
Comparison of Characteristics of Definition Criteria for Respiratory Sarcopenia—The Otassya Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
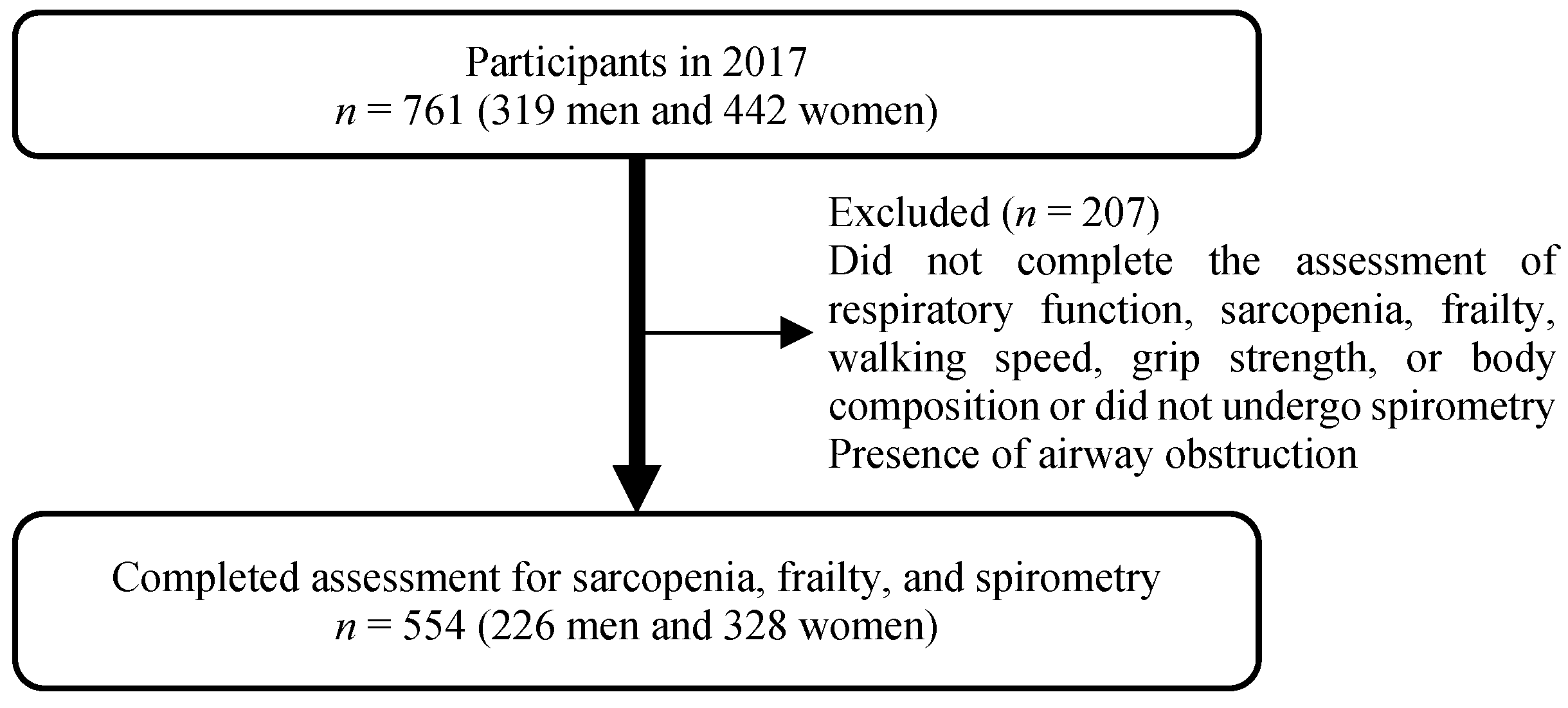
2.1. Participants
2.2. Measurement of Physical and Respiratory Function and Questionnaire
2.3. Definition of Sarcopenia and Frailty
2.4. Definition of Respiratory Sarcopenia
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenberg, I.H. Summary comments: Epidemiologic and methodologic problems in determining nutritional status of older persons. Am. J. Clin. Nutr. 1989, 50, 1231–1233. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lalley, P.M. The aging respiratory system—Pulmonary structure, function and neural control. Respir. Physiol. Neurobiol. 2013, 187, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Black, L.F.; Hyatt, R.E. Maximal respiratory pressures: Normal values and relationship to age and sex. Am. Rev. Respir. Dis. 1969, 99, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Enright, P.L.; Kronmal, R.A.; Manolio, T.A.; Schenker, M.B.; Hyatt, R.E. Respiratory muscle strength in the elderly. Correlates and reference values. Cardiovascular Health Study Research Group. Am. J. Respir. Crit. Care Med. 1994, 149, 430–438. [Google Scholar] [CrossRef] [PubMed]
- McConnell, A.K.; Copestake, A.J. Maximum static respiratory pressures in healthy elderly men and women: Issues of reproducibility and interpretation. Respiration 1999, 66, 251–258. [Google Scholar] [CrossRef]
- Polkey, M.I.; Green, M.; Moxham, J. Measurement of respiratory muscle strength. Thorax 1995, 50, 1131–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef] [PubMed]
- Ju, S.; Lee, S.J.; Park, M.J.; Cho, Y.J.; Jeong, Y.Y.; Jeon, K.N.; Bae, K.; Lee, J.D.; Kim, H.C. Clinical importance of cross-sectional area of intercostal muscles in patients with chronic obstructive pulmonary disease. Clin. Respir. J. 2018, 12, 939–947. [Google Scholar] [CrossRef]
- Kera, T.; Kawai, H.; Hirano, H.; Kojima, M.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Relationships among peak expiratory flow rate, body composition, physical function, and sarcopenia in community-dwelling older adults. Aging Clin. Exp. Res. 2018, 30, 331–340. [Google Scholar] [CrossRef]
- Cook, N.R.; Evans, D.A.; Scherr, P.A.; Speizer, F.E.; Vedal, S.; Branch, L.G.; Huntley, J.C.; Hennekens, C.H.; Taylor, J.O. Peak expiratory flow rate in an elderly population. Am. J. Epidemiol. 1989, 130, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Kera, T.; Kawai, H.; Hirano, H.; Kojima, M.; Watanabe, Y.; Motokawa, K.; Fujiwara, Y.; Ihara, K.; Kim, H.; Obuchi, S. Definition of respiratory sarcopenia with peak expiratory flow rate. J. Am. Med. Dir. Assoc. 2019, 20, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Wakabayashi, H.; Maeda, K.; Kokura, Y.; Miyazaki, S.; Mori, T.; Fujiwara, D. Respiratory sarcopenia and sarcopenic respiratory disability: Concepts, diagnosis, and treatment. J. Nutr. Health Aging 2021, 25, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Arai, H.; Satake, S. English translation of the Kihon Checklist. Geriatr. Gerontol. Int. 2015, 15, 518–519. [Google Scholar] [CrossRef]
- Long-Term Care, Health and Welfare Services for the Elderly. Japan Ministry of Health, Labour and Welfare. 2017. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/index.html (accessed on 19 August 2021).
- Sewo Sampaio, P.Y.; Sampaio, R.A.C.; Yamada, M.; Ogita, M.; Arai, H. Comparison of frailty among Japanese, Brazilian Japanese descendants and Brazilian community-dwelling older women. Geriatr. Gerontol. Int. 2015, 15, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Satake, S.; Senda, K.; Hong, Y.J.; Miura, H.; Endo, H.; Sakurai, T.; Kondo, I.; Toba, K. Validity of the Kihon Checklist for assessing frailty status. Geriatr. Gerontol. Int. 2016, 16, 709–715. [Google Scholar] [CrossRef]
- Kubota, M.; Kobayashi, H.; Quanjer, P.H.; Omori, H.; Tatsumi, K.; Kanazawa, M. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir. Investig. 2014, 52, 242–250. [Google Scholar] [CrossRef]
- West, J.B.; Luks, A.M. West’s Pulmonary Pathophysiology: The Essentials, 10th ed.Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2021; pp. 3–67. [Google Scholar]
- Ohara, D.G.; Pegorari, M.; dos Santos, N.O.; Silva, C.d.F.R.; Monteiro, R.; Matos, A.; Jamami, M. Respiratory muscle strength as a discriminator of sarcopenia in community-dwelling elderly: A cross-sectional study. J. Nutr. Health Aging 2018, 22, 952–958. [Google Scholar] [CrossRef]
- Morisawa, T.; Kunieda, Y.; Koyama, S.; Suzuki, M.; Takahashi, Y.; Takakura, T.; Kikuchi, Y.; Matsuda, T.; Fujino, Y.; Sawa, R.; et al. The relationship between sarcopenia and respiratory muscle weakness in community-dwelling older adults. Int. J. Environ. Res. Public Health 2021, 18, 13257. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Nakamura, M.; Kida, K.; Kanbe, S.; Takahashi, K.; Fujimura, M. The spirometry and arterial blood gas partial pressure reference value in Japanese adult people. Nihon Kokyuki Gakkai Zasshi 2001, 39, 1–17. (In Japanese) [Google Scholar]


{kind=link}
{kind=link}
| Low FVC and sarcopenia (JARN model) | ||||||
| Men | Women | |||||
| Robust (n = 216) | Respiratory sarcopenia (n = 10) | p-value | Robust (n = 317) | Respiratory sarcopenia (n = 11) | p-value | |
| Age, year | 72.5 (6.4) | 78.8 (6.1) | 0.005 | 73.3 (6.0) | 80.6 (6.0) | 0.001 |
| BMI, kg/m2 | 23.7 (3.3) | 20.7 (2.1) | 0.003 | 22.4 (3.2) | 21.4 (2.3) | 0.300 |
| Grip strength, kg | 34.6 (7.1) | 24.7 (5.2) | <0.001 | 22.4 (4.6) | 14.8 (2.0) | <0.001 |
| Walk speed (usual), m/s | 1.43 (0.27) | 1.17 (0.25) | 0.005 | 1.44 (0.24) | 1.21 (0.2) | 0.002 |
| ASM/ht2, kg/m2 | 7.51 (0.78) | 6.62 (0.24) | <0.001 | 5.94 (0.71) | 5.37 (0.18) | <0.001 |
| PEFR, L/s | 6.54 (1.81) | 4.29 (1.51) | <0.001 | 4.45 (1.11) | 2.98 (1.44) | 0.001 |
| FVC.L | 3.04 (0.57) | 2.06 (0.33) | <0.001 | 2.1 (0.37) | 1.48 (0.18) | <0.001 |
| VC, L | 3.24 (0.64) | 2.18 (0.41) | <0.001 | 2.22 (0.41) | 1.60 (0.19) | <0.001 |
| %VC, % | 92.3 (14.7) | 68.2 (7.4) | <0.001 | 94.2 (14.2) | 74.9 (5.5) | <0.001 |
| FEV1, L | 2.42 (0.46) | 1.63 (0.3) | <0.001 | 1.69 (0.31) | 1.14 (0.14) | <0.001 |
| %FEV1, % | 88.6 (14.1) | 67.9 (12.4) | <0.001 | 98.6 (14.6) | 76.7 (9.7) | <0.001 |
| Low PEFR (Kera’s model) | ||||||
| Men | Women | |||||
| Robust (n = 192) | Respiratory sarcopenia (n = 34) | p-value | Robust (n = 271) | Respiratory sarcopenia (n = 57) | p-value | |
| Age, year | 71.9 (6.1) | 77.7 (6.9) | <0.001 | 73 (5.8) | 76.2 (6.8) | <0.001 |
| BMI, kg/m2 | 23.6 (3.2) | 23.1 (3.9) | 0.408 | 22.4 (3.2) | 22.3 (3.2) | 0.835 |
| Grip strength, kg | 35.1 (6.9) | 29.4 (7.5) | <0.001 | 22.7 (4.6) | 19.6 (4.7) | <0.001 |
| Walk speed (usual), m/s | 1.44 (0.27) | 1.27 (0.28) | 0.001 | 1.45 (0.24) | 1.33 (0.26) | <0.001 |
| ASM/ht2, kg/m2 | 7.52 (0.77) | 7.20 (0.83) | 0.031 | 5.98 (0.67) | 5.64 (0.81) | 0.001 |
| PEFR, L/s | 6.97 (1.46) | 3.47 (0.63) | <0.001 | 4.77 (0.87) | 2.66 (0.54) | <0.001 |
| FVC, L | 3.08 (0.56) | 2.53 (0.58) | <0.001 | 2.14 (0.36) | 1.76 (0.31) | <0.001 |
| VC, L | 3.30 (0.62) | 2.61 (0.61) | <0.001 | 2.28 (0.4) | 1.86 (0.34) | <0.001 |
| %VC, % | 93.2 (14.1) | 80.6 (17.3) | <0.001 | 95.7 (14.1) | 83.5 (11.8) | <0.001 |
| FEV1, L | 2.46 (0.45) | 1.93 (0.44) | <0.001 | 1.73 (0.3) | 1.41 (0.26) | <0.001 |
| %FEV1, % | 89.3 (13.6) | 78.6 (16.8) | <0.001 | 99.8 (14.4) | 88.5 (14.1) | <0.001 |
| Men | FVC | VC | %VC | PEFR | FEV1/ FVC | ASM/ height2 | Grip strength | Walking speed | KCL |
| FVC | 1.000 | 0.939 ** | 0.772 *** | 0.494 *** | −0.056 | 0.317 *** | 0.517 *** | 0.309 *** | −0.201 ** |
| VC | 1.000 | 0.847 *** | 0.509 *** | −0.037 ** | 0.358 *** | 0.553 *** | 0.379 *** | −0.219 ** | |
| %VC | 1.000 | 0.393 *** | −0.016 | 0.151 * | 0.344 *** | 0.298 *** | −0.226 ** | ||
| PEFR | 1.000 | 0.206 ** | 0.185 ** | 0.380 ** | 0.308 ** | −0.190 ** | |||
| FEV1/FVC | 1.000 | −0.015 | 0.032 | 0.067 | −0.055 | ||||
| ASM/height2 | 1.000 | 0.446 *** | 0.100 | −0.089 | |||||
| Grip strength | 1.000 | 0.328 *** | −0.273 *** | ||||||
| Walking speed | 1.000 | −0.346 *** | |||||||
| KCL | 1.000 | ||||||||
| Women | FVC | VC | %VC | PEFR | FEV1/ FVC | ASM/ height2 | Grip strength | Walking speed | KCL |
| FVC | 1.00 | 0.931 *** | 0.743 *** | 0.589 *** | −0.052 | 0.164 ** | 0.440 *** | 0.270 *** | −0.045 |
| VC | 1.000 | 0.844 *** | 0.589 *** | −0.054 | 0.225 *** | 0.438 *** | 0.285 *** | −0.046 | |
| %VC | 1.000 | 0.434 *** | −0.094 | 0.059 | 0.225 *** | 0.143 ** | 0.040 | ||
| PEFR | 1.000 | 0.168 ** | 0.234 *** | 0.349 *** | 0.224 *** | −0.053 | |||
| FEV1/FVC | 1.000 | 0.012 | −0.019 | −0.071 | 0.050 | ||||
| ASM/height2 | 1.000 | 0.392 *** | 0.152 ** | −0.116 * | |||||
| Grip strength | 1.000 | 0.350 *** | −0.239 *** | ||||||
| Walking speed | 1.000 | −0.361 *** | |||||||
| KCL | 1.000 |
| Men | Women | ||||
|---|---|---|---|---|---|
| AUC | p | AUC | p | ||
| AWGS sarcopenia | FVC | 0.76 (0.67–0.85) | <0.001 | 0.67 (0.57–0.76) | 0.002 |
| PEFR | 0.74 (0.64–0.83) | <0.001 | 0.69 (0.60–0.79) | <0.001 | |
| Certified for LTCI # | FVC | 0.90 (0.81–0.98) | <0.001 | 0.77 (0.63–0.91) | 0.002 |
| PEFR | 0.82 (0.68–0.97) | <0.001 | 0.70 (0.58–0.82) | 0.023 | |
| Frail | FVC | 0.64 (0.51–0.77) | 0.040 | 0.59 (0.38–0.80) | 0.310 |
| PEFR | 0.60 (0.46–0.74) | 0.132 | 0.60 (0.46–0.75) | 0.242 |
| Low FVC and Sarcopenia of Whole-Body (JARN Model) | Low PEFR (Kera′s Model) | |||||
|---|---|---|---|---|---|---|
| AWGS Sarcopenia | LTCI | Frail | AWGS Sarcopenia | LTCI | Frail | |
| Sensitivity, % | 32.8 (21.6–45.7) | 27.3 (10.7–50.2) | 16.1 (5.5–33.7) | 42.2 (29.9–55.2) | 50.0 (28.2–71.8) | 25.8 (11.9–44.6) |
| Specificity, % | 100.0 (99.3–100.0) | 97.2 (95.4–98.4) | 96.9 (95.1–98.2) | 86.9 (83.6–89.8) | 85.0 (81.6–87.9) | 84.1 (80.7–87.2) |
| Positive likelihood ratio | Infinity | 9.67 (4.15–22.52) | 4.70 (1.87–11.83) | 3.22 (2.23–4.65) | 3.33 (2.09–5.29) | 1.63 (0.87–3.05) |
| Negative likelihood ratio | 0.67 (0.57–0.80) | 0.75 (0.58–0.97) | 0.87 (0.70–1.00) | 0.66 (0.50–0.80) | 0.59 (0.40–0.90) | 0.88 (0.71–1.09) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kera, T.; Kawai, H.; Ejiri, M.; Ito, K.; Hirano, H.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Comparison of Characteristics of Definition Criteria for Respiratory Sarcopenia—The Otassya Study. Int. J. Environ. Res. Public Health 2022, 19, 8542. https://doi.org/10.3390/ijerph19148542
Kera T, Kawai H, Ejiri M, Ito K, Hirano H, Fujiwara Y, Ihara K, Obuchi S. Comparison of Characteristics of Definition Criteria for Respiratory Sarcopenia—The Otassya Study. International Journal of Environmental Research and Public Health. 2022; 19(14):8542. https://doi.org/10.3390/ijerph19148542
Chicago/Turabian StyleKera, Takeshi, Hisashi Kawai, Manami Ejiri, Kumiko Ito, Hirohiko Hirano, Yoshinori Fujiwara, Kazushige Ihara, and Shuichi Obuchi. 2022. "Comparison of Characteristics of Definition Criteria for Respiratory Sarcopenia—The Otassya Study" International Journal of Environmental Research and Public Health 19, no. 14: 8542. https://doi.org/10.3390/ijerph19148542
APA StyleKera, T., Kawai, H., Ejiri, M., Ito, K., Hirano, H., Fujiwara, Y., Ihara, K., & Obuchi, S. (2022). Comparison of Characteristics of Definition Criteria for Respiratory Sarcopenia—The Otassya Study. International Journal of Environmental Research and Public Health, 19(14), 8542. https://doi.org/10.3390/ijerph19148542