
Location-Allocation Model to Improve the Distribution of COVID-19 Vaccine Centers in Jeddah City, Saudi Arabia

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
Contribution
2. Literature Review
3. Materials and Methods
3.1. Location-Allocation Models
3.2. Maximal Covering Location Problem
- the set of demand nodes ,
- the set of potential facilities ,
- a pre–defined maximum distance,
- = the distance from a demand i to facility j,
- = the number of demands at a given node i (e.g., the population at a given node),
- = the set of facilities nodes j that can cover demand node i. ,
- = a binary variable indicates whether a facility is located at j (1) or not (0),
- = a binary decision variable indicates whether the node/demand i is covered (1) or not (0).
- = the percentage of uncovered demands,
- = the fraction of demand at node i assigned to facility j,
- = the capacity of a facility location,
- the set of demand nodes i that can be covered by a facility node j. .
3.2.1. Maximize Coverage
3.2.2. Maximize Capacitated Coverage
3.2.3. Minimize Facilities
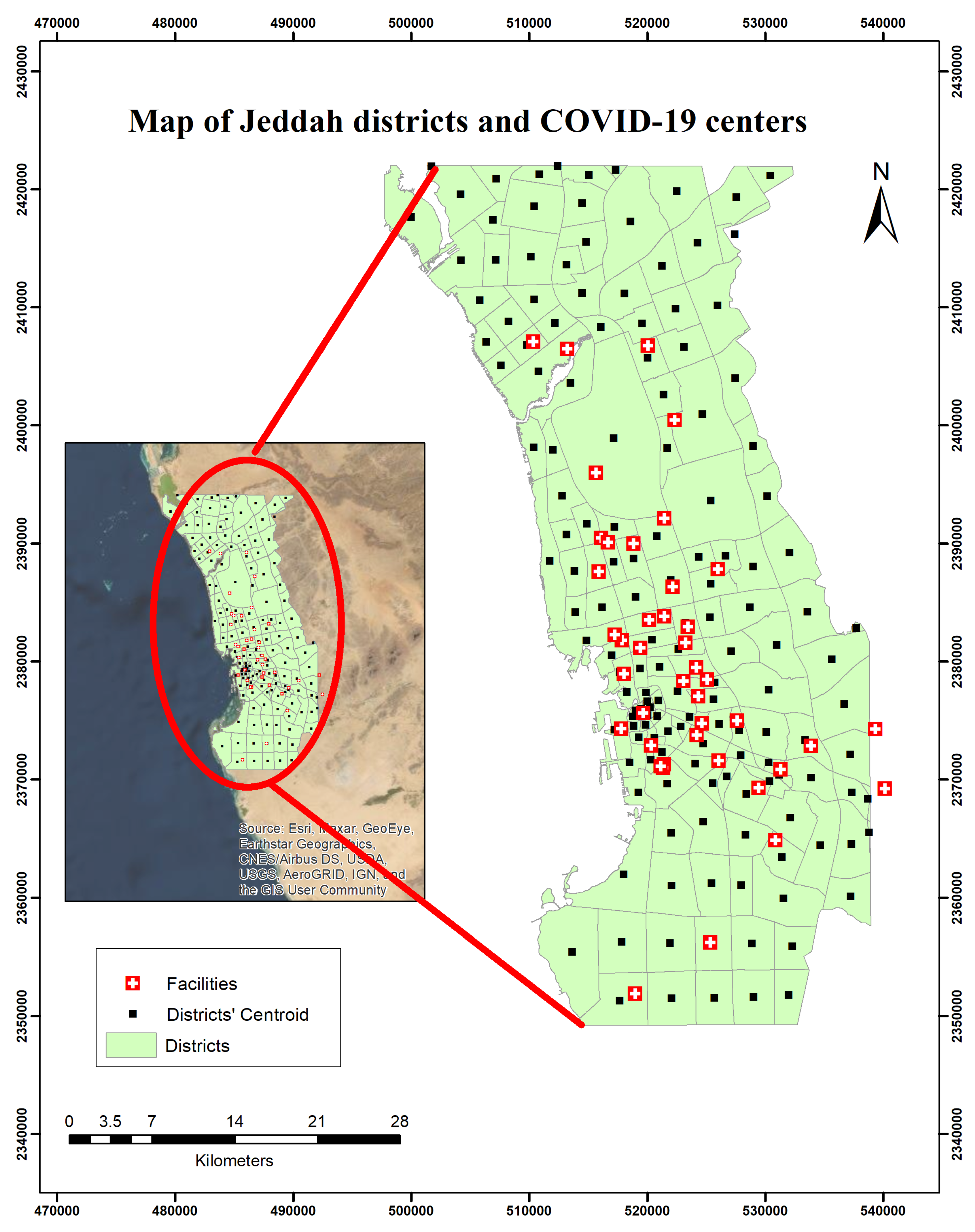
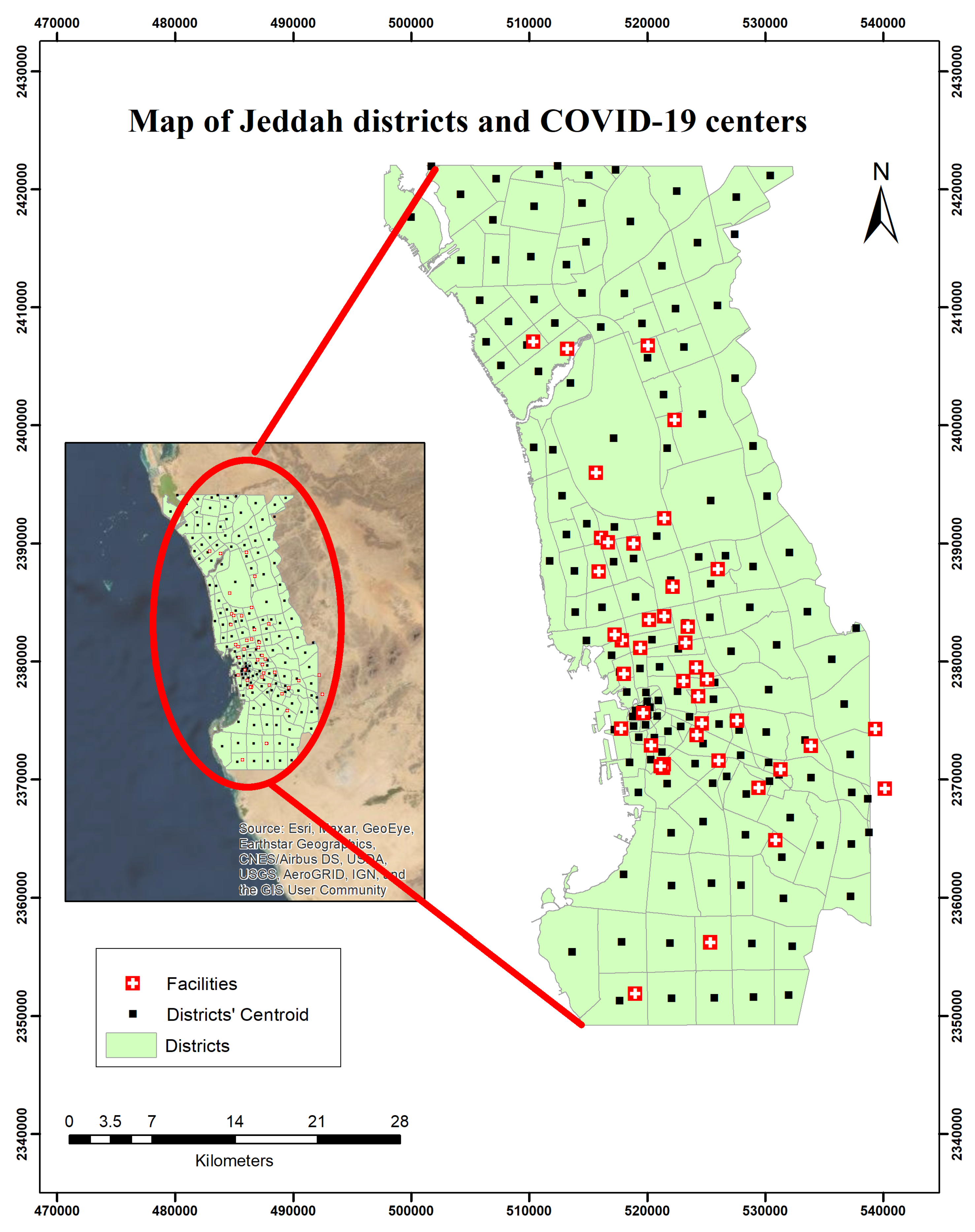
3.3. Study Area
3.4. Data
3.5. Objective Function
3.6. Software
4. Experiments and Results
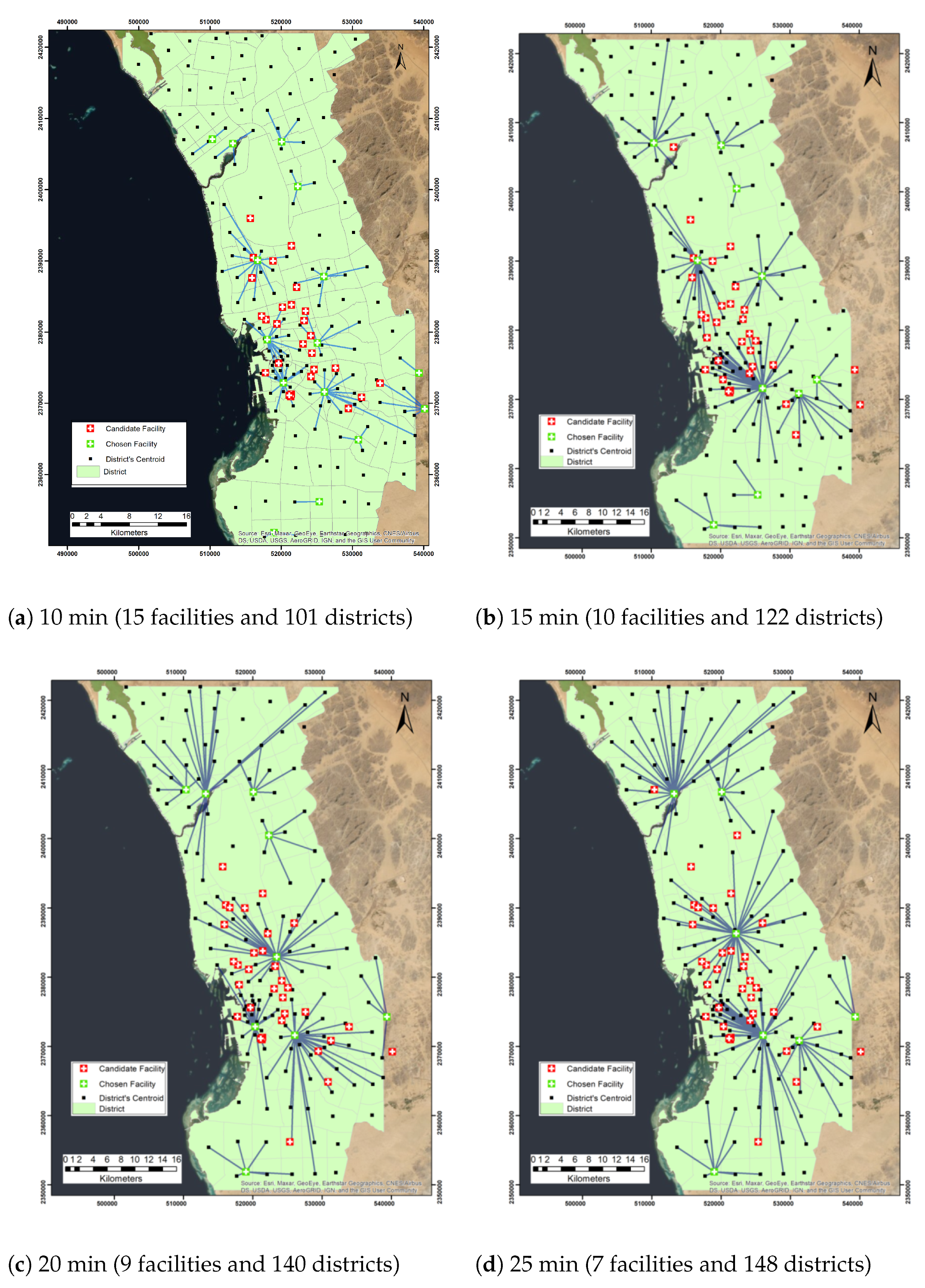
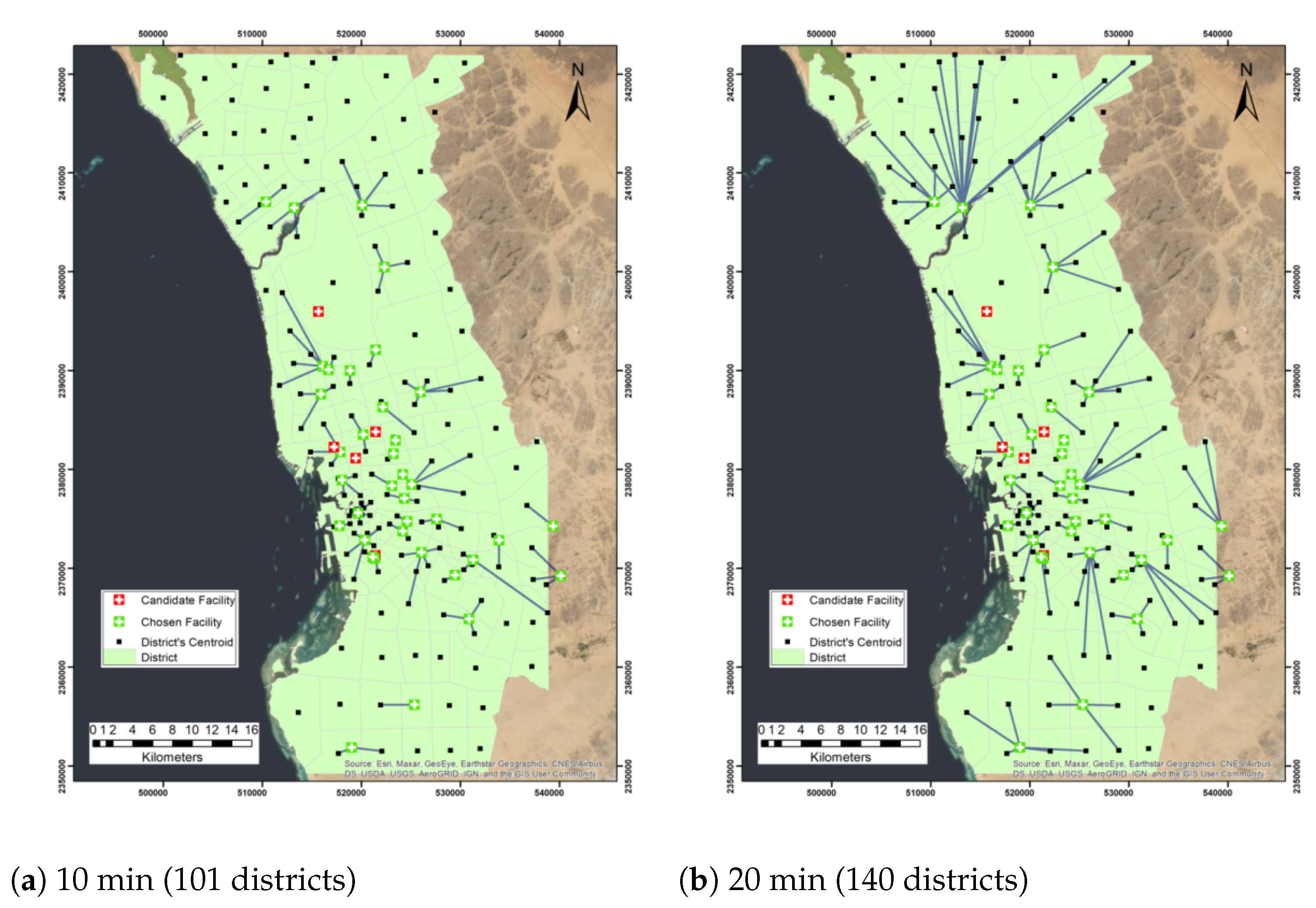
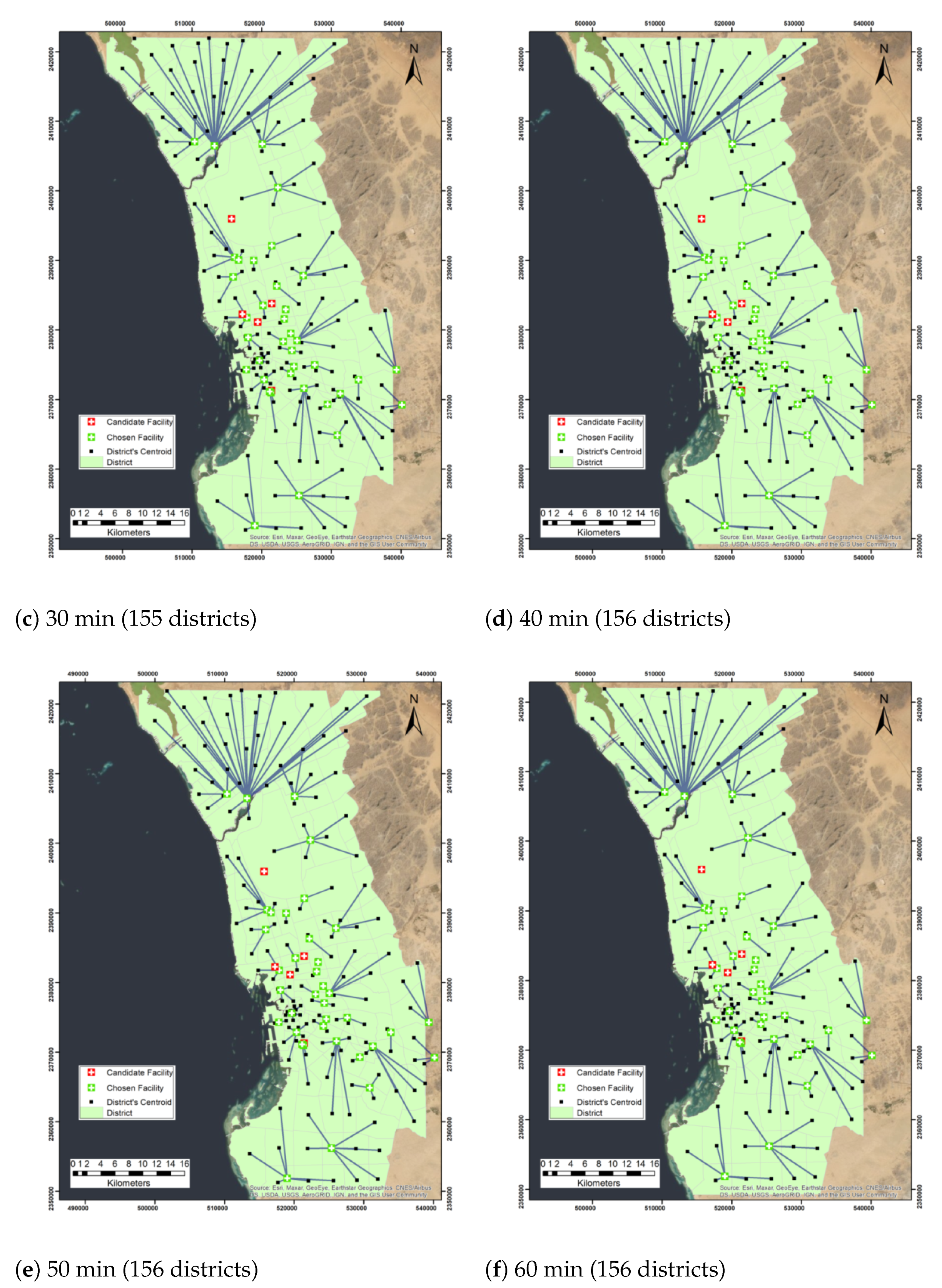
4.1. Maximize Coverage
- Facilities are uncapacitated.
- The impedance is based on time in minutes.
- The travel type is from demand point to facility.
- The impedance transformation is linear.
- Roads are bidirectional.
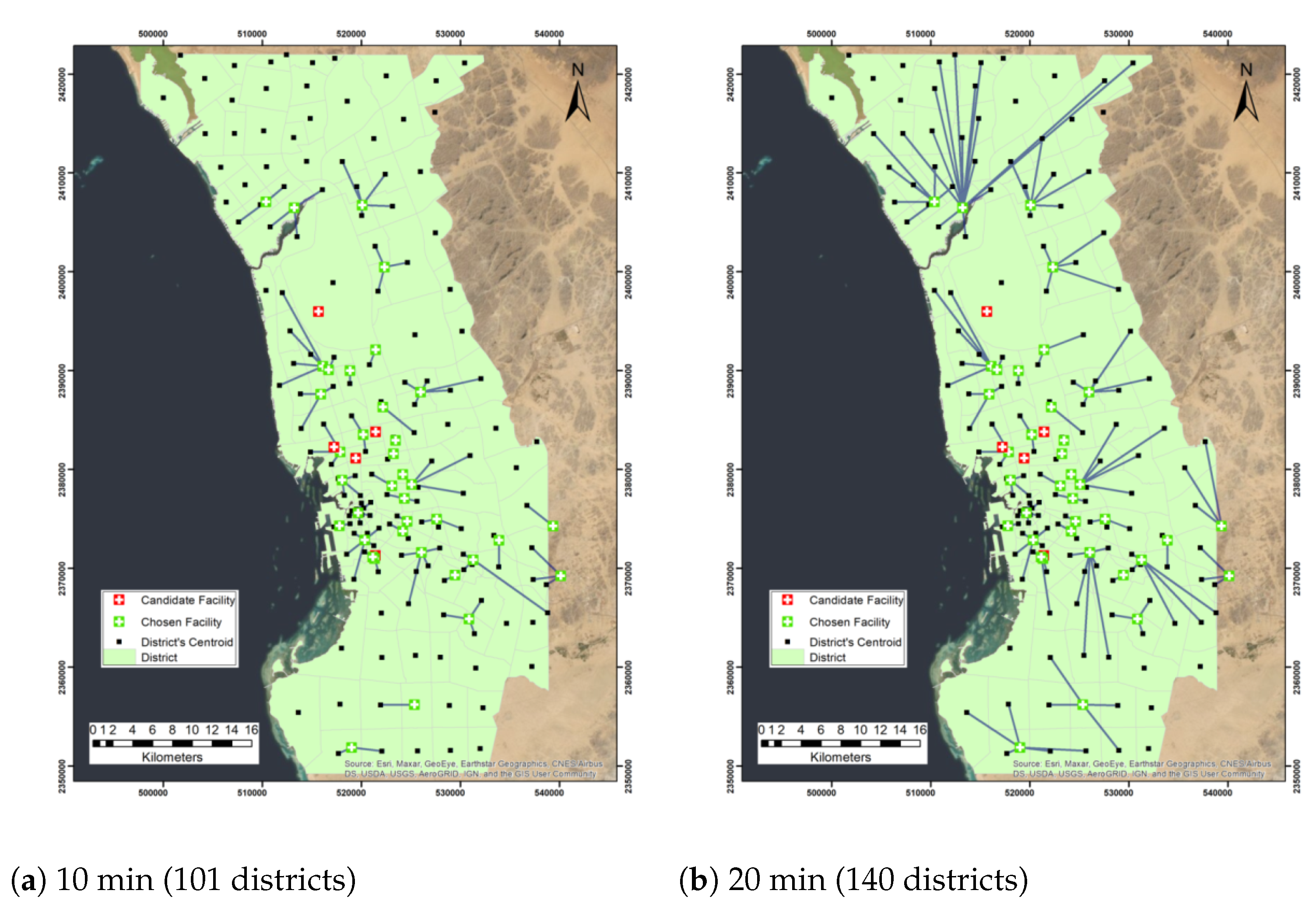
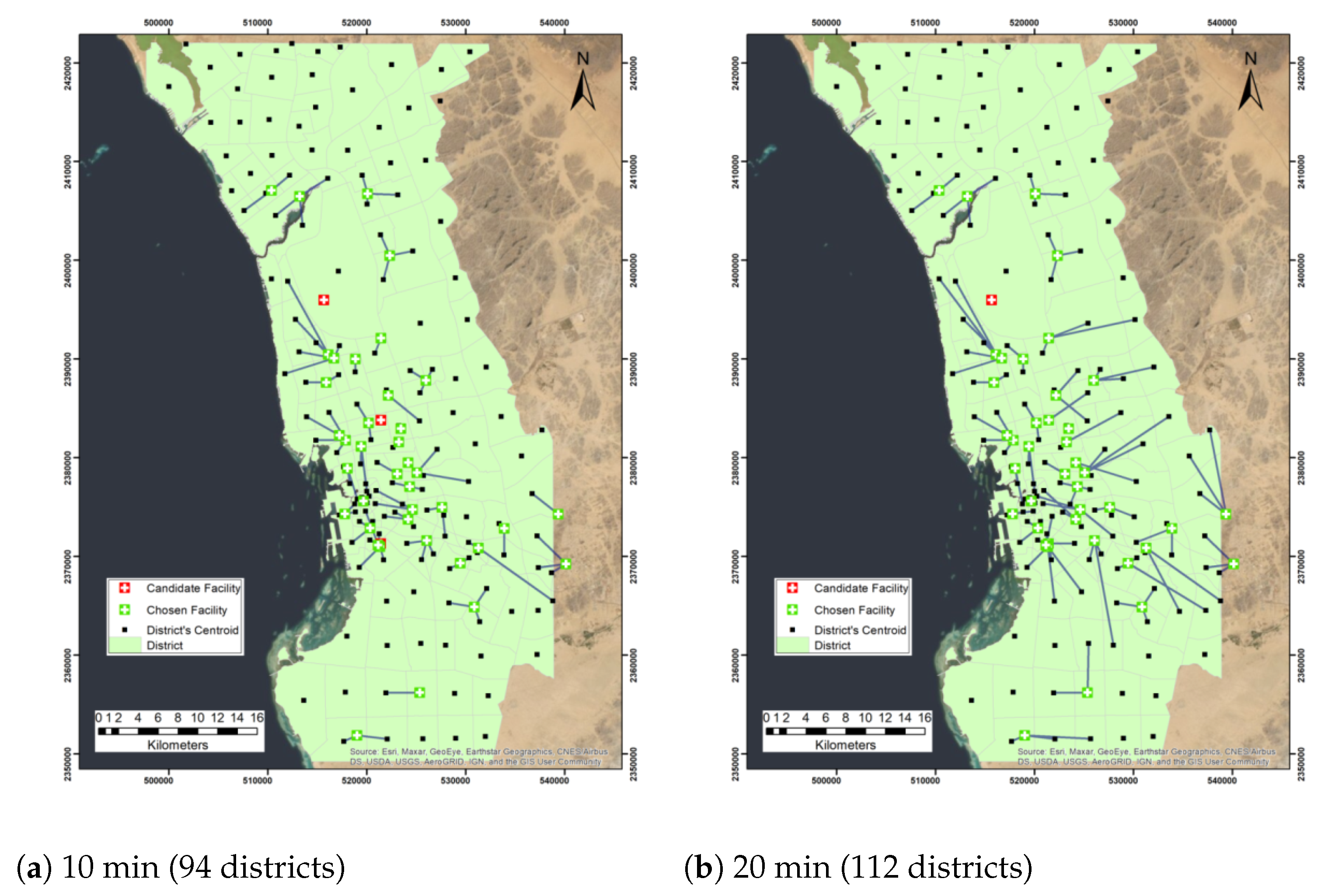
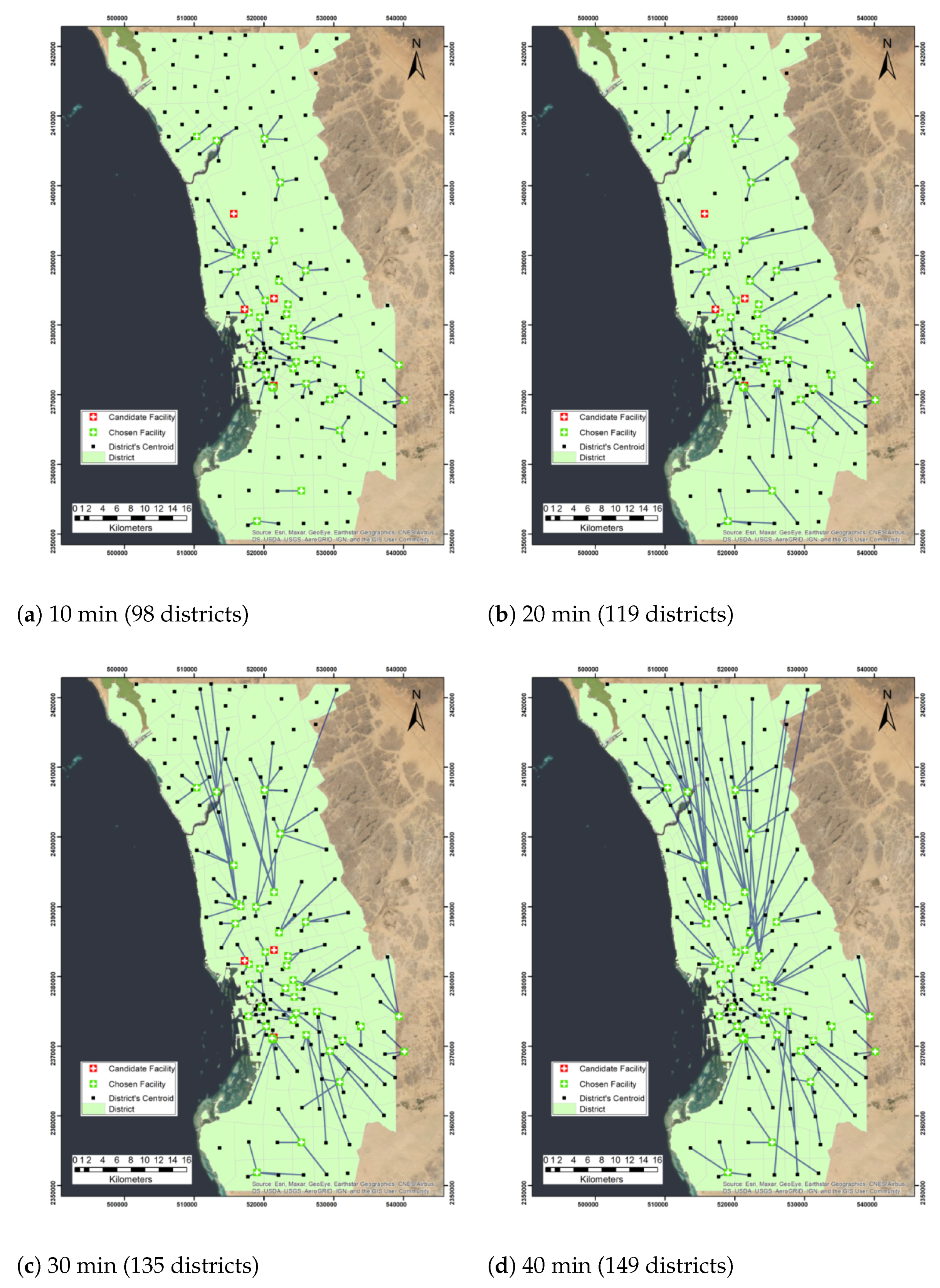
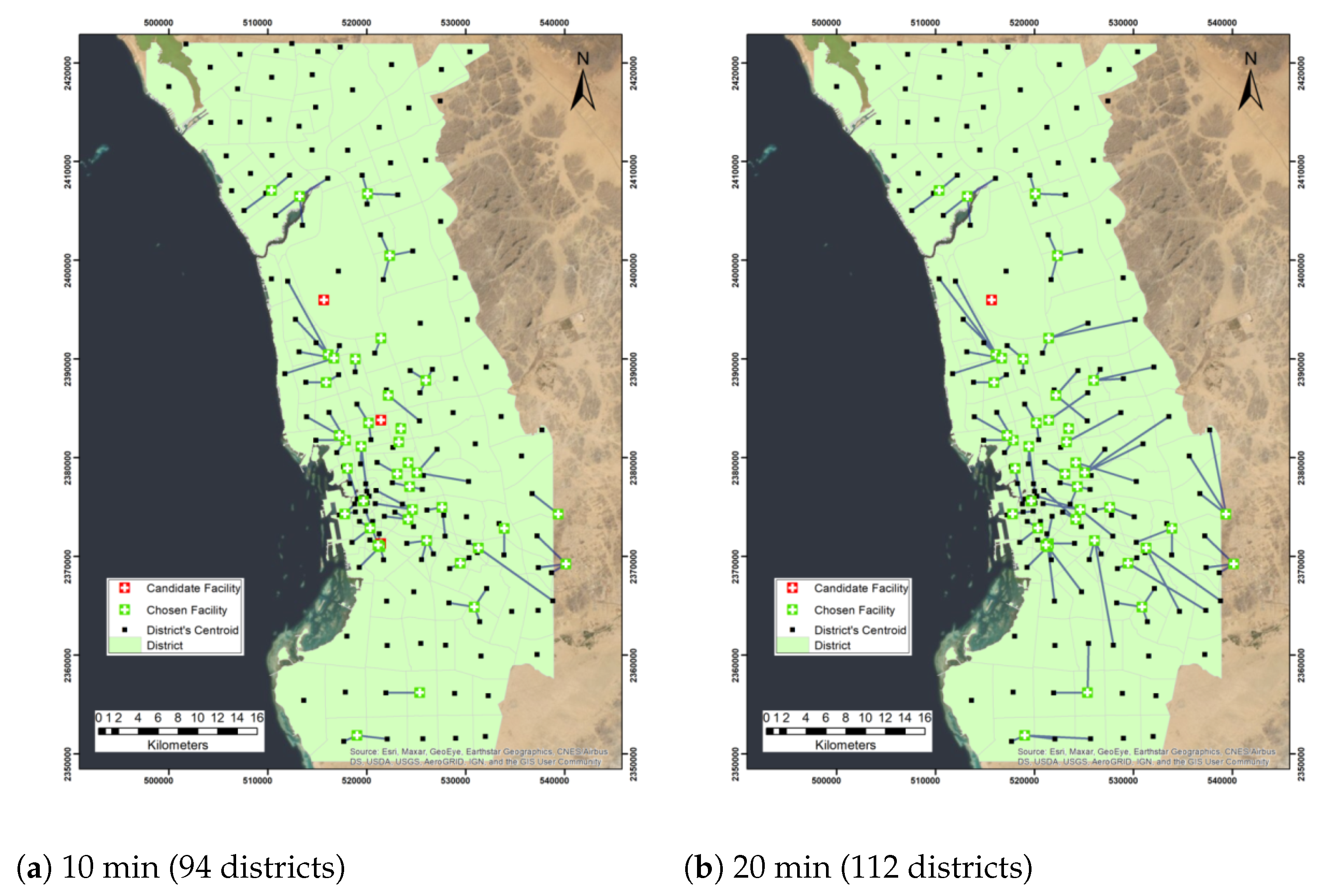
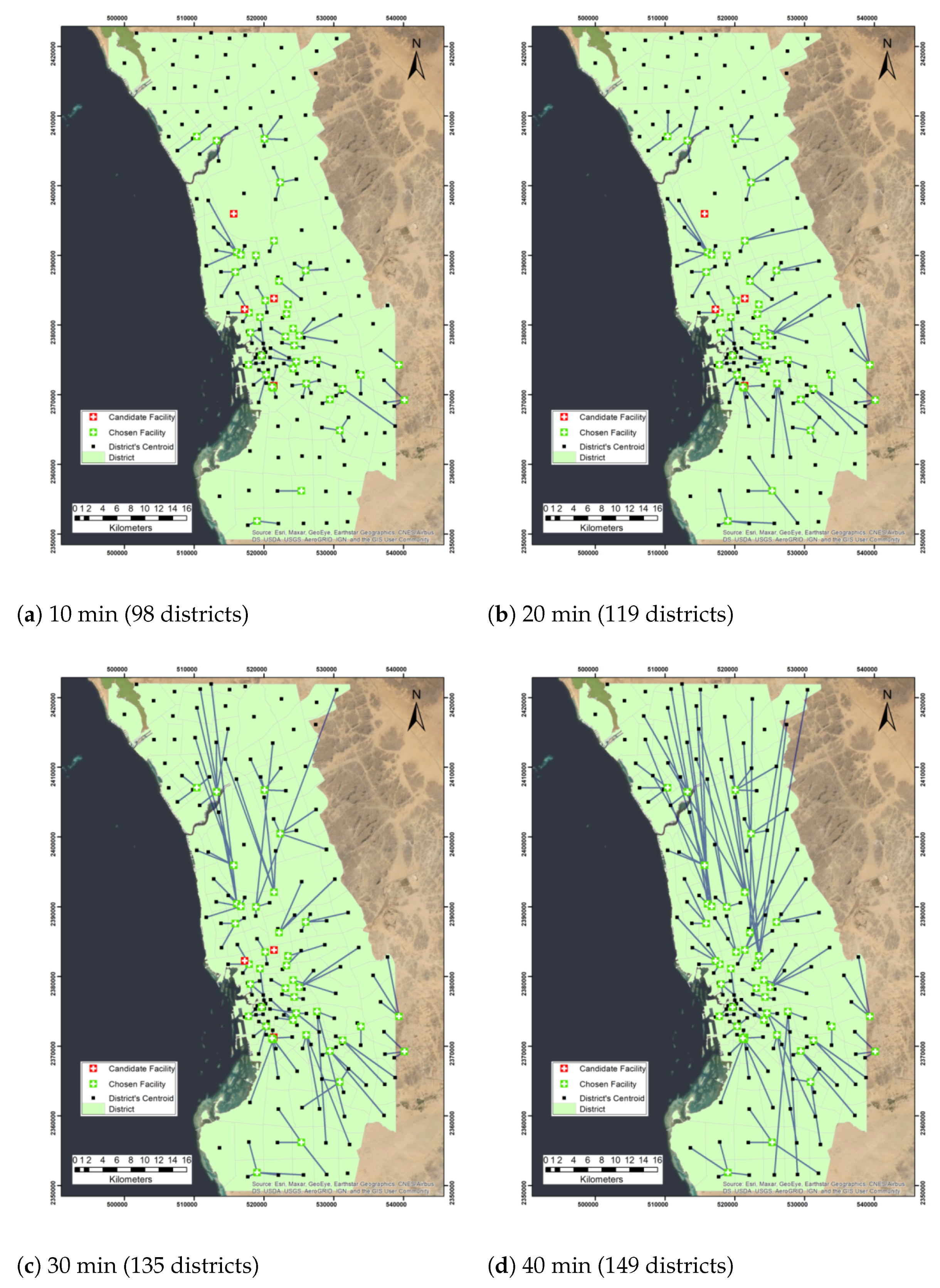
4.2. Maximize Capacitated Coverage
- Each facility has a limited capacity to cover demand from a fixed number of districts (analyzed scenarios with three and four districts).
- The impedance is based on time in minutes.
- The travel type is from demand point to facility.
- The impedance transformation is linear (equal to the cost of the shortest path between the demand point and the facility).
- Roads are bidirectional.
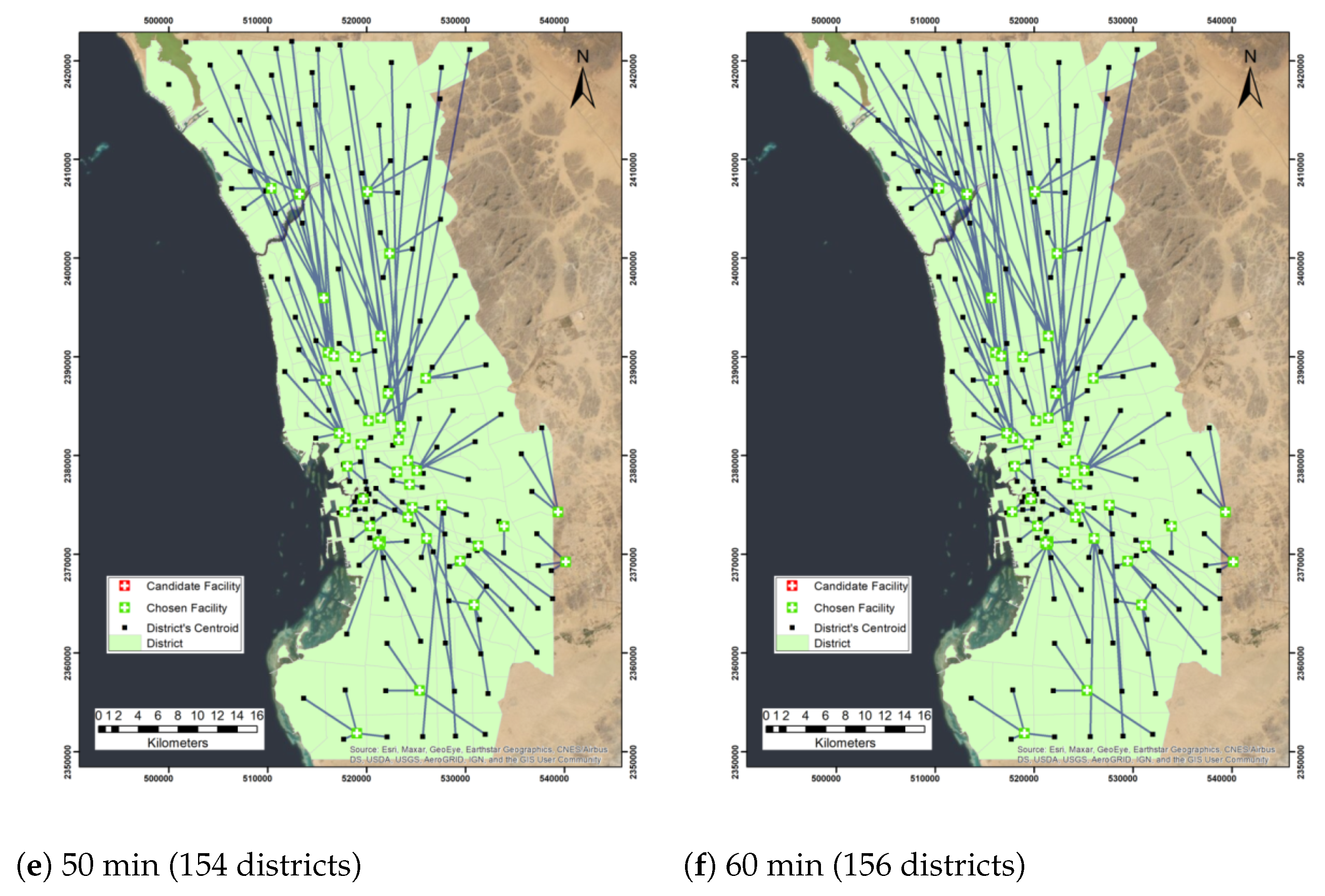
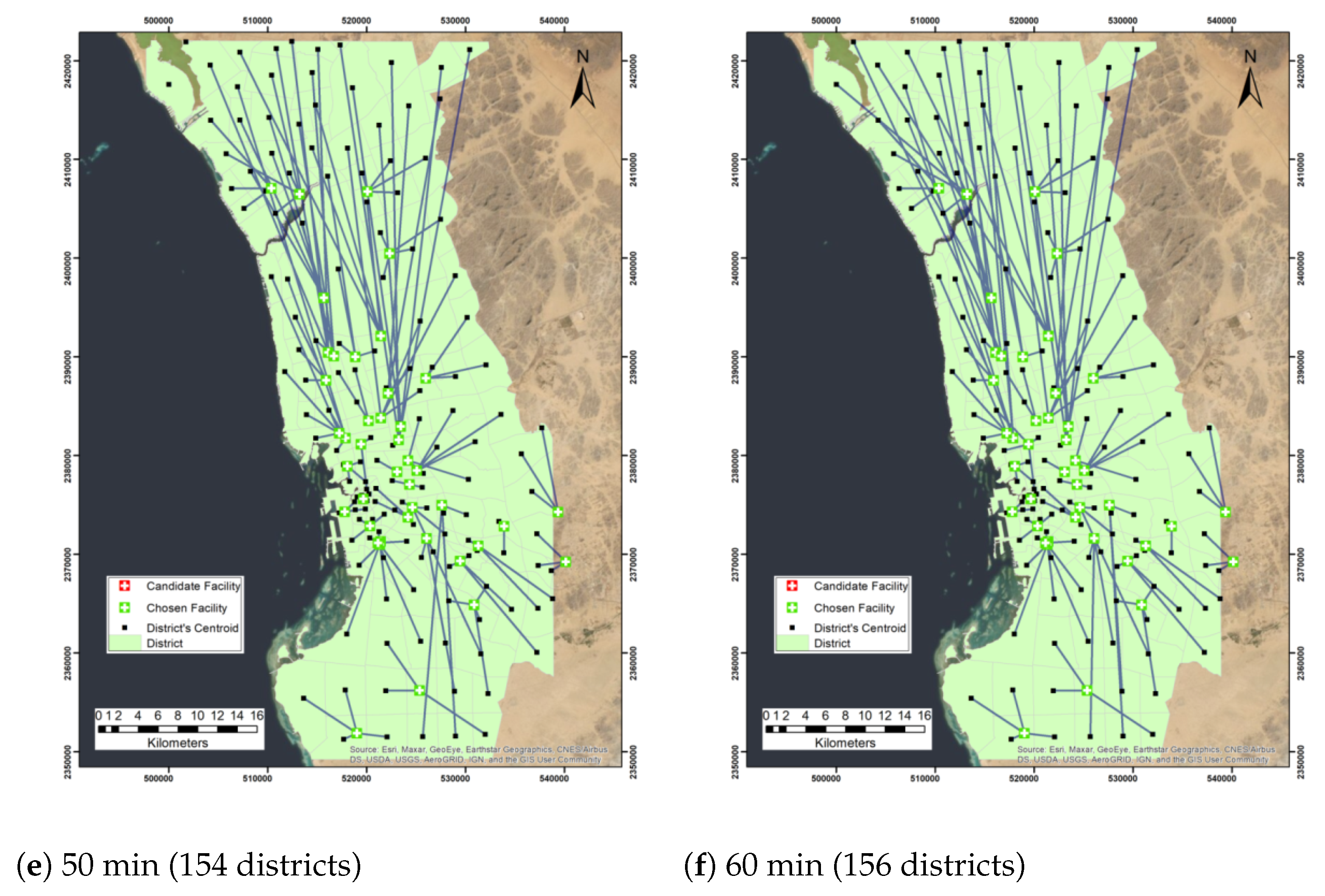
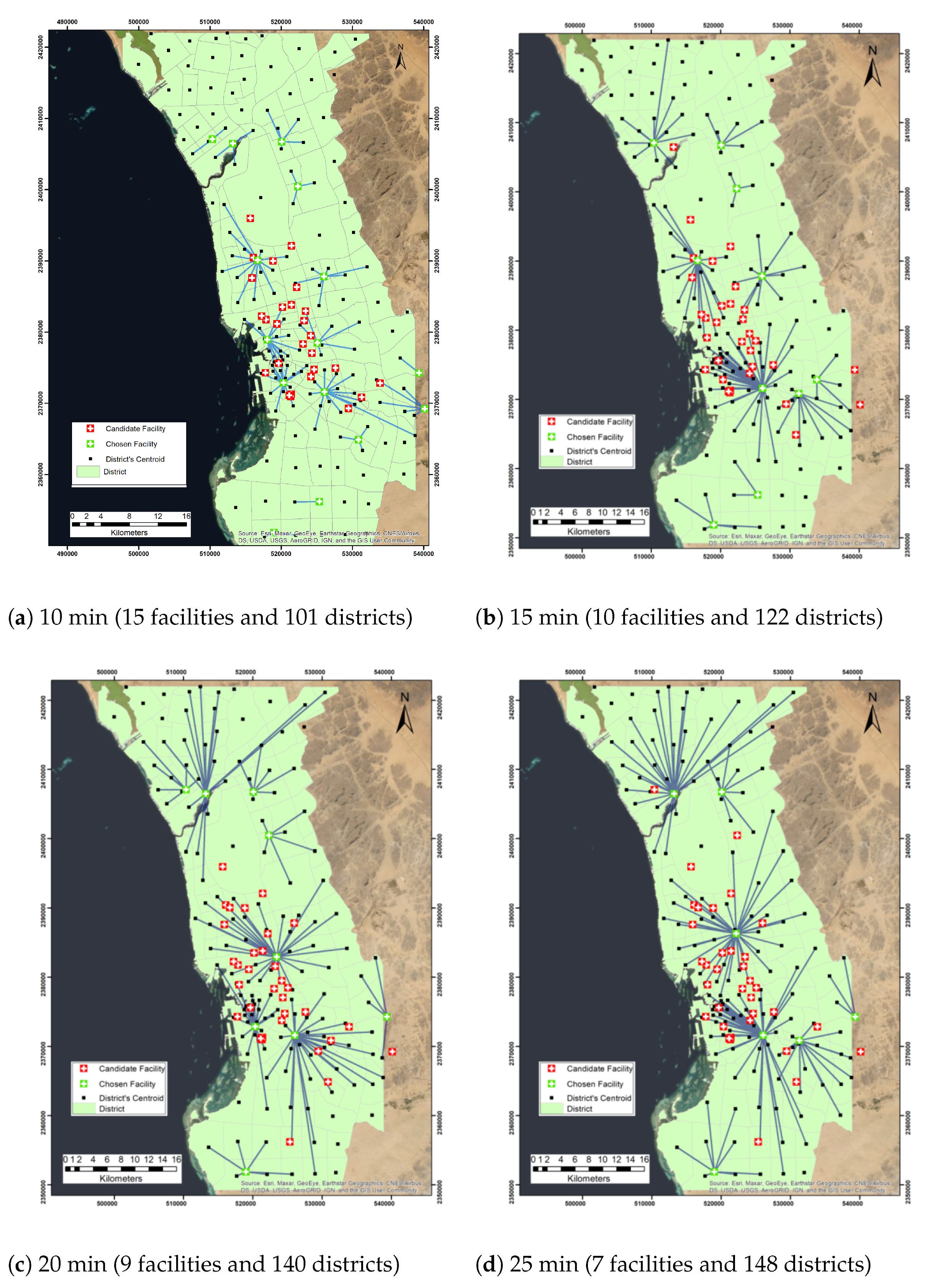
4.3. Minimizing Facilities
- Facilities are uncapacitated.
- The impedance is based on time in minutes.
- The travel type is from demand point to facility.
- The impedance transformation is linear.
- Roads are bidirectional.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, S.; Richter, A. Dispensing mass prophylaxis? The search for the perfect solution. Homel. Secur. Aff. 2012, 8, 3. [Google Scholar]
- Rahman, S.; Smith, D.K. Deployment of rural health facilities in a developing country. J. Oper. Res. Soc. 1999, 50, 892–902. [Google Scholar] [CrossRef]
- Alghanmi, N.; Alotaibi, R.; Alshammari, S.; Alhothali, A.; Bamasag, O.; Faisal, K. A Survey of Location-Allocation of Points of Dispensing During Public Health Emergencies. Front. Public Health 2022, 10, 811858. [Google Scholar] [CrossRef] [PubMed]
- Dasaklis, T.K.; Pappis, C.P.; Rachaniotis, N.P. Epidemics control and logistics operations: A review. Int. J. Prod. Econ. 2012, 139, 393–410. [Google Scholar] [CrossRef]
- Rahman, S.U.; Smith, D.K. Use of Location-Allocation Models in Health Service Development Planning in Developing Nations. Eur. J. Oper. Res. 2000, 123, 437–452. [Google Scholar] [CrossRef]
- Jia, H.; Ordóñez, F.; Dessouky, M. A modeling framework for facility location of medical services for large-scale emergencies. IIE Trans. 2007, 39, 41–55. [Google Scholar] [CrossRef]
- Brimberg, J.; Drezner, Z.; Mladenović, N.; Salhi, S. A new local search for continuous location problems. Eur. J. Oper. Res. 2014, 232, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Mestre, A.M.; Oliveira, M.D.; Barbosa-Póvoa, A.P. Location–allocation approaches for hospital network planning under uncertainty. Eur. J. Oper. Res. 2015, 240, 791–806. [Google Scholar] [CrossRef]
- Hepbasli, A.; Biyik, E.; Ekren, O.; Gunerhan, H.; Araz, M. A key review of wastewater source heat pump (WWSHP) systems. Energy Convers. Manag. 2014, 88, 700–722. [Google Scholar] [CrossRef]
- Cardoso, T.; Oliveira, M.D.; Barbosa-Póvoa, A.P.; Nickel, S. Modeling inter-sector health policy options and health gains in a long-term care network: A location-allocation stochastic planning approach. In Operations Research and Big Data; Springer: Berlin/Heidelberg, Germany, 2015; pp. 23–31. [Google Scholar]
- Zahiri, B.; Tavakkoli-Moghaddam, R.; Pishvaee, M.S. A robust possibilistic programming approach to multi-period location–allocation of organ transplant centers under uncertainty. Comput. Ind. Eng. 2014, 74, 139–148. [Google Scholar] [CrossRef]
- Wang, L.; Shi, H.; Gan, L. Healthcare facility location-allocation optimization for China’s developing cities utilizing a multi-objective decision support approach. Sustainability 2018, 10, 4580. [Google Scholar] [CrossRef] [Green Version]
- Kaveh, M.; Kaveh, M.; Mesgari, M.S.; Paland, R.S. Multiple criteria decision-making for hospital location-allocation based on improved genetic algorithm. Appl. Geomat. 2020, 12, 291–306. [Google Scholar] [CrossRef]
- Hajipour, V.; Fattahi, P.; Tavana, M.; Di Caprio, D. Multi-objective multi-layer congested facility location-allocation problem optimization with Pareto-based meta-heuristics. Appl. Math. Model. 2016, 40, 4948–4969. [Google Scholar] [CrossRef]
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts in Shenzhen, China: A retrospective cohort study. Lancet Infect. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- WHO. WHO Director-General’s Remarks at the Media Briefing on 2019-ncov on 11 February 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. WHO Coronavirus (COVID-19) Dashboard; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Yin, L.; Zhang, H.; Li, Y.; Liu, K.; Chen, T.; Luo, W.; Lai, S.; Li, Y.; Tang, X.; Ning, L.; et al. Effectiveness of Contact Tracing, Mask Wearing and Prompt Testing on Suppressing COVID-19 Resurgences in Megacities: An Individual-Based Modelling Study; SSRN: Rochester, NY, USA, 2020. [Google Scholar]
- Andreadakis, Z.; Kumar, A.; Román, R.G.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar]
- Li, X.; Zhao, Z.; Zhu, X.; Wyatt, T. Covering models and optimization techniques for emergency response facility location and planning: A review. Math. Methods Oper. Res. 2011, 74, 281–310. [Google Scholar] [CrossRef]
- Ahmadi-Javid, A.; Seyedi, P.; Syam, S.S. A survey of healthcare facility location. Comput. Oper. Res. 2017, 79, 223–263. [Google Scholar] [CrossRef]
- Rahman, M.; Chen, N.; Islam, M.M.; Dewan, A.; Pourghasemi, H.R.; Washakh, R.M.A.; Nepal, N.; Tian, S.; Faiz, H.; Alam, M.; et al. Location-allocation modeling for emergency evacuation planning with GIS and remote sensing: A case study of Northeast Bangladesh. Geosci. Front. 2021, 12, 101095. [Google Scholar] [CrossRef]
- Rahmaniani, R.; Rahmaniani, G.; Jabbarzadeh, A. Variable neighborhood search based evolutionary algorithm and several approximations for balanced location–allocation design problem. Int. J. Adv. Manuf. Technol. 2014, 72, 145–159. [Google Scholar] [CrossRef]
- Zhang, W.; Cao, K.; Liu, S.; Huang, B. A multi-objective optimization approach for health-care facility location-allocation problems in highly developed cities such as Hong Kong. Comput. Environ. Urban Syst. 2016, 59, 220–230. [Google Scholar] [CrossRef]
- Beheshtifar, S.; Alimoahmmadi, A. A multiobjective optimization approach for location-allocation of clinics. Int. Trans. Oper. Res. 2015, 22, 313–328. [Google Scholar] [CrossRef]
- Zahiri, B.; Torabi, S.; Mousazadeh, M.; Mansouri, S. Blood collection management: Methodology and application. Appl. Math. Model. 2015, 39, 7680–7696. [Google Scholar] [CrossRef]
- Ezugwu, A.E.; Olusanya, M.O.; Govender, P. Mathematical model formulation and hybrid metaheuristic optimization approach for near-optimal blood assignment in a blood bank system. Expert Syst. Appl. 2019, 137, 74–99. [Google Scholar] [CrossRef]
- Elalouf, A.; Hovav, S.; Tsadikovich, D.; Yedidsion, L. Minimizing operational costs by restructuring the blood sample collection chain. Oper. Res. Health Care 2015, 7, 81–93. [Google Scholar] [CrossRef]
- Saveh-Shemshaki, F.; Shechter, S.; Tang, P.; Isaac-Renton, J. Setting sites for faster results: Optimizing locations and capacities of new tuberculosis testing laboratories. IIE Trans. Healthc. Syst. Eng. 2012, 2, 248–258. [Google Scholar] [CrossRef]
- Doerner, K.; Focke, A.; Gutjahr, W.J. Multicriteria tour planning for mobile healthcare facilities in a developing country. Eur. J. Oper. Res. 2007, 179, 1078–1096. [Google Scholar] [CrossRef] [Green Version]
- Syam, S.S.; Côté, M.J. A comprehensive location-allocation method for specialized healthcare services. Oper. Res. Health Care 2012, 1, 73–83. [Google Scholar] [CrossRef]
- Hood, K.B.; Robertson, A.A.; Baird-Thomas, C. Implementing solutions to barriers to on-site HIV testing in substance abuse treatment: A tale of three facilities. Eval. Program Plan. 2015, 49, 1–9. [Google Scholar] [CrossRef]
- Chan, T.C.; Demirtas, D.; Kwon, R.H. Optimizing the deployment of public access defibrillators. Manag. Sci. 2016, 62, 3617–3635. [Google Scholar] [CrossRef] [Green Version]
- Silva, F.; Serra, D. Locating emergency services with different priorities: The priority queuing covering location problem. J. Oper. Res. Soc. 2008, 59, 1229–1238. [Google Scholar] [CrossRef]
- Sha, Y.; Huang, J. The multi-period location-allocation problem of engineering emergency blood supply systems. Syst. Eng. Procedia 2012, 5, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Gao, X.; Zhou, Y.; Amir, M.I.H.; Rosyidah, F.A.; Lee, G.M. A hybrid genetic algorithm for multi-emergency medical service center location-allocation problem in disaster response. Int. J. Ind. Eng. 2017, 24, 663–679. [Google Scholar]
- Beraldi, P.; Bruni, M.E.; Conforti, D. Designing robust emergency medical service via stochastic programming. Eur. J. Oper. Res. 2004, 158, 183–193. [Google Scholar] [CrossRef]
- Kaveh, M.; Mesgari, M.S. Improved biogeography-based optimization using migration process adjustment: An approach for location-allocation of ambulances. Comput. Ind. Eng. 2019, 135, 800–813. [Google Scholar] [CrossRef]
- Sharma, B.; Ramkumar, M.; Subramanian, N.; Malhotra, B. Dynamic temporary blood facility location-allocation during and post-disaster periods. Ann. Oper. Res. 2019, 283, 705–736. [Google Scholar] [CrossRef]
- Oksuz, M.K.; Satoglu, S.I. A two-stage stochastic model for location planning of temporary medical centers for disaster response. Int. J. Disaster Risk Reduct. 2020, 44, 101426. [Google Scholar] [CrossRef]
- Drezner, T. Location of casualty collection points. Environ. Plan. Gov. Policy 2004, 22, 899–912. [Google Scholar] [CrossRef]
- Apte, A.; Heidtke, C.; Salmerón, J. Casualty collection points optimization: A study for the district of columbia. Interfaces 2015, 45, 149–165. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.K.; Chen, C.H.; Pietz, F.; Benecke, B. Modeling and optimizing the public-health infrastructure for emergency response. Interfaces 2009, 39, 476–490. [Google Scholar] [CrossRef]
- Ramirez-Nafarrate, A.; Lyon, J.D.; Fowler, J.W.; Araz, O.M. Point-of-dispensing location and capacity optimization via a decision support system. Prod. Oper. Manag. 2015, 24, 1311–1328. [Google Scholar] [CrossRef]
- Araz, O.M.; Fowler, J.W.; Nafarrate, A.R. Optimizing service times for a public health emergency using a genetic algorithm: Locating dispensing sites and allocating medical staff. IIE Trans. Healthc. Syst. Eng. 2014, 4, 178–190. [Google Scholar] [CrossRef]
- Toregas, C.; Swain, R.; ReVelle, C.; Bergman, L. The location of emergency service facilities. Oper. Res. 1971, 19, 1363–1373. [Google Scholar] [CrossRef]
- Baray, J.; Cliquet, G. Optimizing locations through a maximum covering/p-median hierarchical model: Maternity hospitals in France. J. Bus. Res. 2013, 66, 127–132. [Google Scholar] [CrossRef]
- McCormack, R.; Coates, G. A simulation model to enable the optimization of ambulance fleet allocation and base station location for increased patient survival. Eur. J. Oper. Res. 2015, 247, 294–309. [Google Scholar] [CrossRef] [Green Version]
- Shishebori, D.; Yousefi Babadi, A.; Noormohammadzadeh, Z. A Lagrangian relaxation approach to fuzzy robust multi-objective facility location network design problem. Sci. Iran. 2018, 25, 1750–1767. [Google Scholar] [CrossRef] [Green Version]
- Bertsimas, D.; Tsitsiklis, J. Simulated annealing. Stat. Sci. 1993, 8, 10–15. [Google Scholar] [CrossRef]
- De Campos, M.V.A.; de Sá, M.V.S.M.; Rosa, P.M.; Penna, P.H.V.; de Souza, S.R.; Souza, M.J.F. A Mixed Linear Integer Programming Formulation and a Simulated Annealing Algorithm for the Mammography Unit Location Problem. In Proceedings of the ICEIS, Prague, Czech Republic, 5–7 May 2020; pp. 428–439. [Google Scholar]
- ElKady, S.K.; Abdelsalam, H.M. A modified particle swarm optimization algorithm for solving capacitated maximal covering location problem in healthcare systems. In Applications of Intelligent Optimization in Biology and Medicine; Springer: Berlin/Heidelberg, Germany, 2016; pp. 117–133. [Google Scholar]
- Murali, P.; Ordóñez, F.; Dessouky, M.M. Facility location under demand uncertainty: Response to a large-scale bio-terror attack. Soc. Econ. Plan. Sci. 2012, 46, 78–87. [Google Scholar] [CrossRef]
- Manupati, V.K.; Schoenherr, T.; Wagner, S.M.; Soni, B.; Panigrahi, S.; Ramkumar, M. Convalescent plasma bank facility location-allocation problem for COVID-19. Transp. Res. Part Logist. Transp. Rev. 2021, 156, 102517. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Zhou, S.; Zheng, Z.; Lu, J. Optimizing spatial allocation of COVID-19 vaccine by agent-based spatiotemporal simulations. GeoHealth 2021, 5, e2021GH000427. [Google Scholar] [CrossRef] [PubMed]
- Tomé, T.; De Oliveira, M.J. Susceptible-infected-recovered and susceptible-exposed-infected models. J. Phys. Math. Theor. 2011, 44, 095005. [Google Scholar] [CrossRef]
- Tavana, M.; Govindan, K.; Nasr, A.K.; Heidary, M.S.; Mina, H. A mathematical programming approach for equitable COVID-19 vaccine distribution in developing countries. Ann. Oper. Res. 2021, 1–34. [Google Scholar] [CrossRef]
- Lusiantoro, L.; Mara, S.T.W.; Rifai, A.P. A Locational Analysis Model of the COVID-19 Vaccine Distribution. Oper. Supply Chain. Manag. 2022, 15, 240–250. [Google Scholar] [CrossRef]
- Kuvvetli, Y. A goal programming model for two-stage COVID19 test sampling centers location-allocation problem. Cent. Eur. J. Oper. Res. 2022, 1–20. [Google Scholar] [CrossRef]
- Faisal, K.; Alshammari, S.; Alotaibi, R.; Alhothali, A.; Bamasag, O.; Alghanmi, N.; Bin Yamin, M. Spatial Analysis of COVID-19 Vaccine Centers Distribution: A Case Study of the City of Jeddah, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 3526. [Google Scholar] [CrossRef]
- Polo, G.; Acosta, C.M.; Ferreira, F.; Dias, R.A. Location-allocation and accessibility models for improving the spatial planning of public health services. PLoS ONE 2015, 10, e0119190. [Google Scholar] [CrossRef] [Green Version]
- Church, R.L.; Gerrard, R.A. The multi-level location set covering model. Geogr. Anal. 2003, 35, 277–289. [Google Scholar] [CrossRef]
- Dijkstra, E.W. A note on two problems in connexion with graphs. Numer. Math. 1959, 1, 269–271. [Google Scholar] [CrossRef] [Green Version]
- Hillsman, E.L. The p-median structure as a unified linear model for location—Allocation analysis. Environ. Plan. A 1984, 16, 305–318. [Google Scholar] [CrossRef]
- Teitz, M.B.; Bart, P. Heuristic methods for estimating the generalized vertex median of a weighted graph. Oper. Res. 1968, 16, 955–961. [Google Scholar] [CrossRef]
- Church, R.; ReVelle, C. The maximal covering location problem. Pap. Reg. Sci. 1974, 32, 101–118. [Google Scholar] [CrossRef]
- Current, J.R.; Storbeck, J.E. Capacitated Covering Models. Environ. Plan. Plan. Des. 1988, 15, 153–163. [Google Scholar] [CrossRef]
- Chung, C.; Schilling, D.; Carbone, R. The capacitated maximal covering problem: A heuristic solution. Model. Simul. 1983, 14, 1383–1388. [Google Scholar]
- Özceylan, E.; Uslu, A.; Erbaş, M.; Çetinkaya, C.; İşleyen, S.K. Optimizing the location-allocation problem of pharmacy warehouses: A case study in Gaziantep. Int. J. Optim. Control. Theor. Appl. IJOCTA 2017, 7, 117–129. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Facility’s Name | Vaccine Type | x | y |
|---|---|---|---|
| King Abdulaziz Airport | Pfizer | 515,688 | 2,395,991 |
| King Abdulaziz University | Pfizer | 524,344 | 2,377,067 |
| Maternity and Children’s Hospital | Pfizer | 517,872 | 2,381,778 |
| Jeddah field hospital | Pfizer | 516,132 | 2,390,450 |
| Specialized clinics Comprehensive National Guard | Pfizer | 523,252 | 2,381,605 |
| International Medical Center Hospital | Pfizer | 518,054 | 2,378,941 |
| Prince Abdulmajeed PHC Center | AstraZeneca | 529,472 | 2,369,307 |
| King Abdullah Medical Complex | AstraZeneca | 510,369 | 2,407,092 |
| King Abdulaziz Hospital | AstraZeneca | 521,435 | 2,371,302 |
| Al Mahgar Medical Center | AstraZeneca | 521,359 | 2,370,983 |
| Obhur Medical Center | AstraZeneca | 513,239 | 2,406,473 |
| Health Centre AlBawadi | AstraZeneca | 516,702 | 2,390,092 |
| District Name | x Centroid (m) | y Centroid (m) |
|---|---|---|
| Al Thagur | 523,617 | 2,375,293 |
| Al Sharafeyyah | 519,394 | 2,379,374 |
| Al Azizeyyah | 520,155 | 2,383,348 |
| Al Dahyh | 521,946 | 2,356,167 |
| Al Naeem | 514,888 | 2,391,636 |
| Al Ajaweed | 532,149 | 2,366,756 |
| Al Khaledeyyah | 513,925 | 2,384,152 |
| Al Basateen | 512,025 | 2,397,900 |
| Al Wazeereyyah | 524,073 | 2,371,332 |
| Al Rabbwah | 518,856 | 2,388,693 |
| Al Faysaleyyah | 519,020 | 2,385,444 |
| Al Ameer Fawaz Al Shamaly | 531,195 | 2,370,382 |
| Al Hada | 531,444 | 2,363,401 |
| Al Ameer Abdoulmajjed | 528,407 | 2,368,760 |
| Al Sahefah | 520,266 | 2,376,112 |
| Al Gharbeyah | 512,434 | 2,421,965 |
| Al Zohor | 510,880 | 2,421,238 |
| Al Hazazia | 514,508 | 2,418,802 |
| Al Eusala | 532,077 | 2,389,199 |
| Betrumeen | 520,328 | 2,371,655 |
| Al Hamadhnyah | 520,046 | 2,405,711 |
| Al Barakah | 529,009 | 2,351,588 |
| Al Mountazahat | 530,106 | 2,374,006 |
| Al Samer | 525,395 | 2,386,573 |
| Al Worood | 521,071 | 2,379,535 |
| Al Bashaer | 518,079 | 2,411,159 |
| Al Sheraa | 509,818 | 2,406,800 |
| Al Ammareyyah | 520,031 | 2,376,598 |
| Al Kandarah | 520,956 | 2,376,690 |
| Impedance Cutoff | No. of Facilities | No. of Districts |
|---|---|---|
| 10 | 37 | 101 |
| 20 | 37 | 140 |
| 30 | 37 | 155 |
| 40 | 37 | 156 |
| 50 | 37 | 156 |
| 60 | 37 | 156 |
| Impedance Cutoff | Capacity = 3 Districts | Capacity = 4 Districts | ||
|---|---|---|---|---|
| No. of Facilities | No. of Districts | No. of Facilities | No. of Districts | |
| 10 | 39 | 94 | 38 | 98 |
| 20 | 41 | 112 | 38 | 119 |
| 30 | 42 | 124 | 39 | 135 |
| 40 | 42 | 126 | 42 | 149 |
| 50 | 42 | 126 | 42 | 154 |
| 60 | 42 | 126 | 42 | 156 |
| Impedance Cutoff | No. of Facilities | No. of Districts |
|---|---|---|
| 10 | 15 | 101 |
| 15 | 10 | 122 |
| 20 | 9 | 140 |
| 25 | 7 | 148 |
| 30 | 5 | 155 |
| 40 | 2 | 156 |
| No. | Facility Name | Minimize Facilities | Maximize Coverage | MCC Capacity 3 | MCC Capacity 4 | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 15 | 20 | 25 | 30 | 40 | 10 | 20 | 30 | 40 | 50 | 60 | 10 | 20 | 30 | 40 | 50 | 60 | 10 | 20 | 30 | 40 | 50 | 60 | ||
| 1 | King Abdulaziz Airport | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| 2 | King Abdulaziz University | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 3 | Maternity and Children’s Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 4 | Jeddah field hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 5 | Comprehensive National Guard | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 6 | International Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 7 | Prince Abdulmajeed PHC Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 8 | King Abdullah Medical Complex | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| 9 | King Abdulaziz Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| 10 | Al Mahgar Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 11 | Obhur Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| 12 | Health Centre AlBawadi | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| 13 | Al Thaghr Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| 14 | Ophthalmology Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 15 | King Fahad General Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||||||
| 16 | East Jeddah General Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| 17 | Mental health hospital in Jeddah | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 18 | Al Majed Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| 19 | University District PHC Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 20 | Al Aziziyah M and C Hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||||||
| 21 | Tayba Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 22 | Al Rayan Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| 23 | Madain Al Fahd Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 24 | Al Balad Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 25 | Al Thaalba Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| 26 | Al Qryniah Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| 27 | Al Qwizain Medical Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| 28 | Al Rabwah PHC Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 29 | Al Azziziyah Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 30 | Al Mishrifah Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| 31 | Al Salamah Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 32 | Al Marwah Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 33 | Health Center East of The Highway | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| 34 | Al Rawabi Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 35 | Al Rehab Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 36 | Al Harazat Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| 37 | Kilo 14 Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 38 | Old Airport Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 39 | Umm Al Salam Health Center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| 40 | Health Surveillance Center JIP | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 41 | Al Salaam Mall | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| 42 | Prince Abdullah Al Faisal Stadium | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhothali, A.; Alwated, B.; Faisal, K.; Alshammari, S.; Alotaibi, R.; Alghanmi, N.; Bamasag, O.; Bin Yamin, M. Location-Allocation Model to Improve the Distribution of COVID-19 Vaccine Centers in Jeddah City, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 8755. https://doi.org/10.3390/ijerph19148755
Alhothali A, Alwated B, Faisal K, Alshammari S, Alotaibi R, Alghanmi N, Bamasag O, Bin Yamin M. Location-Allocation Model to Improve the Distribution of COVID-19 Vaccine Centers in Jeddah City, Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(14):8755. https://doi.org/10.3390/ijerph19148755
Chicago/Turabian StyleAlhothali, Areej, Budoor Alwated, Kamil Faisal, Sultanah Alshammari, Reem Alotaibi, Nusaybah Alghanmi, Omaimah Bamasag, and Manal Bin Yamin. 2022. "Location-Allocation Model to Improve the Distribution of COVID-19 Vaccine Centers in Jeddah City, Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 14: 8755. https://doi.org/10.3390/ijerph19148755
APA StyleAlhothali, A., Alwated, B., Faisal, K., Alshammari, S., Alotaibi, R., Alghanmi, N., Bamasag, O., & Bin Yamin, M. (2022). Location-Allocation Model to Improve the Distribution of COVID-19 Vaccine Centers in Jeddah City, Saudi Arabia. International Journal of Environmental Research and Public Health, 19(14), 8755. https://doi.org/10.3390/ijerph19148755