Abstract
Adiposity rebound (AR), which is defined as a situation in which the body mass index (BMI) starts to increase after infancy, is a predictive marker of future development of type 2 diabetes. The patient was a 20-year-old male. He was born at 28 gestational weeks with a birthweight of 642 g (−3.20 standard deviation, small-for-gestational age [SGA]). AR during early childhood or obesity in later childhood was not observed. At the onset of type 2 diabetes (20 years of age), his BMI, body fat percentage, and body fat mass were within normal ranges (20.4, 18.4% and 10.8 kg, respectively). However, his muscle mass was 44.7 kg, with low muscle mass of the trunk and upper limbs, which was lower than the standard reference, indicating that myogenic insulin resistance was involved in the development of non-obese type 2 diabetes. This case report describes a patient with no presentation of AR and obesity during childhood, who was born extremely preterm SGA, developed non-obese type 2 diabetes with low muscle mass. We suggest that patients born extremely preterm SGA should be carefully observed for the development of type 2 diabetes, even if they did not have AR in early childhood or had not become obese.
1. Introduction
Small-for-gestational-age (SGA) infants, who have restricted growth in utero resulting in low birthweight, are at high risk of lifestyle-related diseases, such as hypertension, hyperlipidemia, and type 2 diabetes mellitus in adulthood after developing obesity [1]. Predictive markers in childhood have attracted attention and have been studied worldwide to prevent lifestyle-related diseases. Adiposity rebound (AR), which is defined as a situation in which the body mass index (BMI) starts to increase after infancy, has been found to be a promising factor for prediction [2,3,4,5,6,7,8,9]. The early timing of AR has been reported to be related to the development of obesity, metabolic syndrome, and type 2 diabetes mellitus [2,3,4,5,6,7,8], especially when AR occurs before the age of five years (early AR) [3]. For example, Barker et al. reported that low BMI until two years of age and marked increase in BMI after two years of age constituted high-risk conditions for ischemic heart disease in adults [2]. Arisaka et al. reported that children with AR before three years of age have increased insulin resistance at 12 years of age, compared with those with AR after three years of age [8].
Our previous study found that growth patterns during infancy and early childhood in SGA infants differed by gestational age at birth [9]. We suggested that early AR may be a predictive marker for the development of obesity, metabolic syndrome, or type 2 diabetes in term SGA infants, but not preterm SGA infants. We hypothesized that patients born preterm SGA develop lifestyle-related diseases without presenting early AR.
We report here the case of a 20-year-old male patient who developed non-obese type 2 diabetes and was born as an extremely preterm SGA infant. This patient did not exhibit early AR and developed non-obese type 2 diabetes due to low muscle mass. This observation was different from previous reports where patients with early AR developed obese type 2 diabetes due to increased fat mass [2,3,4,5,6,7,8].
2. Case Presentation
2.1. Clinical Course and Condition
The patient was a Japanese 20-year-old male. His blood type was type A and Rhesus D positive. He was born by Cesarean section at 28 weeks and two days of gestation as an SGA infant. His birthweight was 642 g (−3.20 standard deviation [SD]), and his birth height and head circumference were 31.5 cm (−2.38 SD) and 24.2 cm (−0.87 SD), showing an asymmetrical SGA. SGA was caused by hypertensive disorders during pregnancy. Severe hypoglycemia or hyperglycemia was not observed during his stay in the neonatal intensive care unit. Regarding diseases related to extremely preterm birth, retinopathy of prematurity recovered without any treatment. No chronic lung disease developed. The head magnetic resonance imaging and auditory brainstem response test were normal at term-equivalent age. At three years of age, the patient’s developmental quotient, according to the Kyoto scale of psychological development, was 91 (standard range: ≥85). At six years of age, his intelligence quotient, measured using the Wechsler intelligence scale for children-III, was 82 (standard range: ≥80).
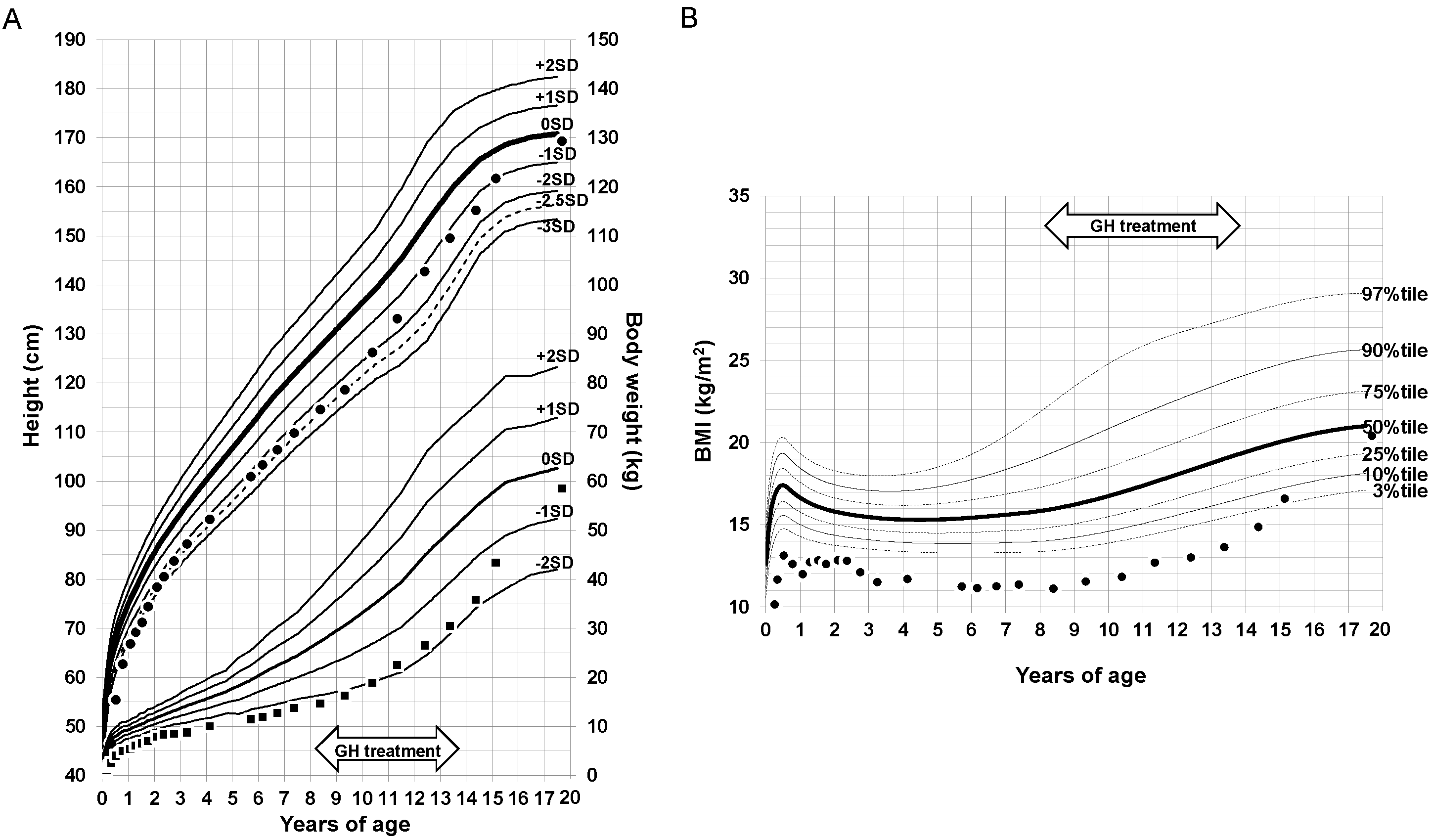
The patient’s height and body weight growth curve and BMI transition are shown in Figure 1A,B. Early AR or obesity was not observed in his infancy, childhood, or school age. Because of the severe short stature in children born SGA, the patient received growth hormone (GH) treatment from 8 to 14 years of age. Effective height responses were observed, and no abnormal blood glucose levels were found during the GH treatment. After discontinuing the treatment, the patient’s body weight and BMI gradually increased and type 2 diabetes without obesity developed.
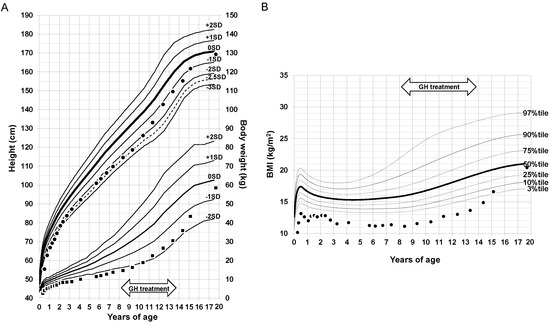
Figure 1.
Growth curve of height and body weight from birth to the onset of diabetes. (A) Height and body weight. ●: height of the patient, ■: body weight of the patient. (B) Body mass index. ●: BMI of the patient. BMI, body mass index; GH, growth hormone; SD, standard deviation.
The patient visited his family physician with a primary complaint of pain when urinating. A urinalysis revealed positive urine glucose levels (4+); hence, he was referred to a diabetologist. At the time of admission (20 years of age), the patient’s height, body weight, and BMI were 169.3 cm, 58.5 kg, and 20.4, respectively. His blood pressure was 101/70 mmHg; the detailed laboratory examination results are shown in Table 1. His fasting blood glucose and HbA1c levels were 175 mg/dL and 11.6%, respectively. The serum total cholesterol and non-high-density lipoprotein cholesterol levels were high (223 mg/dL and 172 mg/dL, respectively). Serum liver enzyme levels and renal function levels were within normal ranges. The insulin response on a glucagon load test and urinary storage connecting peptide immunoreactivity test was normal. The results were negative for anti-glutamic acid decarboxylase antibody and anti-insulinoma-associated antigen-2 antibody. Based on these results, the patient was diagnosed with type 2 diabetes.

Table 1.
Laboratory data.
The patient’s body composition analyses using an InBody s10® (medical device approval number: 223AFBZX00130000; InBody Japan Inc., Tokyo, Japan) at the onset of diabetes are shown in Table 2. His body fat percentage and body fat mass were within normal ranges (18.4% and 10.8 kg, respectively). However, the patient’s total muscle mass was 44.7 kg, which was low compared with the standard range, especially those of the upper limbs and trunk. Low muscle mass without significant fat accumulation was confirmed.
Table 2.
Body composition analysis.
2.2. Treatments
Soon after diagnosis, the patient started diet therapy (1760 kcal/day) and insulin therapy (38 units/day). Five weeks after starting the treatments, his HbA1c levels improved to 9.1%; insulin therapy was reduced to 26 units/day, and oral metformin administration was started (500 mg/day). Seven weeks later, the patient’s HbA1c level was 7.3% and his glycemic control further improved. His insulin dose was reduced to 17 units/day and metformin dose was increased to 1000 mg/day. Insulin therapy will be withdrawn in the future. To treat hyperlipidemia, rosuvastatin (2.5 mg/day) was also started, after which the patient’s non-high-density lipoprotein cholesterol level improved to 122 mg/dL.
3. Discussion
We reported a patient who was born extremely preterm SGA and developed non-obese type 2 diabetes at the age of 20 years. Surprisingly, early AR or obesity was not observed in his infancy, childhood, or school age. However, low total muscle mass, without significant fat accumulation, was noted at diabetes onset. This was a different clinical course and condition from reports of previous studies that SGA infants are more likely to develop type 2 diabetes when they become obese [2,3,4,5,6,7,8].
A relationship between the transition of BMI in childhood and the future onset of type 2 diabetes has been reported [3]. Generally, AR is defined when BMI decreases in early childhood and begins to increase at approximately five to six years of age. The appearance of AR earlier than five years of age is associated with future onset of obesity and type 2 diabetes [3]. A recent study reported that extremely preterm SGA children did not catch up in height or body weight until around six years of age [10]. In our case, the BMI remained low until the onset of type 2 diabetes, but it began developing at a young adult age. Even when early AR and obesity are not observed in extremely preterm SGA children, type 2 diabetes may develop.
Skeletal muscle is the main organ that insulin acts on to take up glucose, and accounts for approximately 70% of the total glucose processing capacity of the body [11]. Insulin resistance in the skeletal muscle results in conversion of ingested carbohydrates into lipids (de novo lipogenesis) in the liver rather than glycogen in muscle [11]. Recent reports showed that extremely preterm infants exhibited insulin resistance until adulthood [12,13]. A human study including 100 adults with an average age of 32 years who were born with an extremely low birthweight reported a four-fold risk of developing impaired glucose tolerance, compared with adults born at term [12]. Another human study involving 163 preterm-born adults found that insulin resistance was significantly higher than that in term-born adults [13]. It has been speculated that patients born preterm and with extremely low birthweight have lesser lean body mass (mainly muscle mass) than term-born patients [14]. A basic study using mice showed that dysgenesis at birth led to decreased muscle volume and degeneration of muscle composition during adulthood. This was associated with insulin resistance [15]. Our patient exhibited a normal range of fat mass but a decrease in muscle mass. Kaga et al., found that healthy non-obese males have low muscle insulin sensitivity [16]. Myogenic insulin resistance may be involved in the development of non-obese type 2 diabetes in patients born as extremely preterm SGA infants.
Tajiri et al., reported that reduction in skeletal muscle mass, especially in the lower limbs, is associated with insulin resistance in Japanese type 2 diabetes patients [17]. In this case, the muscle masses of the trunk and upper limbs were small, but the muscle mass of the lower limbs was relatively large. Chao et al., have also shown that upper limb circumference can be an indicator of insulin resistance in non-obese elderly individuals [18]. Low muscle mass of the trunk or upper limbs may also be associated with insulin resistance.
In general, the accumulation of visceral fat is more strongly associated with insulin resistance than that of subcutaneous fat [19,20]. Even if the amount of fat is the same, insulin resistance depends on the type of fat (visceral fat or subcutaneous fat). In our case, the body composition analyzer showed normal fat mass; however, the distribution of visceral fat and subcutaneous fat could not be evaluated, which is a limitation of this case study.
This case was treated with GH from 8 to 14 years of age due to severe SGA short stature. There are currently debates regarding the association between long-term GH treatment and the development of diabetes. Many studies have found that GH treatment was not related to insulin resistance or abnormal sensitivity [21,22,23]. However, some have reported that GH treatment reduced insulin sensitivity [24]. In healthy older subjects, GH administration for 26 weeks impaired insulin sensitivity in the liver, but not in skeletal muscle [25]. Although we considered that the development of type 2 diabetes was not caused by GH treatment in this case, because no abnormal blood glucose levels were found during the GH treatment and six years had already passed after the end of the treatment, long-term GH treatment might have been involved in the pathogenesis. Further studies using more patients are needed to determine this.
4. Conclusions
This is the first report of a patient who was born extremely preterm SGA who did not have AR during early childhood but developed non-obese type 2 diabetes with significant decrease in muscle mass. Insulin resistance due to decrease in muscle mass, not fat accumulation, might account for the pathogenesis. Patients born extremely preterm SGA should be carefully observed for the development of type 2 diabetes, even without obesity or early AR. In particular, children with SGA short stature who received GH treatment should be followed-up regularly to monitor the potential development of type 2 diabetes after discontinuation of the treatment.
Author Contributions
Conceptualization, N.N., I.T. and I.M.; formal analysis, N.N. and C.K.; investigation, N.N., C.K., S.O., M.S., I.T. and K.M.; funding acquisition, N.N. writing—original draft preparation, N.N. and I.M.; writing—review and editing, C.K., S.O., M.S., I.T. and K.M.; visualization, N.N. and I.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Nihon University School of Medicine Alumni Association’s 60th anniversary fund research grant (2020), the Grants-in-Aid for Young Scientists (grant number: 19K20194) and Scientific Research (C) (grant number: 21K11582) of JSPS KAKENHI, and the Kawano Masanori Memorial Public Interest Incorporated Foundation for Promotion of Pediatrics (2022).
Institutional Review Board Statement
This case study was approved by the Ethics Committee of the Nihon University School of Medicine (no. RK-190910-3) and was carried out in accordance with the relevant guidelines and regulations.
Informed Consent Statement
Formal written informed consent was obtained from the patient and the patient’s parents.
Data Availability Statement
The data that support the findings of this case study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Barker, D.J.P.; Hales, C.N.; Fall, C.H.D.; Osmond, C.; Phipps, K.; Clark, P.M. Type 2 (Non-insulin Dependent) Diabetes Mellitus, Hypertension and Hyperlipidemia (Syndrome X); Relation to Reduced Fetal Growth. Diabetologia 1993, 36, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, D.J.P.; Osmond, C.; Forsén, T.J.; Kajantie, E.; Eriksson, J.G. Trajectories of Growth Among Children Who Have Coronary Events as Adults. N. Engl. J. Med. 2005, 353, 1802–1809. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.G.; Forsén, T.; Tuomilehto, J.; Osmond, C.; Barker, D.J. Early Adiposity Rebound in Childhood and Risk of Type 2 Diabetes in Adult Life. Diabetologia 2003, 46, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, S.K.; Sachdev, H.S.; Fall, C.H.; Osmond, C.; Lakshmy, R.; Barker, D.J.; Biswas, S.K.; Ramji, S.; Prabhakaran, D.; Reddy, K.S. Relation of Serial Changes in Childhood Body-Mass Index to Impaired Glucose Tolerance in Young Adulthood. N. Engl. J. Med. 2004, 350, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Rolland-Cachera, M.F.; Deheeger, M.; Bellisle, F.; Sempé, M.; Guilloud-Bataille, M.; Patois, E. Adiposity Rebound in Children: A Simple Indicator for Predicting Obesity. Am. J. Clin. Nutr. 1984, 39, 129–135. [Google Scholar] [CrossRef]
- Rolland-Cachera, M.F.; Deheeger, M.; Maillot, M.; Bellisle, F. Early Adiposity Rebound: Causes and Consequences for Obesity in Children and Adults. Int. J. Obes. 2006, 30 (Suppl. 4), S11–S17. [Google Scholar] [CrossRef] [Green Version]
- Koyama, S.; Ichikawa, G.; Kojima, M.; Shimura, N.; Sairenchi, T.; Arisaka, O. Adiposity Rebound and the Development of Metabolic Syndrome. Pediatrics 2014, 133, e114–e119. [Google Scholar] [CrossRef] [Green Version]
- Arisaka, O.; Sairenchi, T.; Ichikawa, G.; Koyama, S. Increase of Body Mass Index (BMI) from 1.5 to 3 Years of Age Augments the Degree of Insulin Resistance Corresponding to BMI at 12 Years of Age. J. Pediatr. Endocrinol. Metab. 2017, 30, 455–457. [Google Scholar] [CrossRef]
- Maeyama, K.; Morioka, I.; Iwatani, S.; Fukushima, S.; Kurokawa, D.; Yamana, K.; Nishida, K.; Ohyama, S.; Fujioka, K.; Awano, H.; et al. Gestational Age-Dependency of Height and Body Mass Index Trajectories During the First 3 Years in Japanese Small-for-Gestational Age Children. Sci. Rep. 2016, 6, 38659. [Google Scholar] [CrossRef]
- Shoji, H.; Murano, Y.; Nojiri, S.; Arai, Y.; Awata, K.; Ikeda, N.; Ohkawa, N.; Nishizaki, N.; Suganuma, H.; Hisata, K.; et al. Growth Trajectories During the First 6 Years in Survivors Born at Less Than 25 Weeks of Gestation Compared with Those Between 25 and 29 Weeks. J. Clin. Med. 2022, 11, 1418. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Tripathy, D. Skeletal Muscle Insulin Resistance Is the Primary Defect in Type 2 Diabetes. Diabetes Care 2009, 32 (Suppl. 2), S157–S163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, K.M.; Ramsingh, L.; Gunn, E.; Streiner, D.; Van Lieshout, R.; Boyle, M.; Gerstein, H.; Schmidt, L.; Saigal, S. Cardiometabolic Health in Adults Born Premature with Extremely Low Birth Weight. Pediatrics 2016, 138, e20160515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovi, P.; Andersson, S.; Eriksson, J.G.; Järvenpää, A.L.; Strang-Karlsson, S.; Mäkitie, O.; Kajantie, E. Glucose Regulation in Young Adults with Very Low Birth Weight. N. Engl. J. Med. 2007, 356, 2053–2063. [Google Scholar] [CrossRef] [PubMed]
- Giannì, M.L.; Roggero, P.; Piemontese, P.; Morlacchi, L.; Bracco, B.; Taroni, F.; Garavaglia, E.; Mosca, F. Boys Who Are Born Preterm Show a Relative Lack of Fat-Free Mass at 5 Years of Age Compared to Their Peers. Acta Paediatr. 2015, 104, e119–e123. [Google Scholar] [CrossRef] [PubMed]
- Beauchamp, B.; Ghosh, S.; Dysart, M.W.; Kanaan, G.N.; Chu, A.; Blais, A.; Rajamanickam, K.; Tsai, E.C.; Patti, M.E.; Harper, M.E. Low Birth Weight Is Associated with Adiposity, Impaired Skeletal Muscle Energetics and Weight Loss Resistance in Mice. Int. J. Obes. 2015, 39, 702–711. [Google Scholar] [CrossRef] [Green Version]
- Kaga, H.; Tamura, Y.; Takeno, K.; Kakehi, S.; Someya, Y.; Funayama, T.; Furukawa, Y.; Suzuki, R.; Sugimoto, D.; Kadowaki, S.; et al. Shape of the Glucose Response Curve During an Oral Glucose Tolerance Test Is Associated with Insulin Clearance and Muscle Insulin Sensitivity in Healthy Non-obese Men. J. Diabetes Investig. 2020, 11, 874–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajiri, Y.; Kato, T.; Nakayama, H.; Yamada, K. Reduction of Skeletal Muscle, Especially in Lower Limbs, in Japanese Type 2 Diabetic Patients with Insulin Resistance and Cardiovascular Risk Factors. Metab. Syndr. Relat. Disord. 2010, 8, 137–142. [Google Scholar] [CrossRef]
- Chao, Y.P.; Lai, Y.F.; Kao, T.W.; Peng, T.C.; Lin, Y.Y.; Shih, M.T.; Chen, W.L.; Wu, L.W. Mid-arm Muscle Circumference as a Surrogate in Predicting Insulin Resistance in Non-obese Elderly Individuals. Oncotarget 2017, 8, 79775–79784. [Google Scholar] [CrossRef] [Green Version]
- Abe, Y.; Urakami, T.; Hara, M.; Yoshida, K.; Mine, Y.; Aoki, M.; Suzuki, J.; Saito, E.; Yoshino, Y.; Iwata, F.; et al. The Characteristics of Abdominal Fat Distribution in Japanese Adolescents with Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. 2019, 12, 2281–2288. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, R.; Urakami, T.; Yoshida, K.; Morioka, I. Case of Type 2 Diabetes Possibly Caused by Excessive Accumulation of Visceral Fat in a Child Born Small-for-Gestational Age. J. Diabetes Investig. 2020, 11, 1366–1369. [Google Scholar] [CrossRef]
- Clemmons, D.R.; Miller, S.; Mamputu, J.C. Safety and metabolic effects of tesamorelin, a growth hormone-releasing factor analogue, in patients with type 2 diabetes: A randomized, placebo-controlled trial. PLoS ONE 2017, 12, e0179538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horikawa, R.; Tanaka, T.; Nishinaga, H.; Ogawa, Y.; Yokoya, S. The influence of a long-term growth hormone treatment on lipid and glucose metabolism: A randomized trial in short Japanese children born small for gestational age. Int. J. Pediatr. Endocrinol. 2016, 2016, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sydlik, C.; Weissenbacher, C.; Roeb, J.; Pozza, S.B.; Schmidt, H. Evaluation of changes in insulin sensitivity in prepubertal small for gestational age children treated with growth hormone. Indian J. Endocrinol. Metab. 2019, 23, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Cutfield, W.S.; Jackson, W.E.; Jefferies, C.; Robinson, E.M.; Breier, B.H.; Richards, G.E.; Hofman, P.L. Reduced insulin sensitivity during growth hormone therapy for short children born small for gestational age. J. Pediatr. 2003, 142, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Forrest, L.; Sedmak, C.; Sikder, S.; Grewal, S.; Harman, S.M.; Blackman, M.R.; Muniyappa, R. Effects of growth hormone on hepatic insulin sensitivity and glucose effectiveness in healthy older adults. Endocrine 2019, 63, 497–506. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).