
Refugee Camps as Torturing Environments—An Analysis of the Conditions in the Moria Reception Center (Greece) Based on the Torturing Environment Scale

Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Torturing Environment
2.1.2. Interpersonal Violence
2.1.3. Emotional Distress
2.1.4. Legal Safeguards
2.2. Ethical Aspects
3. Results
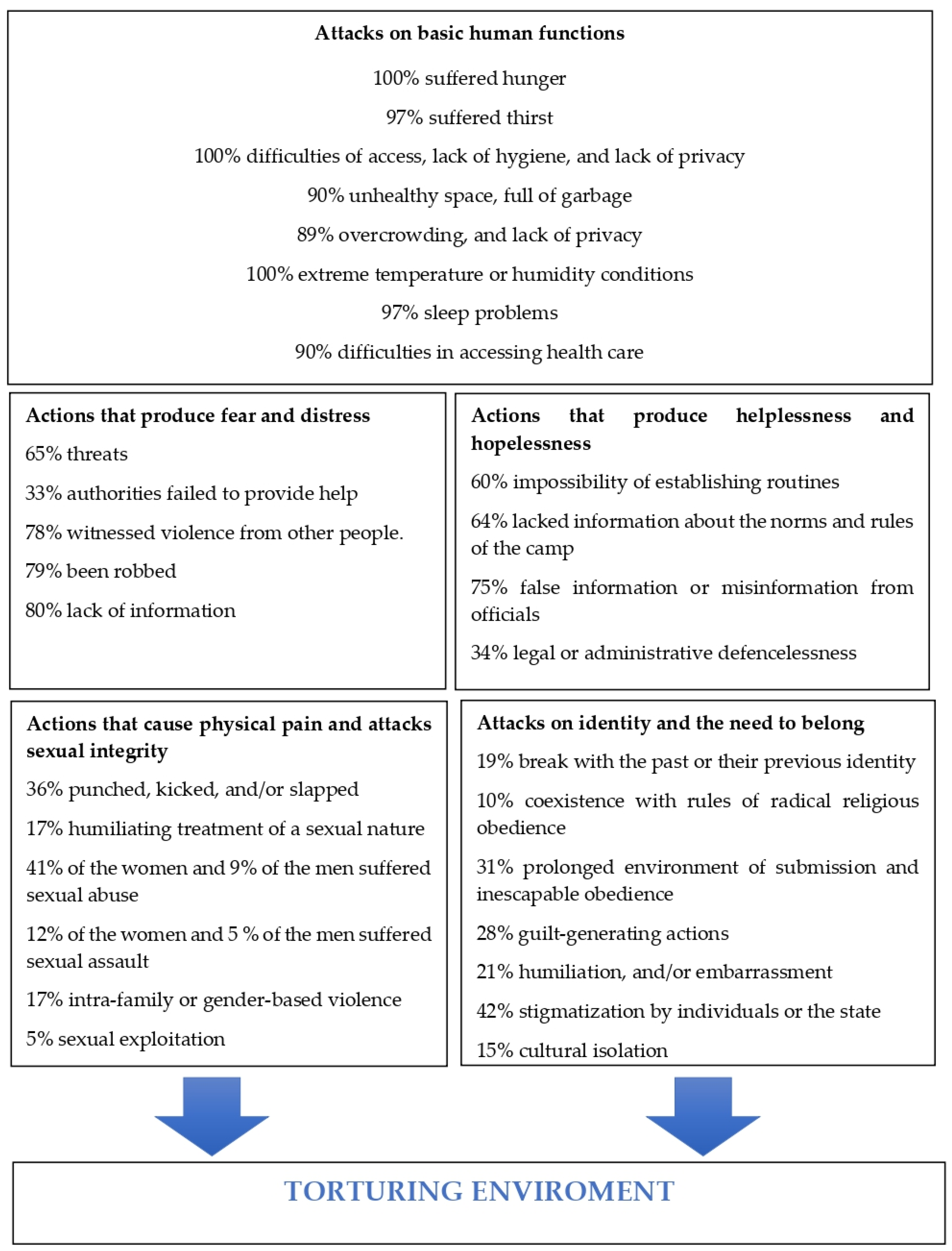
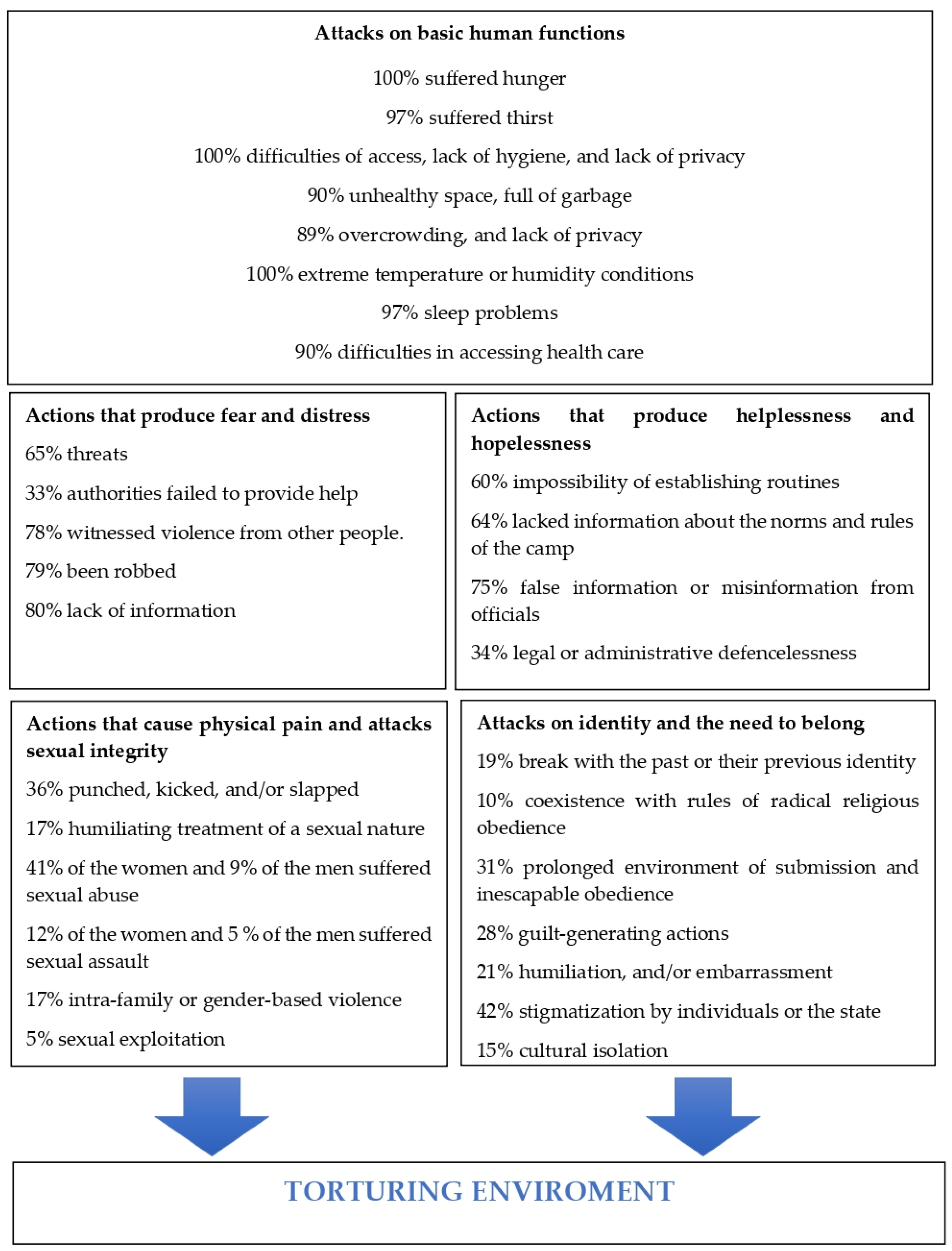
3.1. Attacks on Basic Human Functions
3.2. Actions That Produce Fear and Distress
3.3. Actions That Produce Helplessness and Hopelessness
3.4. Actions That Cause Physical Pain
3.5. Attacks on Sexual Integrity
3.6. Attacks on Identity and the Need to Belong
3.7. Impact on Mental Health
3.8. Legal Safeguards
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- -
- Mark column NO: When it is possible to reasonably state that the indicator designated by the item has not happened to the person.
- -
- Mark column L-C (Limited-Circumstantial): When the indicator is present, albeit in a limited or circumstantial manner. The marker has eventually appeared but is not part of a systematic attack or strategy or one of the nuclear techniques used in the case.
- -
- Mark the YES column: When there is a clear and consistent presence of the indicator.
| Block 1. Attacks on Basic Human Functions | NO | L-C | YES | I | ||
| 1. | Starvation, torture by hunger 1 □ Insufficient food (less than 1000 calories/day, check L-C; less than 500 calories/day, check Yes) ☐ Less than three mealtimes ☐ Unhealthy/Bad quality ☐ Lack of specific nutrition (babies, specific medical needs) ☐ Waiting lines of more than one hour to receive the meal ☐ If food is dependent on the person, lack of resources to buy or obtain it | |||||
| 2. | Restriction of urination, defecation, or hygiene 1 ☐ Access prohibited, arbitrary, or used as a form of punishment or pressure ☐ Dirt—extreme unhealthiness ☐ Difficulty of access to the toilets (distance over 1 km or risk of attack or aggression on the way...) ☐ Overcrowding ☐ Lack of privacy shower/toilet—security-intimacy ☐ Absence of elementary hygiene products (soap, sanitary towels...) ☐ Lack of replacement clothing/inability to wash | |||||
| 3. | Dehydration or torture by thirst 1 ☐ Insufficient water (less than 2 L/person/day, mark L-C; less than 1 L/person/day mark Yes) ☐ Difficulty of access to water point (distance over 1 km, risk of attack or aggression on the way...) or less than one water point (tap) per 500 people | |||||
| 4. | Induction of disease by exposure, intoxication, or inoculation
| |||||
| 5. | Habitability conditions 1: ☐ In detention, less than 4 m2 in individual cells, less than 3 m2 in group cells, less than 2 m2 in camp areas
| |||||
| 6. | Exposure to extreme temperature or humidity conditions (with no possibility of protection against them): ☐ Cold. ☐ Heat. ☐ Humidity—Moisture. ☐ Water leak due to rain without any protection possible. | |||||
| 7. | Sleep deprivation (LC: On average less than 6 h of uninterrupted daily sleep, yes: average less than 4 h): ☐ Primary deprivation (intentional—deliberate actions to prevent or interrupt sleep, such as nighttime rounds, interrogations, music, or sounds intended to break sleep) ☐ Secondary or incidental deprivation (not clearly intentional—resulting from the conditions of detention: absence of bed, mattress, blankets in insanitary conditions, incidental shouting or shooting at night...) | |||||
| 8. | Refusing medical treatment: ☐ Analgesia in severe pain. ☐ Necessary treatments for survival (e.g., insulin) ☐ Necessary treatments for alcohol/drug abstinence ☐ Psychiatric or psychological treatment requested and denied in serious mental disorder, including suicide ☐ Access to urgent health care | |||||
| Block 3. Actions Producing Extreme Fear—Anguish | NO | L-C | YES | I | ||
| 1. | Direct or indirect threats against the person to inflict, repeat, or increase acts of torture or death. | |||||
| 2. | Threats against relatives, friends, or acquaintances or threats against other detainees (e.g., rape, detention, punishment, reprisals).
| |||||
| 3. | Situations of perceived imminent death (e.g., mock executions). | |||||
| 4. | Intimidating, grotesque, or terrifying environments that produce fear
| |||||
| 5. | Exposure to the violent actions of others
| |||||
| 6. | Forced to witness the death or torture of others. | |||||
| 7. | Lack of information: ☐ Denial of information to the person. ☐ Denial of information to the family. ☐ Relatives, friends, or colleagues of missing persons. | |||||
| 8. | Use of situations that cause extreme fear ☐ Phobias (exposure to snakes, rats, infectious diseases, blood, etc.) ☐ Claustrophobia (mock burial, confinement in coffins, etc.) | |||||
| Block 4. Actions That Produce Helplessness and Despair | NO | L-C | YES | I | ||
| 1. | Arbitrariness and unpredictability of living conditions (e.g., arbitrary meals, changing sleep cycles, etc.) | |||||
| 2. | Denying information about the rules. Imposing absurd or grotesque rules. Arbitrary, illogical, or contradictory rewards and sanctions. | |||||
| 3. | Forcing the victim to participate in their own torture without the possibility of avoiding it. | |||||
| 4. | Lies or deceptions that cause disorientation or confusion (e.g., unfounded, fabricated, or false information, accusations, or evidence regarding motives or place of detention, family, witnesses, or perpetrators). | |||||
| 5. | Detention of indefinite duration. | |||||
| 6. | Empty times or long waiting times between threats, between interrogations, or between episodes of violence. | |||||
| 7. | General suppression of all rights during a detention (e.g., right to notify family, medical care, legal assistance, interpreter...). Includes incommunicado detention. | |||||
| 8. | Lack of fair legal procedure
| |||||
| Block 5. Actions That Produce Physical Pain | NO | L-C | YES | I | ||
| 1. | Punching, kicking, and/or slapping. Being shaken, dragged, or thrown. | |||||
| 2. | Flagellation, whipping, or beating with batons, sticks, or cables that do not leave permanent marks. Falanga. | |||||
| 3. | Ear slaps with open hands. Pressure on the eyeballs. | |||||
| 4. | Being forced to be permanently in the sun, ice, extreme electrical heating/blinding light, etc. | |||||
| 5. | Prolonged restriction of movement, straitjackets, flanges, shackles, or loops.
| |||||
| 6. | Being forced to stand, sit in a forced position, or kneel for hours; chairs and other implements with restraints | |||||
| 7. | Strenuous exercises (specify): ☐ Forced to run, military training. ☐ Forced labor. ☐ Pushups, squats, sit-ups. ☐ Others: | |||||
| 8. | Dry/wet suffocation—asphyxia (plastic bag, waterboarding...) | |||||
| Block 7. Attacks on Sexual Integrity | NO | L-C | YES | I | ||
| 1. | Humiliations of a sexual nature or related to sexual orientation (e.g., forced nudity, debasing treatment, etc.) | |||||
| 2. | Harassment with signs, suggestions, or threats of sexual assault. | |||||
| 3. | Sexual abuse (e.g., touching, groping, etc.) | |||||
| 4. | Anglerfish | |||||
| 5. | Recording or dissemination of photographs with sexual content | |||||
| 6. | Forced breaking of taboos of a sexual nature (incestuous relationships, forced intercourse with friends, animals, etc.). | |||||
| 7. | Reproductive violence (block abortion in cases of rape, forced abortion, non-aid in birth, forced sterilization, etc.) | |||||
| 8. | Attacks based on sexual or gender identity or orientation (e.g., genital mutilation, conversion therapies, forced virginity tests, honor killings, etc.). | |||||
| Block 8. Attacks on Identity and the Need to Belong | NOT | L-C | YES | I | ||
| 1. | Attacks against the self or sense of self (e.g., forcing a break with the past and previous identity, questioning basic values, breaking relevant worldviews)
| |||||
| 2. | Prolonged periods in environments of inescapable and complete submission and obedience to a person, a group, or an institution
| |||||
| 3. | Manipulation of affect (e.g., actions that promote a traumatic bond with those who exercise dominance or control
| |||||
| 4. | Induction of guilt (e.g., forcing the detainee to do or cause harm to others, induced denunciation or betrayal, failure to protect family or friends, etc.). | |||||
| 5. | Induction of humiliation and/or shame not linked to sexual integrity (e.g., treatment as an animal, impeding personal hygiene, forcing humiliating acts, exhibited in public, repeated vexations, etc.) | |||||
| 6. | Prolonged solitary confinement (more than 15 days). | |||||
| 7. | Prolonged isolation from sources of affect, breaking of social, cultural, or political ties and networks of belonging. Cultural isolation. Separation from relatives (i.e., children, parents) if they are in the same space. | |||||
| 8. | Stigmatization or social criminalization by individuals or by the state, including public attacks, threats, or denigration through the media or social networks or through community or relevant networks of belonging | |||||
| 1 Calculated as 50% of the minimum required for refugee or displaced populations in the Sphere Project Guidelines. | ||||||
References
- United Nations—UN. Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment. 1984. Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-against-torture-and-other-cruel-inhuman-or-degrading (accessed on 15 December 2021).
- Pérez-Sales, P. Psychological Torture. Definition, Evaluation and Measurement; Routledge: London, UK, 2017. [Google Scholar]
- United Nations—UN. Report of the Special Rapporteur on Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment, 20 March 2020. A/HRC/43/49. Available online: https://documents-dds-ny.un.org/doc/UNDOC/GEN/G20/070/73/PDF/G2007073.pdf?OpenElement (accessed on 15 December 2021).
- Manek, J.; Galan-Santamarina, A.; Pérez-Sales, P. Torturing environments and multiple injuries in Mexican migration detention. Humanit. Soc. Sci. Commun. 2022, in press. [CrossRef] [PubMed]
- Grupo de Acción Comunitaria—GAC. Arquitectura de la Tortura en Europa. Los Campos de Refugiados Como Entornos Torturantes: Estudio del Campo de Moria. [Architecture of Torture in Europe. Refugee Camps as Torturing Environments: Study of Moria Camp]. Available online: http://www.psicosocial.net/investigacion/lesbos/ (accessed on 15 December 2021).
- Grupo de Acción Comunitaria—GAC. El Limbo de la Frontera. Impactos de las Condiciones de la Acogida en la Frontera sur Española. 2022. Available online: http://www.psicosocial.net/investigacion/frontera-sur/ (accessed on 1 March 2022).
- Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions a European Agenda on Migration: Brussels, 13.5.2015, COM. 2015. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A52015DC0240 (accessed on 15 December 2021).
- Amnesty International. “Greece 2020”. 2020. Available online: https://www.amnesty.org/es/countries/europe-and-central-asia/greece/report-greece/ (accessed on 15 December 2021).
- United Nations High Commissioner for Refugees—UNHCR. Sea Arrivals Dashboard December 2019. London: UNHCR. 2020. Available online: data2.unhcr.org/en/documents/download/73442 (accessed on 15 December 2021).
- Pérez-Sales, P.; González-Rubio, R.; Mellor-Marsá, B.; Martínez-Alés, G. Beyond torture checklists: An exploratory study of the reliability and construct validity of the Torturing Environment Scale (TES). BMC Public Health 2021, 21, 372. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization & United Nations High Commissioner for Refugees. WHO-UNHCR. Assessment Schedule of Serious Symptoms in Humanitarian Settings (WASSS) (field-test version). In Assessing Mental Health and Psychosocial Needs and Resources: Toolkit for Major Humanitarian Settings; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Save the Children. Multi-Sector Needs Assessment of Migrants and Refugees in Greece. 2015. Available online: https://resourcecentre.savethechildren.net/sites/default/files/documents/greece_assessment_report.pdf (accessed on 15 December 2021).
- Save the Children. A tide of Self-Harm and Depression. The EU-Turkey Deal’s Devastating Impact on Child Refugees and Migrants. 2017. Available online: http://www.savethechildren.ca/wp-content/uploads/2017/03/FINAL-Report_EU-Turkey-deal_-A-tide-of-self-harm-and-depression_March-20171.pdf (accessed on 15 December 2021).
- Refugee Rights Europe—RRE. An Island in Despair. Documentating the Situation for Refugees and Displaced People in Lesvos, Greece. 2018. Available online: https://refugee-rights.eu/wp-content/uploads/2018/11/RRE_AnIslandInDespair.pdf (accessed on 15 December 2021).
- Medecins sans Frontieres. Confronting the Mental Health Emergency on Samos and Lesvos. Why the Containment of Asylum Seekers on the Greek Islands Must End. 2017. Available online: http://urbanspaces.msf.org/wp-content/uploads/2019/03/confronting-the-mental-health-emergency-on-samos-and-Lesbos.pdf (accessed on 15 December 2021).
- Ben Farhat, J.; Blanchet, K.; Juul Bjertrup, P.; Veizis, A.; Perrin, C.; Coulborn, R.M.; Mayaud, P.; Cohuet, S. Syrian refugees in Greece: Experience with violence, mental health status, and access to information during the journey and while in Greece. BMC Med. 2018, 16, 40. [Google Scholar] [CrossRef] [PubMed]
- Episkopou, M.; Venables, E.; Whitehouse, K.; Eleftherakos, C.; Zamatto, F.; de Bartolomé Gisbert, F.; Severy, N.; Barry, D.; Van den Bergh, R. In island containment: A qualitative exploration of social support systems among asylum seekers in a mental health care programme on Lesvos Island, Greece. Confl. Health 2019, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Global Detention Project. Country report. Immigration Detention in Greece: Stranded in Aegean Limbo. 2019. Available online: https://www.globaldetentionproject.org/wp-content/uploads/2019/09/GDP-Immigration-Detention-in-Greece-Stranded-in-Aegean-Limbo.pdf (accessed on 15 December 2021).
- EU Agency for Fundamental Rights. Update of the 2016 FRA Opinion on Fundamental Rights in the Hotspots Set Up in Greece and Italy. Available online: https://fra.europa.eu/en/publication/2019/update-2016-fra-opinion-fundamental-rights-hotspots-set-greece-and-italy (accessed on 22 July 2022).
- EU Agency for Fundamental Rights. Update Fra Opinion on the Hotspots. 2016. Available online: https://fra.europa.eu/sites/default/files/fra_uploads/fra-opinion-5-2016-hotspots_en.pdf (accessed on 22 July 2022).
- International Rescue Committee—IRC. Unprotected, Unsupported, Uncertain: Recommendations to Improve the Mental Health of Asylum Seekers on Lesvos. 2018. Available online: www.rescue.org/sites/default/files/document/3153/unprotectedunsupporteduncertain.pdf (accessed on 10 December 2021).
- Van de Wiel, W.; Castillo-Laborde, C.; Urzúa, F.; Fish, M.; Scholte, W.F. Mental health consequences of long-term stays in refugee camps: Preliminary evidence from Moria. BMC Public Health 2021, 21, 1290. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | N (%) | |
|---|---|---|
| Gender | Women | 80 (50) |
| Men | 80 (50) | |
| Age | <18 | 2 (1.3) |
| 18–65 | 155 (96.8) | |
| >66 | 3 (1.9) | |
| Nationality | Afghanistan | 80 (50) |
| Cameroon | 8 (5) | |
| Congo | 16 (10) | |
| Ivory Coast | 3 (1.9) | |
| Guinea | 1 (0.6) | |
| Iraq | 7 (4.3) | |
| Mali | 2 (1.3) | |
| Palestine | 1 (0.6) | |
| Syria | 22(13.8) | |
| Somalia | 20 (12.5) | |
| Risk of vulnerability | 104 (65) | |
| Time in the camp | 0–4 months | 21 (13.2) |
| 5–8 months | 103 (64.4) | |
| 9–12 | 35 (21.8) | |
| >1 year | 1 (0.6) | |
| With family members in the camp | 87 (54.4) | |
| Mental Health Impact | Total (%) | Extremely (%) |
|---|---|---|
| Fear | 99 | 32 |
| Anger | 97 | 31 |
| Apathy | 96 | 35 |
| Hopelessness | 89 | 31 |
| Suicidal ideation | 94 | 29 |
| Functional impact | 99 | 35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Sales, P.; Galán-Santamarina, A.; Zunzunegui, M.V.; López-Martin, S. Refugee Camps as Torturing Environments—An Analysis of the Conditions in the Moria Reception Center (Greece) Based on the Torturing Environment Scale. Int. J. Environ. Res. Public Health 2022, 19, 10233. https://doi.org/10.3390/ijerph191610233
Pérez-Sales P, Galán-Santamarina A, Zunzunegui MV, López-Martin S. Refugee Camps as Torturing Environments—An Analysis of the Conditions in the Moria Reception Center (Greece) Based on the Torturing Environment Scale. International Journal of Environmental Research and Public Health. 2022; 19(16):10233. https://doi.org/10.3390/ijerph191610233
Chicago/Turabian StylePérez-Sales, Pau, Andrea Galán-Santamarina, María Victoria Zunzunegui, and Sara López-Martin. 2022. "Refugee Camps as Torturing Environments—An Analysis of the Conditions in the Moria Reception Center (Greece) Based on the Torturing Environment Scale" International Journal of Environmental Research and Public Health 19, no. 16: 10233. https://doi.org/10.3390/ijerph191610233
APA StylePérez-Sales, P., Galán-Santamarina, A., Zunzunegui, M. V., & López-Martin, S. (2022). Refugee Camps as Torturing Environments—An Analysis of the Conditions in the Moria Reception Center (Greece) Based on the Torturing Environment Scale. International Journal of Environmental Research and Public Health, 19(16), 10233. https://doi.org/10.3390/ijerph191610233