
Assessing Relationships between Physically Demanding Work and Late-Life Disability in Italian Nonagenarian Women Living in a Rural Area

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
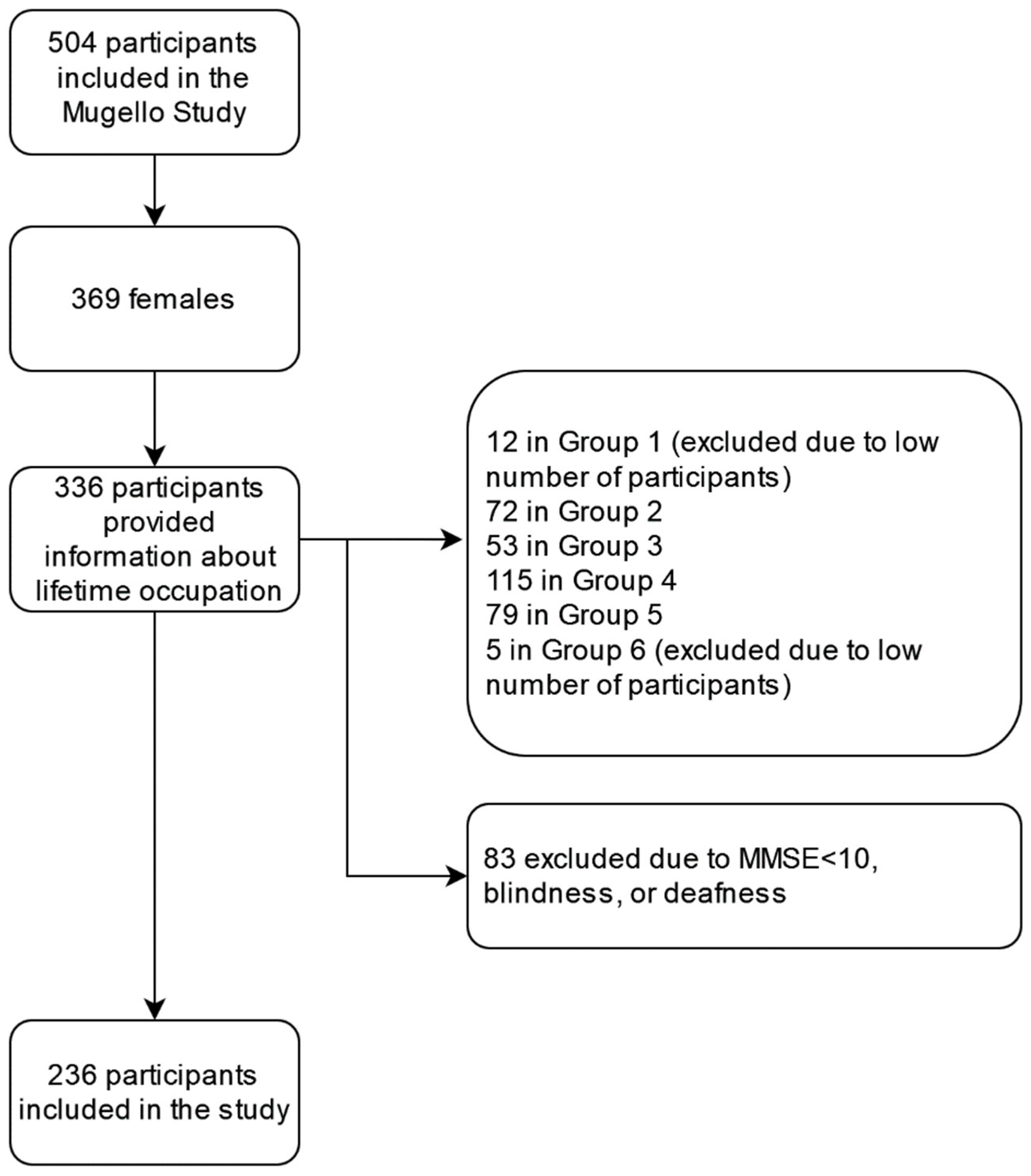
2.1. Study Population
2.2. Sociodemographic and Lifestyle
2.3. Medical History and Drug Consumption
2.4. Physical and Functional Status
2.5. Cognitive and Psychological Status, Self-Perceived Quality of Life
2.6. Lifetime Occupation
2.7. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Christensen, K.; Doblhammer, G.; Rau, R.; Vaupel, J.W. Ageing populations: The challenges ahead. Lancet 2009, 374, 1196–1208. [Google Scholar] [CrossRef]
- Seccombe, K.; Ishii-Kuntz, M. Perceptions of Problems Associated with Aging: Comparisons Among Four Older Age Cohorts. Gerontologist 1991, 31, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Berlau, D.; Corrada, M.; Peltz, C.B.; Kawas, C.H. Disability in the Oldest-Old: Incidence and Risk Factors in The 90+ Study. Am. J. Geriatr. Psychiatry 2012, 20, 159–168. [Google Scholar] [CrossRef]
- Herr, M.; Arvieu, J.; Robine, J.; Ankri, J. Health, frailty and disability after ninety: Results of an observational study in France. Arch. Gerontol. Geriatr. 2016, 66, 166–175. [Google Scholar] [CrossRef]
- Van Houwelingen, A.H.; Cameron, I.D.; Gussekloo, J.; Putter, H.; Kurrle, S.; De Craen, A.J.M.; Maier, A.; Elzen, W.D.; Blom, J.W. Disability transitions in the oldest old in the general population. The Leiden 85-plus study. AGE 2013, 36, 483–493. [Google Scholar] [CrossRef]
- Cecchi, F.; Pancani, S.; Molino-Lova, R.; Castagnoli, C.; Paperini, A.; Boni, R.; Gori, G.; Macchi, C.; The Mugello Study Working Group. Mugello Study Working Group Independent Functioning in Nonagenarians Living in a Rural Italian Community: The Mugello Study. J. Appl. Gerontol. 2019, 39, 259–268. [Google Scholar] [CrossRef]
- Møller, A.; Reventlow, S.; Hansen, M.; Andersen, L.L.; Siersma, V.; Lund, R.; Avlund, K.; Andersen, J.H.; Mortensen, O.S. Does physical exposure throughout working life influence chair-rise performance in midlife? A retrospective cohort study of associations between work and physical function in Denmark. BMJ Open 2015, 5, e009873. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Leino-Arjas, P.; Solovieva, S.; Riihimäki, H.; Kirjonen, J.; Telama, R. Leisure time physical activity and strenuousness of work as predictors of physical functioning: A 28 year follow up of a cohort of industrial employees. Occup. Environ. Med. 2004, 61, 1032–1038. [Google Scholar] [CrossRef]
- Mc Carthy, V.J.C.; Perry, I.J.; Greiner, B.A. Has your work worked you too hard? Physically demanding work and disability in a sample of the older Irish population. Ir. J. Med Sci. 2012, 182, 47–55. [Google Scholar] [CrossRef][Green Version]
- Prakash, K.C.; Neupane, S.; Leino-Arjas, P.; von Bonsdorff, M.B.; Rantanen, T.; von Bonsdorff, M.E.; Seitsamo, J.; Ilmarinen, J.; Nygård, C.-H. Midlife job profiles and disabilities in later life: A 28-year follow-up of municipal employees in Finland. Int. Arch. Occup. Environ. Health 2016, 89, 997–1007. [Google Scholar] [CrossRef]
- Missikpode, C.; Michael, Y.L.; Wallace, R.B. Midlife Occupational Physical Activity and Risk of Disability Later in Life: National Health and Aging Trends Study. J. Am. Geriatr. Soc. 2016, 64, 1120–1127. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, L.H.; Done, N.; Baum, M. Lifetime job demands and later life disability. J. Econ. Ageing 2018, 17, 100184. [Google Scholar] [CrossRef] [PubMed]
- Enroth, L.; Raitanen, J.; Hervonen, A.; Jylhä, M. Do Socioeconomic Health Differences Persist in Nonagenarians? J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2013, 68, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Geroldi, C.; Frisoni, G.B.; Rozzini, R.; Trabucchi, M. Disability and Principal Lifetime Occupation in the Elderly. Int. J. Aging Hum. Dev. 1996, 43, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Ravesteijn, B.; Van Kippersluis, H.; Van Doorslaer, E. The wear and tear on health: What is the role of occupation? Health Econ. 2017, 27, e69–e86. [Google Scholar] [CrossRef]
- Kwak, Y.; Kim, Y. Health-related Quality of Life and Mental Health of Elderly by Occupational Status. Iran. J. Public Health 2017, 46, 1028–1037. [Google Scholar]
- Shockey, T.M.; Zack, M.; Sussell, A. Health-Related Quality of Life Among US Workers: Variability Across Occupation Groups. Am. J. Public Health 2017, 107, 1316–1323. [Google Scholar] [CrossRef]
- Holtermann, A.; Krause, N.; Van Der Beek, A.J.; Straker, L. The physical activity paradox: Six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br. J. Sports Med. 2017, 52, 149–150. [Google Scholar] [CrossRef]
- Coenen, P.; Huysmans, M.A.; Holtermann, A.; Krause, N.; Van Mechelen, W.; Straker, L.M.; Van Der Beek, A.J. Do highly physically active workers die early? A systematic review with meta-analysis of data from 193 696 participants. Br. J. Sports Med. 2018, 52, 1320–1326. [Google Scholar] [CrossRef]
- Väisänen, D.; Kallings, L.V.; Andersson, G.; Wallin, P.; Hemmingsson, E.; Ekblom-Bak, E. Lifestyle-associated health risk indicators across a wide range of occupational groups: A cross-sectional analysis in 72,855 workers. BMC Public Health 2020, 20, 1656. [Google Scholar] [CrossRef]
- Li, J.; Loerbroks, A.; Angerer, P. Physical activity and risk of cardiovascular disease: What does the new epidemiological evidence show? Curr. Opin. Cardiol. 2013, 28, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Harbin, S.; Irvin, E.; Johnston, H.; Begum, M.; Tiong, M.; Apedaile, D.; Koehoorn, M.; Smith, P. Sex and Gender Differences in Occupational Hazard Exposures: A Scoping Review of the Recent Literature. Curr. Environ. Health Rep. 2021, 8, 267–280. [Google Scholar] [CrossRef] [PubMed]
- Elser, H.; Falconi, A.M.; Bass, M.; Cullen, M.R. Blue-collar work and women’s health: A systematic review of the evidence from 1990 to 2015. SSM Popul. Health 2018, 6, 195–244. [Google Scholar] [CrossRef] [PubMed]
- Louzado, J.; Cortes, M.L.; Oliveira, M.G.; Bezerra, V.M.; Mistro, S.; de Medeiros, D.S.; Soares, D.A.; Silva, K.O.; Kochergin, C.N.; Carvalho, V.H.d.S.d.; et al. Gender Differences in the Quality of Life of Formal Workers. Int. J. Environ. Res. Public Health 2021, 18, 5951. [Google Scholar] [CrossRef] [PubMed]
- Molino-Lova, R.; Sofi, F.; Pasquini, G.; Gori, A.; Vannetti, F.; Abbate, R.; Gensini, G.F.; Macchi, C. The Mugello Study, a survey of nonagenarians living in Tuscany: Design, methods and participants’ general characteristics. Eur. J. Intern. Med. 2013, 24, 745–749. [Google Scholar] [CrossRef] [PubMed]
- De Cock, A.-M.; Fransen, E.; Perkisas, S.; Verhoeven, V.; Beauchet, O.; Vandewoude, M.; Remmen, R. Comprehensive Quantitative Spatiotemporal Gait Analysis Identifies Gait Characteristics for Early Dementia Subtyping in Community Dwelling Older Adults. Front. Neurol. 2019, 10, 313. [Google Scholar] [CrossRef]
- Paffenbarger, R.S.; Hyde, R.T.; Wing, A.L.; Hsieh, C. Physical activity, all-cause mortality, and longevity of college alumni. New Engl. J. Med. 1986, 314, 605–613. [Google Scholar] [CrossRef]
- Macchi, C.; Polcaro, P.; Cecchi, F.; Zipoli, R.; Sofi, F.; Romanelli, A.; Pepi, L.; Sibilio, M.; Lipoma, M.; Petrilli, M.; et al. One-Year Adherence to Exercise in Elderly Patients Receiving Postacute Inpatient Rehabilitation After Cardiac Surgery. Am. J. Phys. Med. Rehabilitation 2009, 88, 727–734. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Broeiro-Gonçalves, P.; Nogueira, P.; Aguiar, P. Multimorbidity and Disease Severity by Age Groups, in Inpatients: Cross-Sectional Study. Port. J. Public Health 2019, 37, 1–9. [Google Scholar] [CrossRef]
- Bravell, M.E.; Berg, S.; Malmberg, B. Health, functional capacity, formal care, and survival in the oldest old: A longitudinal study. Arch. Gerontol. Geriatr. 2008, 46, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association With Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M. Assessing the impact of comorbidity in the older population. Ann. Epidemiology 1996, 6, 376–380. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The index of Adl: A standardized measure of biological and phychological funcation. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Barberger-Gateau, P.; Rainville, C.; Letenneur, L.; Dartigues, J.-F. A hierarchical model of domains of disablement in the elderly: A longitudinal approach. Disabil. Rehabilitation 2000, 22, 308–317. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Lucca, U.; Tettamanti, M.; Logroscino, G.; Tiraboschi, P.; Landi, C.; Sacco, L.; Garrì, M.; Ammesso, S.; Bertinotti, C.; Biotti, A.; et al. Prevalence of dementia in the oldest old: The Monzino 80-plus population based study. Alzheimer’s Dement. 2015, 11, 258–270.e3. [Google Scholar] [CrossRef] [PubMed]
- Cevenini, E.; The GEHA Project Consortium; Cotichini, R.; Stazi, M.A.; Toccaceli, V.; Palmas, M.G.; Capri, M.; De Rango, F.; Dato, S.; Passarino, G.; et al. Health status and 6 years survival of 552 90+ Italian sib-ships recruited within the EU Project GEHA (GEnetics of Healthy Ageing). AGE 2013, 36, 949–966. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Flaherty, J.; Dong, B.; Liu, G.; Deng, J.; Zhang, Y.; Wu, J.; Zeng, G.; Ren, X.; Hu, J.; et al. Impact of Geriatric Conditions Versus Medical Diagnoses on ADL Disability Among Nonagenarians and Centenarians. J. Aging Health 2012, 24, 1298–1319. [Google Scholar] [CrossRef] [PubMed]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomised controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Marengoni, A.; von Strauss, E.; Rizzuto, D.; Winblad, B.; Fratiglioni, L. The impact of chronic multimorbidity and disability on functional decline and survival in elderly persons. A community-based, longitudinal study. J. Intern. Med. 2009, 265, 288–295. [Google Scholar] [CrossRef]
- Parry, S.P.; Coenen, P.; Shrestha, N.; O’Sullivan, P.B.; Maher, C.G.; Straker, L.M. Workplace interventions for increasing standing or walking for decreasing musculoskeletal symptoms in sedentary workers. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Shiri, R.; Coggon, D.; Falah-Hassani, K. Exercise for the Prevention of Low Back Pain: Systematic Review and Meta-Analysis of Controlled Trials. Am. J. Epidemiol. 2018, 187, 1093–1101. [Google Scholar] [CrossRef]
- Bertuccio, P.; Alicandro, G.; Sebastiani, G.; Zengarini, N.; Costa, G.; La Vecchia, C.; Frova, L. Mortality by occupation-based social class in Italy from 2012 to 2014. Int. J. Public Health 2018, 63, 865–874. [Google Scholar] [CrossRef]
- Yong, S.-J.; Gwini, S.M.; Tembo, M.C.; Ng, B.L.; Low, C.H.; Malon, R.G.; Dunning, T.L.; Pasco, J.A.; Kotowicz, M.A. Frailty associations with socioeconomic status, healthcare utilisation and quality of life among older women residing in regional Australia. J. Frailty Sarcopenia Falls 2021, 6, 209–217. [Google Scholar] [CrossRef]


{kind=link}
| n | Tot | Group 2 (n = 57) | Group 3 (n = 41) | Group 4 (n = 90) | Group 5 (n = 48) | p-Value | |
|---|---|---|---|---|---|---|---|
| Age (years) | 236 | 92 [4] | 92 [5] | 92 [4] | 92 [4] | 91.5 [4] | 0.754 |
| Work duration (years) | 227 | 47 [38] | 35 [40] * | 30 [37] * | 46 [39] * | 70 [15] | <0.001 |
| Education (years) | 234 | 3 [2] | 5 [2] †,‡ range 1–11 | 3 [2] range 0–8 | 3 [2] range 0–5 | 5 [2]† range 0–8 | <0.001 |
| Non-institutionalized | 236 | 216 (91.5%) | 50 (87.7%) | 36 (87.8%) | 85 (94.4%) | 45 (93.8%) | 0.378 |
| BMI (kg/m2) | 227 | 25 [6] | 25 [7] | 25 [7] | 26 [5] | 25 [7] | 0.583 |
| Marital status | 236 | 0.342 | |||||
| Single | 8 (3.4%) | 4 (7%) | 2 (4.9%) | 1 (1.1%) | 1 (2.1%) | ||
| Married | 7 (3.0%) | 2 (3.5%) | 1 (2.4%) | 4 (4.4%) | 0 (0%) | ||
| Widowed | 221 (93.6%) | 51 (89.5%) | 38 (92.7%) | 85 (94.4%) | 47 (97.9%) | ||
| Use of tobacco | 234 | 0.380 | |||||
| No | 201 (85.9%) | 44 (80%) | 33 (80.5%) | 82 (91.1%) | 42 (87.5%) | ||
| Previous history | 29 (12.4%) | 10 (18.2%) | 7 (17.1%) | 7 (7.8%) | 5 (10.4%) | ||
| Yes | 4 (1.7%) | 1 (1.8%) | 1 (2.4%) | 1 (1.1%) | 1 (2.1%) | ||
| Pregnancies≥ 2 | 234 | 161 (68.8%) | 27 (48.2%)† | 21 (51.2%)† | 79 (88.8%) | 34 (70.8%) | <0.001 |
| MMSE | 236 | 23 [9] | 25 [6]† | 22 [10] | 21 [9] | 24.5 [11] | 0.001 |
| CCI | 236 | 0.397 | |||||
| ≤5 | 123 (52.1%) | 33 (57.9%) | 16 (39.0%) | 48 (53.3%) | 26 (54.2%) | ||
| 6–8 | 92 (39.0%) | 17 (29.8%) | 22 (53.3%) | 35 (38.9%) | 18 (37.5%) | ||
| >8 | 21 (8.9%) | 7 (12.3%) | 3 (7.3%) | 7 (7.8%) | 4 (8.3%) | ||
| Number of drugs | 235 | 0.403 | |||||
| <4 | 90 (38.3%) | 27 (47.4%) | 13 (31.7%) | 33 (36.7%) | 17 (36.2%) | ||
| ≥4 | 145 (61.7%) | 30 (52.6%) | 28 (68.3%) | 57 (63.3%) | 30 (63.8%) | ||
| MCS | 220 | 46 [11] | 45 [11] | 45 [8] | 47 [11] | 48 [11] | 0.639 |
| GDS > 8 | 227 | 64 (28.2%) | 17 (30.9%) | 7 (17.5%) | 27 (31.8%) | 13 (27.7%) | 0.391 |
| n | Tot | Group 2 (n = 57) | Group 3 (n = 41) | Group 4 (n = 90) | Group 5 (n = 48) | p-Value | |
|---|---|---|---|---|---|---|---|
| SPPB | 235 | 3 [5] | 4 [6] | 2 [5] | 2 [4] | 3 [5] | 0.511 |
| Physical activity | 234 | 0.137 | |||||
| Active | 108 (46.2%) | 27 (48.2%) | 14 (34.1%) | 39 (43.8%) | 28 (58.3%) | ||
| Sedentary | 126 (53.8%) | 29 (51.8%) | 27 (65.9%) | 50 (56.2%) | 20 (41.7%) | ||
| Handgrip max | 224 | 12 [6] | 12 [5] | 12 [5] | 12 [6] | 15 [8] | 0.335 |
| BADL lost | 231 | 1 [3] | 1 [3] | 1 [3] | 1 [2] | 1 [2] | 0.067 |
| No BADL lost | 231 | 74 (32.0%) | 21 (39.6%)† | 16 (39.0%)† | 18 (20.0%) | 19 (40.4%)† | 0.020 |
| IADL lost | 231 | 3 [6] | 2 [7] | 3 [6] | 3 [7] | 3 [5] | 0.395 |
| No IADL lost | 231 | 49 (21.2%) | 17 (32.1%) | 7 (17.1%) | 17 (18.9%) | 8 (17.0%) | 0.176 |
| PCS | 220 | 42 [12] | 44 [14] | 43 [11] | 41 [11] | 42 [12] | 0.405 |
| B | S.E. | p-Value | OR | 95%CI Low | 95%CI High | |
|---|---|---|---|---|---|---|
| Education (years) | −0.007 | 0.103 | 0.942 | 0.993 | 0.811 | 1.215 |
| MMSE | 0.171 | 0.035 | 0.000 | 1.186 | 1.106 | 1.271 |
| Group 2 (Group 5 = ref) | −0.348 | 0.457 | 0.447 | 0.706 | 0.288 | 1.731 |
| Group 3 (Group 5 = ref) | 0.000 | 0.494 | 1.000 | 1.000 | 0.379 | 2.635 |
| Group 4 (Group 5 = ref) | −0.672 | 0.453 | 0.138 | 0.511 | 0.210 | 1.241 |
| Number of pregnancies ≥ 2 | −0.299 | 0.358 | 0.403 | 0.741 | 0.368 | 1.494 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lombardi, G.; Pancani, S.; Lorenzini, F.; Vannetti, F.; Pasquini, G.; Frandi, R.; Turcan, N.; Razzolini, L.; Molino Lova, R.; Cecchi, F.; et al. Assessing Relationships between Physically Demanding Work and Late-Life Disability in Italian Nonagenarian Women Living in a Rural Area. Int. J. Environ. Res. Public Health 2022, 19, 8880. https://doi.org/10.3390/ijerph19148880
Lombardi G, Pancani S, Lorenzini F, Vannetti F, Pasquini G, Frandi R, Turcan N, Razzolini L, Molino Lova R, Cecchi F, et al. Assessing Relationships between Physically Demanding Work and Late-Life Disability in Italian Nonagenarian Women Living in a Rural Area. International Journal of Environmental Research and Public Health. 2022; 19(14):8880. https://doi.org/10.3390/ijerph19148880
Chicago/Turabian StyleLombardi, Gemma, Silvia Pancani, Francesca Lorenzini, Federica Vannetti, Guido Pasquini, Roberta Frandi, Nona Turcan, Lorenzo Razzolini, Raffaello Molino Lova, Francesca Cecchi, and et al. 2022. "Assessing Relationships between Physically Demanding Work and Late-Life Disability in Italian Nonagenarian Women Living in a Rural Area" International Journal of Environmental Research and Public Health 19, no. 14: 8880. https://doi.org/10.3390/ijerph19148880
APA StyleLombardi, G., Pancani, S., Lorenzini, F., Vannetti, F., Pasquini, G., Frandi, R., Turcan, N., Razzolini, L., Molino Lova, R., Cecchi, F., & Macchi, C. (2022). Assessing Relationships between Physically Demanding Work and Late-Life Disability in Italian Nonagenarian Women Living in a Rural Area. International Journal of Environmental Research and Public Health, 19(14), 8880. https://doi.org/10.3390/ijerph19148880