.; Kanchanatawan, B. Inflammatory and Oxidative Pathways Are New Drug Targets in Multiple Episode Schizophrenia and Leaky Gut, Klebsiella pneumoniae, and C1q Immune Complexes Are Additional Drug Targets in First Episode Schizophrenia. Mol. Neurobiol. 2021, 58, 3319–3334. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- World Health Organization. WHOQOL: Measuring Quality of Life; The World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck Depression Inventory–II (BDI-II) [Database Record]. APA PsycTests 1996. [Google Scholar] [CrossRef]
- Zachrisson, O.; Regland, B.; Jahreskog, M.; Kron, M.; Gottfries, C.G. A rating scale for fibromyalgia and chronic fatigue syndrome (the FibroFatigue scale). J. Psychosom. Res. 2002, 52, 501–509. [Google Scholar] [CrossRef]
- Hamilton, M. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Nunes, C.S.; Maes, M.; Roomruangwong, C.; Moraes, J.B.; Bonifacio, K.L.; Vargas, H.O.; Barbosa, D.S.; Anderson, G.; de Melo, L.G.P.; Drozdstoj, S.; et al. Lowered quality of life in mood disorders is associated with increased neuro-oxidative stress and basal thyroid-stimulating hormone levels and use of anticonvulsant mood stabilizers. J. Eval. Clin. Pract. 2018, 24, 869–878. [Google Scholar] [CrossRef]
- Cavicchioli, F.L.; Maes, M.; Roomruangwong, C.; Bonifacio, K.L.; Barbosa, D.S.; Anderson, G.; Vargas, H.O.; Nunes, S.O.V. Associations between severity of anxiety and clinical and biological features of major affective disorders. Psychiatry Res. 2018, 260, 17–23. [Google Scholar] [CrossRef]
- Kanchanatawan, B.; Sriswasdi, S.; Maes, M. Supervised machine learning to decipher the complex associations between neuro-immune biomarkers and quality of life in schizophrenia. Metab. Brain Dis. 2019, 34, 267–282. [Google Scholar] [CrossRef]
- Al-Musawi, A.F.; Al-Hakeim, H.K.; Al-Khfaji, Z.A.; Al-Haboby, I.H.; Almulla, A.F.; Maes, M. In schizophrenia, the effects of the IL-6/IL-23/Th17 axis on health-related quality of life and disabilities are partly mediated by generalized cognitive decline and the symptomatome. medRxiv 2022. [Google Scholar] [CrossRef]
- Sirivichayakul, S.; Kanchanatawan, B.; Thika, S.; Carvalho, A.F.; Maes, M. A New Schizophrenia Model: Immune Activation is Associated with the Induction of Different Neurotoxic Products which Together Determine Memory Impairments and Schizophrenia Symptom Dimensions. CNS Neurol. Disord. Drug Targets 2019, 18, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Moraes, J.B.; Congio, A.; Bonifacio, K.L.; Barbosa, D.S.; Vargas, H.O.; Michelin, A.P.; Carvalho, A.F.; Nunes, S.O.V. Development of a Novel Staging Model for Affective Disorders Using Partial Least Squares Bootstrapping: Effects of Lipid-Associated Antioxidant Defenses and Neuro-Oxidative Stress. Mol. Neurobiol. 2019, 56, 6626–6644. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Moraes, J.B.; Bonifacio, K.L.; Barbosa, D.S.; Vargas, H.O.; Michelin, A.P.; Nunes, S.O.V. Towards a new model and classification of mood disorders based on risk resilience, neuro-affective toxicity, staging, and phenome features using the nomothetic network psychiatry approach. Metab. Brain Dis. 2021, 36, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Kubera, M.; Stoyanova, K.; Leunis, J.C. The Reification of the Clinical Diagnosis of Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome (ME/CFS) as an Immune and Oxidative Stress Disorder: Construction of a Data-driven Nomothethic Network and Exposure of ME/CFS Subgroups. Curr. Top. Med. Chem. 2021, 21, 1488–1499. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Al-Naqeeb, T.H.; Almulla, A.F.; Maes, M. The physio-affective phenome of major depression is strongly associated with biomarkers of astroglial and neuronal projection toxicity which in turn are associated with peripheral inflammation, insulin resistance and lowered calcium. medRxiv 2022. [Google Scholar] [CrossRef]
- Mousa, R.F.; Smesam, H.N.; Qazmooz, H.A.; Al-Hakeim, H.K.; Maes, M. A pathway phenotype linking metabolic, immune, oxidative, and opioid pathways with comorbid depression, atherosclerosis, and unstable angina. CNS Spectr. 2021, 27, 1–15. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Hadi, H.H.; Jawad, G.A.; Maes, M. Intersections between Copper, β-Arrestin-1, Calcium, FBXW7, CD17, Insulin Resistance and Atherogenicity Mediate Depression and Anxiety Due to Type 2 Diabetes Mellitus: A Nomothetic Network Approach. J. Pers. Med. 2022, 12, 23. [Google Scholar] [CrossRef]
- Fong, J.; Khan, A. Hypocalcemia: Updates in diagnosis and management for primary care. Can. Fam. Physician 2012, 58, 158–162. [Google Scholar]
- Bove-Fenderson, E.; Mannstadt, M. Hypocalcemic disorders. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 639–656. [Google Scholar] [CrossRef]
- Lewis, J.L. Hypercalcemia (High Level of Calcium in the Blood)—Hormonal and Metabolic Disorders—MSD Manual Consumer Version. Content last modified October 2021. Available online: https://www.msdmanuals.com/ (accessed on 22 July 2022).
- Alemzadeh, E.; Alemzadeh, E.; Ziaee, M.; Abedi, A.; Salehiniya, H. The effect of low serum calcium level on the severity and mortality of COVID patients: A systematic review and meta-analysis. Immun. Inflamm. Dis. 2021, 9, 1219–1228. [Google Scholar] [CrossRef]
- Faro, M.; Sàez-Francás, N.; Castro-Marrero, J.; Aliste, L.; Fernández de Sevilla, T.; Alegre, J. Gender differences in chronic fatigue syndrome. Reumatol. Clin. 2016, 12, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Noble, R.E. Depression in women. Metabolism 2005, 54 (Suppl. S1), 49–52. [Google Scholar] [CrossRef] [PubMed]
- Somers, J.M.; Goldner, E.M.; Waraich, P.; Hsu, L. Prevalence and incidence studies of anxiety disorders: A systematic review of the literature. Can. J. Psychiatry 2006, 51, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Songtachalert, T.; Roomruangwong, C.; Carvalho, A.F.; Bourin, M.; Maes, M. Anxiety Disorders: Sex Differences in Serotonin and Tryptophan Metabolism. Curr. Top. Med. Chem. 2018, 18, 1704–1715. [Google Scholar] [CrossRef] [PubMed]
- Almulla, A.F.; Supasitthumrong, T.; Tunvirachaisakul, C.; Algon, A.A.A.; Al-Hakeim, H.K.; Maes, M. The tryptophan catabolite or kynurenine pathway in COVID-19 and critical COVID-19: A systematic review and meta-analysis. BMC Infect. Dis. 2022, 22, 615. [Google Scholar] [CrossRef]
- Couzin-Frankel, J.; Vogel, G. Vaccines may cause rare, Long COVID-like symptoms. Science 2022, 375, 364–366. [Google Scholar] [CrossRef]
- Seneff, S.; Nigh, G.; Kyriakopoulos, A.M.; McCullough, P.A. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes, and MicroRNAs. Food Chem. Toxicol. 2022, 164, 113008. [Google Scholar] [CrossRef]
- Keskin, I.; Gunal, M.Y.; Ayturk, N.; Kilic, U.; Ozansoy, M.; Kilic, E. Dose-dependent neuroprotective effect of enoxaparin on cold-induced traumatic brain injury. Neural Regen. Res. 2017, 12, 761–764. [Google Scholar] [CrossRef]
- Cardillo, G.; Viggiano, G.V.; Russo, V.; Mangiacapra, S.; Cavalli, A.; Castaldo, G.; Agrusta, F.; Bellizzi, A.; Amitrano, M.; Iannuzzo, M.; et al. Antithrombotic and Anti-Inflammatory Effects of Fondaparinux and Enoxaparin in Hospitalized COVID-19 Patients: The Fondenoxavid Study. J. Blood. Med. 2021, 12, 69–75. [Google Scholar] [CrossRef]
- Stutzmann, J.M.; Mary, V.; Wahl, F.; Grosjean-Piot, O.; Uzan, A.; Pratt, J. Neuroprotective profile of enoxaparin, a low molecular weight heparin, in in vivo models of cerebral ischemia or traumatic brain injury in rats: A review. CNS Drug Rev. 2002, 8, 1–30. [Google Scholar] [CrossRef]
- Shastri, M.D.; Stewart, N.; Horne, J.; Zaidi, S.T.; Sohal, S.S.; Peterson, G.M.; Korner, H.; Gueven, N.; Patel, R.P. Non-Anticoagulant Fractions of Enoxaparin Suppress Inflammatory Cytokine Release from Peripheral Blood Mononuclear Cells of Allergic Asthmatic Individuals. PLoS ONE 2015, 10, e0128803. [Google Scholar] [CrossRef] [PubMed]
- Dos Reis Louzano, A.S.; de Moura, E.; Dias, M.; Lopes da Conceição, L.; Antônio de Oliveira Mendes, T.; Gouveia Peluzio, M.D.C. Ceftriaxone causes dysbiosis and changes intestinal structure in adjuvant obesity treatment. Pharmacol. Rep. 2022, 74, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Scharpé, S.; De Meester, I.; Goossens, P.; Wauters, A.; Neels, H.; Verkerk, R.; De Meyer, F.; D’Hondt, P.; Peeters, D.; et al. Components of biological variation in prolyl endopeptidase and dipeptidyl-peptidase IV activity in plasma of healthy subjects. Clin. Chem. 1994, 40, 1686–1691. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Normal WHO-QoL A n = 42 | Moderate Low WHO-QoL B n = 37 | Very Low WHO-QoL C n = 46 | F/χ2 | df | p |
|---|---|---|---|---|---|---|
| WHO-QoL, physical * | 27.46 ± 0.66 B,C | 21.60 ± 0.51 A,C | 16.83 ± 0.49 A,B | 66.83 | 2/114 | <0.001 |
| WHO-QoL, psychological * | 25.70 ± 0.57 B,C | 21.40 ± 0.43 A,C | 16.43 ± 0.42 A,B | 77.50 | 2/114 | <0.001 |
| WHO-QoL, social * | 11.92 ± 0.43 | 10.58 ± 0.33 | 10.56 ± 0.32 | 2.50 | 2/114 | 0.086 |
| WHO-QoL, environment * | 33.60 ± 0.71 B,C | 26.78 ± 0.54 A,C | 22.89 ± 0.53 A,B | 54.03 | 2/114 | <0.001 |
| PC 4 WHO-QoL domains * | 1.121 ± 0.087 | −0.124 ± 0.066 | −0.924 ± 0.064 | 135.31 | 2/114 | <0.001 |
| HC/Long COVID | 38/4 | 1/36 | 0/46 | FFHE | <0.001 | |
| Age (years) | 28.0 ± 7.4 | 29.3 ± 6.5 | 27.9 ± 5.9 | 0.35 | 2/127 | 0.706 |
| Female/Male ratio | 19/23 | 15/22 | 20/26 | 0.18 | 2 | 0.914 |
| BMI (kg/m2) | 25.84 ± 4.08 | 25.83 ± 3.53 | 26.21 ± 5.23 | 0.05 | 2/127 | 0.950 |
| Education (years) | 15.0 ±1.2 B,C | 15.8 ± 1.9 A,C | 15.6 ± 1.7 A,B | 9.99 | 2/127 | <0.001 |
| Married/Single (No/Yes) | 19/23 | 21/31 | 15/21 | 0.23 | 2 | 0.901 |
| Rural/Urban (No/Yes) | 8/34 | 8/29 | 7/39 | 0.58 | 2 | 0.749 |
| TUD (No/Yes) | 29/13 | 24/13 | 32/14 | 2.40 | 2 | 0.887 |
| Vaccination A/Pf/S | 9/23/10 | 5/23/9 | 15/23/8 | 4.46 | 4 | 0.347 |
| Dexamethasone (No/Yes) | 39/3 | 24/13 | 23/23 | 19.17 | 2 | <0.001 |
| Ceftriaxone (No/Yes) | 41/1 | 18/19 | 16/30 | 38.94 | 2 | <0.001 |
| Azithromycine (No/Yes) | 38/4 | 17/20 | 25/21 | 19.87 | 2 | <0.001 |
| Enoxaparin sodium (No/Yes) | 38/4 | 4/33 | 8/38 | 67.52 | 2 | <0.001 |
| Bromhexine (No/Yes) | 39/3 | 10/27 | 8/38 | 57.71 | 2 | <0.001 |
| Variables | Normal WHO-QoL A n = 42 | Moderate Lower WHO-QoL B n = 52 | Very Low WHO-QoL C n = 36 | F (df = 2/122) | p |
|---|---|---|---|---|---|
| Total FF score | 11.0 ± 4.1 B,C | 20.4 ± 10.1 A,C | 36.0 ± 12.1 A,B | 78.42 | <0.001 |
| Total HAMA score | 7.9 ± 3.9 B,C | 13.8 ± 6.6 A,C | 19.7 ± 8.5 A,B | 34.26 | <0.001 |
| Total BDI-II score | 9.1 ± 4.1 B,C | 20.3 ± 5.8 A,C | 28.9 ± 6.4 A,B | 140.46 | <0.001 |
| Total HAMD score | 6.4 ± 3.7 B,C | 14.5 ± 4.8 A,C | 18.8 ± 4.5 A,B | 90.23 | <0.001 |
| Pure FF | −0.867 ± 0.385 B,C | −0.079 ± 0.746 A,C | 0.855 ± 0.849 A,B | 68.31 | <0.001 |
| Pure HAMD | −0.987 ± 0.395 B,C | 0.136 ± 0.636 A,C | 0.792 ± 0.851 A,B | 80.21 | <0.001 |
| Physiosom HMD | −0.862 ± 0.672 B,C | 0.247 ± 0.949 A,C | 0.588 ± 0.726 A,B | 40.35 | <0.001 |
| Pure HAMA | −0.547 ± 0.766 B,C | −0.084 ± 0.853 A,C | 0.568 ± 1.012 A,B | 17.53 | <0.001 |
| Physiosom HAMA | −0.517 ± 0.564 B,C | 0.002 ± 0.958 A | 0.470 ± 1.120 A | 12.73 | <0.001 |
| Pure BDI | −0.998 ± 0.605 B,C | 0.209 ± 0.663 A,C | 0.743 ± 0.735 A,B | 76.11 | <0.001 |
| PC Physio-affective phenome | −0.963 ± 0.368 B,C | 0.0498 ± 0.706 A,C | 0.839 ± 0.804 A,B | 82.90 | <0.001 |
| Peak body temperature | 37.07 (0.78) B,C | 38.30 (0.74) A,C | 38.75 (0.93) A,B | 47.85 | <0.001 |
| Lowest SpO2 (%) | 94.86 ± 1.96 B,C | 91.62 ± 3.59 A | 90.37 ± 4.29 A | 19.46 | <0.001 |
| TO2 index (zBT-zSpO2 in z scores) | −0.880 ± 0.586 B,C | 0.218 ± 0.759 A,C | 0.628 ± 0.903 A,B | 44.71 | <0.001 |
| NLRP3 (z scores) | −0.406 ± 0.945 B,C | 0.030 ± 0.833 A | 0.347 ± 1.052 A | 6.85 | 0.002 |
| OSTOX (z scores) | −0.380 ± 1.018 B,C | 0.140 ± 0.478 A | 0.269 ± 1.057 A | 5.45 | 0.005 |
| OSTOX+NLRP3 (z scores) | −0.527 ± 0.880 B,C | 0.088 ± 0.794 A,C | 0.492 ± 0.905 A,B | 15.23 | <0.001 |
| zIR (z scores) | −0.426 ± 0.678 B,C | 0.307 ± 1.112 A | 0.142 ± 1.040 A | 6.57 | 0.002 |
| OSTOX+NLRP3+IR (NT) | −0.625 ± 0.892 B,C | 0.188 ± 0.741 A | 0.419 ± 1.010 A | 16.04 | <0.001 |
| NT+TO2 (z scores) | −0.857 ± 0.795 B,C | 0.240 ± 0.677 A,C | 0.589 ± 0.851 A,B | 39.76 | <0.001 |
| Dependent Variables | Explanatory Variables | B | t | p | F Model | df | p | R2 |
|---|---|---|---|---|---|---|---|---|
| PC_WHO-QoL domains | Model#1 | 132.74 | 2/121 | <0.001 | 0.767 | |||
| Pure BDI | −0.476 | −6.96 | <0.001 | |||||
| Pure FF | −0.292 | −5.04 | <0.001 | |||||
| Total HAMD | −0.238 | −3.02 | 0.003 | |||||
| WHO-QoL physical | Model#2 | 90.00 | 3/120 | <0.001 | 0.750 | |||
| Pure FF | −0.523 | −8.63 | <0.001 | |||||
| Pure BDI | −0.254 | −3.56 | <0.001 | |||||
| Sex | −0.125 | −2.72 | 0.007 | |||||
| Total HAMD | −0.221 | −2.69 | 0.008 | |||||
| WHO-QoL psychological | Model#3 | 133.17 | 2/122 | <0.001 | 0.686 | |||
| Pure BDI | −0.619 | −10.41 | <0.001 | |||||
| Total FF | −0.316 | −5.31 | <0.001 | |||||
| WHO-QoL social | Model#4 | 24.61 | 1/123 | <0.001 | 0.167 | |||
| Total HAMD | −0.408 | −4.96 | <0.001 | |||||
| WHO-QoL environmental | Model#5 | 85.53 | 2/122 | <0.001 | 0.584 | |||
| Pure BDI | −0.586 | −8.78 | <0.001 | |||||
| Pure FF | −0.283 | −4.24 | <0.001 | |||||
| Dependent Variables | Explanatory Variables | B | t | p | F Model | df | p | R2 |
|---|---|---|---|---|---|---|---|---|
| PC_WHO-QoL domains | Model#1 | 57.47 | 3/120 | <0.001 | 0.590 | |||
| PBT | −0.290 | −3.02 | 0.003 | |||||
| Calcium | 0.302 | 4.57 | <0.001 | |||||
| NT+TO2 | −0.329 | −3.56 | <0.001 | |||||
| WHO-QoL physical | Model#2 | 54.93 | 3/120 | <0.001 | 0.579 | |||
| PBT | −0.465 | −6.22 | <0.001 | |||||
| Calcium | 0.256 | 3.82 | <0.001 | |||||
| NT | −0.241 | −3.58 | <0.001 | |||||
| WHO-QoL psychological | Model#3 | 40.13 | 2/121 | <0.001 | 0.399 | |||
| NT+TO2 | −0.446 | −5.83 | <0.001 | |||||
| Calcium | 0.305 | 3.99 | <0.001 | |||||
| WHO-QoL social | Model#4 | 21.33 | 2/121 | <0.001 | 0.261 | |||
| Calcium | 0.401 | 5.04 | <0.001 | |||||
| NT | −0.251 | −3.16 | 0.002 | |||||
| WHO-QoL environmental | Model#5 | 37.87 | 3/120 | <0.001 | 0.486 | |||
| PBT | −0.276 | −2.57 | 0.011 | |||||
| Calcium | 0.288 | 3.89 | <0.001 | |||||
| NT+TO2 | −0.274 | −2.65 | 0.009 | |||||
| PC phenome | Model#6 | 47.71 | 4/119 | <0.001 | 0.616 | |||
| PBT | 0.480 | 6.70 | <0.001 | |||||
| Calcium | −0.266 | −4.13 | <0.001 | |||||
| Female sex | −0.206 | −3.61 | <0.001 | |||||
| NT | 0.223 | 3.45 | <0.001 | |||||
| Dependent Variables | Explanatory Variables | B | t | p | F Model | df | p | R2 |
|---|---|---|---|---|---|---|---|---|
| PC_WHO-QoL 4 domains | Model#1 | 167.94 | 4/120 | <0.001 | 0.848 | |||
| Acute infection | −0.644 | −8.50 | <0.001 | |||||
| Pure BDI | −0.354 | −6.95 | <0.001 | |||||
| Pure FF | −0.274 | −6.10 | <0.001 | |||||
| Enoxaparin | 0.262 | 4.08 | <0.001 | |||||
| WHO-QoL physical | Model#2 | 65.39 | 4/120 | <0.001 | 0.686 | |||
| Acute infection | −0.525 | −6.49 | <0.001 | |||||
| PBT | −0.238 | −3.16 | 0.002 | |||||
| Ceftriaxone | −0.165 | −2.68 | 0.008 | |||||
| Vaccination A | −0.103 | −2.00 | 0.048 | |||||
| WHO-QoL environmental | Model#3 | 89.82 | 2/122 | <0.001 | 0.596 | |||
| Acute infection | −1.054 | −10.35 | <0.001 | |||||
| Enoxaparin | 0.379 | 3.72 | <0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maes, M.; Al-Rubaye, H.T.; Almulla, A.F.; Al-Hadrawi, D.S.; Stoyanova, K.; Kubera, M.; Al-Hakeim, H.K. Lowered Quality of Life in Long COVID Is Predicted by Affective Symptoms, Chronic Fatigue Syndrome, Inflammation and Neuroimmunotoxic Pathways. Int. J. Environ. Res. Public Health 2022, 19, 10362. https://doi.org/10.3390/ijerph191610362
Maes M, Al-Rubaye HT, Almulla AF, Al-Hadrawi DS, Stoyanova K, Kubera M, Al-Hakeim HK. Lowered Quality of Life in Long COVID Is Predicted by Affective Symptoms, Chronic Fatigue Syndrome, Inflammation and Neuroimmunotoxic Pathways. International Journal of Environmental Research and Public Health. 2022; 19(16):10362. https://doi.org/10.3390/ijerph191610362
Chicago/Turabian StyleMaes, Michael, Haneen Tahseen Al-Rubaye, Abbas F. Almulla, Dhurgham Shihab Al-Hadrawi, Kristina Stoyanova, Marta Kubera, and Hussein Kadhem Al-Hakeim. 2022. "Lowered Quality of Life in Long COVID Is Predicted by Affective Symptoms, Chronic Fatigue Syndrome, Inflammation and Neuroimmunotoxic Pathways" International Journal of Environmental Research and Public Health 19, no. 16: 10362. https://doi.org/10.3390/ijerph191610362
APA StyleMaes, M., Al-Rubaye, H. T., Almulla, A. F., Al-Hadrawi, D. S., Stoyanova, K., Kubera, M., & Al-Hakeim, H. K. (2022). Lowered Quality of Life in Long COVID Is Predicted by Affective Symptoms, Chronic Fatigue Syndrome, Inflammation and Neuroimmunotoxic Pathways. International Journal of Environmental Research and Public Health, 19(16), 10362. https://doi.org/10.3390/ijerph191610362