
Associations between Physical Fitness Index and Body Mass Index in Tibetan Children and Adolescents in Different High-Altitude Areas: Based on a Study in Tibet, China


Abstract
:1. Introduction
2. Materials and Methods
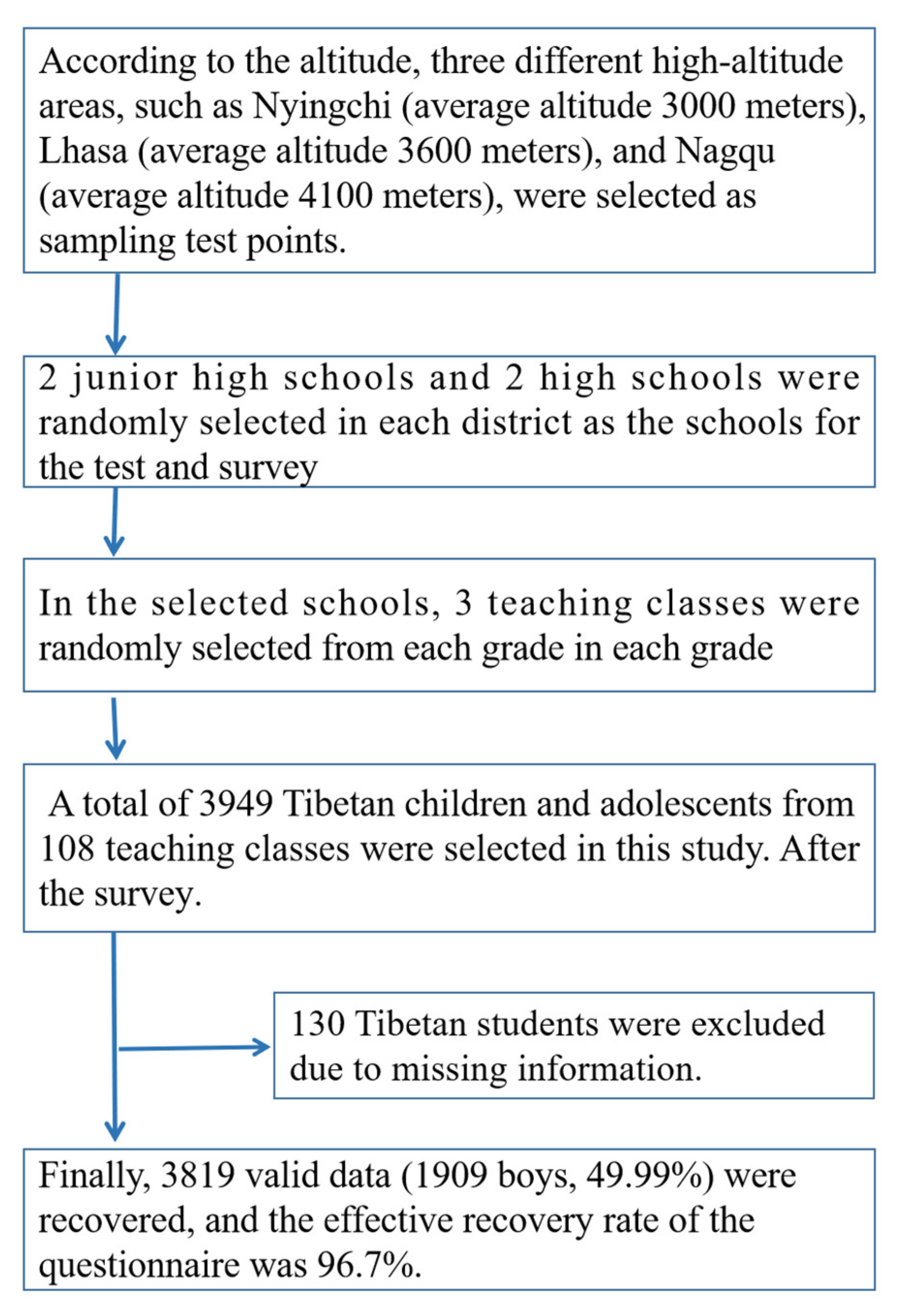
2.1. Participants and Procedures
2.2. Body Mass Index (BMI)
2.3. Physical Fitness Index (PFI)
2.4. Quality Control
2.5. Statistical Analysis
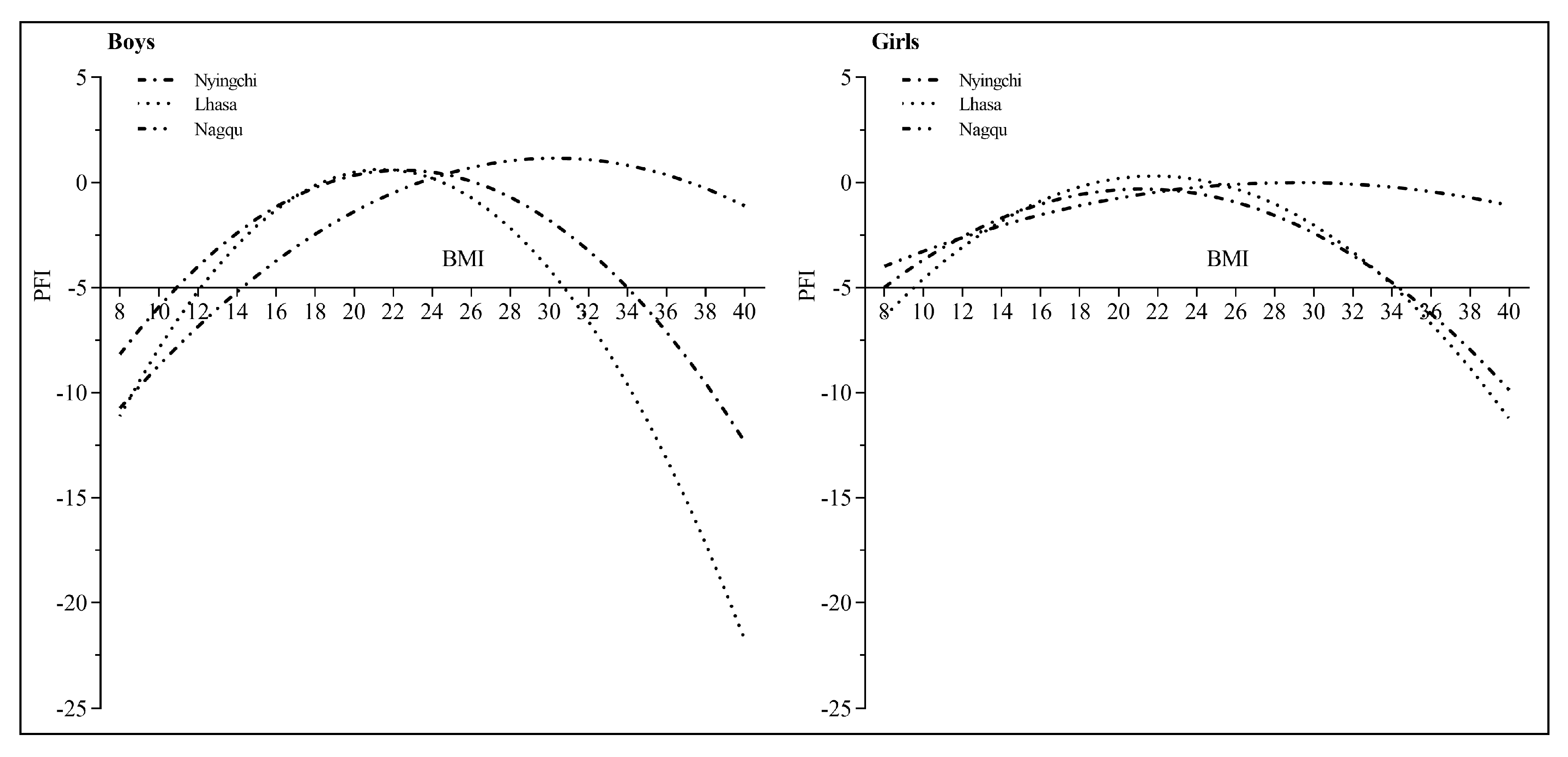
3. Results
- Boys:
- Girls:
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Secchi, J.D.; Garcia, G.C.; Espana-Romero, V.; Castro-Pinero, J. Physical fitness and future cardiovascular risk in argentine children and adolescents: An introduction to the ALPHA test battery. Arch. Argent. Pediatr. 2014, 112, 132–140. [Google Scholar] [PubMed]
- Dong, Y.; Jan, C.; Zou, Z.; Dong, B.; Hu, P.; Ma, Y.; Yang, Z.; Wang, X.; Li, Y.; Gao, D.; et al. Comprehensive physical fitness and high blood pressure in children and adolescents: A national cross-sectional survey in China. J. Sci. Med. Sport 2020, 23, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Qie, R.; Shi, X.; Yang, Y.; Lu, J.; Hu, F.; Zhang, M.; Zhang, Z.; Hu, D.; Zhao, Y. Cardiorespiratory fitness and mortality from all causes, cardiovascular disease and cancer: Dose-response meta-analysis of cohort studies. Br. J. Sports Med. 2022, 56, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Visier-Alfonso, M.E.; Alvarez-Bueno, C.; Sanchez-Lopez, M.; Cavero-Redondo, I.; Martinez-Hortelano, J.A.; Nieto-Lopez, M.; Martinez-Vizcaino, V. Fitness and executive function as mediators between physical activity and academic achievement. J. Sports Sci. 2021, 39, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- Steell, L.; Ho, F.K.; Sillars, A.; Petermann-Rocha, F.; Li, H.; Lyall, D.M.; Iliodromiti, S.; Welsh, P.; Anderson, J.; Mackay, D.F.; et al. Dose-response associations of cardiorespiratory fitness with all-cause mortality and incidence and mortality of cancer and cardiovascular and respiratory diseases: The UK Biobank cohort study. Br. J. Sports Med. 2019, 53, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Ludyga, S.; Puhse, U.; Gerber, M.; Mucke, M. Muscle strength and executive function in children and adolescents with autism spectrum disorder. Autism Res. 2021, 14, 2555–2563. [Google Scholar] [CrossRef]
- Rrecaj-Malaj, S.; Beqaj, S.; Krasniqi, V.; Qorolli, M.; Tufekcievski, A. Outcome of 24 weeks of combined schroth and pilates exercises on cobb angle, angle of trunk rotation, chest expansion, flexibility and quality of life in adolescents with idiopathic scoliosis. Med. Sci. Monit Basic Res. 2020, 26, e920449. [Google Scholar] [CrossRef]
- Liu, Y.; Yin, X.; Zhang, F.; Li, Y.; Bi, C.; Sun, Y.; Li, M.; Zhang, T. Relationship between waist circumference and cardiorespiratory fitness in Chinese children and adolescents: Results from a cross-sectional survey. J. Exerc. Sci. Fit. 2022, 20, 1–8. [Google Scholar] [CrossRef]
- Sengupta, P.; Krajewska-Kulak, E. Evaluation of physical fitness and weight status among fisherwomen in relation to their occupational workload. J. Epidemiol. Glob. Health 2014, 4, 261–268. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, F.; Chen, Q.; Yin, X.; Bi, C.; Yang, X.; Sun, Y.; Li, M.; Zhang, T.; Liu, Y.; et al. Levels of physical fitness and weight status in children and adolescents: A comparison between China and Japan. Int. J. Environ. Res. Public Health 2020, 17, 9569. [Google Scholar] [CrossRef]
- Zhao, Y.Q.; Wang, F.Y.; Zhu, P.; Liu, R.; Hao, J.H.; Su, P.Y.; Wang, L.; Zu, P.; Tao, F.B. Association between body mass index and physical fitness index among children and adolescents. Zhonghua Liu Xing Bing Xue Za Zhi 2012, 33, 265–268. [Google Scholar]
- Huang, Y.C.; Malina, R.M. BMI and health-related physical fitness in Taiwanese youth 9-18 years. Med. Sci. Sports Exerc. 2007, 39, 701–708. [Google Scholar] [CrossRef]
- Choudhuri, D.; Choudhuri, S.; Kulkarni, V.A. Physical fitness: A comparative study between students of residential (Sainik) and non-residential schools (aged 12–14 years). Indian J. Physiol. Pharm. 2002, 46, 328–332. [Google Scholar]
- Dong, Y.; Jan, C.; Ma, Y.; Dong, B.; Zou, Z.; Yang, Y.; Xu, R.; Song, Y.; Ma, J.; Sawyer, S.M.; et al. Economic development and the nutritional status of Chinese school-aged children and adolescents from 1995 to 2014: An analysis of five successive national surveys. Lancet Diabetes Endocrinol. 2019, 7, 288–299. [Google Scholar] [CrossRef]
- Department of Physical Health and Art Education Ministry of Education. The Eighth National Student Physique and Health Survey Results Released. Chin. J. School Health 2021, 42. [Google Scholar] [CrossRef]
- Artero, E.G.; Espana-Romero, V.; Ortega, F.B.; Jimenez-Pavon, D.; Ruiz, J.R.; Vicente-Rodriguez, G.; Bueno, M.; Marcos, A.; Gomez-Martinez, S.; Urzanqui, A.; et al. Health-related fitness in adolescents: Underweight, and not only overweight, as an influencing factor. AVENA Study Scand. J. Med. Sci. Sports 2010, 20, 418–427. [Google Scholar] [CrossRef]
- Garcia-Pastor, T.; Salinero, J.J.; Sanz-Frias, D.; Pertusa, G.; Del, C.J. Body fat percentage is more associated with low physical fitness than with sedentarism and diet in male and female adolescents. Physiol. Behav. 2016, 165, 166–172. [Google Scholar] [CrossRef]
- Monyeki, M.A.; Koppes, L.L.; Kemper, H.C.; Monyeki, K.D.; Toriola, A.L.; Pienaar, A.E.; Twisk, J.W. Body composition and physical fitness of undernourished South African rural primary school children. Eur. J. Clin. Nutr. 2005, 59, 877–883. [Google Scholar] [CrossRef]
- Yang, X.; Yin, X.; Ji, L.; Song, G.; Wu, H.; Li, Y.; Wang, G.; Bi, C.; Sun, Y.; Li, M.; et al. Differences in cardiorespiratory fitness between chinese and japanese children and adolescents. Int. J. Environ. Res. Public Health 2019, 16, 2316. [Google Scholar] [CrossRef]
- Gou, Q.; Shi, R.; Zhang, X.; Meng, Q.; Li, X.; Rong, X.; Gawa, Z.; Zhuoma, N.; Chen, X. The prevalence and risk factors of High-Altitude pulmonary hypertension among native tibetans in sichuan province, china. High. Alt. Med. Biol. 2020, 21, 327–335. [Google Scholar] [CrossRef]
- Zhang, F.; Bi, C.; Yin, X.; Chen, Q.; Liu, Y.; Li, Y.; Sun, Y.; Zhang, T.; Yang, X.; Li, M. Roles of age, sex, and weight status in the muscular fitness of Chinese Tibetan children and adolescents living at altitudes over 3600 m: A cross-sectional study. Am. J. Hum. Biol. 2022, 34, e23624. [Google Scholar] [CrossRef]
- Xi, H.; Li, W.; Zhao, H. Review of tibetan biological anthropology research. J. Anthropol. 2015, 34, 260–266. [Google Scholar]
- Chai, X. A Study on the Relationship between BMI and Cardiorespiratory Endurance in Tibetan and Chinese Children and Adolescents. Master’s Thesis, East China Normal University, Shanghai, China, 2018. [Google Scholar]
- National Health and Family Planning. Malnutrition Screening for School-Age Children and Adolescents WS/T456-2014. Available online: http://www.moh.gov.cn/zwgkzt/pgt/201407/386/5coa/ed444e89e12752decatta.shtml (accessed on 25 July 2022).
- National Health and Family Planning. Screening for Overweight and Obesity in School-Aged Children and Adolescents WS/T586-2018. Available online: http://www.nhc.gov.cn/ewebeditor/uploadlife/2018/03/20180330094031236.pdf (accessed on 25 July 2022).
- Dong, Y.H.; Yang, Z.G.; Yang, Y.D.; Wang, S.; Wang, Z.H.; Wang, X.J.; Chen, Y.J.; Zou, Z.Y.; Ma, J. The association between the malnutrition and blood pressure in Chinese Han students aged 7–18 years in 2014. Zhonghua Yu Fang Yi Xue Za Zhi 2018, 52, 791–797. [Google Scholar]
- Dong, Y.H.; Wang, Z.H.; Yang, Z.G.; Wang, X.J.; Chen, Y.J.; Zou, Z.Y.; Ma, J. Epidemic status and secular trends of malnutrition among children and adolescents aged 7–18 years from 2005 to 2014 in China. Beijing Da Xue Xue Bao Yi Xue Ban 2017, 49, 424–432. [Google Scholar]
- Chinese Student Physique and Health Research Group. 2014 Survey Report on Chinese Students’ Physical Fitness and Health; Higher Education Press: Beijing, China, 2016. [Google Scholar]
- Ministry of Education of the People’s Republic of China. Implementation Plan of National Student Physique and Health Survey and Nationalstudent Physique Health Standard Spot Check in 2019. Available online: http://www.moe.gov.cn/2019-07-12 (accessed on 10 July 2019).
- Zhang, F.; Bi, C.; Yin, X.; Chen, Q.; Li, Y.; Liu, Y.; Zhang, T.; Li, M.; Sun, Y.; Yang, X. Physical fitness reference standards for Chinese children and adolescents. Sci. Rep. 2021, 11, 4991. [Google Scholar] [CrossRef]
- Bi, C.; Zhang, F.; Gu, Y.; Song, Y.; Cai, X. Secular Trend in the Physical Fitness of Xinjiang Children and Adolescents between 1985 and 2014. Int. J. Environ. Res. Public Health 2020, 17, 2195. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1.6 million participants. Lancet Child. Adolesc Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Huang, W.; Shi, X.; Wang, Y.; Li, X.; Gao, P.; Lu, J.; Zhuang, J. Determinants of student’s physical activity: A 12-month follow-up study in Ningxia province. BMC Public Health 2021, 21, 512. [Google Scholar] [CrossRef] [PubMed]
- Duruturk, N.; Ozkoslu, M.A. Effect of tele-rehabilitation on glucose control, exercise capacity, physical fitness, muscle strength and psychosocial status in patients with type 2 diabetes: A double blind randomized controlled trial. Prim. Care Diabetes 2019, 13, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.R.; Lichtblau, M.; Furian, M.; Mayer, L.C.; Berlier, C.; Muller, J.; Saxer, S.; Schwarz, E.I.; Bloch, K.E.; Ulrich, S. Cardiorespiratory adaptation to Short-Term exposure to altitude vs. Normobaric hypoxia in patients with pulmonary hypertension. J. Clin. Med. 2022, 11, 2769. [Google Scholar] [PubMed]
- Cossio-Bolanos, M.; Gomez-Campos, R.; Castelli, C.D.C.L.; Sulla-Torres, J.; Urra-Albornoz, C.; Pires, L.V. Muscle strength and body fat percentage in children and adolescents from the Maule region, Chile. Arch. Argent. Pediatr. 2020, 118, 320–326. [Google Scholar] [PubMed]
- Maher, C.; Olds, T.S.; Eisenmann, J.C.; Dollman, J. Screen time is more strongly associated than physical activity with overweight and obesity in 9- to 16-year-old Australians. Acta Paediatr. 2012, 101, 1170–1174. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Chen, M.; Song, Y.; Ma, J.; Lau, P. Geographical Variation in Physical Fitness among Chinese Children and Adolescents from 2005 to 2014. Front. Public Health 2021, 9, 694070. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Age (yrs) | Boys | H-Value | p-Value | Girls | H-Value | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Nyingchi | Lhasa | Nagqu | Nyingchi | Lhasa | Nagqu | |||||
| 13 | 0.03 (−1.6, 1.97) | −0.06 (−2.55, 1.62) | −5.17 (−7.55, −2.77) | 96.423 | <0.01 | −0.13 (−1.78, 1.22) | 0.03 (−1.29, 1.68) | −1.17 (−3.52, 0.27) | 8.679 | <0.05 |
| 14 | 0.03 (−1.70, 1.65) | −0.40 (−2.80, 1.66) | −1.37 (−3.50, 0.08) | 11.397 | <0.01 | −0.23 (−1.64, 1.01) | −0.02 (−1.46, 2.28) | −1.16 (−3.12, 0.39) | 10.120 | <0.01 |
| 15 | −0.42 (−2.82, 1.40) | −0.58 (−2.22, 1.56) | −2.88 (−4.56, −1.00) | 23.439 | <0.01 | −1.26 (−3.12, 0.73) | −1.08 (−3.30, 0.94) | −1.10 (−2.43, 0.48) | 0.068 | 0.967 |
| 16 | 0.65 (−1.04, 1.75) | 0.94 (−0.33, 2.38) | −1.38 (−3.07, 1.93) | 22.260 | <0.01 | −0.03 (−2.05, 1.44) | −1.08 (−3.30, 0.94) | −0.97 (−3.53, 1.62) | 11.465 | <0.01 |
| 17 | 0.38 (−0.78, 2.12) | 0.84 (−1.25, 2.00) | −0.66 (−2.67, 1.57) | 3.418 | 0.181 | −0.47 (−1.84, 1.45) | 0.57 (−0.86, 2.32) | −0.64 (−2.86, 0.40) | 16.482 | <0.01 |
| 18 | 0.56 (−0.80, 2.31) | 1.21 (−0.21, 2.37) | −1.60 (−3.23, 0.65) | 32.916 | <0.01 | −1.03 (−2.95, 1.19) | −0.48 (−1.89, 1.57) | 0.43 (−0.83, 1.92) | 7.690 | <0.05 |
| Age (yrs) | Boys | H-Value | p-Value | Girls | H-Value | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Malnutrition | Normal | Overweight and Obesity | Malnutrition | Normal | Overweight and Obesity | |||||
| 13 | −3.31 (−5.62, −0.70) | −1.11 (−3.51, 1.48) | −1.02 (−5.12, 0.37) | 12.712 | <0.01 | −3.02 (−4.85, −1.01) | −0.12 (−1.75, 1.4) | −0.55 (−2.53, 0.6) | 10.836 | <0.01 |
| 14 | −3.38 (−4.61, −1.49) | −0.10 (−1.82, 1.63) | −1.10 (−3.73, 0.75) | 36.462 | <0.01 | −1.71 (−3.52, −0.88) | −0.32 (−1.79, 1.18) | −0.43 (−2.02, 0.85) | 3.815 | 0.148 |
| 15 | −3.42 (−5.45, −1.20) | −0.64 (−2.78, 1.46) | −2.20 (−3.96, −1.12) | 18.654 | <0.01 | −1.28 (−4.21, −0.43) | −1.07 (−2.94, 0.93) | −1.34 (−3.2, 0.44) | 0.777 | 0.678 |
| 16 | −1.65 (−4.47, 0.88) | 0.61 (−1.53, 2.14) | 0.04 (−2.03, 0.80) | 3.874 | 0.144 | 1.41 (−0.44, 3.28) | −0.04 (−2.15, 2.10) | −0.44 (−1.99, 1.50) | 0.223 | 0.894 |
| 17 | −1.24 (−2.46, 1.07) | 0.51 (−1.04, 2.10) | −0.07 (−2.81, 1.73) | 10.833 | <0.01 | −0.37 (−2.12, 1.02) | 0.04 (−1.54, 1.99) | −0.74 (−2.30, 0.55) | 4.580 | 0.101 |
| 18 | 0.10 (−1.73, 1.32) | 0.38 (−1.46, 2.09) | −0.77 (−2.15, 1.21) | 1.634 | 0.442 | −0.83 (−2.06, 1.88) | −0.18 (−2.06, 1.74) | −0.65 (−2.21, 1.68) | 2.825 | 0.243 |
| Gender | Area | Arguments/Constants | B-Value | Standard Error | β-Value | t-Value | p-Value |
|---|---|---|---|---|---|---|---|
| Boys (n = 1909) | Nyingchi | BMI | 1.886 | 0.245 | 2.034 | 7.691 | <0.01 |
| BMI2 | −0.042 | 0.005 | −2.032 | −7.683 | <0.01 | ||
| (Constants) | −20.577 | 2.726 | −7.547 | <0.01 | |||
| Lhasa | BMI | 2.788 | 0.341 | 2.693 | 8.171 | <0.01 | |
| BMI2 | −0.065 | 0.008 | −2.736 | −8.301 | <0.01 | ||
| (Constants) | −29.267 | 3.690 | −7.932 | <0.01 | |||
| Nagqu | BMI | 1.453 | 0.240 | 1.146 | 6.064 | <0.01 | |
| BMI2 | −0.024 | 0.005 | −0.876 | −4.634 | <0.01 | ||
| (Constants) | −20.837 | 2.698 | −7.723 | <0.01 | |||
| Girls (n = 1910) | Nyingchi | BMI | 1.143 | 0.320 | 1.308 | 3.568 | <0.01 |
| BMI2 | −0.027 | 0.007 | −1.391 | −3.795 | <0.01 | ||
| (Constants) | −12.403 | 3.568 | −3.476 | <0.01 | |||
| Lhasa | BMI | 1.528 | 0.349 | 1.540 | 4.373 | <0.01 | |
| BMI2 | −0.035 | 0.008 | −1.556 | −4.419 | <0.01 | ||
| (Constants) | −16.365 | 3.845 | −4.256 | <0.01 | |||
| Nagqu | BMI | 0.523 | 0.303 | 0.547 | 1.728 | 0.085 | |
| BMI2 | −0.009 | 0.007 | −0.405 | −1.280 | 0.201 | ||
| (Constants) | −7.601 | 3.121 | −2.436 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Su, F.; Song, Y.; Lu, J. Associations between Physical Fitness Index and Body Mass Index in Tibetan Children and Adolescents in Different High-Altitude Areas: Based on a Study in Tibet, China. Int. J. Environ. Res. Public Health 2022, 19, 10155. https://doi.org/10.3390/ijerph191610155
Zhang Y, Su F, Song Y, Lu J. Associations between Physical Fitness Index and Body Mass Index in Tibetan Children and Adolescents in Different High-Altitude Areas: Based on a Study in Tibet, China. International Journal of Environmental Research and Public Health. 2022; 19(16):10155. https://doi.org/10.3390/ijerph191610155
Chicago/Turabian StyleZhang, Yunjie, Fan Su, Yongjing Song, and Jinkui Lu. 2022. "Associations between Physical Fitness Index and Body Mass Index in Tibetan Children and Adolescents in Different High-Altitude Areas: Based on a Study in Tibet, China" International Journal of Environmental Research and Public Health 19, no. 16: 10155. https://doi.org/10.3390/ijerph191610155
APA StyleZhang, Y., Su, F., Song, Y., & Lu, J. (2022). Associations between Physical Fitness Index and Body Mass Index in Tibetan Children and Adolescents in Different High-Altitude Areas: Based on a Study in Tibet, China. International Journal of Environmental Research and Public Health, 19(16), 10155. https://doi.org/10.3390/ijerph191610155