
Assessment of the Feasibility of a Future Integrated Larger-Scale Epidemiological Study to Evaluate Health Risks of Air Pollution Episodes in Children

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
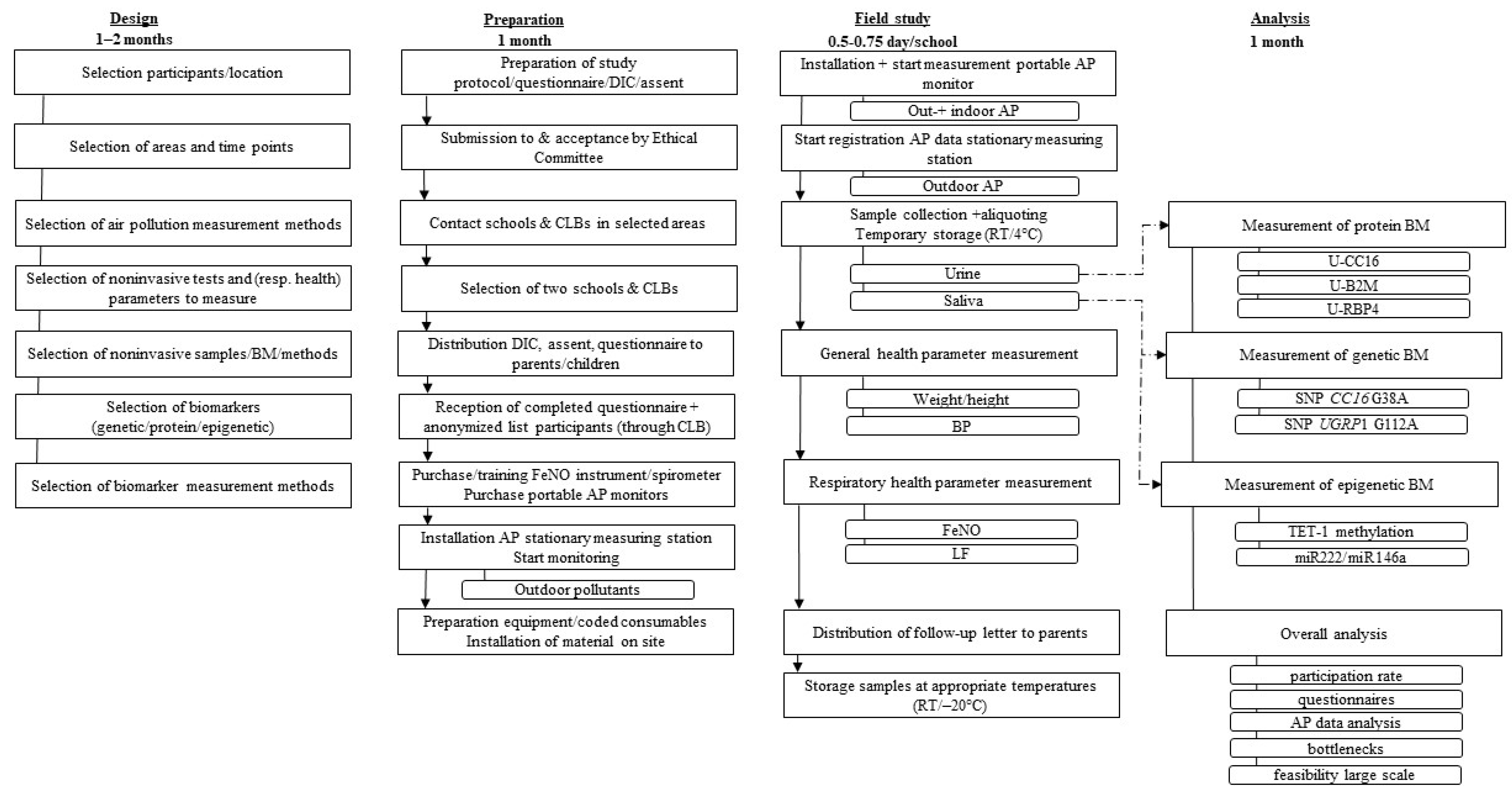
2.1. Field Study Design
2.2. Field Study Preparation
2.3. Examinations and Sample Collection
2.3.1. Urine Collection
2.3.2. Saliva Collection
2.3.3. General Health Parameters
2.3.4. Respiratory Health Parameters
2.4. Air Pollution Measurement
2.5. Sample Analysis
2.5.1. Protein Biomarker
2.5.2. Genetic Biomarker
2.5.3. Epigenetic Biomarkers
3. Results and Discussion
3.1. Field Study Design
3.2. Field Study Preparation
3.3. Examinations and Sample Collection
3.4. Air Pollution Measurement
3.5. Sample Analysis at Protein, Genetic and Epigenetic Levels
3.6. Evaluation of Willingness to Participate
3.7. Ideal Workflow of Larger-Scale Field Study
3.7.1. Adaptations Based on the Workflow of the Feasibility Study
Field Study Design
Field Study Preparation
Examinations and Sample Collection
Air Pollution Measurement
Sample Analysis (Genetic, Protein, Epigenetic)
3.7.2. Alternative Workflow: Self-Sampling
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boogaard, H.; Walker, K.; Cohen, A.J. Air pollution: The emergence of a major global health risk factor. Int. Health 2019, 11, 417–421. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Europe. Review of Evidence on Health Aspects of Air Pollution—REVIHAAP Project: Technical Report; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/193108/REVIHAAP-Final-technical-report-final-version.pdf (accessed on 22 March 2020).
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Copenhagen, Denmark, 2021.
- World Health Organization. Air Quality Guidelines: Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide, and Sulfur Dioxide; World Health Organization: Copenhagen, Denmark, 2006.
- Schwartz, J. Air pollution and children’s health. Pediatrics 2004, 113, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Hoek, G.; Chang, L.-Y.; Bo, Y.; Lin, C.; Huang, B.; Chan, T.-C.; Tam, T.; Lau, A.K.H.; Lao, X.Q. Long-Term Exposure to Ambient Fine Particulate Matter (PM 2.5) and Lung Function in Children, Adolescents, and Young Adults: A Longitudinal Cohort Study. Environ. Health Perspect. 2019, 127, 127008. [Google Scholar] [CrossRef] [PubMed]
- Orellano, P.; Quaranta, N.; Reynoso, J.; Balbi, B.; Vasquez, J. Effect of outdoor air pollution on asthma exacerbations in children and adults: Systematic review and multilevel meta-analysis. PLoS ONE 2017, 12, e0174050. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef]
- Buteau, S.; Shekarrizfard, M.; Hatzopolou, M.; Gamache, P.; Liu, L.; Smargiassi, A. Air pollution from industries and asthma onset in childhood: A population-based birth cohort study using dispersion modeling. Environ. Res. 2020, 185, 109180. [Google Scholar] [CrossRef]
- Gascon, M.; Sunyer, J. Air Pollution and Respiratory Health in Childhood. Arch. Bronconeumol. 2015, 51, 371–372. [Google Scholar] [CrossRef]
- GBD 2015. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2015, 17, 1133–1161. [Google Scholar] [CrossRef]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef]
- Renzetti, G.; Silvestre, G.; D’Amario, C.; Bottini, E.; Gloria-Bottini, F.; Bottini, N.; Auais, A.; Perez, M.K.; Piedimonte, G. Less Air Pollution Leads to Rapid Reduction of Airway Inflammation and Improved Airway Function in Asthmatic Children. Pediatrics 2009, 123, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Barraza-Villarreal, A.; Sunyer, J.; Cadena, L.H.; Escamilla-Nuñez, M.C.; Sienra-Monge, J.J.; Ramírez-Aguilar, M.; Cortez-Lugo, M.; Holguin, F.; Diaz-Sanchez, D.; Olin, A.C.; et al. Air Pollution, Airway Inflammation, and Lung Function in a Cohort Study of Mexico City Schoolchildren. Environ. Health Perspect. 2008, 116, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Chen, J.; Yang, Y.; Yuan, H.; Huang, Z.; Lu, Y. Effects of Ambient Air Pollution on Blood Pressure Among Children and Adolescents: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e017734. [Google Scholar] [CrossRef] [PubMed]
- Shijubo, N.; Itoh, Y.; Yamaguchi, T.; Sugaya, F.; Hirasawa, M.; Yamada, T.; Kawai, T.; Abe, S. Serum Levels of Clara Cell 10-kDa Protein Are Decreased in Patients with Asthma. Lung 1999, 177, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Almuntashiri, S.; Zhu, Y.; Han, Y.; Wang, X.; Somanath, P.R.; Zhang, D. Club Cell Secreted Protein CC16: Potential Applications in Prognosis and Therapy for Pulmonary Diseases. J. Clin. Med. 2020, 9, 4039. [Google Scholar] [CrossRef]
- Nauwelaerts, S.J.D.; Roosens, N.H.C.; Bernard, A.; De Keersmaecker, S.C.J.; De Cremer, K. Development of a multiplex mass spectrometry method for simultaneous quantification of urinary proteins related to respiratory health. Sci. Rep. 2021, 11, 10107. [Google Scholar] [CrossRef]
- Wang, H.; Dumont, X.; Haufroid, V.; Bernard, A. The physiological determinants of low-level urine cadmium: An assessment in a cross-sectional study among schoolchildren. Environ. Health 2017, 16, 99. [Google Scholar] [CrossRef]
- Arsalane, K.; Broeckaert, F.; Knoops, B.; Clippe, A.; Buchet, J.; Bernard, A. Increased Serum and Urinary Concentrations of Lung Clara Cell Protein in Rats Acutely Exposed to Ozone. Toxicol. Appl. Pharmacol. 1999, 159, 169–174. [Google Scholar] [CrossRef]
- Stockfelt, L.; Sallsten, G.; Olin, A.-C.; Almerud, P.; Samuelsson, L.; Johannesson, S.; Molnár, P.; Strandberg, B.; Almstrand, A.-C.; Bergemalm-Rynell, K.; et al. Effects on airways of short-term exposure to two kinds of wood smoke in a chamber study of healthy humans. Inhal. Toxicol. 2011, 24, 47–59. [Google Scholar] [CrossRef]
- Nauwelaerts, S.J.; Van Goethem, N.; Ureña, B.T.; De Cremer, K.; Bernard, A.; Saenen, N.D.; Nawrot, T.S.; Roosens, N.H.; De Keersmaecker, S.C. Urinary CC16, a potential indicator of lung integrity and inflammation, increases in children after short-term exposure to PM2.5/PM10 and is driven by the CC16 38GG genotype. Environ. Res. 2022, 212, 113272. [Google Scholar] [CrossRef]
- Egron, C.; Labbé, A.; Rochette, E.; Mulliez, A.; Bernard, A.; Amat, F. Urinary club cell protein 16 (CC16): Utility of its assay during acute bronchiolitis. Pediatr. Pulmonol. 2020, 55, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Rosas-Salazar, C.; Gebretsadik, T.; Carroll, K.N.; Reiss, S.; Wickersham, N.; Larkin, E.K.; James, K.M.; Miller, E.K.; Anderson, L.J.; Hartert, T.V. Urine Club Cell 16-kDa Secretory Protein and Childhood Wheezing Illnesses After Lower Respiratory Tract Infections in Infancy. Pediatr. Allergy Immunol. Pulmonol. 2015, 28, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-C.; Tseng, H.-M.; Wu, C.-J.; Kuo, M.-L.; Wu, C.-J.; Gao, P.-S.; Yeh, K.-W.; Yao, T.-C.; Lee, W.-I.; Ou, L.-S.; et al. Evaluation of a Common Variant of the Gene Encoding Clara Cell 10 kd Protein (CC10) as a Candidate Determinant for Asthma Severity and Steroid Responsiveness Among Chinese Children. J. Asthma 2012, 49, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Seok, H.; Park, H.J.; Han, K.; Kang, S.W.; Ban, J.Y.; Jung, H.-J.; Kim, K.-I.; Lee, B.-J.; Kim, J.; et al. Association Between Secretoglobin Family 3A Member 2 (SCGB3A2) Gene Polymorphisms and Asthma in a Korean Population. Med. Sci. Monit. 2017, 23, 1880–1885. [Google Scholar] [CrossRef][Green Version]
- Ku, M.-S.; Sun, H.-L.; Lu, K.-H.; Sheu, J.-N.; Lee, H.-S.; Yang, S.-F.; Lue, K.-H. The CC16 A38G polymorphism is associated with the development of asthma in children with allergic rhinitis: CC16 polymorphism and asthma development. Clin. Exp. Allergy 2011, 41, 794–800. [Google Scholar] [CrossRef]
- Laing, I.A.; Hermans, C.; Bernard, A.; Burton, P.R.; Goldblatt, J.; Le Souëf, P.N. Association between Plasma CC16 Levels, the A38G Polymorphism, and Asthma. Am. J. Respir. Crit. Care Med. 2000, 161, 124–127. [Google Scholar] [CrossRef]
- Niimi, T.; Munakata, M.; Keck-Waggoner, C.L.; Popescu, N.C.; Levitt, R.C.; Hisada, M.; Kimura, S. A Polymorphism in the Human UGRP1 Gene Promoter That Regulates Transcription Is Associated with an Increased Risk of Asthma. Am. J. Hum. Genet. 2002, 70, 718–725. [Google Scholar] [CrossRef][Green Version]
- Taniguchi, N.; Konno, S.; Hattori, T.; Isada, A.; Shimizu, K.; Shimizu, K.; Shijubo, N.; Huang, S.-K.; Hizawa, N.; Nishimura, M. The CC16 A38G polymorphism is associated with asymptomatic airway hyper-responsiveness and development of late-onset asthma. Ann. Allergy Asthma Immunol. 2013, 111, 376–381.e1. [Google Scholar] [CrossRef]
- Nauwelaerts, S.J.D.; Van Geel, D.; Delvoye, M.; De Cremer, K.; Bernard, A.; Roosens, N.H.C.; De Keersmaecker, S.C.J. Selection of a Noninvasive Source of Human DNA Envisaging Genotyping Assays in Epidemiological Studies: Urine or Saliva? J. Biomol. Tech. 2020, 31, 27–35. [Google Scholar] [CrossRef][Green Version]
- Nauwelaerts, S.J.D.; Roosens, N.H.C.; De Cremer, K.; Bernard, A.; De Keersmaecker, S.C.J. Gender-dependent association between exhaled nitric oxide and the CC16 38AA genotype in young school children. Immun. Inflamm. Dis. 2020, 8, 497–505. [Google Scholar] [CrossRef]
- Vrijens, K.; Bollati, V.; Nawrot, T.S. MicroRNAs as Potential Signatures of Environmental Exposure or Effect: A Systematic Review. Environ. Health Perspect. 2015, 123, 399–411. [Google Scholar] [CrossRef]
- Silveyra, P.; Floros, J. Air pollution and epigenetics: Effects on SP-A and innate host defence in the lung. Swiss Med. Wkly. 2012, 142, w13579. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Hershey, G.K.K. Genetic and epigenetic influence on the response to environmental particulate matter. J. Allergy Clin. Immunol. 2012, 129, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Somineni, H.K.; Zhang, X.; Myers, J.M.; Kovacic, M.B.; Ulm, A.; Jurcak, N.; Ryan, P.H.; Hershey, G.; Ji, H. Ten-eleven translocation 1 (TET1) methylation is associated with childhood asthma and traffic-related air pollution. J. Allergy Clin. Immunol. 2016, 137, 797–805.e795. [Google Scholar] [CrossRef]
- Bollati, V.; Angelici, L.; Rizzo, G.; Pergoli, L.; Rota, F.; Hoxha, M.; Nordio, F.; Bonzini, M.; Tarantini, L.; Cantone, L.; et al. Microvesicle-associated microRNA expression is altered upon particulate matter exposure in healthy workers and in A549 cells. J. Appl. Toxicol. 2014, 35, 59–67. [Google Scholar] [CrossRef]
- Bollati, V.; Marinelli, B.; Apostoli, P.; Bonzini, M.; Nordio, F.; Hoxha, M.; Pegoraro, V.; Motta, V.; Tarantini, L.; Cantone, L.; et al. Exposure to Metal-Rich Particulate Matter Modifies the Expression of Candidate MicroRNAs in Peripheral Blood Leukocytes. Environ. Health Perspect. 2010, 118, 763–768. [Google Scholar] [CrossRef]
- Fossati, S.; Baccarelli, A.; Zanobetti, A.; Hoxha, M.; Vokonas, P.S.; Wright, R.; Schwartz, J. Ambient Particulate Air Pollution and MicroRNAs in Elderly Men. Epidemiology 2014, 25, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Motta, V.; Angelici, L.; Nordio, F.; Bollati, V.; Fossati, S.; Frascati, F.; Tinaglia, V.; Bertazzi, P.A.; Battaglia, C.; Baccarelli, A.A. Integrative Analysis of miRNA and Inflammatory Gene Expression After Acute Particulate Matter Exposure. Toxicol. Sci. 2013, 132, 307–316. [Google Scholar] [CrossRef]
- Vriens, A.; Nawrot, T.S.; Saenen, N.D.; Provost, E.B.; Kicinski, M.; Lefebvre, W.; Vanpoucke, C.; Van Deun, J.; De Wever, O.; Vrijens, K.; et al. Recent exposure to ultrafine particles in school children alters miR-222 expression in the extracellular fraction of saliva. Environ. Health 2016, 15, 80. [Google Scholar] [CrossRef]
- Lee, D.H.; Yao, C.; Bhan, A.; Schlaeger, T.; Keefe, J.; Rodriguez, B.A.; Hwang, S.-J.; Chen, M.-H.; Levy, D.; Johnson, A.D. Integrative Genomic Analysis Reveals Four Protein Biomarkers for Platelet Traits. Circ. Res. 2020, 127, 1182–1194. [Google Scholar] [CrossRef]
- Hillary, R.F.; McCartney, D.L.; Harris, S.E.; Stevenson, A.; Seeboth, A.; Zhang, Q.; Liewald, D.C.; Evans, K.L.; Ritchie, C.W.; Tucker-Drob, E.M.; et al. Genome and epigenome wide studies of neurological protein biomarkers in the Lothian Birth Cohort 1936. Nat. Commun. 2019, 10, 3160. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; LeFave, C.; Sirosh, I.; Siegel, A.B.; Tycko, B.; Santella, R.M. Integrative epigenomic and genomic filtering for methylation markers in hepatocellular carcinomas. BMC Med. Genom. 2015, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Sardella, A.; Voisin, C.; Dumont, X.; Marcucci, F.; Bernard, A. Nasal epithelium biomarkers in young children: Associations with allergic sensitization and environmental stressors. Pediatr. Pulmonol. 2013, 48, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Voisin, C.; Sardella, A.; Marcucci, F.; Bernard, A. Infant swimming in chlorinated pools and the risks of bronchiolitis, asthma and allergy. Eur. Respir. J. 2010, 36, 41–47. [Google Scholar] [CrossRef]
- Nunes, A.P.; Oliveira, I.O.; Santos, B.R.; Millech, C.; Silva, L.P.; González, D.A.; Hallal, P.C.; Menezes, A.M.B.; Araújo, C.L.; Barros, F.C. Quality of DNA extracted from saliva samples collected with the OrageneTM DNA self-collection kit. BMC Med. Res. Methodol. 2012, 12, 65. [Google Scholar] [CrossRef]
- ATS/ERS—American Thoracic Society, European Respiratory Society. ATS/ERS Recommendations for Standardized Procedures for the Online and Offline Measurement of Exhaled Lower Respiratory Nitric Oxide and Nasal Nitric Oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson JA, T.S.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Neven, K.Y.; Saenen, N.D.; Tarantini, L.; Janssen, B.G.; Lefebvre, W.; Vanpoucke, C.; Bollati, V.; Nawrot, T.S. Placental promoter methylation of DNA repair genes and prenatal exposure to particulate air pollution: An ENVIR ON AGE cohort study. Lancet Planet. Health. 2018, 2, e174–e183. [Google Scholar] [CrossRef]
- Saenen, N.D.; Vrijens, K.; Janssen, B.G.; Roels, H.A.; Neven, K.Y.; Berghe, W.V.; Gyselaers, W.; Vanpoucke, C.; Lefebvre, W.; De Boever, P.; et al. Lower Placental Leptin Promoter Methylation in Association with Fine Particulate Matter Air Pollution during Pregnancy and Placental Nitrosative Stress at Birth in the ENVIR ON AGE Cohort. Environ. Health Perspect. 2017, 125, 262–268. [Google Scholar] [CrossRef]
- Roberts, T.C.; Coenen-Stass, A.M.L.; Wood, M.J.A. Assessment of RT-qPCR Normalization Strategies for Accurate Quantification of Extracellular microRNAs in Murine Serum. PLoS ONE 2014, 9, e89237. [Google Scholar] [CrossRef]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating microRNAs as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef] [PubMed]
- Gai, C.; Camussi, F.; Broccoletti, R.; Gambino, A.; Cabras, M.; Molinaro, L.; Carossa, S.; Camussi, G.; Arduino, P.G. Salivary extracellular vesicle-associated miRNAs as potential biomarkers in oral squamous cell carcinoma. BMC Cancer 2018, 18, 439. [Google Scholar] [CrossRef] [PubMed]
- Hermans, C.; Bernard, A. Lung Epithelium–specific Proteins. Am. J. Respir. Crit. Care Med. 1999, 159, 646–678. [Google Scholar] [CrossRef] [PubMed]
- Nishitani, S.; Parets, S.E.; Haas, B.W.; Smith, A.K. DNA methylation analysis from saliva samples for epidemiological studies. Epigenetics 2018, 13, 352–362. [Google Scholar] [CrossRef]
- Di Pietro, V.; Porto, E.; Ragusa, M.; Barbagallo, C.; Davies, D.; Forcione, M.; Logan, A.; Di Pietro, C.; Purrello, M.; Grey, M.; et al. Salivary MicroRNAs: Diagnostic Markers of Mild Traumatic Brain Injury in Contact-Sport. Front. Mol. Neurosci. 2018, 11, 290. [Google Scholar] [CrossRef]
- Nemoda, Z. The Use of Saliva for Genetic and Epigenetic Research. In Salivary Bioscience: Foundations of Interdisciplinary Saliva Research and Applications; Granger, D.A., Taylor, M.K., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 115–138. [Google Scholar] [CrossRef]
- E Abraham, J.; Maranian, M.J.; Spiteri, I.; Russell, R.; Ingle, S.; Luccarini, C.; Earl, H.M.; Pharoah, P.P.; Dunning, A.M.; Caldas, C. Saliva samples are a viable alternative to blood samples as a source of DNA for high throughput genotyping. BMC Med. Genom. 2012, 5, 19. [Google Scholar] [CrossRef]
- Rylander-Rudqvist, T.; Haåkansson, N.; Tybring, G.; Wolk, A. Quality and Quantity of Saliva DNA Obtained from the Self-administrated Oragene Method—A Pilot Study on the Cohort of Swedish Men. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1742–1745. [Google Scholar] [CrossRef]
- Brunst, K.; Leung, Y.-K.; Ryan, P.H.; Hershey, G.K.; Levin, L.; Ji, H.; LeMasters, G.K.; Ho, S.-M. Forkhead box protein 3 (FOXP3) hypermethylation is associated with diesel exhaust exposure and risk for childhood asthma. J. Allergy Clin. Immunol. 2012, 131, 592–594.e3. [Google Scholar] [CrossRef]
- Lovinsky-Desir, S.; Jung, K.H.; Jezioro, J.R.; Torrone, D.Z.; De Planell-Saguer, M.; Yan, B.; Perera, F.P.; Rundle, A.G.; Perzanowski, M.S.; Chillrud, S.N.; et al. Physical activity, black carbon exposure, and DNA methylation in the FOXP3 promoter. Clin. Epigenetics 2017, 9, 65. [Google Scholar] [CrossRef]
- Baccarelli, A.; Rusconi, F.; Bollati, V.; Catelan, D.; Accetta, G.; Hou, L.; Barbone, F.; Bertazzi, P.A.; Biggeri, A. Nasal cell DNA methylation, inflammation, lung function and wheezing in children with asthma. Epigenomics 2012, 4, 91–100. [Google Scholar] [CrossRef]
- Comfort, N.; Smith, C.; Chillrud, S.; Yang, Q.; Baccarelli, A.; Jack, D. Extracellular Vesicles in Saliva as Biomarkers of Exposure and Effect: A feasibility pilot in the context of the New York City biking and breathing study. Environ. Epidemiology 2019, 3, 80. [Google Scholar] [CrossRef]
- Kim, K.M.; Abdelmohsen, K.; Mustapic, M.; Kapogiannis, D.; Gorospe, M. RNA in extracellular vesicles. Wiley Interdiscip. Rev. RNA 2017, 8, e1413. [Google Scholar] [CrossRef] [PubMed]
- Bahn, J.H.; Zhang, Q.; Li, F.; Chan, T.-M.; Lin, X.; Kim, Y.; Wong, D.T.W.; Xiao, X. The Landscape of MicroRNA, Piwi-Interacting RNA, and Circular RNA in Human Saliva. Clin. Chem. 2015, 61, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Karvinen, S.; Sievänen, T.; Karppinen, J.E.; Hautasaari, P.; Bart, G.; Samoylenko, A.; Vainio, S.J.; Ahtiainen, J.P.; Laakkonen, E.K.; Kujala, U.M. MicroRNAs in Extracellular Vesicles in Sweat Change in Response to Endurance Exercise. Front. Physiol. 2020, 11, 676. [Google Scholar] [CrossRef]
- Foley, H.B.; Howe, C.G.; Eckel, S.P.; Chavez, T.; Gevorkian, L.; Reyes, E.G.; Kapanke, B.; Martinez, D.; Xue, S.; Suglia, S.F.; et al. Extracellular vesicle-enriched miRNA profiles across pregnancy in the MADRES cohort. PLoS ONE 2021, 16, e0251259. [Google Scholar] [CrossRef] [PubMed]
- Irceline. Irceline Map Air Quality—Ozone. 2018. Available online: https://www.irceline.be/nl/luchtkwaliteit/metingen/ozon/historiek (accessed on 25 August 2018).
- Irceline. Irceline Map Air Quality—PM. 2018. Available online: https://www.irceline.be/nl/luchtkwaliteit/metingen/fijnstof/historiek (accessed on 25 August 2018).
- Thomas, C.E.; Sexton, W.; Benson, K.; Sutphen, R.; Koomen, J. Urine Collection and Processing for Protein Biomarker Discovery and Quantification. Cancer Epidemiol. Biomark. Prev. 2010, 19, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Thongboonkerd, V.; Saetun, P. Bacterial Overgrowth Affects Urinary Proteome Analysis: Recommendation for Centrifugation, Temperature, Duration, and the Use of Preservatives during Sample Collection. J. Proteome Res. 2007, 6, 4173–4181. [Google Scholar] [CrossRef]
- Adam, M.; Schikowski, T.; Carsin, A.E.; Cai, Y.; Jacquemin, B.; Sanchez, M.; Vierkötter, A.; Marcon, A.; Keidel, D.; Sugiri, D.; et al. Adult lung function and long-term air pollution exposure. ESCAPE: A multicentre cohort study and meta-analysis. Eur. Respir. J. 2015, 45, 38–50. [Google Scholar] [CrossRef]
- Dons, E.; Panis, L.I.; Van Poppel, M.; Theunis, J.; Willems, H.; Torfs, R.; Wets, G. Impact of time–activity patterns on personal exposure to black carbon. Atmos. Environ. 2011, 45, 3594–3602. [Google Scholar] [CrossRef]
- Buonanno, G.; Fuoco, F.; Morawska, L.; Stabile, L. Airborne particle concentrations at schools measured at different spatial scales. Atmos. Environ. 2013, 67, 38–45. [Google Scholar] [CrossRef]
- Sousan, S.; Koehler, K.; Hallett, L.; Peters, T.M. Evaluation of consumer monitors to measure particulate matter. J. Aerosol Sci. 2017, 107, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Vercauteren, J. Performance Evaluation of Six Low-Cost Particulate Matter Sensors in the Field. 2021. Available online: https://vaquums.eu/sensor-db/tests/life-vaquums_pmfieldtest.pdf (accessed on 21 October 2021).
- Zusman, M.; Schumacher, C.S.; Gassett, A.J.; Spalt, E.W.; Austin, E.; Larson, T.V.; Carvlin, G.; Seto, E.; Kaufman, J.D.; Sheppard, L. Calibration of low-cost particulate matter sensors: Model development for a multi-city epidemiological study. Environ. Int. 2019, 134, 105329. [Google Scholar] [CrossRef] [PubMed]
- Crilley, L.R.; Singh, A.; Kramer, L.J.; Shaw, M.D.; Alam, M.S.; Apte, J.S.; Bloss, W.J.; Ruiz, L.H.; Fu, P.; Fu, W.; et al. Effect of aerosol composition on the performance of low-cost optical particle counter correction factors. Atmos. Meas. Tech. 2020, 13, 1181–1193. [Google Scholar] [CrossRef]
- Snyder, E.G.; Watkins, T.H.; Solomon, P.A.; Thoma, E.D.; Williams, R.W.; Hagler, G.S.W.; Shelow, D.; Hindin, D.A.; Kilaru, V.J.; Preuss, P.W. The Changing Paradigm of Air Pollution Monitoring. Environ. Sci. Technol. 2013, 47, 11369–11377. [Google Scholar] [CrossRef]
- Wennlöf, A.H.; Yngve, A.; Sjöström, M. Sampling procedure, participation rates and representativeness in the Swedish part of the European Youth Heart Study (EYHS). Public Health Nutr. 2003, 6, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Vanaelst, B.; Vyncke, K.; Sioen, I.; Huybrechts, I.; De Vriendt, T.; De Henauw, S. Children’s Body composition and Stress—The ChiBS study: Aims, design, methods, population and participation characteristics. Arch. Public Health 2012, 70, 17. [Google Scholar] [CrossRef]
- Denessen, E.; Driessen, G.; Smit, F.; Sleegers, P. Culture Differences in Education: Implications for Parental Involvement and Educational Policies; Instituut Voor Toegepaste Sociale Wetenschappen (ITS): Nijmegen, The Netherlands, 2001. [Google Scholar]
- U.S. Department of Education, National Center for Education Statistics. The Condition of Education 2004; NCES 2004–077; Government Printing Office: Washington, DC, USA, 2004.
- Bernard, A.; Carbonnelle, S.; Nickmilder, M.; de Burbure, C. Non-invasive biomarkers of pulmonary damage and inflammation: Application to children exposed to ozone and trichloramine. Toxicol. Appl. Pharmacol. 2005, 206, 185–190. [Google Scholar] [CrossRef]
- Li, W.; Xiao, L.; Zhou, Y.; Wang, D.; Ma, J.; Xie, L.; Yang, M.; Zhu, C.; Wang, B.; Chen, W. Plasma CC16 mediates the associations between urinary metals and fractional exhaled nitric oxide: A cross-sectional study. Environ. Pollut. 2020, 258, 113713. [Google Scholar] [CrossRef]
- Wang, H.; Duan, H.; Meng, T.; Yang, M.; Cui, L.; Bin, P.; Dai, Y.; Niu, Y.; Shen, M.; Zhang, L.; et al. Local and Systemic Inflammation May Mediate Diesel Engine Exhaust–Induced Lung Function Impairment in a Chinese Occupational Cohort. Toxicol. Sci. 2017, 162, 372–382. [Google Scholar] [CrossRef]
- Morawska, L.; Thai, P.K.; Liu, X.; Asumadu-Sakyi, A.; Ayoko, G.; Bartonova, A.; Bedini, A.; Chai, F.; Christensen, B.; Dunbabin, M.; et al. Applications of low-cost sensing technologies for air quality monitoring and exposure assessment: How far have they gone? Environ. Int. 2018, 116, 286–299. [Google Scholar] [CrossRef]
- Castell, N.; Dauge, F.R.; Schneider, P.; Vogt, M.; Lerner, U.; Fishbain, B.; Broday, D.; Bartonova, A. Can commercial low-cost sensor platforms contribute to air quality monitoring and exposure estimates? Environ. Int. 2017, 99, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Trost, B.; Walker, S.; Haider, S.A.; Sung, W.W.L.; Pereira, S.; Phillips, C.L.; Higginbotham, E.J.; Strug, L.J.; Nguyen, C.; Raajkumar, A.; et al. Impact of DNA source on genetic variant detection from human whole-genome sequencing data. J. Med. Genet. 2019, 56, 809–817. [Google Scholar] [CrossRef]
- Eynden, J.V.D.; Descamps, T.; Delporte, E.; Roosens, N.H.C.; De Keersmaecker, S.C.J.; De Wit, V.; Vermeesch, J.R.; Goetghebeur, E.; Tafforeau, J.; Demarest, S.; et al. The genetic structure of the Belgian population. Hum. Genom. 2018, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- The Human Genomics Strategy Group. Building on Our Inheritance: Genomic Technology in Healthcare. 2012. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/213705/dh_132382.pdf (accessed on 1 October 2020).
- Burton, H.; Jackson, C.; Abubakar, I. The impact of genomics on public health practice. Br. Med. Bull. 2014, 112, 37–46. [Google Scholar] [CrossRef]
- Rozalski, R.; Gackowski, D.; Siomek-Gorecka, A.; Banaszkiewicz, Z.; Olinski, R. Urinary Measurement of Epigenetic DNA Modifications: A Non-Invasive Assessment of the Whole-Body Epigenetic Status in Healthy Subjects and Colorectal Cancer Patients. ChemistryOpen 2016, 5, 550–553. [Google Scholar] [CrossRef]
- Setti, G.; Pezzi, M.E.; Viani, M.V.; Pertinhez, T.A.; Cassi, D.; Magnoni, C.; Bellini, P.; Musolino, A.; Vescovi, P.; Meleti, M. Salivary MicroRNA for Diagnosis of Cancer and Systemic Diseases: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 907. [Google Scholar] [CrossRef] [PubMed]
- Lam, D.; Luu, P.-L.; Song, J.Z.; Qu, W.; Risbridger, G.P.; Lawrence, M.G.; Lu, J.; Trau, M.; Korbie, D.; Clark, S.J.; et al. Comprehensive evaluation of targeted multiplex bisulphite PCR sequencing for validation of DNA methylation biomarker panels. Clin. Epigenet. 2020, 12, 90. [Google Scholar] [CrossRef]
- Patel, P.; Shiao, Y.-H.; Fortina, P. Multiplex Pyrosequencing® for DNA Variation Analysis. Methods Mol. Biol. 2007, 373, 75–88. [Google Scholar] [CrossRef]
- Kurdyukov, S.; Bullock, M. DNA Methylation Analysis: Choosing the Right Method. Biology 2016, 5, 3. [Google Scholar] [CrossRef]
- Okuda, Y.; Shimura, T.; Iwasaki, H.; Fukusada, S.; Nishigaki, R.; Kitagawa, M.; Katano, T.; Okamoto, Y.; Yamada, T.; Horike, S.-I.; et al. Urinary microRNA biomarkers for detecting the presence of esophageal cancer. Sci. Rep. 2021, 11, 8508. [Google Scholar] [CrossRef]
- Thingholm, L.B.; Andersen, L.; Makalic, E.; Southey, M.C.; Thomassen, M.; Hansen, L.L. Strategies for Integrated Analysis of Genetic, Epigenetic, and Gene Expression Variation in Cancer: Addressing the Challenges. Front. Genet. 2016, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Zaghlool, S.B.; Kühnel, B.; Elhadad, M.A.; Kader, S.; Halama, A.; Thareja, G.; Engelke, R.; Sarwath, H.; Al-Dous, E.K.; Mohamoud, Y.A.; et al. Epigenetics meets proteomics in an epigenome-wide association study with circulating blood plasma protein traits. Nat. Commun. 2020, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mariani, M.; He, S.; McHugh, M.; Andreoli, M.; Pandya, D.; Sieber, S.; Wu, Z.; Fiedler, P.; Shahabi, S.; Ferlini, C. Integrated Multidimensional Analysis Is Required for Accurate Prognostic Biomarkers in Colorectal Cancer. PLoS ONE 2014, 9, e101065. [Google Scholar] [CrossRef] [PubMed]
- Bakulski, K.M.; Fisher, J.D.; Dou, J.F.; Gard, A.; Schneper, L.; Notterman, D.A.; Ware, E.B.; Mitchell, C. Prenatal Particulate Matter Exposure Is Associated with Saliva DNA Methylation at Age 15: Applying Cumulative DNA Methylation Scores as an Exposure Biomarker. Toxics 2021, 9, 262. [Google Scholar] [CrossRef]
- Huybrechts, I.; Himes, J.H.; Ottevaere, C.; De Vriendt, T.; De Keyzer, W.; Cox, B.; Van Trimpont, I.; De Bacquer, D.; De Henauw, S. Validity of parent-reported weight and height of preschool children measured at home or estimated without home measurement: A validation study. BMC Pediatric 2011, 11, 63. [Google Scholar] [CrossRef]


{kind=link}
| Urban | Rural | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Participation a | n | % | N | n | % | N | n | % | N |
| Children participating | 19 | 53 | 36 | 23 | 41 | 56 | 42 | 46 | 92 |
| No response/no interest | 17 | 47 | 36 | 33 | 59 | 56 | 50 | 54 | 92 |
| Parents accept but child does not want to participate | 3 | 18 | 17 | 1 | 0 | 33 | 4 | 8 | 50 |
| Child accepts but parents do not want child to participate | 2 | 12 | 17 | 0 | 0 | 33 | 2 | 4 | 50 |
| Both parent and child do not want to participate | 12 | 71 | 17 | 32 | 97 | 33 | 44 | 88 | 50 |
| Questionnaire | |||||||||
| Completed questionnaires (partially or fully completed) | 19 | 100 | 19 | 23 | 100 | 23 | 42 | 100 | 42 |
| Type of questions answered incompletely 1 | |||||||||
| Frequency or age of a certain condition in childhood | 4 | 53 | 7 3 | 5 | 68 | 7 3 | 9 | 60 | 14 3 |
| Frequency of a certain activity performed by the child | 3 | 43 | 9 3 | 4 | 59 | 9 3 | 7 | 39 | 18 3 |
| Questions related to smoking habits of the mother or father | 8 | 53 | 13 3 | 1 | 33 | 3 3 | 9 | 56 | 16 3 |
| Incomplete probably due to recto–verso layout | 2 | 11 | 19 | 0 | 0 | 23 | 2 | 5 | 42 |
| Information retrieved from returned follow-up letters | |||||||||
| Completion | |||||||||
| Completed by parents of all children (participating and non-participating) | 10 | 28 | 36 | 44 | 79 | 56 | 54 | 59 | 92 |
| Consent received from child | 9 | 90 | 10 | 21 | 48 | 44 | 30 | 56 | 54 |
| Consent received from parents | 9 | 90 | 10 | 23 | 52 | 44 | 32 | 59 | 54 |
| Completed by parents of participating children | 9 | 47 | 19 | 21 | 91 | 23 | 30 | 71 | 42 |
| Completed by parents of non-participating children | 1 | 6 | 17 | 23 | 70 | 33 | 24 | 48 | 50 |
| Reasons for non-participation in current study | |||||||||
| Reason for no consent/no participation from the child | |||||||||
| No answer (not filled in) | 0 | 0 | 1 | 5 | 22 | 23 | 5 | 21 | 24 |
| Scared | 0 | 0 | 1 | 6 | 26 | 23 | 6 | 25 | 24 |
| No interest | 0 | 0 | 1 | 8 | 35 | 23 | 8 | 33 | 24 |
| Other reasons 2 | 1 | 100 | 1 | 4 | 17 | 23 | 5 | 21 | 24 |
| Reason for no consent for child to participate from the parent | |||||||||
| No answer (not filled in) | 0 | 0 | 1 | 7 | 33 | 21 | 7 | 32 | 22 |
| Scared | 0 | 0 | 1 | 1 | 5 | 21 | 1 | 5 | 22 |
| No interest | 0 | 0 | 1 | 4 | 19 | 21 | 4 | 18 | 22 |
| Only one of the parents consented | 0 | 0 | 1 | 1 | 5 | 21 | 1 | 5 | 22 |
| Other reasons 2 | 1 | 100 | 1 | 8 | 38 | 21 | 9 | 41 | 22 |
| Feedback from a parent after the study for those who participated | |||||||||
| No answer (not filled in) | 0 | 0 | 9 | 1 | 5 | 21 | 1 | 3 | 30 |
| Enthusiastic | 3 | 33 | 9 | 12 | 57 | 21 | 15 | 50 | 30 |
| Uncomfortable | 0 | 0 | 9 | 0 | 0 | 21 | 0 | 0 | 30 |
| No opinion | 4 | 44 | 9 | 8 | 38 | 21 | 12 | 40 | 30 |
| Other/not specified | 2 | 22 | 9 | 0 | 0 | 21 | 2 | 7 | 30 |
| Consent for future studies | |||||||||
| From the children participating in the current study | |||||||||
| Parent not willing to let child participate again | 1 | 11 | 9 | 1 | 5 | 21 | 2 | 7 | 30 |
| Parents willing give consent again for a new study | 8 | 89 | 9 | 20 | 95 | 21 | 28 | 93 | 30 |
| Number of times/year that new study can be conducted | |||||||||
| No answer (not filled in) | 1 | 13 | 8 | 3 | 15 | 20 | 4 | 14 | 28 |
| 2×/year | 3 | 38 | 8 | 9 | 45 | 20 | 12 | 43 | 28 |
| 3×/year | 1 | 13 | 8 | 3 | 15 | 20 | 4 | 14 | 28 |
| 4×/year | 2 | 25 | 8 | 3 | 15 | 20 | 5 | 18 | 28 |
| As much as needed | 1 | 13 | 8 | 2 | 10 | 20 | 3 | 11 | 28 |
| Consent for sampling | 7 | 88 | 8 | 20 | 100 | 20 | 27 | 96 | 28 |
| Consent for sample type—not specified (not filled in) | 1 | 14 | 7 | 1 | 5 | 20 | 2 | 7 | 27 |
| Consent for sample of urine | 6 | 86 | 7 | 19 | 100 | 19 | 25 | 96 | 26 |
| Consent for sample of saliva | 6 | 86 | 7 | 18 | 95 | 19 | 24 | 92 | 26 |
| Consent for sample of NALF | 5 | 71 | 7 | 9 | 47 | 19 | 14 | 54 | 26 |
| Consent for sample of feces | 3 | 43 | 7 | 10 | 53 | 19 | 13 | 50 | 26 |
| Consent for sample of blood | 3 | 43 | 7 | 9 | 47 | 19 | 12 | 46 | 26 |
| Consent for sample of blood if parents receive: | |||||||||
| blood type information for their child | 0 | 0 | 7 | 13 | 68 | 19 | 13 | 50 | 26 |
| personal results from the study for their child | 0 | 0 | 7 | 12 | 63 | 19 | 12 | 46 | 26 |
| From the children not participating in the current study | |||||||||
| Parent not willing to let child participate again | 0 | 0 | 1 | 13 | 57 | 23 | 13 | 54 | 24 |
| Parents did not answer (not filled in) | 0 | 0 | 1 | 8 | 35 | 23 | 8 | 33 | 24 |
| Parents willing to give consent again for a new study | 1 | 100 | 1 | 2 | 9 | 23 | 3 | 13 | 24 |
| Number of times/year that new study can be conducted | |||||||||
| no answer (not filled in) | 1 | 100 | 1 | 2 | 100 | 2 | 3 | 100 | 3 |
| Urban | Rural | |||
|---|---|---|---|---|
| Measuring Station | t1 in Summer | t2 in Winter | t1 in Summer | t2 in Winter |
| Ozone | 68 | 34 | 80 | 50 |
| BC | 0.7 | NA | 0.9 | 2.3 |
| NO2 | 41 | 49 | 29 | 62 |
| PM10 | 13 | 29 | 17 | 24 |
| PM2.5 | 5 | 19 | 9 | 13 |
| Portable BC monitor | ||||
| Streetside | 1.9 | 5.3 | / | / |
| Portable Airbeam (PM2.5) | ||||
| Streetside | 7.1 | 34.8 | 22.3 | 8.9 * |
| Playground | 4 | 30.4 | 26.2 | 8.9 * |
| Classroom | 5.2 | 12.7 | 14.6 | 3.9 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nauwelaerts, S.J.D.; De Cremer, K.; Bustos Sierra, N.; Gand, M.; Van Geel, D.; Delvoye, M.; Vandermassen, E.; Vercauteren, J.; Stroobants, C.; Bernard, A.; et al. Assessment of the Feasibility of a Future Integrated Larger-Scale Epidemiological Study to Evaluate Health Risks of Air Pollution Episodes in Children. Int. J. Environ. Res. Public Health 2022, 19, 8531. https://doi.org/10.3390/ijerph19148531
Nauwelaerts SJD, De Cremer K, Bustos Sierra N, Gand M, Van Geel D, Delvoye M, Vandermassen E, Vercauteren J, Stroobants C, Bernard A, et al. Assessment of the Feasibility of a Future Integrated Larger-Scale Epidemiological Study to Evaluate Health Risks of Air Pollution Episodes in Children. International Journal of Environmental Research and Public Health. 2022; 19(14):8531. https://doi.org/10.3390/ijerph19148531
Chicago/Turabian StyleNauwelaerts, Sarah J. D., Koen De Cremer, Natalia Bustos Sierra, Mathieu Gand, Dirk Van Geel, Maud Delvoye, Els Vandermassen, Jordy Vercauteren, Christophe Stroobants, Alfred Bernard, and et al. 2022. "Assessment of the Feasibility of a Future Integrated Larger-Scale Epidemiological Study to Evaluate Health Risks of Air Pollution Episodes in Children" International Journal of Environmental Research and Public Health 19, no. 14: 8531. https://doi.org/10.3390/ijerph19148531
APA StyleNauwelaerts, S. J. D., De Cremer, K., Bustos Sierra, N., Gand, M., Van Geel, D., Delvoye, M., Vandermassen, E., Vercauteren, J., Stroobants, C., Bernard, A., Saenen, N. D., Nawrot, T. S., Roosens, N. H. C., & De Keersmaecker, S. C. J. (2022). Assessment of the Feasibility of a Future Integrated Larger-Scale Epidemiological Study to Evaluate Health Risks of Air Pollution Episodes in Children. International Journal of Environmental Research and Public Health, 19(14), 8531. https://doi.org/10.3390/ijerph19148531